
Abstract
Background
The objective of this study was to determine the effects of a moderate exercise training program on functional capacity, quality of life, and hospital readmission rate in chronic heart failure patients with implantable cardioverter defibrillators and cardiac resynchronization therapy.
Methods and results
We studied 52 men (mean age 55 ± 10 years, ejection fraction 31 ± 7%) in chronic heart failure II (n = 29) and III (n = 23) NYHA functional class with ischemic cardiomyopathy who received implantable cardioverter defibrillators with or without cardiac resynchronization therapy. Patients were randomized into two groups. Group T (n = 30 patients, 15 implantable cardioverter defibrillator, 15 implantable cardioverter defibrillator + cardiac resynchronization therapy) underwent a supervised exercise training program at 60% of peak Vo2 three times a week for 8 weeks. Group C (n = 22 patients, 12 implantable cardioverter defibrillator, 10 implantable cardioverter defibrillator + cardiac resynchronization therapy) avoided physical training. At 8 weeks, only trained patients had improvements in peak Vo2 (P < 0.01 versus C), endothelium-dependent dilatation of the brachial artery (P < 0.001 versus C) and quality of life (P < 0.001 versus C). Among trained patients, those with cardiac resynchronization therapy had greater improvements in peak Vo2 and quality of life. During the follow-up (24 ± 6 months), eight controls had sustained ventricular tachycardia requiring hospital readmission, while no trained patients had adverse events (log rank 8.56; P < 0.001). The improvement in peak Vo2 was correlated with the improvement in endothelium-dependent dilatation (r=0.65).
Conclusion
Moderate exercise training is safe and has beneficial effects after implantable cardioverter defibrillator implantation, especially when cardiac resynchronization therapy is present. These effects are associated with improvement in quality of life and outcome.
Keywords
Introduction
Patients with chronic heart failure have reduced exercise tolerance as compared with healthy subjects, as a result of several abnormalities in multiple organ systems. The reduced exercise tolerance further deteriorates exercise capacity, creating a vicious cycle of progressive deconditioning and worsening heart failure. In the last decade, several studies have demonstrated that heart failure patients in New York Heart Association (NYHA) functional class II and III receive an advantage from moderate exercise training, as indicated by significant improvements in exercise capacity, quality of life (QOL), and reduction in hospitalizations [1–6]. These benefits were obtained in the absence of any serious side effects during exercise training, and were the result of central and peripheral adaptations. Adverse events have been rare during follow-up, making exercise training safe in this population [7, 8].
A common feature predictive of adverse outcome in heart failure patients is, among others, prolongation of QRS duration [9]. Previous studies demonstrated that QRS delay, particularly left bundle branch block, creates electrical and mechanical dyssynchrony in patients with depressed left ventricular (LV) function. Nowadays, a growing number of patients with advanced heart failure receive an implantable cardioverter defibrillator (ICD), sometimes with cardiac resynchronization therapy (CRT) [10–12]. Shortening of the QRS duration with biventricular pacing has been demonstrated to translate into better LV mechanical performance [13, 14]. These effects have been associated with improvements in peak Vo2, anaerobic threshold and ventilation. All improvements are generally observed after a few weeks from implantation and are correlated with a better QOL [15]. More recently, a large-scale trial showed a significant reduction in the combined end point of all-cause mortality and all-cause hospitalization with cardiac resynchronization therapy in an advanced heart failure population [16]. It is unknown, however, whether the beneficial effects of exercise training described in patients with stable CHF may be also observed in patients with an implantable cardioverter defibrillator with less functional impairment (NYHA functional class II and III). Moreover, it is unknown whether the contribution of cardiac resynchronization therapy may potentiate the benefits of exercise conditioning. The rationale of exercise training in patients with ICD with and without CRT is based on its favorable documented effects on functional capacity, autonomic balance, myocardial perfusion and LV function already described in patients with CHF in stable condition [17]. Although few recent studies have reported on the safety and feasibility of exercise training in patients with ICD [18–21], it is not clear whether a program of exercise conditioning may have similar effects in patients with CRT, and whether it may influence the outcome.
The objective of the present study was to determine the effects of a moderate exercise-training program on functional capacity and QOL in a group of CHF patients in NYHA functional class II and III with ICD. Another objective was to evaluate whether exercising is safe and reduces the hospital readmission rate during the training period and follow-up. Moreover, we sought to determine whether patients with CRT have a different response to exercise training as compared to patients without CRT.
Methods
Study population
We screened 68 patients, 10 were excluded because they did not fit the eligibility criteria and six patients were excluded for other reasons (personal, logistic). The duration of the enrolment period was 8 months. The study group comprised 52 CHF patients in NYHA functional classes II and III who had ICD implantation during the last 3 months. CRT was delivered in 25 patients using a transvenous lead placed into the lateral or posterolateral side branch of the coronary sinus. All patients had a documented coronary artery disease, a depressed LV systolic function, and they were clinically stable during the last 2 months. The clinical characteristics are depicted in Table 1. The majority of the patients were on both angiotensin-converting enzyme (ACE) inhibitors and beta-blockers. Oral medications were not changed during the study (Table 1).
Study protocol
This is a longitudinal randomized controlled study. Stable CHF patients in NYHA functional class II and III without hospital admission or change in medications in the last 3 months and no evidence of ICD discharge were included in the study. Thirty patients were randomized to an exercise training program at 60% of peak Vo2, three times a week for 8 weeks, and 22 patients were randomized to a sedentary or control group. The two groups were well matched (Table 1). In the training group, 15 patients received an ICD and 15 patients ICD-CRT. Similarly, in the control group, 12 patients received an ICD and 10 patients ICD-CRT. The maximal tracking rate of any device was set 20 beats higher than the maximum peak heart rate achieved during the familiarization exercise test, in order to minimize the risk of inappropriate electric shocks. Patients were excluded if they had decompensated CHF, uncontrolled hypertension or diabetes mellitus, severe respiratory disease, significant anemia (or hemoglobin of less than 10 g/dl), renal insufficiency (creatinine greater than 2 mg/dl), or inability to exercise. Follow-up was 24 ± 6 months and started the day after the completion of the training program and ended with one of the following cardiac events: cardiac or any-cause of death, ventricular tachycardia, ventricular fibrillation, and acute cardiac decompensation requiring hospitalization. The protocol was approved by the Lancisi Institutional Research Board review committee. Informed consent was obtained by all patients participating in the study.
Exercise training
A supervised exercise training program was performed at the hospital's gym, three times a week for 8 weeks, as previously described [6]. Exercise intensity was chosen at 60% of peak Vo2. Each session lasted about 1 h, beginning with stretching exercise for 15 min, followed by 40 min of cycling on electronically braked cycle ergometers (Ergometrics 800 S; Ergometrics, Roscrea, Ireland) that were calibrated weekly. Blood pressure and heart rate were measured at rest, at the end of cycling, and after a 5-min loadless recovery. Patients were asked to avoid regular exercise at home during the study period.
Characteristics of study population
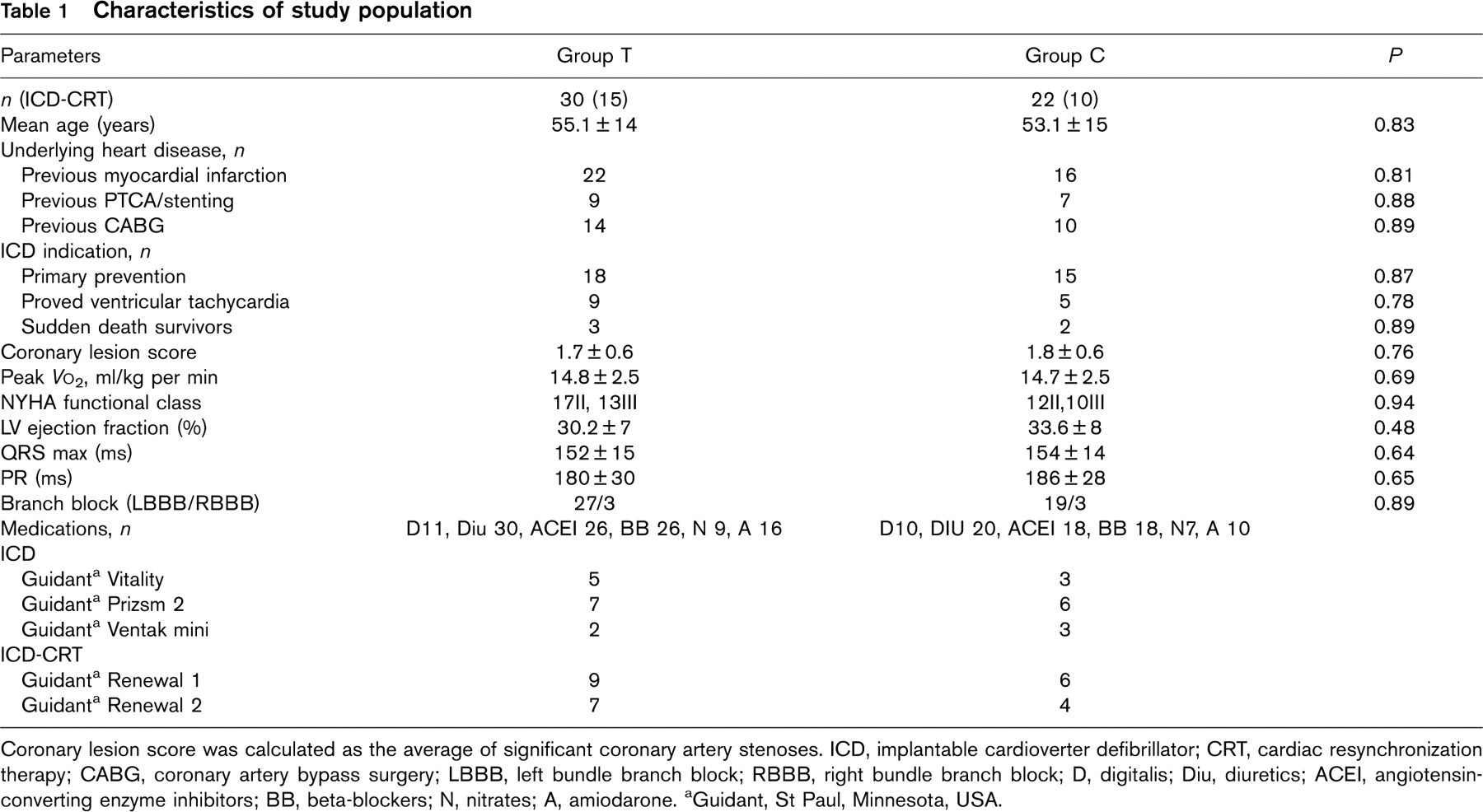
Coronary lesion score was calculated as the average of significant coronary artery stenoses. ICD, implantable cardioverter defibrillator; CRT, cardiac resynchronization therapy; CABG, coronary artery bypass surgery; LBBB, left bundle branch block; RBBB, right bundle branch block; D, digitalis; Diu, diuretics; ACEI, angiotensin-converting enzyme inhibitors; BB, beta-blockers; N, nitrates; A, amiodarone.
aGuidant, St Paul, Minnesota, USA.
Cardiopulmonary exercise testing
Cardiopulmonary exercise study was symptom-limited or until electrocardiographic signs of ischemia were noted. Breath-by-breath analysis of ventilation and gas exchange were performed using a metabolic cart (QUARK PFT; Cosmed, Pavulla, Italy). A 12-lead electrocardiogram and blood pressure were measured every minute. A Δ Vo2/Δ WR slope was automatically calculated as peak Vo2-unloaded Vo2/T-0.75 × S, where peak Vo2 is Vo2 at peak exercise, T is the time of incremental exercise; S is the slope of work rate increment in watts per minute [6]. In healthy subjects, the Δ Vo2/Δ WR slope is approximately 10 ml/min per W, and the increase in Vo2 is linear with increase in work rate until peak exercise is reached [22]. The anaerobic threshold was measured by the V-slope method [23]. Peak Vo2 was considered as the average Vo2 during the last 15 s of exercise, and was used to estimate cardiac output [24].
Brachial artery vasomotor function
Patients were evaluated in the morning in a fasting state. After 5 min of relaxation in supine position, a 7.5 MHz ultrasound probe was positioned over the dominant arm to detect good quality brachial artery images (ESAOTE Challenge, Florence, Italy). Acquisition started after fixation of the probe in a stereotaxic arm in order to avoid artifacts due to operator movements. Images were taken at baseline for 30 s, 90 s after cuff release (flow-mediated response) and 30 s after 0.3 mg of sublingual nitroglycerin (endothelium-independent response) according to recently published recommendations [25]. Flow-mediated dilatation was evaluated after release of a pediatric sphygmomanometer inflated at 240 mmHg for 4.5 min at the wrist. We considered a normal response as 7% or greater change in diameter from resting values (2 SDs of the difference between repeated measurements at our laboratory and other laboratories) [25, 26]. Images were evaluated by two independent experienced operators unaware of the clinical picture and blinded to each other's interpretation. Intraobserver and interobserver variability were assessed in 250 consecutive subjects with a variety of conditions, and results were in agreement with those of other laboratories (1.2 ± 0.8 and 1.9 ± 0.9%), respectively.
Echocardiography
M-mode, two-dimensional and Doppler echocardiography examinations were performed with an ultrasound system (ESAOTE Challenge, Florence, Italy). We used a two-dimensional mechanical sector scanner (2.5 MHz) with a Doppler flow analyzer. All studies were read twice and values were averaged for analysis. Disagreement between the two readers occurred in 8% of the cases. A consensus decision was reached in any case after reviewing the discordant studies. Intraobserver and interobserver variability from our laboratory was previously published [27].
Quality of life
The Minnesota Living with Heart Failure Questionnaire was used [28]. This method contains 21 self-administered items with three domains: the effects of heart failure on physical; emotional; and socio-economic factors.
Statistical analysis
Data were expressed as mean ± SD. Differences of continued data were evaluated by means of paired t test and differences in categorical data were assessed by the log rank test. The analysis of variance model was used and applied for comparisons between groups. Relationship between changes in peak Vo2 and changes in other variables after exercise training was assessed by linear regression analysis, and a correlation coefficient was expressed. Stepwise logistic regression was performed to determine the best predictors of QOL change. Cardiac event-free curves for the trained and untrained groups were computed using the Kaplan–Meier method. A P value under 0.05 was considered statistically significant.
Results
Hemodynamic and metabolic effects
As shown in Table 2, at 8 weeks significant improvements in peak Vo2, anaerobic threshold, minute ventilation, and work rate were observed only in the trained group. The improvement in peak Vo2 and anaerobic threshold after exercise training was more marked in patients with CRT than patients with ICD alone. These improvements were independent of the baseline NYHA functional class and type of ICD device (Table 3). No changes were observed in the control group. Interestingly, despite a larger improvement in peak Vo2, patients with CRT had no significant changes in vasomotor response as compared with trained patients without CRT (Fig. 1).
Brachial artery and endothelium-dependent vasomotor response
After 8 weeks, the trained group had significant improvements in the endothelium-dependent, vasomotor flow-mediated dilatation regardless of the type of device received, while untrained patients had no changes from baseline. Similarly, there were no changes in the endothelium-independent, flow-mediated vasodilation either in trained or untrained patients (Fig. 1b). Interestingly, there was a good correlation between changes in peak Vo2 and changes in the endothelium-dependent response regardless of whether the patient received ICD or ICD-CRT (r = 0.68 and 0.62, respectively; P < 0.0001 for both) (Fig. 2).
Doppler echocardiography
As shown in Table 4, trained patients with ICD-CRT had a significant reduction in LV end-systolic volume index and a significant increase in LV ejection fraction than trained patients without CRT as well as untrained controls. Mitral regurgitation score improved after training in ICD-CRT patients (from 2 ± 0.7 to 1.45 ± 0.5, P < 0.001). Moreover, in ICD-CRT patients, peak early filling velocity was significantly decreased (from 94 ± 15 to 62 ± 14 cm/s, P < 0.001), while peak atrial filling velocity was increased (from 52 ± 10 to 68 ± 9 cm/s, P < 0.001), so that the E/A ratio was decreased (from 1.82 ± 0.9 to 0.93 ± 1.1, P < 0.001). The isovolumic relaxation time was significantly shorter (from 65 ± 9 to 48 ± 8 ms, P = 0.005). Diastolic filling time increased significantly in both trained subgroups (ICD-CRT from 388 ± 45 to 456 ± 59 ms; ICD from 368 ± 41 to 426 ± 39 ms, P < 0.001 for both comparisons). In trained patients without CRT there were no significant changes except for diastolic filling time.
Haemodynamic and metabolic responses in the two groups
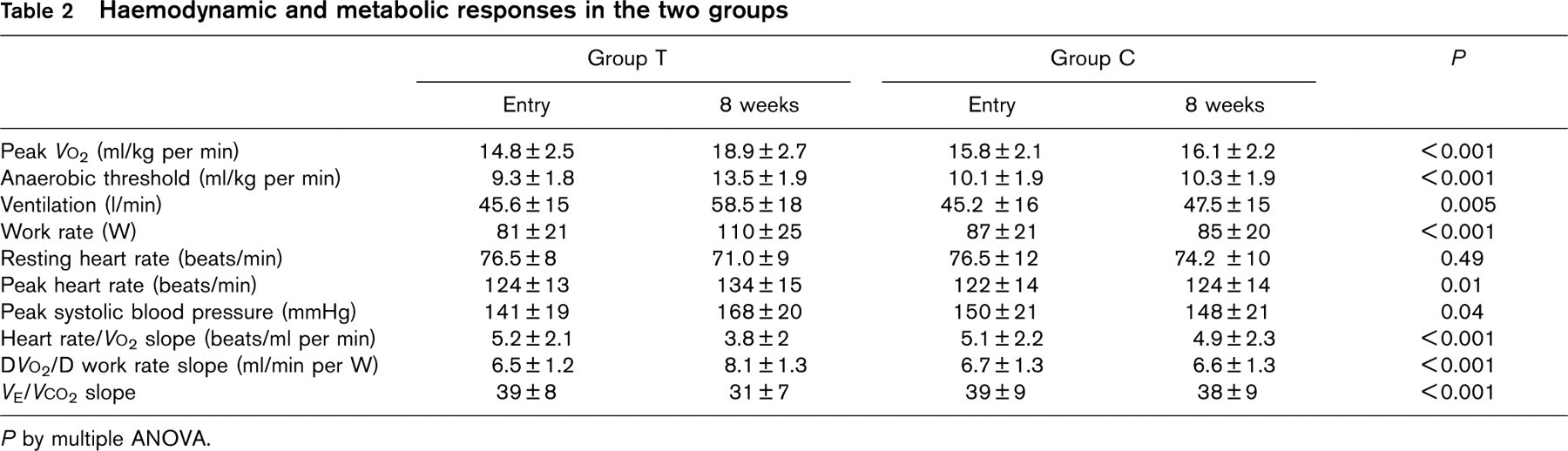
P by multiple ANOVA.
Effects of exercise training stratified by type of device and expressed as post-pre changes

P by Mann–Whitney rank sum test for trained patients with ICD versus trained patients with ICD-CRT. ICD, implantable cardioverter defibrillator; CRT, cardiac resynchronization therapy.
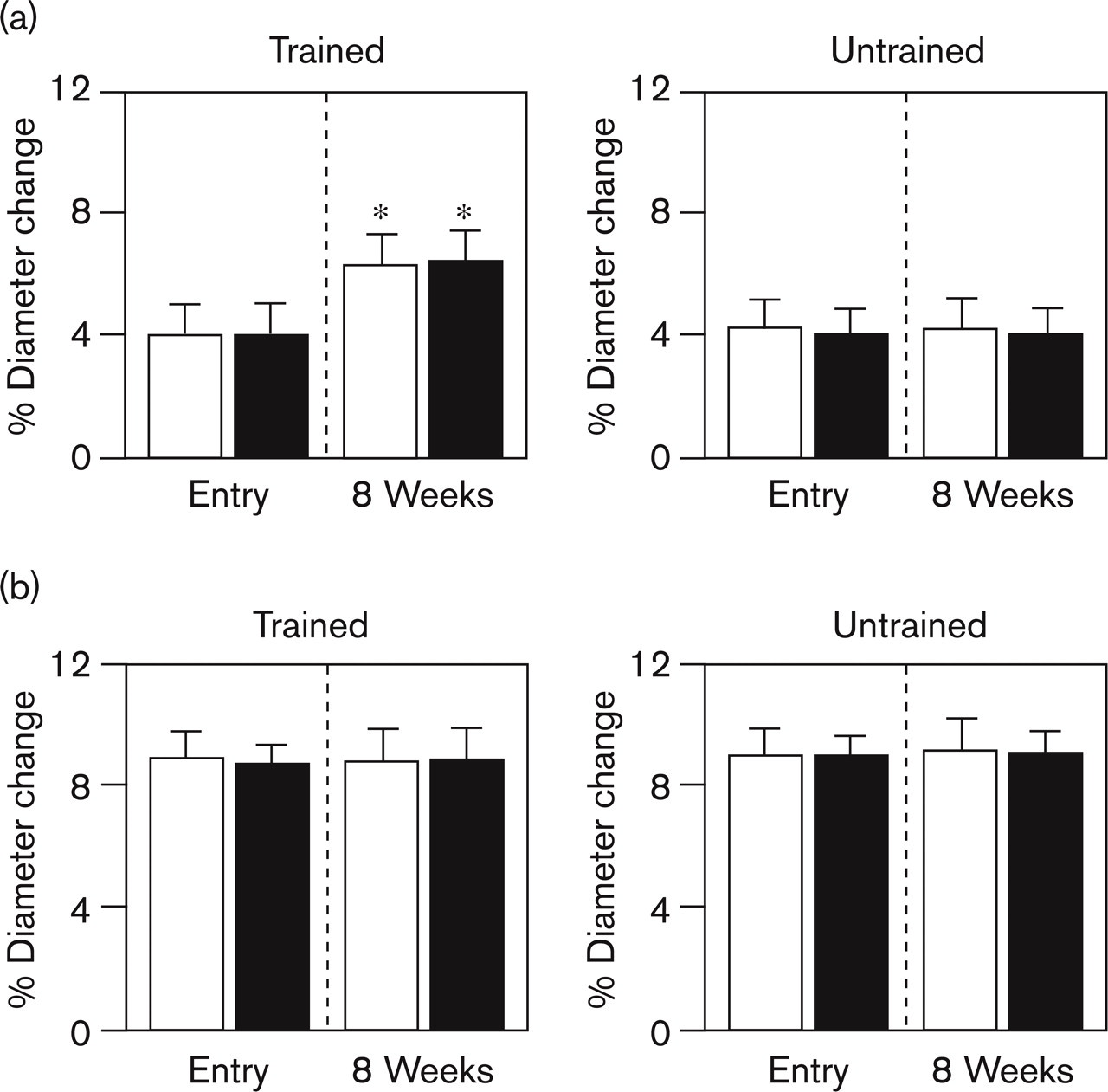
Effects of exercise training on (a) the endothelium-dependent relaxation and (b) endothelium-independent relaxation of the brachial artery in the two groups. Open squares, implantable cardioverter defibrillator (ICD); closed squares, ICD with cardiac resynchronization therapy (CRT). ∗P < 0.001 versus untrained.
Quality of life
As shown in Fig. 3, QOL sum score improved significantly only in trained patients with ICD-CRT (from 54 ± 18 to 40 ± 20; P < 0.0001 versus C and < 0.02 versus trained ICD). No changes were observed in the control patients. The three domains changed as follows: physical (trained ICD from 33 ± 8 to 28 ± 9, trained ICD-CRT from 31 ± 8 to 26 ± 7; control ICD from 34 ± 9 to 33 ± 9, control ICD + CRT from 33 ± 7 to 33 ± 7, P = NS for all comparisons); emotional (trained ICD from 10 ± 4 to 8 ± 4, trained ICD + CRT from 9 ± 4 to 6 ± 4; control ICD from 10 ± 4 to 9 ± 4, control ICD + CRT from 9 ± 4 to 10 ± 4, P = NS for all comparisons); socio-economic (trained ICD from 14 ± 6 to 13 ± 6, trained ICD + CRT from 14 ± 7 to 8 ± 4; control ICD from 13 ± 6 to 13 ± 6, control ICD + CRT from 13 ± 6 to 13 ± 6, P = NS for all comparisons). QOL improvement was correlated with peak Vo2 improvement (r = 0.72, P < 0.001). Logistic regression showed that the strongest predictor of QOL improvement was the change in end-systolic volume index (r = −0.61, P < 0.001).
Follow-up
After 18 months of follow-up, the untrained patients had eight events of sustained ventricular tachycardia regardless of the type of device received, prompting the ICD to discharge eight shocks (log rank 8.56, P < 0.001). Patients were admitted to hospital, and there were no cardiac deaths (Fig. 4). The trained patients had no ICD-related shocks during the follow-up. The hospital readmission rate was 67% in trained patients and 45.4% in untrained controls (P < 0.0001). No difference was observed between patients with ICD and patients with ICD-CRT.
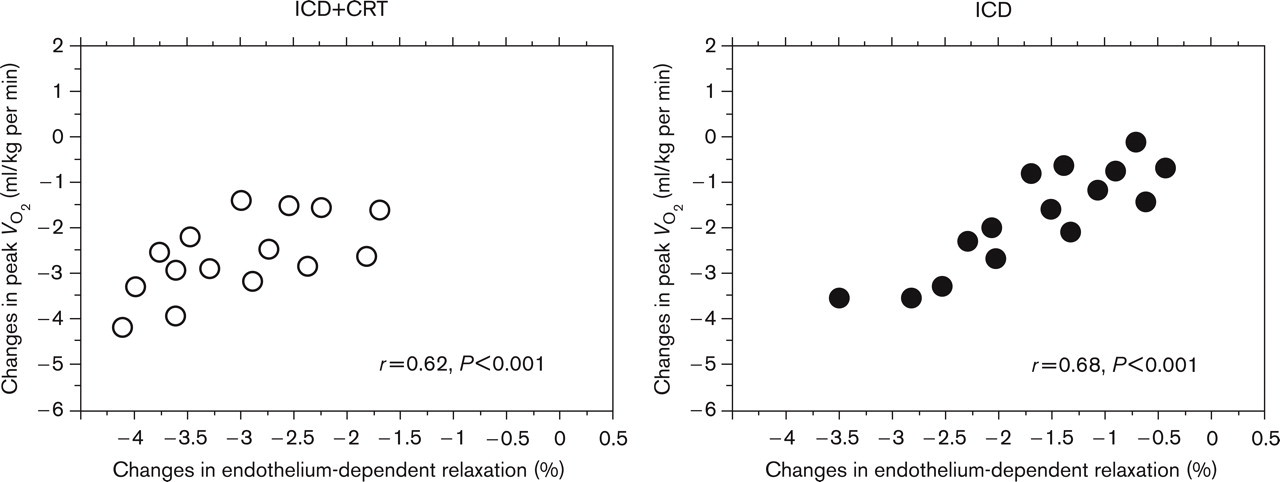
Relation between pre–post training changes in peak Vo2 and endothelium-dependent relaxation in patients with implantable cardioverter defibrillator (ICD; filled circles) and ICD with cardiac resynchronization therapy (CRT; open circles).
Echocardiographic and cardiopulmonary parameters in trained and controls on study entry and at 8 weeks
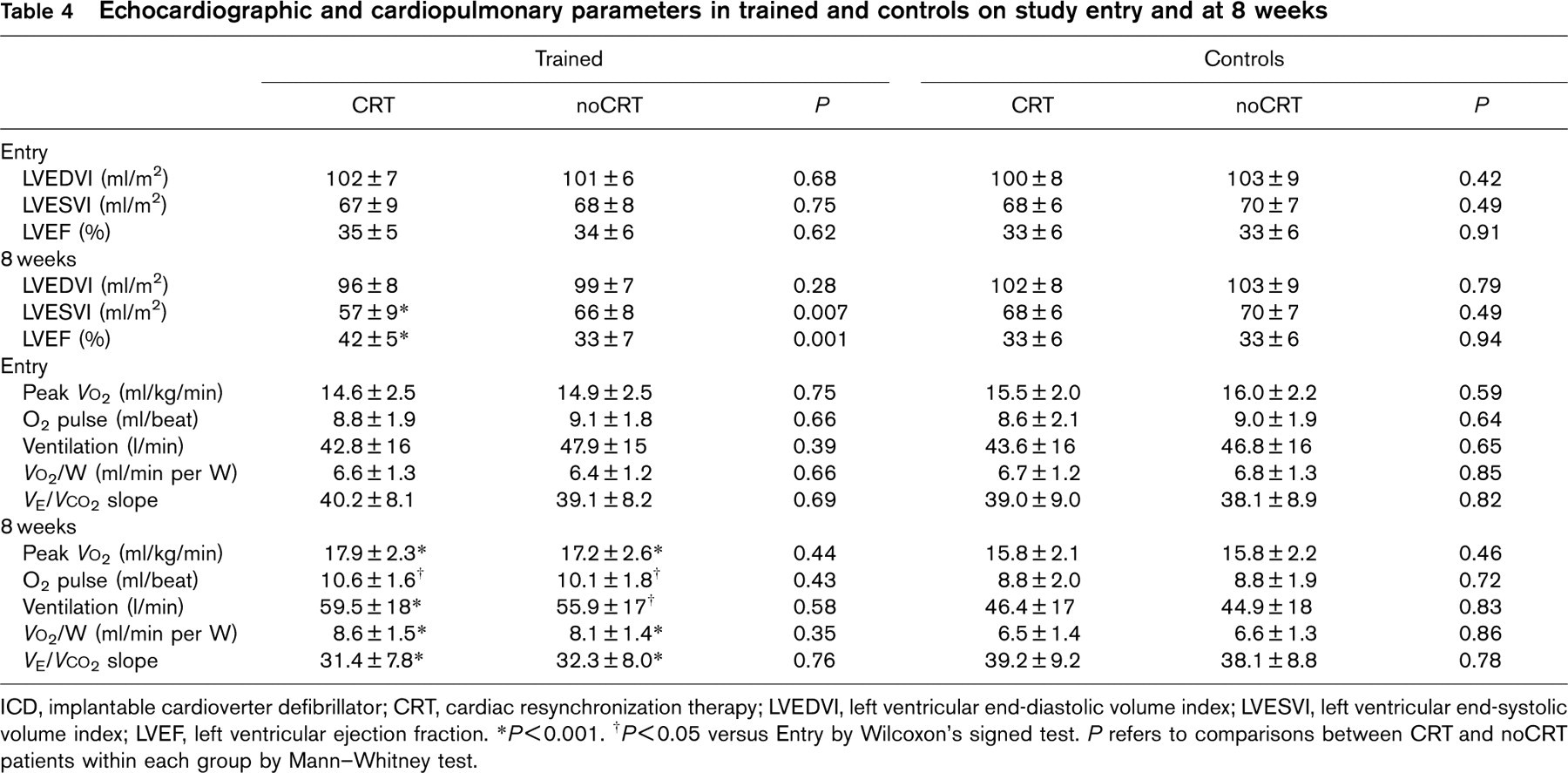
ICD, implantable cardioverter defibrillator; CRT, cardiac resynchronization therapy; LVEDVI, left ventricular end-diastolic volume index; LVESVI, left ventricular end-systolic volume index; LVEF, left ventricular ejection fraction.
∗P < 0.001.
† P < 0.05 versus Entry by Wilcoxon's signed test.
P refers to comparisons between CRT and noCRT patients within each group by Mann–Whitney test.
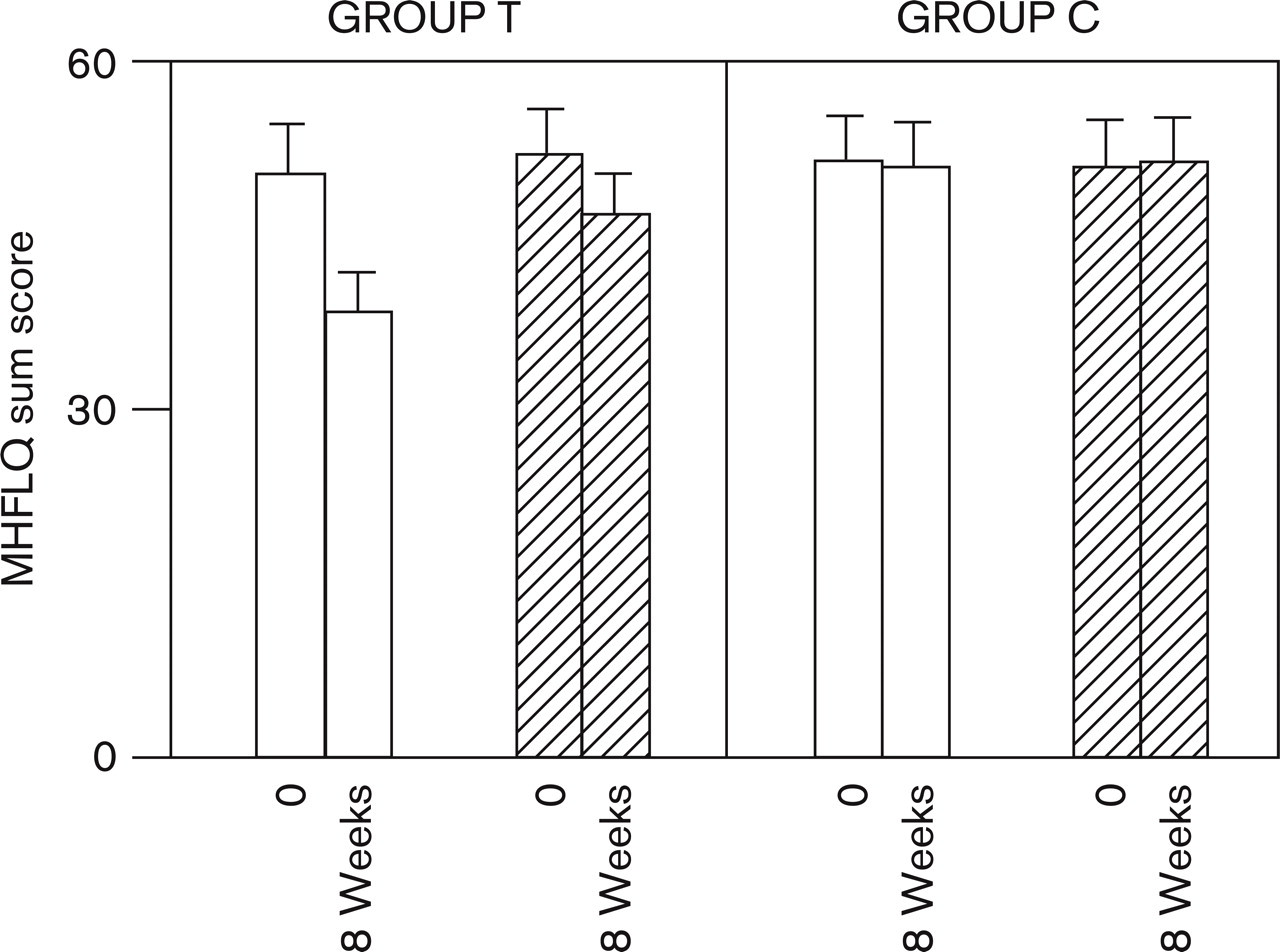
Effects of exercise training on the Minnesota Quality of Life sum score in trained and control patients as related to type of device. Open squares, implantable cardioverter defibrillator (ICD) with cardiac resynchronization therapy (CRT); dashed squares, ICD.
Discussion
This is the first prospective study to demonstrate that moderate aerobic exercise training improves functional capacity, endothelium-dependent vasodilatation, and QOL in CHF patients after ICD implantation. The hospital readmission rate was also significantly lower in trained patients. Improvement in functional capacity and QOL was more pronounced in trained patients who received ICD with CRT therapy. Vasomotor response, however, was similar in trained patients with ICD and ICD-CRT. Finally, trained patients had no adverse events during the exercise sessions or at follow-up (r = −0.61).
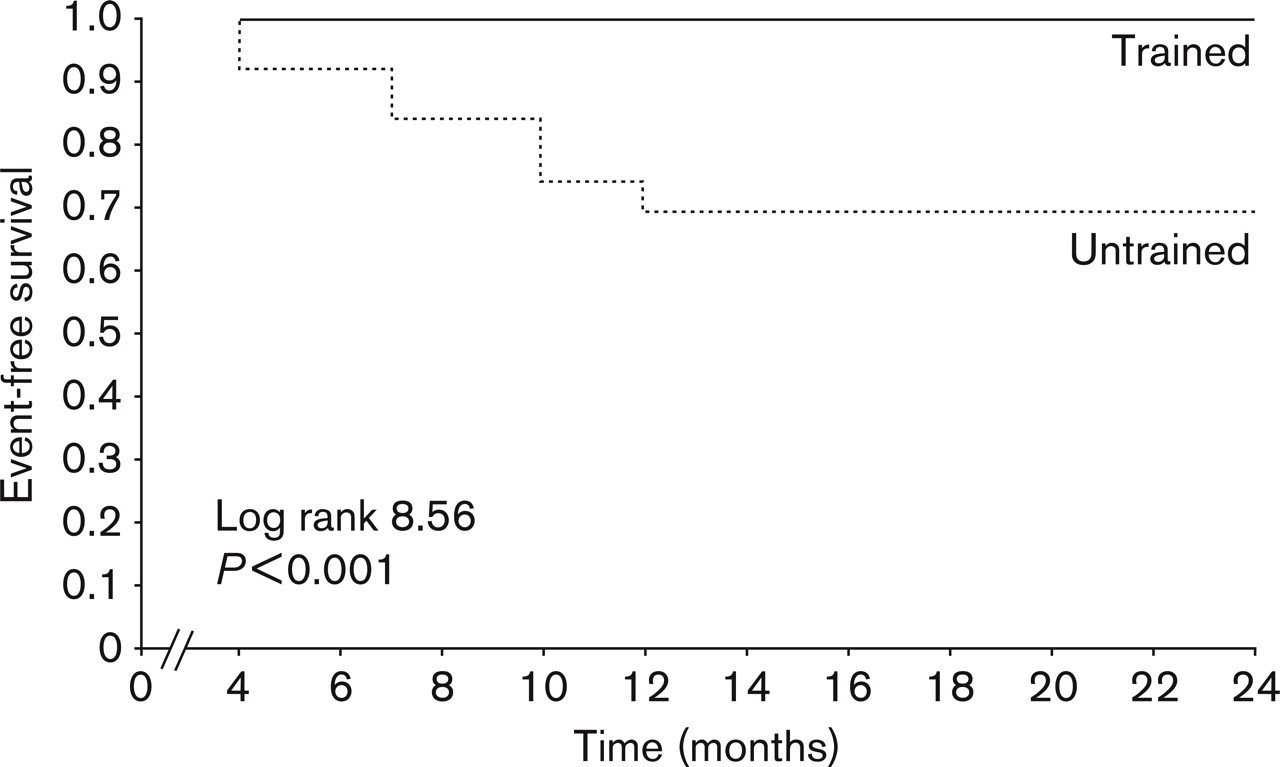
Event-free survival in trained (filled line) and untrained (dashed line) patients.
In the present study, the degree of improvement in functional capacity after exercise training was similar to the average increase in peak Vo2, described in previous randomized trials on CHF patients without ICD [1–6] and it was also in agreement with the results of two recent studies involving 101 and 16 CHF patients with ICD, who underwent a comprehensive cardiac rehabilitation program lasting 3–12 weeks [19, 20]. In both studies, however, neither follow-up nor QOL were evaluated. Moreover, gas exchange and ventilation were not measured and functional capacity was expressed as exercise time or watts. Despite these methodological differences, the amount of improvement in functional capacity was similar to that observed in the present study, suggesting that exercise conditioning represents the core component of a comprehensive cardiac rehabilitation program. In another more recent study, the effect of exercise training on peak Vo2 and O2 pulse was smaller than that observed in control patients without ICD [21]. The study was not randomized, however, and patients with CRT were not included.
In the present study, not only peak Vo2, but also the anaerobic threshold were both more markedly improved after exercise training in patients with ICD-CRT. Other prognostic markers were also improved. The V E/Vco2 slope was flatter, suggesting a greater ventilatory efficiency, while Vo2/W was steeper, indicating less cardio-circulatory impairment (Table 2). Exercise training may exert positive effects in combination with resynchronization therapy. First, exercise training increases the ventricular fibrillation threshold through improved sympatho-vagal autonomic balance, reducing chronotropic incompetence and increasing cardiac output at submaximal and maximal exercise intensities [2]. Second, exercise training improves the aerobic capacity of skeletal muscles by increasing peripheral blood flow and muscle aerobic machinery, and by inducing morphological and functional adaptation [3, 4]. As a result, plasma lactate levels are decreased and metabolic acidosis is also reduced. Third, exercise training improves LV diastolic filling and reduces chronotropic incompetence, as biventricular pacing does [29]. Moreover, exercise improves the endothelium-dependent relaxation of coronary as well as peripheral arteries, with potential improvement in vascular reserve and myocardial perfusion and function [30, 31]. Thus, some central adaptations induced by exercise conditioning are similar to the effects of CRT, and a combination of the two seems to exert an additive effect on cardiac function. Exercise training, however, promotes circulatory and skeletal muscle adaptations that CRT alone cannot induce.
Endothelium dependent vasomotor response
Only trained patients displayed a significant improvement in the endothelium-dependent vasomotor response of the brachial artery. Endothelial function improved to the same extent after exercise training regardless of the type of device received or NYHA functional class, suggesting that exercise training is primarily responsible for the improvement in vasomotor response. Exercise-induced shear stress stimulates endothelium nitric oxide synthase and the subsequent generation of nitric oxide, together with other endothelial vasodilating substances, such as bradykinin and prostacyclin, appears to account for the improvement in vasomotor response. It is of interest that a good correlation was found between changes in peak Vo2 and changes in the endothelium-dependent vasodilatation, underlying the importance of the endothelium in the exercise-induced functional improvement. The results of the present study confirm that leg exercise induces a generalized improvement in endothelial function. This effect seems to be non-site specific and can be measured in untrained body segments, such as, the brachial artery. From the results of the present study, however, arterial vasomotor response seems to play a minor role in patients with CRT, since the improvement in vasomotor response was similar in trained patients regardless of the presence of CRT. Moreover, endothelium-dependent relaxation was unrelated to QOL, since its response to training was similar to functional capacity. This was confirmed by univariate analysis, showing that the strongest predictor of QOL improvement was the reduction in end-systolic volume index (r = 0.61, P < 0.001).
Outcome
Another important point is that exercise training performed according to standardized modalities is safe even in patients with CHF who suffered life-threating arrhythmias before ICD implantation. As a matter of fact, the trained group recorded no deaths and no evidence of any complex ventricular arrhythmias during the training sessions and follow-up. Both trained subgroups, with either ICD or ICD-CRT, were free of secondary adverse events. On the other hand, the untrained patients with ICD or ICD-CRT developed complex ventricular arrhythmias, which resulted in eight shocks, requiring hospital readmissions. Exercise training has been shown to reduce epinephrine and norepinephrine blood levels in CHF patients [4], and also to improve baroreflex sensitivity [4].
Thus, the absence of ventricular tachycardia in the trained group may be explained by reduced neurohormonal activation, and, possibly, also by improved myocardial perfusion [32]. Moreover, exercise training stimulates coronary collateralization in patients with ischemic cardiomyopathy, and enhances also the contractile response of dysfunctional myocardium to low-dose dobutamine [31].
Limitations
We used a moderate aerobic exercise training protocol in a supervised environment. We cannot extrapolate the beneficial effects observed in this study after training to home physical activities such as snow shoveling, carrying heavy weights or other unsupervised activities. Anyway, a training effect should allow a more active lifestyle with less cardiocirculatory and metabolic requirements. The study is small with relatively short follow-up. It was, however, blinded to the interpretation of the results.
Conclusion
Moderate aerobic exercise training improves functional capacity, endothelium-dependent vasorelaxation and quality of life in NYHA class II and III CHF patients after ICD implantation. Improvement in functional capacity and quality of life was more pronounced in trained patients with ICD-CRT, while vasomotor response was similarly improved in trained patients with both ICD and ICD-CRT. Trained patients had no ICD-related shocks during the follow-up of 24 months, while untrained patients had eight shocks requiring hospital admissions regardless of the presence of CRT therapy. Hospital readmission rate was also significantly lower in trained patients without differences between ICD and ICD-CRT, suggesting a reduction of costs.