
Abstract
The number of patients with type 2 diabetes is increasing rapidly in both developed and developing countries around the world. The emerging pandemic is driven by the combined effects of population ageing, rising levels of obesity and inactivity, and greater longevity among patients with diabetes that is attributable to improved management. The vascular complications of type 2 diabetes account for the majority of the social and economic burden among patients and society more broadly. This review summarizes the burden of type 2 diabetes, impaired glucose tolerance, and their vascular complications. It is projected that by 2025 there will be 380 million people with type 2 diabetes and 418 million people with impaired glucose tolerance. Diabetes is a major global cause of premature mortality that is widely underestimated, because only a minority of persons with diabetes dies from a cause uniquely related to the condition. Approximately one half of patients with type 2 diabetes die prematurely of a cardiovascular cause and approximately 10% die of renal failure. Global excess mortality attributable to diabetes in adults was estimated to be 3.8 million deaths. Eur J Cardiovasc Prev Rehabil 17 (Suppl 1):S3-S8 © 2010 The European Society of Cardiology
Keywords
Introduction
The prevalence and incidence rates of type 2 diabetes and impaired fasting glucose (IFG) are rising rapidly throughout most regions of the developed and developing world [1,2]. In large part the emergence of the diabetes pandemic is attributable to established causes, primarily the increasing number of older people and growing levels of obesity and physical inactivity. In addition, enhanced management of patients with type 2 diabetes is improving longevity among this patient group further adding to their numbers. Diabetes greatly increases the risks of vascular disease and much of the burden of type 2 diabetes is caused by macrovascular and microvascular complications [3,4]. Quantifying the number of patients with type 2 diabetes and its complications is of great importance to governments and healthcare providers, not least because of the huge drain that it puts on already scarce healthcare resources. This is particularly true for developing regions of the world in which the greatest expansion in the numbers with diabetes is projected to occur [1]. We summarize here key data describing the global burden of type 2 diabetes, impaired glucose tolerance (IGT), and their complications.
Type 2 diabetes
The prevalence of type 2 diabetes is increasing rapidly worldwide (Fig. 1). In 1995, the prevalence of type 2 diabetes was estimated to be 135 million people, which increased to 171 million people in 2000 [2] and to 220 million in 2004 [5]. Although type 2 diabetes is predominantly a disease of adulthood, there is substantial variation in the age groups of patients with type 2 diabetes between developed and developing countries. In developed countries the risk of type 2 diabetes increases progressively throughout life, and it is the 65 years and above age group that accounts for the majority of cases of diabetes. In contrast, in most developing countries for which data are available, the greatest number of individuals with type 2 diabetes are aged between 45 and 64 years with both the prevalence and absolute number of individuals with diabetes declining above 65 years [2].
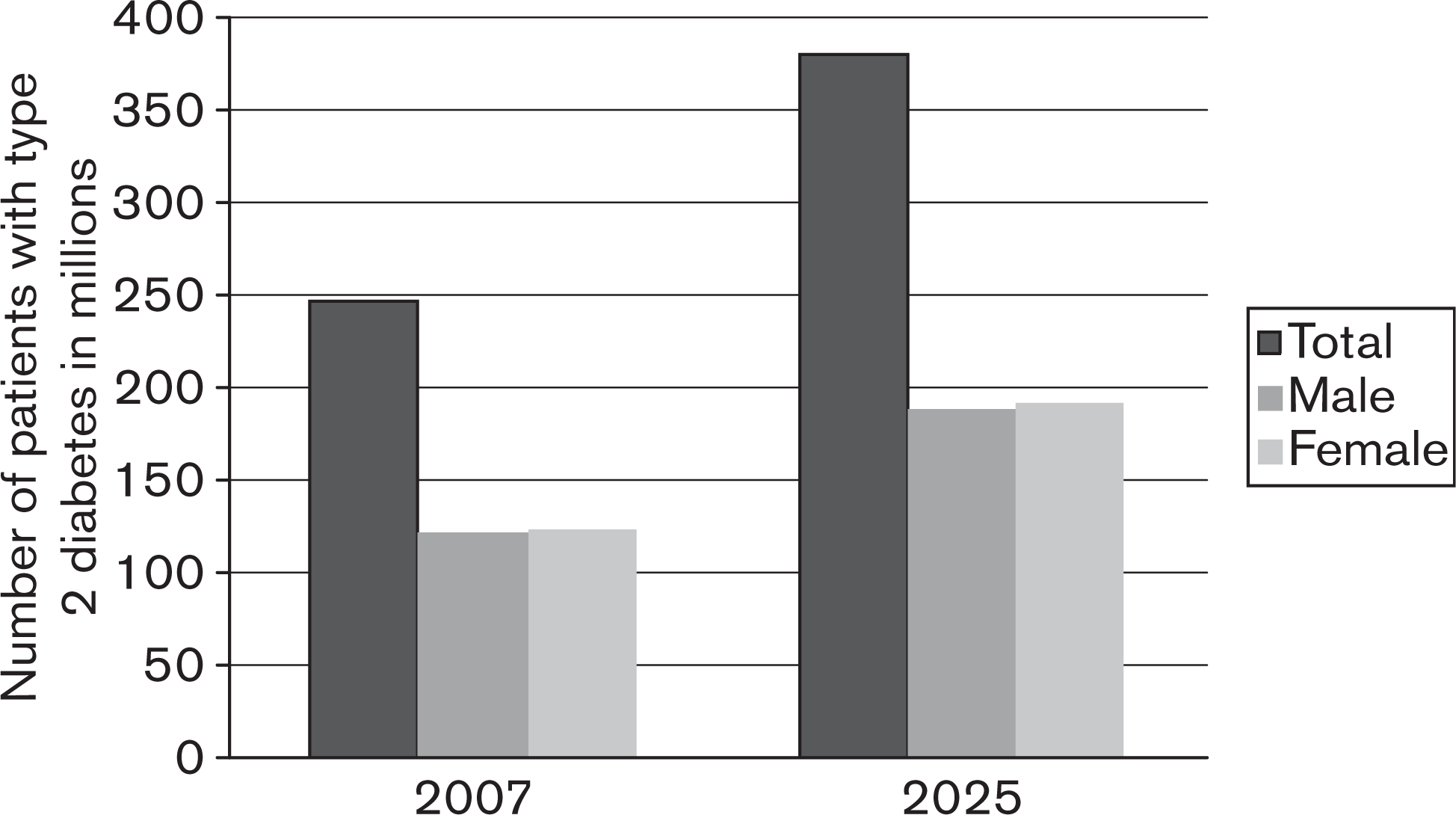
Total number of patients with type 2 diabetes in 2007 and estimated for 2025; total and by sex.
Worldwide, there are more women living with type 2 diabetes than men. Although the prevalence of diabetes is slightly greater in men under the age of 60 years, it is higher in women above this age, reflecting the greater likelihood of premature mortality among men with diabetes against a rising incidence of type 2 diabetes with age in both sexes [2]. The global imbalance in diabetes between the sexes is driven entirely by developed countries, with equal numbers of men and women affected by type 2 diabetes in developing countries [6].
The number of patients with type 2 diabetes is likely to be even higher than current estimates [1] because a substantial proportion of patients with type 2 diabetes go undetected. The onset of type 2 diabetes may occur up to 7 years before clinical diagnosis [7] and even in high-income settings such as the United States and The Netherlands, whereas the prevalence of undiagnosed diabetes is probably approximately 3% of adults [8,9]. Failure to detect diabetes typically rises with age [8] although there is some evidence that enhanced screening systems are decreasing the prevalence of undiagnosed diabetes in some developed countries [10]. The percentage of undiagnosed diabetes is higher in developing countries in which it is not unusual for half [11] or three quarters [1] of all cases of diabetes to remain undiagnosed.
The prevalence of type 2 diabetes is projected to rise from the current estimated 240 million affected (6% of adults) to some 380 million (7%) by 2025 [1]. Most of this growth will be in developing countries and will be substantially attributable to major changes in the number and average ages of the population of countries such as India and China [6]. By 2025 there will be some 192 million women and some 188 million men with type 2 diabetes with a substantially greater number of individuals with diabetes living in urban (179 million) compared with rural areas (81 million) [1].
Impaired glucose tolerance and impaired fasting glucose
The progression from normal-to-abnormal glucose homeostasis is a continuous one and the terms IGT and IFG describe the intermediate stage before the diagnosis of diabetes. IGT [12] is essentially an asymptomatic condition in which glucose regulation is found to be impaired in the 2-hour period after a 75 g oral glucose challenge. IFG [12] in contrast describes the state in which fasting plasma glucose concentration is elevated above usual levels (6.10 and 6.99mmol/l) but not sufficiently to meet the thresholds defined for diabetes [12]. There is some overlap between the two, and these states are often referred to as ‘prediabetes’ [7].
Patients with IGTor IFG are at a high risk of progressing to type 2 diabetes with annual progression rates of 17% for IGT and 12% for IGF observed in European populations [13]. Similarly, Mexicans and other developing country populations with impaired glucose homeostasis have been observed to be at markedly greater risk of developing diabetes [14,15]. Progression to type 2 diabetes is not, however, inevitable among this population group and 30% of people with IGT or IFG will have normal glucose levels on subsequent follow-up [1]. Both IGT and IFG increase the risks of vascular complications and contribute importantly to the total disease burden attributable to deranged glucose metabolism [16,17].
In 2007, there were an estimated 308 million people (7.5% of adults) with IGT [1], of which 80% were believed to be living in developing countries. Most people with IGT are between 40 and 59 years of age [1]. In Europe, China, and Japan, prevalence of IGT rises linearly with age but in India the prevalence of IGT seems to be constant across age groups. Women in Europe and India were more likely to have IGT than men, but in China and Japan the prevalence of IGT was higher in men than in women. The pattern observed for IGT was somewhat different, appearing to be stable across ages in Europe, China, and Japan, and higher in men than in women. For Indian people the prevalence of IFG was higher in women than in men and increased with age until the age of 69 for men and 79 for women.
Overall the prevalence of IGT is higher than IFG with global estimates of 8.4 and 6.3%, respectively, for people aged 40-59 years and a similar pattern for other age groups [13,15]. It is estimated that the global prevalence of IGT will rise to 418 million (8% of adults) by 2025 with an absolute increase in number of approximately 30-70% depending on the region. The greatest absolute increase will be for African, Eastern Mediterranean, and Middle East countries and by 2025 the highest prevalence of IGTwill be in people between 40 and 59 years of age [1].
Macrovascular complications
Cardiovascular disease (CVD) is the leading complication of type 2 diabetes and approximately one half of patients with type 2 diabetes will die of a cardiovascular cause. Angina, myocardial infarction, stroke, peripheral artery disease, and congestive heart failure are all common among patients with type 2 diabetes. IFG or IGT and the risks are further compounded by smoking, abnormal blood lipids, high blood pressure, and the other determinants of vascular risk established in nondiabetic populations [1,18].
Among some subgroups of patients the incidence of coronary heart disease (CHD) is comparable with that of patients without diabetes and with a history of CHD [19], and the rates of prevalent CHD reported among patients with type 2 diabetes are ranged between 5 and 36% depending on the setting [1]. Diabetes seems to confer an approximate doubling of the risk of CHD in men and a quadrupling of risk among women [20,21]. Therefore, although women in general have a lower absolute risk of CVD than men, the greater proportional increase in risk they experience leads to rates of CHD that are directly comparable (29 per 1000 person years for men and 23 per 1000 person years for women) [22].
The prevalence estimates of stroke among patients with type 2 diabetes range from 4 to 12% in clinic-based populations and between 4 and 5% in population-based studies [1]. The incidence of stroke in patients with type 2 diabetes can be more than three times the risk for the general population and seems to be more marked for men than for women. The prevalence of stroke increases linearly with age, the relative risk of stroke among diabetic patients older than 60 years is approximately five times the risk for patients under 50 years of age [23]. In Italy the incidence of stroke was 5.5 per 1000 person years in men and 6.3 per 1000 person years in women [24].
Microvascular complications
The microvascular complications of type 2 diabetes are principally nephropathy, retinopathy, neuropathy, and small vessel vasculopathy causing lower extremity amputation. The complications account for much of the social and financial burden of diabetes [3], and type 2 diabetes is a leading cause of blindness, renal failure, and lower limb amputations [25,26]. However, although the burden is undoubtedly large, the few high quality populationbased studies and the use of different diagnostic tools make it difficult to accurately describe the burden of these complications or make comparisons across different settings [1].
Diabetic nephropathy
Diabetes has recently become the leading cause of endstage renal disease in many developed countries accounting for up to 50% of patients receiving renal replacement therapy [26,27]. Worldwide, the number of patients with diabetes receiving renal replacement therapy has doubled from 12.7 million in 1990-1991 to 23.6 million in 1998-1999 [28]. This increase reflects both a change in referral and acceptance rates and a real increase in incidence. Incidence rates of renal failure among patients with type 2 diabetes are approximately six per 1000 person years, with approximately one-third dying and two-thirds becoming dialysis dependent [29]. Incidence of renal failure was highest among Native Americans (10.7), lowest among Europeans (2.9), and intermediate for East Asians (7.5). Incidence increased with age and duration of diabetes [29]. The incidence of diabetic nephropathy has increased over time in European countries though remaining stable in non-European countries [30] with the difference most likely explained by the rise of type 2 diabetes in developed countries.
Proteinuria is an important marker of diabetic nephropathy that is strongly associated with increases in vascular risk. Estimates vary widely depending on the populations studied and the methods used. In studies included in the Diabetes Atlas [1], prevalence of microalbuminuria ranged from 3 to 57% in clinic-based populations and from 19 to 42% in population-based studies. The prevalence of overt nephropathy was between 5 and 20% in clinic-based studies and 9 to 33% in population-based studies. Comparisons are difficult between countries because of the sporadic nature of the data available, but prevalence of diabetic nephropathy is typically higher among men and rises with age [31,32].
Diabetic retinopathy
Diabetic retinopathy is a progressive disorder of the retinal microcirculation and is the most common cause of blindness among people aged 30-69 years [33,34]. It is estimated to account for 5% of all cases of blindness globally [25,35]. Among patients with type 2 diabetes the prevalence of retinopathy ranges from 11 to 65% in clinic-based populations and from 10 to 55% in population-based studies [1]. Projections of prevalence of diabetic retinopathy and vision-threatening diabetic retinopathy in the United States for the years 2005-2050 suggest a tripling from 5.5 to 16.0 million and from 1.2 to 3.4 million, respectively [36]. Increased prevalence of diabetes, greater longevity among those with the disease, and changes in the age and racial background of the US population are the key drivers of change [36]. With many other parts of the world experiencing qualitatively similar changes, the global prevalence of diabetic retinopathy is likely to mirror that projected for the United States. The annual incidence of proliferative retinopathy is approximately 1% and approximately five times that for any retinopathy with slightly greater rates in women and increased risks with longer duration of diabetes [37]. In developed countries, incidence of serious retinopathy seems to have decreased over time, probably because improved patient management [38–40] and rates of retinopathy in recent trials are much lower [41]. Risks of diabetes-related blindness also increase with age and duration of diabetes but seem to be higher among males [42,43] with prevalence ranging from 3 to 7%. A further 10 to 24% of patients with type 2 diabetes are reported to be visually impaired [39,44–47].
Diabetic neuropathy and lower extremity amputations
Patients with type 2 diabetes have a more than 25 times greater risk of amputation than those without diabetes [48]. The prevalence of diabetic neuropathy ranges from 8 to 68% for clinic-based studies and from 13 to 45% for population-based studies. The prevalence of lower limb amputation is much lower (0.2–4.8%) with annual incidence rates for amputation ranging from 46 to 936 per 100 000. Reported rates are heavily dependent on the diagnostic tools and definitions used and the population studied, but rates seem to increase with duration of diabetes and age [49–51].
Mortality and total disease burden
Diabetes is a major global cause of premature mortality that is widely underestimated, because only a minority of patients with diabetes dies from a cause uniquely related to the condition such as diabetic ketoacidosis or hypoglycemia. Approximately 50% of persons with diabetes die of CVD, and 10% die of renal failure [52,53] both of which are directly attributable to diabetes. In the WHO report of 2004 it is described that 508 000 men have died from direct diabetes-related causes, which is 1.6% of all deaths and 633 000 women have died from type 2 diabetes, which is 2.3%. However, it is possible that this is heavily underestimated as the International Diabetes Federation estimates the deaths caused by diabetes in 2007 to be 3.8 million (6%) of total world mortality in persons between 20 and 79 years of age [1].
The risk of suffering a diabetes-related death is strongly related to age. In individuals with type 2 diabetes under 35 years of age, 75% of all deaths were attributable to diabetes, decreasing to 59% among those aged 35–64 years and 29% among those aged 64 years or older [54].
Women have a higher risk of diabetes-related mortality than men with a relative risk for women of 3.4 and a relative risk for men of 1.9 [19]. There are huge differences in mortality numbers across regions (Fig. 2). For countries with a high income diabetes is the eighth leading cause of death, whereas in middle-income countries it is the 10th leading cause of death. Again, this ranking is likely to be underestimated.
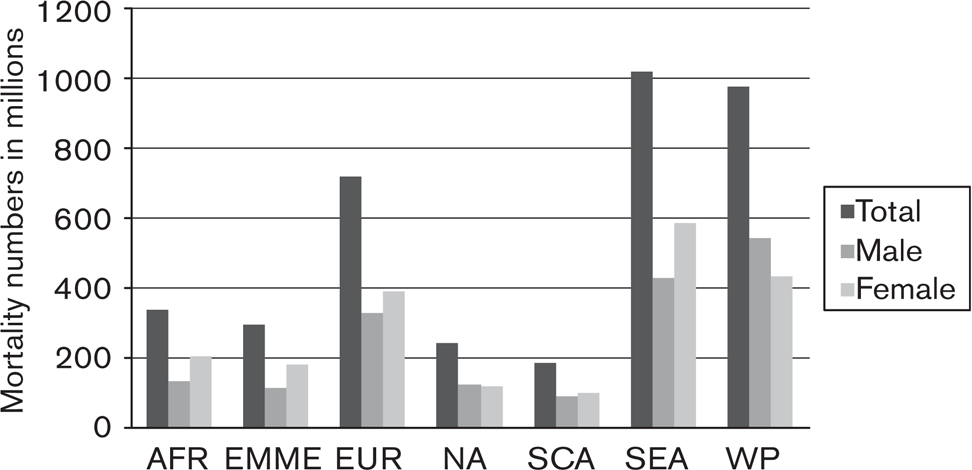
Mortality numbers by regions total and split by sex. AFR, African Region; EMME, Eastern Mediterranean and Middle East; EUR, Europe; NA, North America; SCA, South and Central Asia; SEA, South Eastern Asia; WP, Western Pacific.
In addition to being a substantial cause of death, diabetes also contributes a large total disease burden. In 2004, diabetes was estimated to be the eighth leading cause of years of life lost to premature mortality with approximately 2.3 million years of life lost equating to 3.4% of all life years lost that year. The total disease burden attributable to diabetes rises to 19.7 million disability adjusted life years (DALYs) once the nonfatal disease burden attributable to diabetes is incorporated into the equation. This was 1.3% of all DALYs in 2004 and it is projected that diabetes will rise from 19th place in 2004 to be the 10th leading cause of DALYs in 2030, causing 2.3% of all DALYs that year [5].
Economic costs
Diabetes is one of the world's most important causes of expenditure, mortality, disability, and economic loss. Global health expenditure to treat and prevent diabetes and its complications was approximately 232 billion US dollars in 2007, a figure that will exceed 302 billion by 2025. Approximately 80% of this money is spent in the few wealthy countries and very little in low and middle incomes where some 80% of the people with diabetes live [1]. The costs for patients with macrovascular complications are approximately three times higher than for patients with type 2 diabetes without macrovascular complications and approximately seven times higher than for people with neither type 2 diabetes nor with macrovascular diseases. Outpatient, inpatient, and pharmacy costs are all higher in patients with type 2 diabetes but inpatient costs are the main drive among those with macrovascular diseases, and pharmacy costs are the greatest component overall [55,56]. Costs for patients with microvascular complications are approximately two times higher compared with patients with type 2 diabetes and with no microvascular complications. Patients with microvascular complications used more oral antidiabetic drugs and insulin, and have had more and longer hospital stays and more outpatient visits [57].
The costs of chronic conditions associated with type 2 diabetes are unevenly distributed with approximately two-thirds of the costs accounted for by cardiovascular complications and much smaller sums for neurological, renal, ophthalmic, and peripheral vascular diseases [24].
Conclusion
The number of patients with type 2 diabetes is increasing, especially in developing countries. Patients with type 2 diabetes have greater increased risks of CVDs, renal failure, neurological conditions, and retinopathy. The economic costs for diabetes are high and will continue to rise. The identification of effective new strategies for the control of diabetes and its complications is a public health priority.
Footnotes
Acknowledgements
This research was performed within the framework of CTMM, the Center for
Translational Molecular Medicine (![]() ), project PREDICCt (Grant
01C-104), and supported by the Netherlands Heart Foundation, Dutch Diabetes Research
Foundation, and Dutch Kidney Foundation.
), project PREDICCt (Grant
01C-104), and supported by the Netherlands Heart Foundation, Dutch Diabetes Research
Foundation, and Dutch Kidney Foundation.
In the last five years, Bruce Neal has received consultancy fees from Pfizer, Roche and Takeda. He has received speaking honoraria from Amgen, AstraZeneca, Glaxo SmithKline, Pfizer, Roche, sanofi-aventis, Servier, and Tanabe. He has received research support from Johnson and Johnson, Merck Schering Plough, Servier and the United Healthcare Group.
All other authors report no conflicts of interest.