
Abstract
Background
Physical activity is a healthful behavior that has promise for combating feelings of low energy and fatigue. Despite evidence suggesting that fatigue is a prodromal symptom of major cardiac events, improvements in feelings of energy and fatigue have largely been ignored by reviewers of cardiac rehabilitation literature who have focused on anxiety, depression and general measures of quality of life.
Design
A meta-analytical review.
Methods and results
Computer databases were searched from January 1945 to May 2005 to identify relevant literature. A total of 36 studies consisting of 4765 subjects were included. Cardiac rehabilitation exercise programs were consistently associated with increases in energy and decreases in fatigue. The magnitude of the effect was moderately large (mean delta 0.51; 95% confidence interval 0.42–0.61) but was heterogeneous and modified by features of the research design. Comparison of effect sizes in cardiac rehabilitation studies concurrently measuring energy/fatigue, anxiety and depression suggest that exercise-based cardiac rehabilitation programs have larger effects on feelings of energy and fatigue compared with anxiety and depression.
Conclusion
This review quantifies the potential benefit of cardiac rehabilitation exercise programs on feelings of energy and fatigue, and suggests that cardiac rehabilitation researchers and practitioners may benefit from examining, and perhaps even focusing on, feelings of energy and fatigue as an important outcome variable. A greater understanding of the effect of cardiac rehabilitation exercise programs on feelings of energy and fatigue will be reached when more true experiments are conducted thereby avoiding the primary limitation of the literature reviewed; that is, the frequent use of non-experimental research designs.
Introduction
Physical activity is a healthful behavior that has promise for combating feelings of low energy and fatigue [1–3]. However, improvements in feelings of energy and fatigue have largely been ignored by reviewers of cardiac rehabilitation literature who have focused on anxiety [4, 5], depression [4, 6] and general measures of the quality of life [7]. This is despite evidence suggesting that fatigue is a prodromal symptom of major cardiac events [8–10]. Cardiac rehabilitation researchers and practitioners may benefit from examining, and perhaps even focusing on, feelings of energy and fatigue as an important outcome variable. For example, one meta-analytical review found that exercise training programs had a 0.37 standard deviation effect on the improvement in feelings of low energy and fatigue [2]. The review suggested that the effect of an exercise intervention on feelings of energy and fatigue may be even greater for cardiac rehabilitation patients. Such an effect would be similar to other, more frequently discussed, psychological outcomes of cardiac rehabilitation exercise programs such as anxiety and depression (0.32 and 0.46 standard deviation effect, respectively) [4].
A consensus definition of fatigue has yet to be accepted across the clinical and medical research communities. It is probable that the feelings of energy and fatigue are multidimensional, with emotional, behavioral and cognitive components. Feelings of energy and fatigue have been conceived in various ways, including as symptoms, moods, dimensions of cognitive effort, and aspects of quality of life [11, 12]. However, for our purposes, the focus is on energy and fatigue conceptualized as mood states. Energy when defined as a mood state refers to the subjective feeling of having the capacity to complete mental or physical activities. Fatigue when defined as a mood state refers to the subjective feeling of having a reduced capacity to complete mental and physical activities [12].
One barrier that has hindered the advancement of knowledge about fatigue is the construct's co-morbidity with medical conditions. Symptoms of fatigue are associated with many physical illnesses including heart disease. Individuals with chronic disease are two to three times more likely to have associated feelings of fatigue than the normal population [13]. Psychiatric disorders are also strongly associated with fatigue. The risk of fatigue among those suffering from symptoms of anxiety and depression ranges from three to six times that of the normal population [14]. Despite the high co-morbidity of fatigue in a variety of medical conditions, studies have found prolonged feelings of fatigue to exist independently of physical and psychiatric disorders, thus providing evidence of fatigue being a problem in and of itself [15, 16].
Meta-analysis may be especially useful in quantifying the effect of cardiac rehabilitation exercise programs on feelings of energy and fatigue and comparing this effect with other psychological constructs. This type of analysis could place feelings of energy and fatigue within the framework of other psychological constructs that have been recognized as contributing to the pathogenesis and expression of coronary artery disease [17]. Such information could reveal reduced feelings of fatigue as an important, underappreciated, mental health benefit of cardiac rehabilitation. Therefore, the main objective of this study was to examine the effects of cardiac rehabilitation exercise programs on feelings of energy and fatigue. The comparison of the effects of cardiac rehabilitation programs on feelings of anxiety, depression and fatigue was also examined in an attempt to weigh the construct of energy and fatigue against more commonly recognized psychological constructs in the area of cardiac rehabilitation.
Dependent measures of energy and fatigue
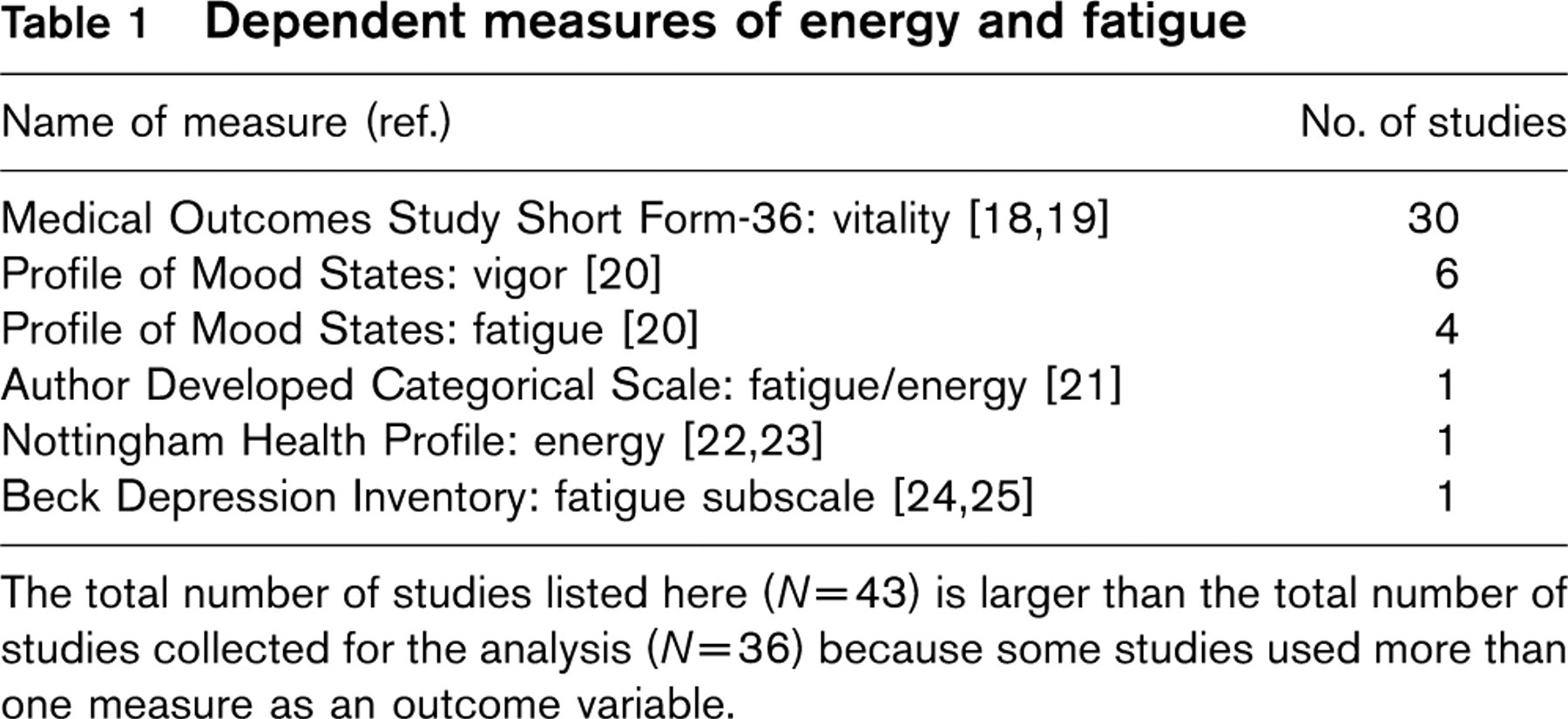
The total number of studies listed here (N=43) is larger than the total number of studies collected for the analysis (N=36) because some studies used more than one measure as an outcome variable.
Methods
Literature search
Google Scholar, Medline, PsycInfo, PubMed and Web of Science databases were searched from January 1945 to May 2005 using the key words cardiac rehabilitation, energy, exercise, fatigue, mood, physical activity, Profile of Mood states, quality of life, resistance training, Short Form 36 (SF-36), and vitality. Searches were supplemented by reference lists from retrieved articles. Criteria for inclusion were: (i) the independent variable involved a cardiac rehabilitation exercise program or chronic exercise intervention of at least 4 weeks; (ii) the dependent variable was a measure of energy or fatigue (Table 1) [18–25] that was assessed before and either during or immediately after the intervention; there is substantial published evidence that the scores from the measures used can be validly interpreted as measures of energy and fatigue [12] with the exception of one author-developed scale [21]; (iii) the sample had coronary heart disease or was recovering from a cardiac event or surgery; and (iv) the design was experimental, quasi-experimental, or pre-experimental (i.e. one-group pretest–posttest). Studies using cross-sectional or correlational designs were excluded. In addition, studies examining the effect of a single bout of exercise on energy/fatigue were excluded as were studies in which the timing of the measurement of the chronic exercise effects appeared to have been confounded by transient effects of an acute bout of exercise. Investigations that measured vital exhaustion were also excluded. This review thus focused on studies that examined feelings of energy and fatigue per se and not the construct of vital exhaustion that by definition includes feelings of hopelessness, loss of libido and increased irritability in addition to feelings of low energy and fatigue [26]. A total of 36 studies and 4765 individuals were included (Table 2) [21, 27–61]. The 36 studies had an average sample size of 132 (range 23–387).
Assessment of study quality
The methodological quality of each study was assessed using a 15-item scale (1 point per item for a maximum of 15) as described elsewhere [62]. The scale addressed the fundamental aspects of the methods and reporting of clinical trials such as randomization, sample selection, outcome measures and statistical analysis. Quality scores were reported for each study for descriptive purposes, with higher scores representing a better research design (Table 2). Quality scores were not used as weights or moderators in the analysis because of the potential disparity that can exist in results depending on the specific quality scale employed [63].
Description of studies included in the meta-analysis
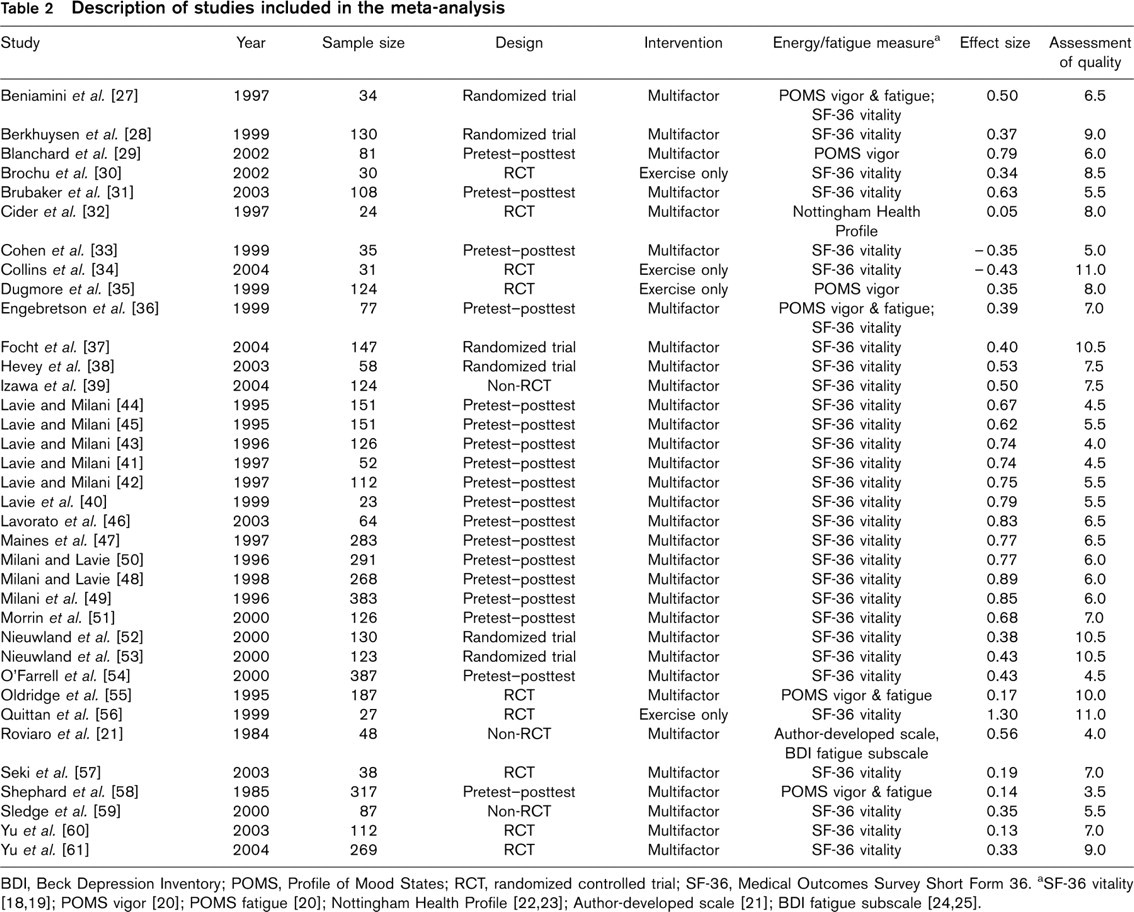
BDI, Beck Depression Inventory; POMS, Profile of Mood States; RCT, randomized controlled trial; SF-36, Medical Outcomes Survey Short Form 36.
Effect size calculations
Effect sizes were calculated by subtracting the mean change for a control group or condition from the mean change for an experimental group or condition and dividing this difference by the pooled standard deviation of pretest scores [64]. In those studies that did not include a comparison group (i.e. one-group pretest–posttest design; studies equal 24), the effect sizes were calculated by subtracting the pretest score from the posttest score and dividing the difference by the pretest standard deviation. Effect sizes were calculated so that increases in feelings of energy and decreases in feelings of fatigue resulted in positive effect sizes. All effect sizes were adjusted using Hedge's small sample size bias correction before being entered into the analysis [64]. When precise mean data were not reported, effect sizes were estimated [65] from F tests [27, 36], t-tests [46] or figures [36, 57, 61]. For studies in which precise standard deviations were not reported [34, 36, 61], the standard deviation was drawn from published norms or the study having the largest sample. In studies in which multiple effects could be obtained (e.g. studies with two or more outcome measures or that involved more than one intervention condition), effects were averaged so that only one value contributed to the analysis.
Statistical analyses
A macro, SPSS version 13.0 (SPSS Inc., Chicago, Illinois, USA) was used to calculate the aggregated mean effect size, the associated 95% confidence interval (CI) and the sampling error variance using a random effects model [66]. The effects were weighed by the inverse of their variance and recalculated with the random effects variance component added [66]. Heterogeneity was indicated if Q Total (the sum of squares of each effect of the weighted mean effect) [64] reached a significance level of P < 0.05 and the sampling error accounted for less than 75% of the observed variance [64]. To estimate the hypothetical impact of null findings from unpublished or unretrieved studies on the aggregated effect size estimate, a ‘failsafe N’ was computed to estimate the number of additional null effects that would attenuate the observed effect to 0.20 standard deviation [67].
Moderator analysis
A previous meta-analysis suggested that effects sizes related to changes in psychological variables (i.e. anxiety, depression) with participation in cardiac rehabilitation programs were not related to methodological characteristics such as the use of a control group [4]. However, it is likely that an investigation's study design (i.e. the use of a control group) could moderate the effect of cardiac rehabilitation exercise programs on feelings of energy and fatigue [2]. It has also been suggested that the specificity of the rehabilitation intervention may moderate the effect of cardiac rehabilitation programs on feelings of energy and fatigue such that multifactor interventions (i.e. exercise plus an additional therapy such as psychotherapy or health education) may produce larger effects than interventions that use exercise alone [2]. Therefore, study design and cardiac rehabilitation intervention were examined as moderator variables. Study design was categorized as a controlled or non-controlled trial. Cardiac rehabilitation intervention was categorized as a multifactor or exercise-alone intervention.
A weighted least squares linear regression analysis was conducted to determine the independent effect of the study design and cardiac rehabilitation intervention variables (P < 0.05) on the variation in effect size [64]. A macro (SPSS version 13.0; SPSS Inc.) was used for the regression analysis [66]. The analysis employed a random effects model to account for heterogeneity of moderator effects. The effects were weighed by the inverse of their variance and recalculated with the random effects variance component added [66].
If the moderators were significant in the regression analysis, the variables were decomposed using a random effects model to compute effect sizes, 95% CI and test the significance of the levels of the moderators [66]. Differences between levels of moderators were determined using the Q B statistic (i.e. the difference between Q computed within each moderator level and Q computed across moderator levels) [64]. Bonferroni post hoc contrasts were tested at P < 0.01.
Direct comparison of effects analysis
Cardiac rehabilitation exercise studies that concurrently measured anxiety, depression and energy/fatigue were selected from the examined literature in order directly to compare the magnitude of the effects among the three mental health outcomes. Effects sizes were calculated as previously described. Anxiety, depression and energy/fatigue effect sizes were then dummy coded. A macro (SPSS version 13.0; SPSS Inc.) was used to compute aggregated effect sizes adjusted for sample size, calculate the 95% CI and test the significance of coded effect size variables [66]. Differences among the effects for anxiety, depression and energy/fatigue were determined using the Q B statistic [64]. If the omnibus test was significant, apriori contrasts comparing anxiety and energy/fatigue and depression and energy/fatigue were tested at P < 0.05. All analyses employed a random effects model in which the effects were weighted by the inverse of their variance and recalculated with the random effects variance component added [66].
Results
The distribution of the 36 effects was negatively skewed (g1 = −0.57) and leptokurtic (g2 = −1.36). Thirty-four of the 36 effects (94.4%) were greater than zero. The mean effect size delta (95% CI) was 0.51 (0.42–0.61). The evidence showed a significant increase in feelings of energy and a decrease in feelings of fatigue after participation in cardiac rehabilitation exercise programs (z = 10.65, P < 0.001). The effect was heterogeneous (Q Total(35) = 134.11, P < 0.001). Sampling error accounted for 36.19% of the observed variance. The ‘failsafe N’ showed that 56 additional effects of zero would be required to reduce the observed value of 0.51 to 0.20.
Moderator analysis
The regression model containing study design and cardiac rehabilitation intervention were significantly related to effect size (Q R(2) = 6.13, P = 0.04, R2 = 0.16; Q E(33) = 32.56, P = 0.49). Study design (β = 0.27, z = 2.28, P = 0.02), but not cardiac rehabilitation intervention (β = 0.03, z = 0.18, P = 0.85), was independently related to the effect size. Decomposition of the study design variable showed that there was a significant difference between controlled and non-controlled trials (Q B(1) = 6.24, P = 0.01). Non-controlled trials (N = 24; Δ = 0.58; 95% CI 0.47–0.68) had a larger effect on feelings of energy/fatigue after a cardiac rehabilitation exercise program than controlled trials (N = 12; Δ = 0.32; 95% CI 0.14–0.50).
Direct comparison of effects
A total of 19 cardiac rehabilitation exercise studies (3025 individuals) concurrently measured anxiety, depression and energy/fatigue [27, 29, 35, 36, 38, 40–44, 47–50, 55, 57, 58, 61]. The 19 studies had an average sample size of 159 (range 23–383). There was a significant difference in effect sizes among the measures (Q B(2) = 8.34, P = 0.02). Improvements in feelings of energy/fatigue were significantly greater than improvements in both anxiety (Q B(1) = 5.46, P = 0.02) and depression (Q B(1) = 5.83, P = 0.02; Table 3).
Comparison of effect sizes in studies measuring anxiety, depression and energy/fatigue

CI, Confidence interval.
Discussion
Magnitude of the effect
Our analysis revealed that cardiac rehabilitation exercise programs were associated with a significant improvement in feelings of energy/fatigue in patients with coronary heart disease or those recovering from a cardiac event or surgery. Cardiac rehabilitation exercise programs had a moderate statistical effect (Δ = 0.51) on improved feelings of energy/fatigue in cardiac patients. This effect can be considered clinically significant. It has been suggested that a quality of life score change of greater than or equal to one standard error of the mean (SE) is clinically important in cardiac rehabilitation research [68]. The mean (SE) SF-36 vitality score at baseline for the 30 cardiac rehabilitation studies that used this measure was 51.0 (1.4) and the mean change during the program was 10.9. The improvement in feelings of energy and fatigue was thus almost eight times what has been suggested as a clinically meaningful effect.
The magnitude of the effect of cardiac rehabilitation exercise programs on feelings of energy/fatigue was similar to meta-analytically derived effects of cardiac rehabilitation programs on other aspects of mental health such as anxiety (mean d = 0.31) [4] and depression (mean d = 0.46) [4]. However, in the current analysis, a direct comparison of the effects of cardiac rehabilitation exercise on feelings of anxiety, depression and energy/fatigue revealed a significantly larger effect for feelings of energy/fatigue compared with that for anxiety and depression.
Moderators of the effect
Caution must be exercised to avoid misinterpreting these results. In this meta-analysis, the effect of chronic exercise on feelings of energy/fatigue in patients involved in cardiac rehabilitation programs was heterogeneous. This indicates that several factors outside of the exercise program itself could have impacted the size of the effect. Two such factors were the study design and cardiac rehabilitation intervention.
Study design
A previous meta-analysis suggested that effects sizes related to changes in psychological variables (i.e. anxiety, depression) with participation in cardiac rehabilitation programs were not related to methodological characteristics such as the use of a control group [4]. The present meta-analysis suggests otherwise for feelings of energy and fatigue. Of the 36 studies found in the literature search, only 12 were controlled trials. Of these controlled trials, six used a usual care control [21, 55, 57, 59–61], four used a no-treatment control [32, 35, 39, 56], and two used an attention control [30, 34]. Based on the interpretation of these results, cardiac rehabilitation studies that incorporated usual care, attention controls and no treatment controls produced effects that were smaller than non-controlled trials.
The infrequent use of control groups has limited the inferences that can be made concerning the effects of cardiac rehabilitation exercise programs on feelings of energy and fatigue. For example, the mean baseline vitality score across the cardiac rehabilitation studies (vitality score = 51.0 ± 7.7) was approximately 0.50 standard deviations below published norms for men and women aged 55 to 74 years [18]. Increased scores at the end of cardiac rehabilitation programs might thus be attributed to a regression to the mean. The use of a control group would allow for this type of artifact to be estimated. The results highlight the importance of incorporating control groups into the design of future cardiac rehabilitation studies.
Cardiac rehabilitation intervention
Multifactor cardiac rehabilitation interventions (Δ = 0.52, 95% CI 0.42–0.62) may have a larger effect on feelings of energy and fatigue than exercise-alone interventions (Δ = 0.34, 95% CI 0.02–0.71) as has been suggested in a previous meta-analysis [2]. However, the limited number of studies (four out of 36) examining the effects of exercise alone on feelings of energy and fatigue provided a sub-optimal data set for testing this ‘cardiac rehabilitation intervention’ moderator variable [30, 34, 35, 56]. More data from studies using exercise-alone interventions are needed to address this issue. More data are also needed to learn which component of a multifactor cardiac rehabilitation intervention accounts for most of the improvement in feelings of energy and fatigue.
Comparison of the effect with other constructs
Psychological benefits occur with exercise-based cardiac rehabilitation programs such as reductions in anxiety and depression [5, 6]. However, it is unknown how increases in feelings of energy and decreases in feelings of fatigue associated with rehabilitation exercise programs compare with other psychological constructs emphasized in cardiac rehabilitation research (i.e. anxiety, depression). Our results, based on studies that concurrently measured anxiety, depression and energy/fatigue, indicated that cardiac rehabilitation exercise programs have the greatest effect on improving feelings of energy/fatigue.
The larger improvements in feelings of energy/fatigue could be an artifact related to changes in medication regimens and fatigue-related side-effects, a variable that is poorly controlled for in the cardiac rehabilitation literature. For example, 36% of the reviewed studies had no discussion of medication use or dose changes during the course of the investigation [21, 29–31, 33, 34, 36, 37, 46, 54, 55, 58, 59]. It is also plausible that improvements in symptoms of fatigue may account for some or all of the anxiety and depression improvements with exercise-based rehabilitation because fatigue is comorbid with anxiety and depression. Moreover, the conclusions of this analysis assume that anxiety, depression and energy/fatigue are measured equally well. The literature did not permit us to assess this assumption.
Few studies have examined the relationship between anxiety, depression and energy/fatigue in relation to cardiac rehabilitation exercise programs. Only two studies in the literature review specifically investigated the effects of cardiac rehabilitation exercise programs on feelings of energy between groups with high compared with low symptoms of depression [48, 49]. No studies directly examined these effects in terms of patient anxiety. The two studies showed that cardiac rehabilitation patients with high pre-intervention symptoms of depression had significantly greater increases in feelings of energy, approximately a 0.25 standard deviation, over the duration of the exercise program compared with those who had few pre-intervention symptoms of depression. This suggests that higher pre-intervention depression scores are associated with greater improvements in feelings of energy and fatigue after cardiac rehabilitation exercise programs. Further research is needed to examine the association between anxiety, depression and energy/fatigue in the hope of understanding the relative importance of each in accounting for the overall psychological changes associated with cardiac rehabilitation exercise programs.
Mechanism of the effect
The mechanism by which improved feelings of energy and fatigue are realized in association with participation in cardiac rehabilitation programs is unknown, but several mechanisms are plausible. The results summarized here may be explained by a placebo effect. That is, the effect may have been caused by a factor incidental to the hypothesized active element (i.e. exercise training). A placebo effect is quantified by comparing the difference between placebo treated and untreated participants. Of the 12 controlled trials, two used an attention placebo [30, 34]. An attention-placebo effect could not be quantified, however, because these investigations did not include untreated controls. Placebo effects are thought to be mediated by conditioning or expectancy, and accumulating evidence suggests they have a central nervous system basis [69, 70].
Because brain neural circuits produce mood states it is logical to speculate that exercise training improves feelings of energy and fatigue by altering the specific neural circuits that underlie these moods. The specific brain circuits that generate the moods of energy and fatigue are poorly understood, but monoamines, histamine, acetylcholine, glutamate and γ-aminobutyric acid-mediated neurotransmission have been implicated in feelings of energy and fatigue based on psychopharmacology research [71–73]. The psychopharmacological findings are consistent with neuroimaging data showing greater activation in numerous brain circuits when fatigued individuals perform a fatiguing cognitive task [74]. Still other data suggest that specific brain regions, such as the dorsolateral prefrontal cortex, play a prominent role in mediating moods of energy and fatigue [71, 73]. Animal research has shown that physical activity can alter the neurotransmitters and neuromodulators mentioned above; however, there is an absence of data from human experiments examining the influence of chronic exercise on energy/fatigue mood states and relating the mood changes to changes in relevant measures of brain activity.
Conclusion
Improvements in feelings of energy and fatigue have largely been ignored by reviewers of the cardiac rehabilitation program literature, and this may be partly due to the fact that the focus of most of the studies into the psychological consequences of this type of rehabilitation has been either on anxiety [4, 5], depression [4, 6] or on general measures of quality of life [7] rather than on components of quality of life such as feelings of energy and fatigue. Our analyses show that cardiac rehabilitation exercise programs almost always improve feelings of energy/fatigue. The effect is moderately large and clinically meaningful. These findings suggest that cardiac rehabilitation researchers and practitioners may benefit from examining, and perhaps even focusing on, feelings of energy and fatigue as a salient outcome variable. Future cardiac rehabilitation studies should focus on finding which exercise characteristic(s) maximize the impact of cardiac rehabilitation exercise programs on feelings of energy and fatigue and which physical and psychological characteristics of cardiac patients should be considered in order to help tailor programs to meet patient needs. These issues could be addressed best through the introduction of control groups into research designs, thus avoiding the limitations of previous cardiac rehabilitation research.