
Abstract
Background
Lifestyle and pharmacological interventions can delay the progression of impaired glucose tolerance (IGT) to type 2 diabetes (T2DM), and there is growing evidence that earlier detection of T2DM and intensified risk factor management may result in improved cardiovascular morbidity and mortality. We studied the prevalence of impaired glucose metabolism (T2DM, IGT and impaired fasting glucose; IFG) in patients referred to cardiac rehabilitation, and further studied whether we could identify groups in which an oral glucose tolerance test (OGTT) need not be performed.
Methods
As part of a cardiac rehabilitation trial, 201 patients participated. Patients without a diagnosis of T2DM (N = 159) underwent an OGTT 3 months after inclusion.
Results
Forty-two patients (21%) had known T2DM at enrolment. Based on the OGTT, 26 patients (13%) had unrecognized T2DM, 36 (18%) had IGT and 19 (9%) were diagnosed with isolated IFG according to the World Health Organization definition. Using fasting plasma glucose alone, 19% of the patients with unrecognized T2DM and two-thirds of patients with IGT would be misclassified. Using IFG as a means to detect IGT showed a sensitivity of only 33% and a positive predictive value of 39%.
Conclusion
More than 60% of the patients (123/201) referred to cardiac rehabilitation had impaired glucose metabolism and 18% of the screened patients (29/159) would be misclassified if an OGTT was omitted. IFG and IGT did not identify the same patients or the same cardiovascular risk profile. An OGTT test should therefore be considered a constituent part of routine care management in cardiac rehabilitation settings.
Keywords
Introduction
Patients with type 2 diabetes (T2DM) and cardiovascular disease have a particularly high risk of further cardiovascular complications, and therefore require specific attention when diagnosed [1, 2]. Impaired glucose tolerance (IGT) also needs to be detected as many of these patients develop T2DM. T2DM and IGT have a high prevalence in patients with ischaemic heart disease and congestive heart failure, but are often unrecognized [3]. In patients with acute myocardial infarction the prevalence of unrecognized T2DM and IGT based on an oral glucose tolerance test (OGTT) 3 months after discharge is 25 and 40%. In the same patients the admission haemoglobin A1c (HbA1C) value and fasting glucose during admission were independent predictors of later impaired glucose metabolism (IGM). The prevalence of unrecognized T2DM among high-risk patients scheduled for coronary angiography is also high, and in half of these patients, T2DM was only detectable by the use of an OGTT [4]. The prevalence of known T2DM mainly in ischaemic patients attending cardiac rehabilitation has been estimated to be 20–30% [5], and recent data from the European cohort studies examining individuals eligible for cardiac rehabilitation are supportive of this high rate [6]. Data on unrecognized T2DM, IGT and IFG among patients who attend cardiac rehabilitation programmes are still lacking, and the advantage of the systematic use of an OGTT compared with fasting glucose values used alone also needs to be determined in the rehabilitation setting.
The purpose of the present study was: (i) to examine the prevalence of IGM in terms of known and unrecognized T2DM, IGT, and IFG in accordance with modern diagnostic criteria in a large group of patients referred to hospital-based cardiac rehabilitation; (ii) to look at the concordance between IFG and IGT to determine the value of the systematic use of an OGTT; (iii) to clarify differences in cardiovascular risk profile in these groups; and (iv) to determine possible predictors of IGT and T2DM.
Methods
The DANSUK study was conducted during the last year of inclusion into a randomized study of the value of a comprehensive cardiac rehabilitation clinic [7]. Patients admitted to the Department of Cardiology at Bispebjerg University Hospital in Copenhagen, Denmark, for ischaemic heart disease, congestive heart failure, or cardiovascular high-risk patients with at least three classic cardiovascular risk factors were screened consecutively and invited into the study from March 2002 to March 2003. There was no age limit for participation, but only patients living at home were eligible. Other exclusion criteria were severe non-cardiovascular disease, New York Heart Association stage IV, unstable patients awaiting revascularization, severe abuse of alcohol and sedatives, dementia, and not speaking or understanding the Danish language [7]. Of 1755 consecutively screened patients, 473 were eligible, and 201 patients (42%) were finally randomly assigned to receive either usual care according to international guidelines or comprehensive cardiac rehabilitation. The majority of the non-consenters thought that the enrolment and assessment visits were too comprehensive. The study was in accordance with the Declaration of Helsinki and was approved by the regional ethics committee of Copenhagen (j.no.(KF) 11–121/01). All patients provided written and oral informed consent. After 3 months of follow-up, patients without T2DM (N = 159) and regardless of their fasting plasma glucose values were invited to an OGTT (Fig. 1). The patients were asked to fast for 10 h and to restrain from smoking, exercise, or other unusual activity before the tests. Fasting plasma glucose was measured as a minimum at baseline and after 3 months. Treatment goals and medical therapy were adjusted and intensified according to the metabolic group assignment.
Measurements
Plasma glucose was determined by the hexokinase/G6P-DH method. HbA1c, plasma insulin, and C-peptide were measured with commercial kits; normal range: HbA1c 4.1–6.4%, plasma insulin 5–69 pmol/l and C-peptide 200–700 pmol/l [8]. Serum cholesterol and high-density lipoprotein (HDL)-cholesterol were analysed by chromatography and triglycerides by colorimetry. Very low-density lipoprotein (VLDL) and low-density lipoprotein (LDL)-cholesterol was calculated using the Friedewald's Equation. Urinary albumin excretion was measured using the albumin-creatinine ratio in a first morning urine sample and the OGTT was a standard 75-g test, with measurements of blood glucose on capillary blood at baseline and after 2 h. Insulin resistance at baseline was estimated by the homeostasis model assessment of insulin resistance (HOMA-IR) as fasting insulin (mU/ml) × fasting plasma glucose (mmol/l)/22.5. Blood pressure estimates were collected as the mean of a 24-h measurement.
Definitions
Diabetes mellitus was considered present if a physician had informed the patients of this diagnosis or if the patient was on prescribed treatment (diet, oral hypoglycaemic agents, or insulin). Patients without a previous diagnosis of T2DM were classified according to the 1997 World Health Organization (WHO) definition [9] and compared with the American Diabetes Association (ADA) criteria proposed in 2003 [10]. Patients were classified as having systemic hypertension if they received medical therapy for hypertension or if they had two resting blood pressure measurements during hospital admission above 140/90 mmHg. Likewise, patients were diagnosed with dyslipidemia if they were treated with lipid-lowering drugs or if a lipid profile taken at admission had shown values of total cholesterol above 5.0 mmol/l, HDL-cholesterol less than 1.0 mmol/l, or triglycerides greater than 1.5 mmol/l. Hyperinsulinemia was defined as the upper quartile of fasting plasma values and insulin resistance (HOMA-IR) by HOMA levels both determined in Danish population-based studies (cut-off value of hyperinsulinemia: 51 pmol/l and HOMA: 1.76) [11, 12]. Myocardial infarction and congestive heart failure were defined according to the criteria recommended by the European Society of Cardiology [13, 14].
Statistical analysis
The SAS statistical package (version 8.2; SAS Institute Inc., Cary, North Carolina, USA) was used for all statistical analyses and a two-tailed P value of less than 0.05 was considered significant. The difference between several study groups was tested by analysis of variance. Multivariable logistic regression was used to determine independent predictors of impaired glucose metabolism. The models were selected using baseline variables: age, sex, body mass index, waist circumference, a history of systemic hypertension and hypercholesterolemia, hyperinsulinemia, HOMA–IR, microalbuminuria, exercise capacity, HbA1c and fasting plasma glucose value. A forward and backward selection procedure was used to select most predictive variables. In all cases forward and backward selection resulted in the same variables being chosen. Two models were finally tested. Model 1 included the variables: body mass index, waist circumference, a history of systemic hypertension and hypercholesterolemia, HbA1c, fasting plasma glucose, hyperinsulinemia, HOMA–IR, microalbuminuria. In model 2, variables closely related to IGM, i.e. HbA1c, fasting plasma glucose, HOMA–IR and hyperinsulinemia were omitted. Covariates were calculated for a 1 SD unit increase of continuous variables and the odds ratio for HbA1c was in terms of a 1% increase over the normal maximal value of 6.4%.
Results
Patient characteristics and classification
We included 201 patients, 60 women and 141 men, with a mean age of 62.5 ± 11.0 years. Of the 201 patients in the DANSUK study, 42 (21%) had known T2DM at inclusion. The remaining 159 patients underwent an OGTT. At baseline there was no significant difference in the use of cardiovascular medication in the patients with and without known T2DM. Patients without T2DM at baseline were divided into four groups based on the result of fasting plasma glucose values and the OGTT (Fig. 1). Twenty-six patients (13%) were diagnosed with previously unrecognized T2DM, 36 patients (18%) had IGT, whereas 19 patients (9%) fulfilled the criteria of having isolated IFG according to the WHO definition. One-third of the patients with IGTalso had IFG. The prevalence of known T2DM among the non-consenters was the same as in the population that participated. Table 1 shows baseline characteristics of the patients subgrouped by the result of the OGTT and fasting plasma glucose values in accordance with the WHO definition.
The value of an oral glucose tolerance test
When glucometabolic classification was based on fasting plasma glucose values alone as defined by the WHO, the proportion of patients with IGM (57/159, 36%) was substantially lower than when the classification was also based on an OGTT (81/159, 51%; Fig. 2). Using the definition recommended by the ADA, 46% (73/159) would be classified as having IFG causing a much higher proportion of patients with IGM (94/159, 59%). In 19% of patients with newly diagnosed T2DM, the disease was detectable only by the use of an OGTT, although all patients had fasting plasma glucose values between 6.1 and 6.9 mmol/l. Among the patients with IFG according to the ADA criteria, only 27% (20/73) would also have IGT (IFG/IGT). Lowering the level of normal glucose tolerance (NGT) to below 5.6 mmol/l still leaves 44% (16/36) of the patients with IGT misclassified.
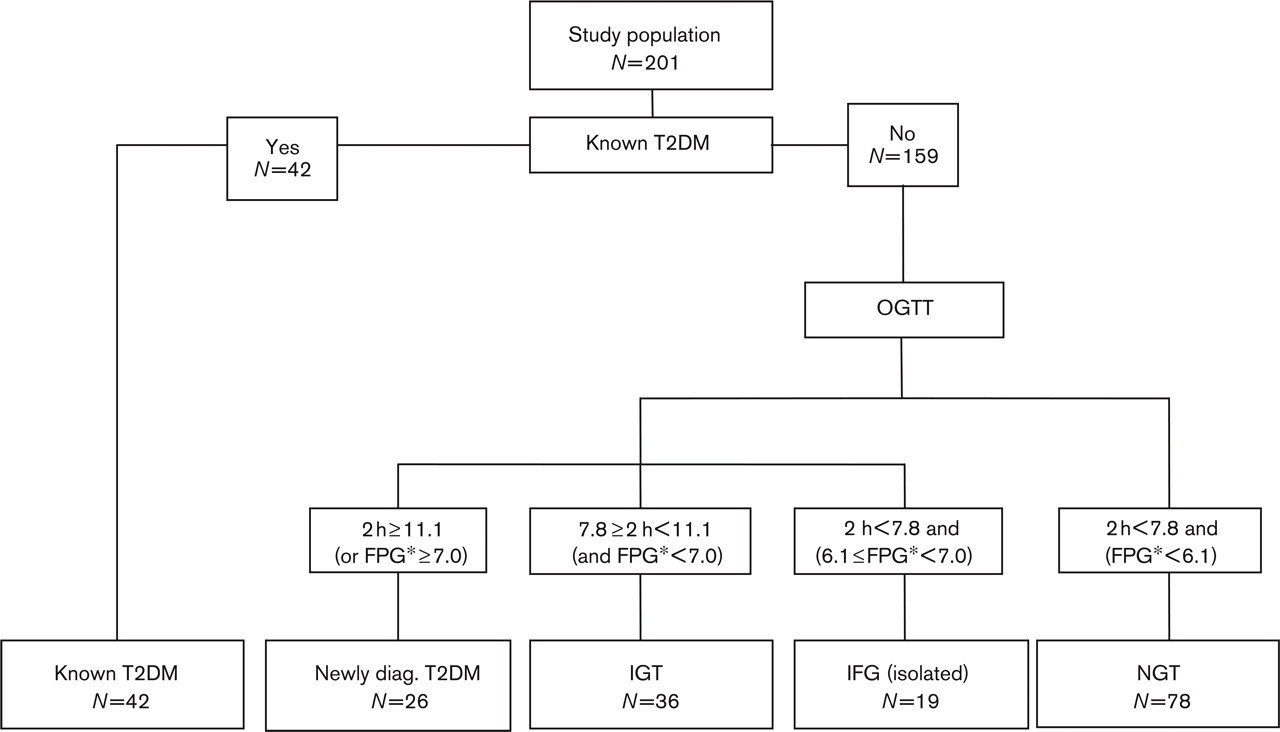
Study flow chart of the DANSUK study.
Baseline characteristics in patients subgrouped by outcome of an oral glucose tolerance test
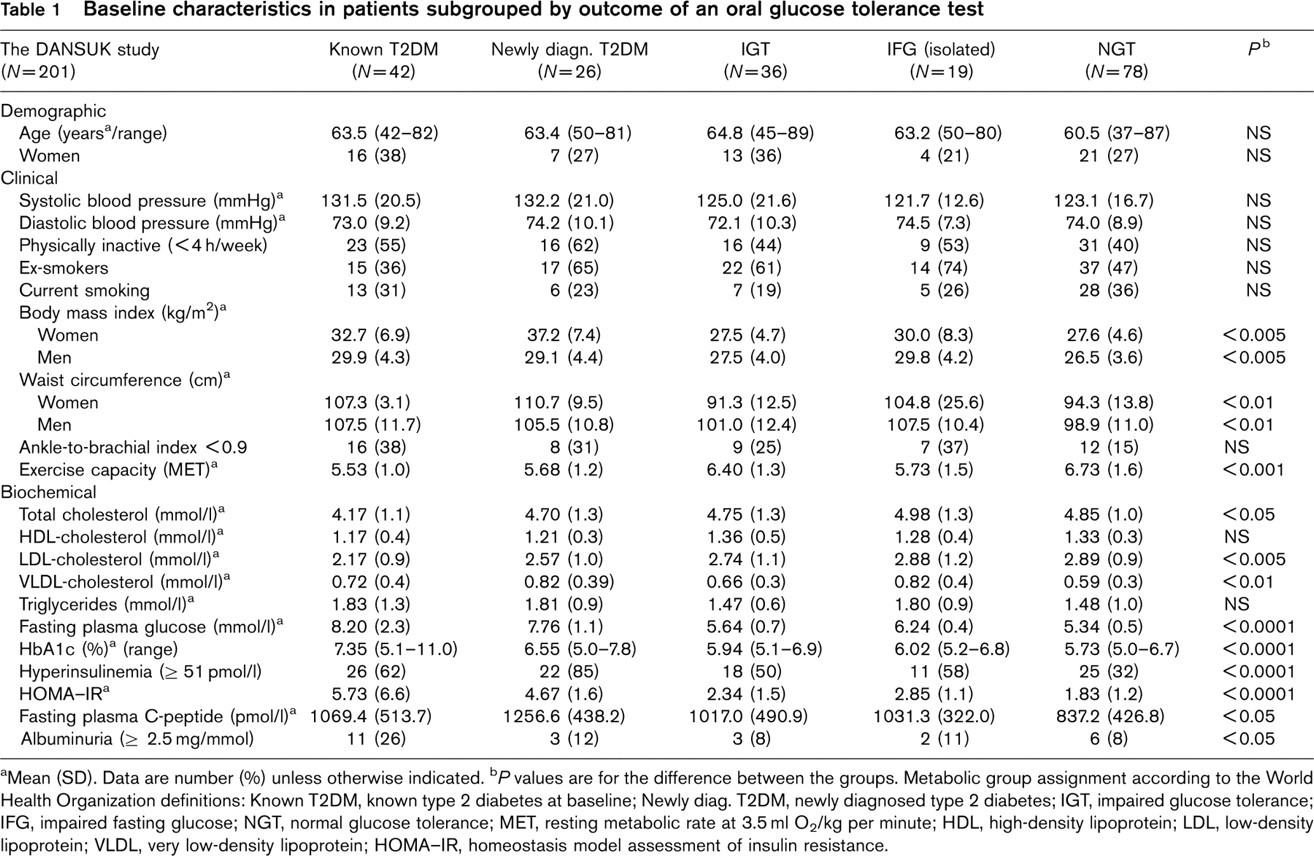
aMean (SD). Data are number (%) unless otherwise indicated.
b P values are for the difference between the groups. Metabolic group assignment according to the World Health Organization definitions: Known T2DM, known type 2 diabetes at baseline; Newly diag. T2DM, newly diagnosed type 2 diabetes; IGT, impaired glucose tolerance; IFG, impaired fasting glucose; NGT, normal glucose tolerance; MET, resting metabolic rate at 3.5 ml O2/kg per minute; HDL, high-density lipoprotein; LDL, low-density lipoprotein; VLDL, very low-density lipoprotein; HOMA-IR, homeostasis model assessment of insulin resistance.
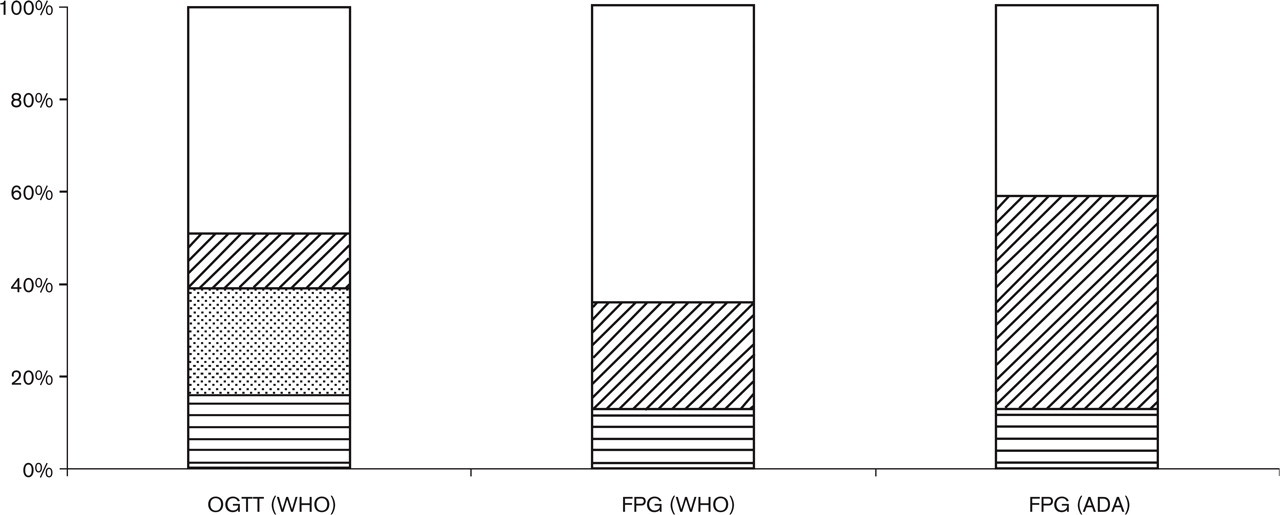
Comparison of glucometabolic characterization by means of the performance of an oral glucose tolerance test (OGTT) or by two independently taken fasting plasma glucose (FPG) values according to the World Health Organization (WHO) definitions and the American Diabetes Association (ADA) criteria in patients without a previously diagnosed glucometabolic abnormality (N = 159).
In patients with newly diagnosed T2DM, 46% (12/26) had an HbA1c above 6.5%, and in more than half of these, HbA1c was above 7.0%. Besides adjusting some of the treatment goals, the diagnosis of T2DM also resulted in an increased use of angiotensin-converting enzyme inhibitors/angiotensin receptor II antagonists by one-third (P < 0.01) and 25% of these patients were treated with metformin at follow-up.
Predictors of impaired glucose metabolism
Using IFG as a means to detect IGT showed a low sensitivity and a relatively high specificity when WHO criteria were used (Table 2). Using the ADA criteria, the sensitivity increased at the expense of a decreased specificity. With a prevalence of IGT in the DANSUK study of 18%, the positive predictive value of fasting plasma glucose alone was low regardless of the chosen diagnostic criteria. An overlap in the HbA1c values between the five groups was observed (Table 1). The predictive power of HbA1c for the diagnosis of IGM was tested in patients with fasting plasma glucose concentrations between 5.6 and 6.9 mmol/l. HbA1c of 6.4% or greater (upper reference range) revealed a sensitivity of 16% and a negative predictive value of 41%. Multivariate logistic regression analyses demonstrated that systemic hypertension [odds ratio (OR) 2.9, P < 0.05] was significantly correlated to IGT in both models 1 and 2. Fasting plasma glucose (OR 4.1, P < 0.0001) and HbA1c (OR 3.5, P < 0.05) in model 1 and age (OR 1.1, P < 0.05), waist circumference (OR 1.2, P < 0.0001), systemic hypertension (OR 2.9, P < 0.01) and low exercise capacity (OR 0.6, P < 0.0001) in model 2 were independently correlated with T2DM.
Comparison between impaired fasting glucose according to the World Health Organization (WHO) definitions and the American Diabetes Association (ADA) criteria and impaired glucose tolerance: WHO/ADA
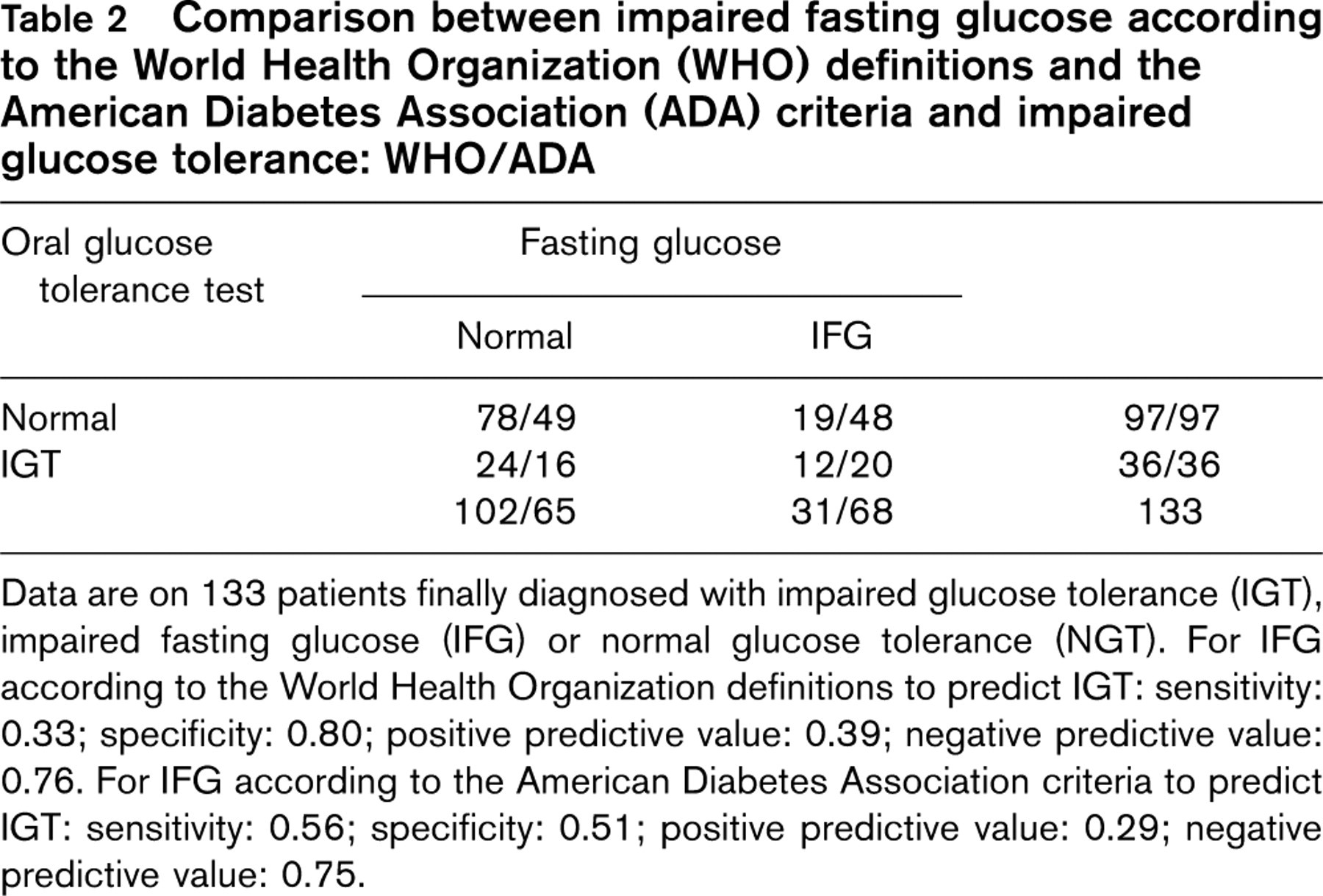
Data are on 133 patients finally diagnosed with impaired glucose tolerance (IGT), impaired fasting glucose (IFG) or normal glucose tolerance (NGT). For IFG according to the World Health Organization definitions to predict IGT: sensitivity: 0.33; specificity: 0.80; positive predictive value: 0.39; negative predictive value: 0.76. For IFG according to the American Diabetes Association criteria to predict IGT: sensitivity: 0.56; specificity: 0.51; positive predictive value: 0.29; negative predictive value: 0.75.
Glycaemic threshold and cardiovascular risk profile
The effect of lowering the diagnostic threshold for IFG on the cardiovascular risk profile was investigated comparing the risk profile in patients with IFG according to the WHO definition (fasting plasma glucose 6.1–6.9 mmol/l) with those additional cases of IFG identified by the ADA criteria (fasting plasma glucose 5.6–6.0 mmol/l). The additional patients identified with IFG according to the ADA criteria had a more favourable cardiovascular risk profile than the patients having IFG according to the WHO definition. Besides a lesser degree of insulin resistance (P < 0.05), lower HbA1c level (P < 0.05) and lower diastolic blood pressure (P < 0.05), fewer patients had an ankle-brachial pressure index below 0.9 (P < 0.05) in the additional IFG patients. When the cardiovascular risk profile of the additional patients with IFG according to the ADA criteria (fasting plasma glucose 5.6–6.0 mmol/l) were compared with the patients with NGT (fasting plasma glucose < 5.6 mmol/l), the additional patients identified with IFG had a poorer cardiovascular risk profile with significantly higher body mass index (P < 0.05), greater waist circumference (P < 0.05), higher HbA1c level (P < 0.05) and higher HOMA–IR (P < 0.001). Sixteen of the IGT patients were identified as having NGT by the ADA criteria and if the cardiovascular risk profile of these patients were compared with the patients with IGT having fasting hyperglycaemia according to the ADA criteria, the patients with NGT according to the ADA criteria also had a more favourable cardiovascular risk profile, with a lower body mass index (P < 0.05) and waist circumference (P < 0.05), a lower degree of insulin resistance (P < 0.01) and the patients had suffered fewer myocardial infarctions (P < 0.05).
Discussion
The findings in the present study demonstrate a high prevalence of IGM in a broad spectrum of patients eligible for comprehensive cardiac rehabilitation. Depending on the performance of an OGTT and the chosen diagnostic criteria, 49–68% of the patients in the DANSUK study had IGM. The prevalence of IGM in the DANSUK study is comparable with the prevalence of IGM in the European cohort studies, although the prevalence of known T2DM in the DANSUK study was somewhat less than the 30% found in the elective consultation group in the European Heart Survey [6]. The prevalence of IFG was higher in the DANSUK study, probably reflecting a less diseased population enrolled in the DANSUK study, in which 32% of patients were stratified as high-risk patients without present signs of ischaemic heart disease or congestive heart failure. Also the prevalence of unrecognized T2DM and IGT was lower in the DANSUK study when compared with trials exclusively investigating ischaemic patients in which the prevalence of IGT constitutes more than one-third of the screened population [3]. In the DANSUK study, 18% (29/159) of the patients would have been incorrectly classified using only fasting plasma glucose concentrations according to the WHO definition.
Since the current criteria of IGM were defined in 1997 [15], studies have compared the concordance between populations diagnosed with IGM based on the fasting glucose values or additionally on an OGTT [3, 16, 17]. The two diagnostic criteria not only differed in classifying the glucometabolic disorders but also in predicting cardiovascular morbidity and mortality [18–20]. In the DANSUK study, we performed an OGTT in all patients without T2DM, as classification based on fasting plasma glucose concentrations alone have been shown to leave 30% of all patients with T2DM undiagnosed and to misclassify individuals with a poor prognosis [19]. Lowering of the threshold for normal fasting plasma glucose from 6.0 to 5.5 mmol/l increased the prevalence of IFG in the screened DANSUK population from 23% (36/159) to 46% (73/159) but only eight more patients with IGT were thereby correctly classified. Among patients classified as IFG by the ADA criteria, the proportion of patients who also had IGT decreased to 29% compared with 39% when using the WHO definition, thus lowering the positive predictive value of IFG for predicting IGT (Table 2).
One-fifth of the patients with unrecognized T2DM would remain undiagnosed when using the fasting glucose criteria alone. This is close to the findings in the population-based Diabetes Epidemiology: Collaborative Analysis of Diagnostic Criteria in Europe (DECODE) study, in which it was concluded that a misclassification would be pronounced especially in the older and the lean patients, if the diagnosis was based on fasting glucose values alone [19]. Identification of patients with IGT is important from a preventive perspective, as this is a group in which lifestyle intervention strategies have proved especially effective in preventing or delaying progression to T2DM [21]. Besides being a condition that may progress to T2DM, IGT is also a risk factor for cardiovascular disease [19]. Less is known about the incidence of diabetes and the risk of cardiovascular diseases in patients with isolated IFG according to the WHO definition or the newly revised ADA criteria. IFG and IGT did not identify the same patients in the DANSUK study, and the cardiovascular risk profile of the patients was dependent on the outcome of the OGTT. We also observed a more favorable cardiovascular risk profile among patients additionally diagnosed with IFG according to the ADA criteria compared with the patients with IFG according to the WHO definition. However, when the additional IFG patients were compared with the final group of patients with NGT, the additionally diagnosed IFG patients had a significantly higher body mass index, HbA1c values and higher levels of insulin resistance. A new population was thereby labeled ‘prediabetic’, but evidence from clinical trials that lifestyle intervention in individuals with isolated IFG will actually benefit them is lacking. A study of patients with acute myocardial infarction recently showed that those additionally diagnosed with IFG according to the ADA criteria had higher 30-day mortality compared with patients with NGT [22]. IFG and IGT represent two different physiological phenotypes in glucose metabolism. Further studies are needed to evaluate whether the existing intervention strategies in cardiac rehabilitation clinics, both in the means of behavioural and pharmacological interventions, are applicable to the new concept of IFG. Showing that waist circumference and exercise capacity were independent predictors of T2DM in the DANSUK study still emphasizes important prevention implications in cardiac rehabilitation clinics, as intervention studies that were based on weight loss and increased exercise capacity successfully reduced the incidence of diabetes [21, 23].
Conclusion
The prevalence of IGM in a broad group of patients attending comprehensive cardiac rehabilitation was high, and IFG and IGT did not identify the same patients nor the same cardiovascular risk profile. If not yet performed at the time of referral, an OGTT seems indispensable in the settings of future cardiac rehabilitation.
Footnotes
Acknowledgements
The authors would like to thank the patients who participated in the DANSUK study and the following for financial support: Danish Pharmacy Foundation of 1991, Eva and Henry Frćnkel's Memorial Foundation, Copenhagen Hospital Corporation Research Council, The Research Foundation at Bispebjerg University Hospital, Builder LP Christensen's Foundation, The Danish Heart Foundation and the Danish Animal Protection Foundation.