
Abstract
Background
Cardiovascular risk factor research has recently broadened its focus based on new data indicating the benefits of low risk, i.e. favorable levels of all major risk factors. The aims of this study were to assess further the relation of low risk to coronary heart disease risk, and implications for prevention.
Design
We conducted a prospective population-based Italian study, of 7438 men and 13 009 women aged 35–69 years, with a mean follow-up of 10.4 years and validated first coronary events.
Methods
Baseline coronary heart disease risk was classified into three categories: low risk; unfavorable but not high risk; and high risk. To analyze the relation of these risk profiles to coronary heart disease incidence, age-adjusted, sex-averaged coronary heart disease incidence was calculated for persons free of coronary heart disease and stroke, stratified as baseline low risk, unfavorable but not high risk or high risk. To assess the independent relationship of individual risk factors to coronary heart disease incidence, multivariate proportional hazards models were computed for combinations of risk factors.
Results
Only 2.7% of participants met low risk criteria; 81.4% were high risk. Age-adjusted coronary heart disease incidence for the whole cohort was 37.1 out of 10000 person-years (men 59.0; women 15.3). No coronary heart disease events occurred in low-risk men, only two in low-risk women. For women and men who were not high risk, the age-sex standardized coronary heart disease rate was 62% lower than for high-risk participants. Blood pressure, need for antihypertensive medication, smoking, hyperglycemia, diabetes, total and high-density lipoprotein cholesterol were independently related to coronary heart disease risk.
Conclusions
Favorable levels of all modifiable readily measured risk factors - rare among Italian adults - assure minimal coronary heart disease risk. Population-wide prevention is needed, especially improved lifestyles, to increase the proportion of the population at low risk.
Introduction
In recent years, an important conceptual advance has been introduced concerning the major cardiovascular disease (CVD) risk factors: the focus is no longer exclusively on their adverse effects, but also on protective effects of favorable levels of all readily measured modifiable major coronary heart disease (CHD) risk factors, namely low risk. Low-risk persons are rare in the general population and therefore research on the impact of low risk requires large cohorts followed long-term. Available data indicate that for low risk substrata, CVD, particularly CHD, is rare and endemic, not epidemic, throughout adulthood. These findings come from only three studies, however, all of US cohorts [1–5].
The possibility that low-risk protects against CHD is important, since CHD remains a major cause of morbidity, disability, and death (European Health for All Database, website: http://www.WHO.dk/hfadb). In this study we assessed the impact of low risk on 10-year CHD incidence in 20447 women and men at baseline ages of 35–69 years, from the Italian longitudinal study, the Progetto CUORE [6].
Methods
Population samples
Twelve random samples of general populations aged 35–69 years were studied: seven from general populations in north Italy (the MONICA study, Brianza 1986, 1990, 1993; Friuli 1986, 1989, 1994; the PAMELA study); five in central or southern Italy (MONICA Latina, 1984–86; MATISS 1984, 1987, 1993; ATENA).
Baseline measurements
Risk factors were assessed by standardized procedures [6, 7]. Blood pressure (right arm) was measured twice with a mercury sphygmomanometer, participant sitting, rested 5 min; systolic blood pressure (SBP)/diastolic blood pressure (DBP) were recorded (first and fifth Korotkoff sounds); these first and second measurements were averaged for analyses. Serum total and high-density lipoprotein (HDL) cholesterol were assayed by enzymatic colorimetry. Fasting plasma glucose was measured in 63% of participants. Height and weight were measured with the participant wearing light clothing without shoes. Body mass index (BMI) was computed as weight/height2 (kg/m2). Information was collected by questionnaire on cigarette smoking, personal history of myocardial infarction (MI), stroke, diabetes mellitus, hospitalization for cardiovascular events and medication use. Sources for checking data included MONICA registers and hospital discharge records (i.e., information from medical doctors). As to medication use, this was checked (verified) by having the participant bring in his or her medications to the baseline examination, for review and recording by trained staff.
Coronary events registration/validation
During follow-up (mean time 10.4 years), deaths were identified from vital statistics. Death certificates were coded using the International Classification of Diseases and Causes of Death, Ninth Revision (ICD-9) [8]. Vital status and death certificates were available for 99% of participants. Underlying causes of death ICD-9 codes 410–414 (ischemic heart disease), 798 (sudden death), 799 (other ill-defined and unknown causes of morbidity and mortality) as well as codes 250 (diabetes mellitus), 428 (heart failure), 440 (atherosclerosis) in association with 410–414 codes, were considered as suspected coronary deaths and further investigated for validation. Non-fatal coronary events were ascertained through record linkage using hospital discharge diagnosis records with ICD-9 410–411 (acute myocardial infarction, other acute and sub-acute forms of ischemic heart disease) codes for suspected acute infarction and ICD-9-CM 36.0–36.9 codes for coronary surgery revascularization; MONICA registers, sample re-examinations, contacts with general practitioners, patients, and relatives were used. Fatal and non-fatal coronary events were validated using MONICA diagnostic criteria [9], based on symptom combinations, electrocardiograms, cardiac enzymes, history of CHD, and available autopsy findings.
Data analyses
Ten-year coronary incidence rates were calculated and age-adjusted (direct method) using the European population 1995 (World Population Prospects: The 2002 Revision United Nations, Population database; website http://esa.un.org/unpp/). For both low-risk and unfavorable-but-not-high-risk men and women, CHD events were few (or none) in 5-year age groups, especially at younger ages. Accordingly, to reduce possible distortion in age adjusted rates, adjustment was based on the strata ages 35–49, 50–59, and 60–69 years, for men and women separately. Given the considerably greater number of women than men, to avoid sex weighting of overall incidence rates, non-weighted averages of male and female rates were calculated. CHD incidence rates were so calculated for the strata classified by baseline risk factor findings as low risk, unfavorable but not high risk, low risk plus unfavorable but not high risk, and high risk (see below for strata definitions). For low risk, paucity of CHD events precluded calculation of age-sex standardized rates. Based on age-sex standardized rates for the low risk plus unfavorable but not high risk stratum, expected numbers of CHD events were calculated for the high-risk stratum.
Risk factors included total cholesterol, HDL cholesterol, fasting glucose, SBP, DBP, BMI; SBP/DBP identified normal (SBP ≤ 120 mmHg and DBP ≤ 80 mmHg), prehypertensive (SBP 121–139 mmHg or DBP 81–89 mmHg), hypertensive stage I (SBP 140–159 mmHg or DBP 90–99 mmHg), or hypertensive stage II (SBP ≥ 160 mmHg or DBP ≥ 100 mmHg or antihypertensive drug treatment irrespective of SBP/DBP) [10]. Diabetes definition was a fasting plasma glucose ≥ 6.99 mmol/l (≥ 126 mg/dl) [11], or self-reported drug-treated diabetes. Cigarette use was classified as never, past only, current and by the number of cigarettes per day.
Low risk included persons with all the following characteristics: total cholesterol <5.17 mmol/l (< 200 mg/dl), SBP ≤ 120 mmHg, DBP ≤ 80 mmHg, no antihypertensive medication, BMI <25.0 kg/m2, no diabetes, no smoking, i.e., favorable levels of all readily measured modifiable major CHD/CVD risk factors.
Unfavorable but not high risk included persons with one or more of the following: total cholesterol 5.17–6.18 mmol/l (200–239 mg/dl), SBP 121–139 mmHg, DBP 81–89 mmHg (no antihypertensive medication), BMI 25.0–29.9 kg/m2; also, no diabetes, no smoking.
High risk included persons with one or more of the following: total cholesterol ≥ 6.19 mmol/l (≥ 240 mg/dl), SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, need for anti-hypertensive medication, BMI ≥ 30.0 kg/m2, diabetes, smoking.
To assess the relationship of each risk factor to CHD incidence, univariate analyses—categorical and continuous as appropriate—adjusted for age, sex and sample were also done, yielding for each risk factor a proportional hazards regression coefficient (standard error, SE), hazard ratio (HR) and 95% confidence interval (CI) [12]. Age, sex, and sample-adjusted multivariate proportional hazards models were then computed for combinations of risk factors significant in the univariate analyses.
Multicolinearity was first checked by partial correlation analysis (controlled for age, sex, sample); no highly correlated variables were included in a multivariate model. Interactions were assessed of sex with each modifiable risk factor; also of smoking with each other risk factor.
Results
Since baseline and follow-up findings were similar for men and women, detailed data tabulated here are for the two sexes combined. Participation rates were between 64 and 78% except for MATISS 1987 (40%) [13]. Less than 1% were lost to 10-year follow-up (150 out of 20 447); they contributed to the follow-up period until the date of the last available information.
Baseline descriptive statistics
Of the 20447 participants, average age 50.4 years, only 543 (2.7%) were low risk (1.4% of men and 3.4% of women); most (81.4%) (84.9% of men and 79.3% of women) were high risk (Table 1). Among both men and women, the high risk proportion was progressively greater with age, for example, for men 76.4% at age 35–39 years, 90.9% at ages 65–69 years; for women, 57.5% and 94.3%. By definition, risk factor levels differed markedly across risk factor strata, especially for low risk compared with high risk, for example, SBP/DBP 111/72 mmHg for low risk, 141/86 for high risk; serum total cholesterol 4.53 and 5.96 mmol/l (175.0 and 234.6 mg/dl); BMI 22.2 and 27.6 kg/m2. Of 16 638 high risk persons, 39% were smokers, 61% were hypertensive (31% stage II elevation or receiving antihypertensive drug treatment).
For all 20 447 participants, the whole cohort, baseline average SBP and DBP were in prehypertensive ranges, only 20% had normal blood pressure; the total cholesterol mean was borderline high; average BMI was in the overweight range; the prevalence of current cigarette smoking was 31% (40% of men and 26% of women) (Table 1).
Coronary heart disease incidence
First coronary events numbered 656 (men 469; women 187), 464 non-fatal, 192 fatal; age-adjusted incidence was 3.9 times higher in men (59.0/10000 person—years) than women (15.3/10000 person—years). CHD incidence increased markedly across the 5-year age groups: for men ages 35–39, 22.9/10000 person—years, at ages 65–69, 115.8; women ages 35–39, 3.1/10000 person—years, at ages 65–69, 50.6 (detailed data not tabulated).
Relation of baseline risk status to coronary heart disease
Of 439 low-risk women, two developed CHD, at ages 57 and 60 years; of 104 low-risk men, none experienced CHD in 10 years; the averaged crude rate for the two sexes combined was 2.3/10000 person—years (Table 2). In contrast, the averaged crude rate for high-risk men and women combined was 40.6/10000 person—years; the corresponding adjusted rate being 39.8 (62.6 for men, 17.0 for women). For persons not high risk (i.e., low risk plus unfavorable but not high risk), the sex-averaged age-adjusted rate was 15.2/10000 person—years (22.0 for men, 8.4 for women); that is, the risk ratio of low risk plus unfavorable but not high risk compared with the high-risk stratum was 0.38 or 62% lower CHD risk. As these data indicate, CHD risk was also much lower for the unfavorable-but-not-high-risk stratum, compared with the high-risk stratum (Table 2).
Expected numbers of CHD events for high-risk men and women, having the age-adjusted, sex-specific rates of those not high risk, were 240.4 (155.7 for men and 84.7 for women), compared with 614.2 (442.0 and 172.2) estimated from their adjusted rates: 373.8 fewer events total (61% fewer events) (Table 2).
Baseline descriptive statistics by risk status, men and women combined
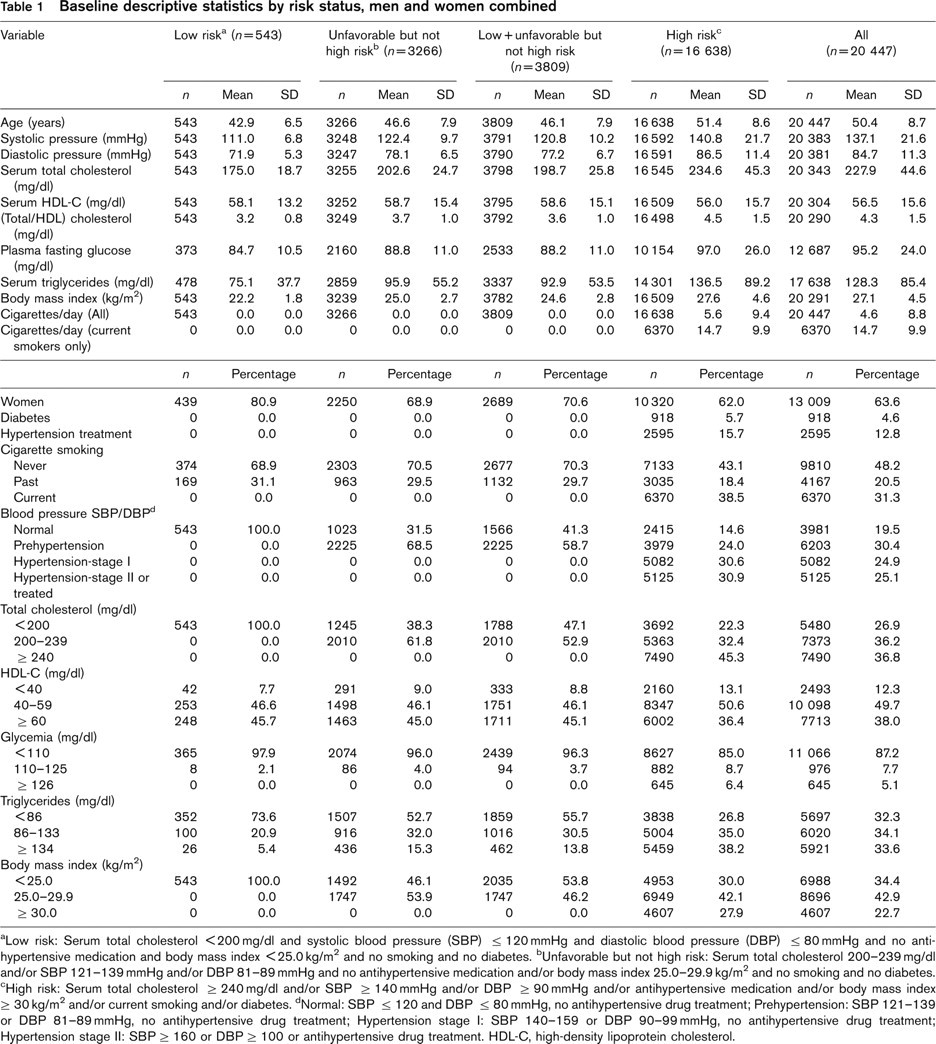
aLow risk: Serum total cholesterol <200 mg/dl and systolic blood pressure (SBP) ≤ 120 mmHg and diastolic blood pressure (DBP) ≤ 80 mmHg and no antihypertensive medication and body mass index <25.0 kg/m2 and no smoking and no diabetes. bUnfavorable but not high risk: Serum total cholesterol 200–239 mg/dl and/or SBP 121–139 mmHg and/or DBP 81–89 mmHg and no antihypertensive medication and/or body mass index 25.0–29.9 kg/m2 and no smoking and no diabetes. cHigh risk: Serum total cholesterol ≥ 240 mg/dl and/or SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg and/or antihypertensive medication and/or body mass index ≥ 30 kg/m2 and/or current smoking and/or diabetes. dNormal: SBP ≤ 120 and DBP ≤ 80 mmHg, no antihypertensive drug treatment; Prehypertension: SBP 121–139 or DBP 81–89 mmHg, no antihypertensive drug treatment; Hypertension stage I: SBP 140–159 or DBP 90–99 mmHg, no antihypertensive drug treatment; Hypertension stage II: SBP ≥ 160 or DBP ≥ 100 or antihypertensive drug treatment. HDL-C, high-density lipoprotein cholesterol.
For high-risk substrata, sex-averaged, age-adjusted CHD incidence increased with number of high-risk factors, such as, with one risk factor only high 26.4/10000 person-years; for two or more high (52.7% of all 20447 participants) 48.5/10000 person—years; four or more high, 66.7 (Table 2).
Relation of risk factors considered singly to coronary heart disease risk
Findings were similar for both sexes with no significant sex risk factor interactions. There were significant continuous graded relations of SBP and DBP to CHD incidence (P <0.001), stronger for SBP than DBP (HR 1.45 and 1.25 with 1 SD higher SBP, DBP) (Table 3). For the large stratum with hypertension stage I, HR was 1.61 compared with those with normal SBP/DBP (P <0.01); for those with stage II high blood pressure, 2.72 (P <0.001). Total cholesterol was significantly related to CHD risk (P <0.001, HR 1.40, 1 SD higher); HDL cholesterol was related inversely (P <0.001, HR 1.35, 1 SD lower); cigarette smoking was strongly related to CHD risk, HR 2.00 for current versus never smokers (P <0.001); past smoking was also significantly related to CHD, HR 1.41 (P <0.01). As a continuous variable, BMI was significantly related to CHD risk (HR 1.12, 1 SD higher; P <0.05); considered as a categoric variable, BMI in both the overweight and in the obese range was associated with increased CHD risk, HR 1.37 (P <0.001) and 1.25 (not statistically significant). Fasting plasma glucose was positively related to CHD risk (P <0.001, HR 1.12, 1 SD higher); for persons with glucose concentration ≥ 126 mg/dl, HRwas 1.69 (P <0.001) compared with those with fasting glucose under 110 mg/dl. For diabetic participants, HR was 1.71 (P <0.001).
Ten-year coronary heart disease incidence by baseline risk status, men and women combined
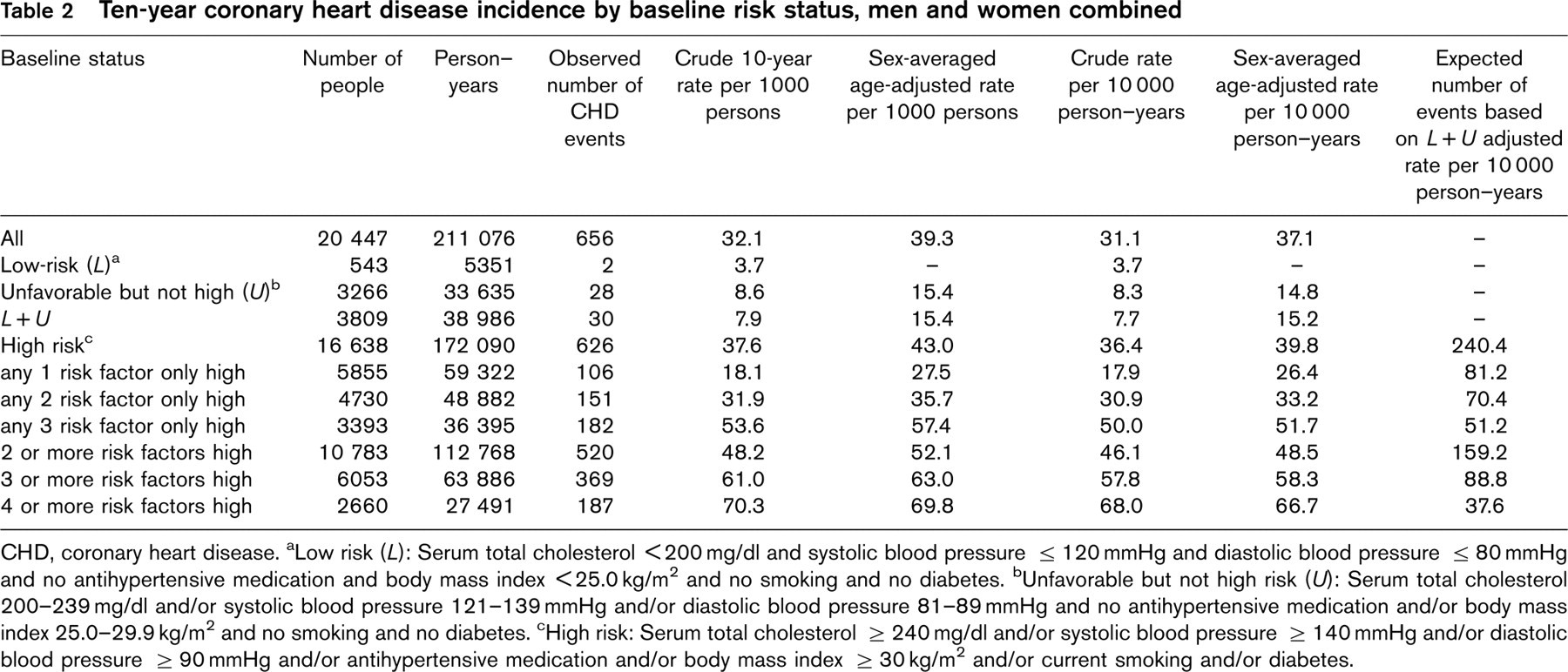
CHD, coronary heart disease. aLow risk (L): Serum total cholesterol <200 mg/dl and systolic blood pressure ≤ 120 mmHg and diastolic blood pressure ≤ 80 mmHg and no antihypertensive medication and body mass index <25.0 kg/m2 and no smoking and no diabetes. bUnfavorable but not high risk (U): Serum total cholesterol 200–239 mg/dl and/or systolic blood pressure 121–139 mmHg and/or diastolic blood pressure 81–89 mmHg and no antihypertensive medication and/or body mass index 25.0–29.9 kg/m2 and no smoking and no diabetes. cHigh risk: Serum total cholesterol ≥ 240 mg/dl and/or systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg and/or antihypertensive medication and/or body mass index ≥ 30 kg/m2 and/or current smoking and/or diabetes.
For each risk factor except total cholesterol and BMI, HRs were higher for women than men: for total cholesterol, the HR for women was less than for men (1.31 and 1.44); for BMI, HRs for the two sexes were virtually identical. There was no significant interaction of smoking and any of the other risk factors.
Relation of multiple risk factors considered together to coronary heart disease risk
In Cox multivariate models, risk factors significantly, independently, directly related to CHD were SBP, total cholesterol, lower HDL cholesterol, need for antihypertensive treatment, current cigarette smoking, diabetes; hazard ratios ranged from 1.33 (SBP) to 1.80 (current cigarette smoking) (Table 4). Given no significant risk factor interactions, these independent risks are multiplicative, such as for persons who smoke (compared with non-smokers) with SBP 137 mmHg (versus 115) and total cholesterol 228 mg/dl (versus 183), from model 1, HR = 1.80 (smoking) × 1.33 (SBP) × 1.38 (total cholesterol) = 3.30 times; or, the inverse, with favorable levels, lower risk HR = 0.30, i.e., CHD risk 70% lower.
As in univariate Cox analyses, sex-specific coefficients were higher for women than men for each risk factor except total cholesterol, conspicuously so for cigarette smoking (2.49 and 1.68) (detailed data not tabulated).
Discussion
The main findings of this Italian longitudinal study of more than 20000 men and women aged 35–69 years, in relation to 10-year CHD incidence of low-risk status (favorable levels of all readily measured modifiable major CVD risk factors) are as follows: at baseline, only 2.7% low risk, 81.4% high risk (one or more risk factor levels high); only two CHD events in 543 low-risk individuals; and for all persons not high risk (low risk plus unfavorable but not high risk), the age-sex standardized coronary event rate was 62% lower than for those high risk. The findings are consistent for men and women.
These results on the protective effects against CHD in both sexes with favorable levels of all (or most) readily measured modifiable major risk factors are concordant with data on the large cohort of men aged 35–57 screened in 18 US cities for the Multiple Risk Factor Intervention Trial (MRFIT) followed for 25 years and on the large cohorts of Chicago men and women ages 18–59 followed for 30 years [1, 4]. Across six cohorts of low-risk young adult and middle-aged men and women, 25–30-year CHD risk was lower by 69–92% compared with all others (not low-risk), and lower by 79–96% compared to those with two or more risk factors high [4]. The Progetto CUORE data are also concordant with 14-year findings from the large Nurses Health Study of US women with baseline ages 30–55, using, absent directly measured major risk factor data, lifestyle data collected by questionnaire [5]. Low-risk was defined as all of no smoking, BMI <25.0 kg/m2, moderate-to-vigorous physical activity at least one-half hour per day; score in the highest 40% of the cohort for diet high in cereal fiber, marine omega-3 fatty acids, folate, polyunsaturated/saturated fatty acids ratio, low in trans fatty acids and glycemic load, and average alcohol intake of at last half a drink per day. For low-risk women so defined, the risk of a major CHD event was 83% less than for all other women (with control for age, diagnosed high blood pressure or serum total cholesterol, menopausal status, and family history of CVD). Across all seven of these US cohorts, only a small minority were low risk, such as in the Nurses Health Study only 3% were low risk based on the stipulated lifestyle criteria [5], as was the case for the Progetto CUORE cohort based on all readily measured modifiable major risk factors. Among all seven US cohorts and the Progetto CUORE cohort, the great majority were high risk at baseline.
Relation of risk factors considered singly to 10-year coronary heart disease risk, men and women combined: hazard ratios (HR) and 95% confidence intervals (CI), Cox proportional hazards regression analyses
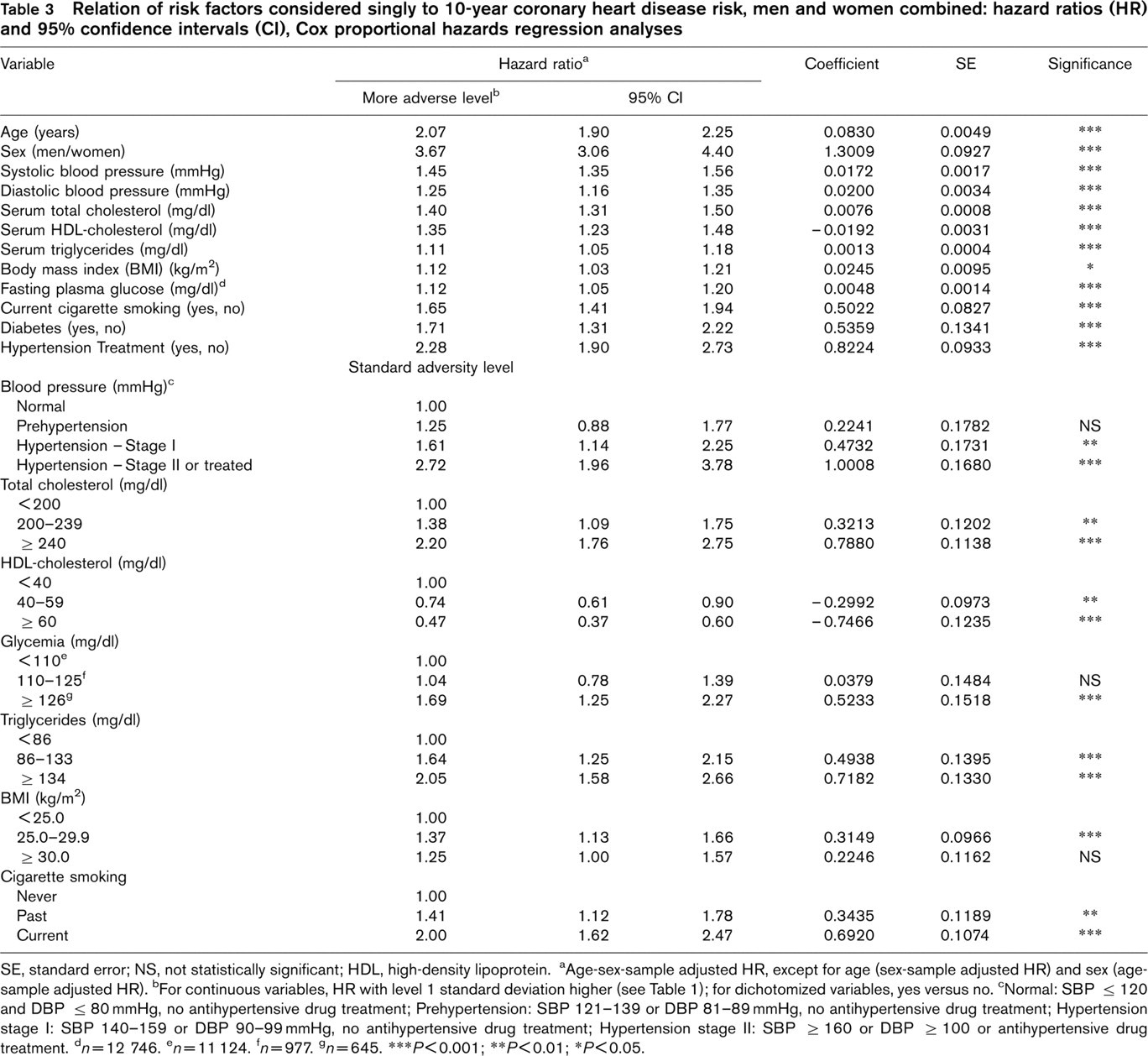
SE, standard error; NS, not statistically significant; HDL, high-density lipoprotein. aAge-sex-sample adjusted HR, except for age (sex-sample adjusted HR) and sex (age-sample adjusted HR). bFor continuous variables, HR with level 1 standard deviation higher (see Table 1); for dichotomized variables, yes versus no. cNormal: SBP ≤ 120 and DBP ≤ 80 mmHg, no antihypertensive drug treatment; Prehypertension: SBP 121–139 or DBP 81–89 mmHg, no antihypertensive drug treatment; Hypertension stage I: SBP 140–159 or DBP 90–99 mmHg, no antihypertensive drug treatment; Hypertension stage II: SBP ≥ 160 or DBP ≥ 100 or antihypertensive drug treatment. d n = 12746. e n = 11124. f n = 977. g n = 645. ∗∗∗P<0.001; ∗∗P<0.01; ∗P<0.05.
For the several population samples from northern, central, and southern Italy making up the Progetto CUORE, the adverse risk factor levels recorded in the 1980–1990s contrast markedly with 1950–1960s population-based data on Italian middle-aged cohorts, such as from the Seven Countries Study, especially in regard to average levels and distributions of serum cholesterol and BMI [14–20]. In Italy during these decades, per capita intakes of total energy, total and saturated fats, cholesterol, sugars have all gone up considerably. Correspondingly, average total cholesterol levels for middle-aged Italian cohorts in the 1980 and 1990s were in the range 5.70–5.96 mmol/l (220–230 mg/dl), which was considerably higher than for Italian cohorts surveyed in the late 1950 and early 1960s [16]. Along with declines in physical activity of work and leisure, the serially more unfavorable eating patterns account also for increasing overweight/obesity.
Relation of risk factors considered together to 10-year coronary heart disease risk, men and women combined: multivariate proportional hazards regression models
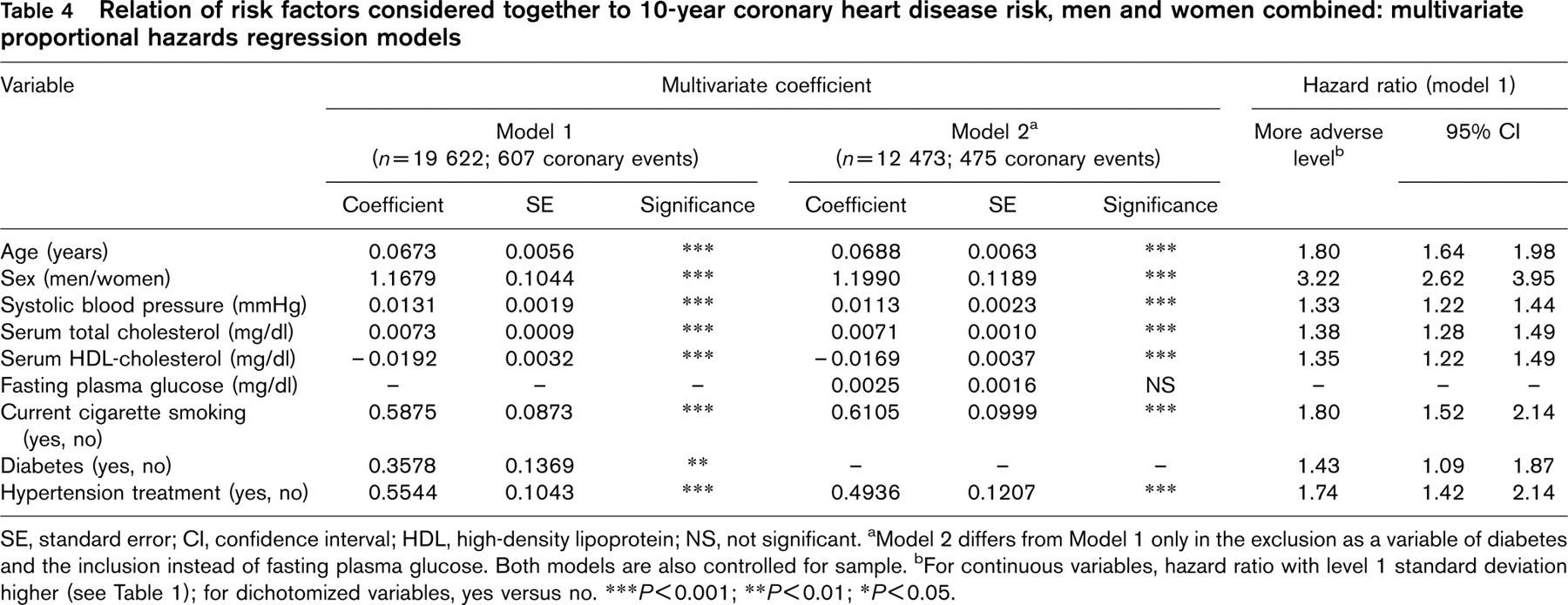
SE, standard error; CI, confidence interval; HDL, high-density lipoprotein; NS, not significant. aModel 2 differs from Model 1 only in the exclusion as a variable of diabetes and the inclusion instead of fasting plasma glucose. Both models are also controlled for sample. bFor continuous variables, hazard ratio with level 1 standard deviation higher (see Table 1); for dichotomized variables, yes versus no. ∗∗∗P<0.001; ∗∗P<0.01; ∗P<0.05.
In these regards it is relevant also to note recent research advances on relations of multiple dietary factors to blood pressure: data from several epidemiologic studies and from the well controlled DASH and OMNIHEART feeding trials indicate that multiple dietary factors—macronutrients and micronutrients, electrolytes (NaCl, K)—influence blood pressure, as well as caloric imbalance (overweight/obesity) and excess alcohol intake [21–28]. Habitual dietary patterns that favorably influence blood pressure are diets lower in salt and alcohol; higher in multiple minerals and vitamins, vegetable and total protein, monounsaturated fats, fiber; lower in total fats, saturated fats, cholesterol, sugars [22, 23]. In all these regards the DASH combination diet, which was highly efficacious in reducing SBP/DBP for both prehypertensive and hypertensive adults, resembles Italian dietary patterns of the late 1950s and 1960s: high in fruits, vegetables, whole grains; emphasizing seafood, lean poultry, fat-free and low fat dairy products, legumes, nuts, olive and seed oils in modest amounts; low in red meats, fat-containing dairy products, eggs, sugars and sweets. The recommended DASH eating pattern, however, differs from traditional Italian fare in two respects: for Italians, salt and alcohol intakes have been on average high, not low. It is a reasonable inference that these two aspects, along with caloric imbalance (overweight/obesity), account importantly for unfavorable average SBP/DBP levels among Italian adults.
In this context a reasonable deduction is that the apparent attrition/loss by the Italian population in the latter decades of the 20th century of the earlier prevailing ‘Mediterranean advantage’ relates to extensive lifestyle changes during these years, particularly altered dietary and physical activity patterns [29].
The limitations of the present study include the small size of low-risk sub-cohorts (male, female); the concordant results on CHD here and for the six low-risk cohorts similarly defined (MRFIT, Chicago), however, support the inference that low risk as defined protects generally against CHD, an inference given further broad support by the concordant results from the Nurses Health Study with low risk defined by favorable lifestyle traits [5]. A further limitation is that low-risk status is based on only one measurement of the risk factors; this limitation, the regression dilution bias problem [30], however, leads to some people being improperly designated low risk, with resultant underestimation of the favorable effects of low risk. Furthermore, there are no data on eating, drinking or exercise, lifestyle traits implicated as important CVD risk factors; the lack of data on these traits, however, makes more impressive the benefit against CHD with favorable levels of readily measured modifiable major risk factors, and again it is relevant to note the concordant findings from the Nurses Health Study with low risk defined based on multiple lifestyle criteria. That only 10-year follow-up data were obtained is another limitation; favorable findings for low risk and CHD prevailed for the Nurses, MRFIT, and Chicago cohorts, however, with 14, 25, and 30-year follow-up [1–5]. Finally, the participation rate was from 40–78%; risk factor average levels and distributions were similar, however, across all 12 samples and like those for samples in other European countries in the 1980s–1990s.
In conclusion, low risk, favorable levels of all readily measured modifiable major CVD risk factors, is associated with low CHD rates. Low prevalence rates of low risk in contemporary populations are products of adverse lifestyles, all amenable to prevention and control, including smoking, adverse eating and drinking patterns, sedentary habit, causing commonality of elevated blood pressure, hyperglycemia/diabetes, dyslipidemia, obesity. Intervention in the general population needs to be implemented, emphasizing improved lifestyles: non-smoking, prevention and control of overweight/obesity with eating patterns of original Mediterranean composition, enhanced to include lower salt and alcohol intakes, and greater habitual physical activity. The priority strategic aim is to increase progressively the proportion of the population at low risk at all ages, and this is key to ending the CHD/CVD epidemic.