
Abstract
Objectives
This study reports on sudden cardiac death (SCD) in sport in the literature and aims at achieving a generally acceptable preparticipation screening protocol (PPSP) endorsed by the consensus meeting of the International Olympic Committee (IOC).
Background
The sudden death of athletes under 35 years engaged in competitive sports is a well-known occurrence; the incidence is higher in athletes (∼ 2/100 000 per year) than in non-athletes (2.5:1), and the cause is cardiovascular in over 90%.
Methods
A systematic review of the literature identified causes of SCD, sex, age, underlying cardiac disease and the type of sport and PPSP in use. Methods necessary to detect pre-existing cardiac abnormalities are discussed to formulate a PPSP for the Medical Commission of the IOC.
Results
SCD occurred in 1101 (1966–2004) reported cases in athletes under 35 years, 50% had congenital anatomical heart disease and cardiomyopathies and 10% had early-onset atherosclerotic heart disease. Forty percent occurred in athletes under 18 years, 33% under 16 years; the female/male ratio was 1/9. SCD was reported in almost all sports; most frequently involved were soccer (30%), basketball (25%) and running (15%). The PPSP were of varying quality and content. The IOC consensus meeting accepted the proposed Lausanne Recommendations based on this research and expert opinions (http://multimedia.olympic.org/pdf/en_report_886.pdf).
Conclusion
SCD occurs more frequently in young athletes, even those under the age of 18 years, than expected and is predominantly caused by pre-existing congenital cardiac abnormalities. Premature atherosclerotic disease forms another important cause in these young adults. A generally acceptable PPSP has been achieved by the IOC's acceptance of the Lausanne Recommendations.
Keywords
Introduction
Active participation in sports is generally considered to be beneficial for the health and well being of the individual [1]. The increased risk of sudden death in adolescents and young adults engaged in competitive sports, a well-known and much feared occurrence, seems to contradict this adagium [2–4]. The leading cause of this mortality is underlying cardiac disease (∼90%) [5–7], triggering sudden death during intensive physical exercise. The non-cardiac causes of sudden death include asthma (or other pulmonary conditions), heat stroke, drug abuse, cerebral embolism, ruptured cerebral artery and some unexplained causes.
The incidence of sudden cardiac death (SCD) in young athletes (aged 12–35 years) is 0.5–2/100 000 per year [4, 6, 8–10], and is approximately 2.5 times higher than in non-athletes [11]. This increased mortality has led to the implementation of various preparticipation screening protocols (PPSP), showing a wide difference depending on the mandating organizations or countries. Some are quite specific and involve serious physical examinations, whereas others are merely questionnaires. The quality of each of these PPSP depends greatly on the way the examinations are carried out, and varies from inadequate to thorough.
A generally accepted and implemented PPSP would be preferable, but the difficulty in achieving a consensus is located in the vast number of governing bodies involved. Several governments have by law implemented different regulations, various sports organizations have started to use their own PPSP, and a diversity of medical organizations have issued, sometimes very different, guidelines.
The aim of our review of the literature was to analyse the reported cases of SCD among young athletes, to identify the sports with the highest risk of SCD, and to compare the PPSP in use.
This was to allow an evaluation of the effect of the different methods and to assemble the parameters required to propose to the International Olympic Committee (IOC) a generally acceptable and safe screening.
Methods
For a meta-analysis of the existing literature on sudden death in sports and the effectiveness of PPSP, the following databases were searched: Medline (OVID Web, 1966–2004), PubMed (1966–2004), Cochrane Database of Systematic Reviews, EBM Reviews – ACP Journal Club, Cinahl 1982–2004, Heracles, Web of Science, Scopus <1960–2004. We used ‘sudden cardiac death’ and ‘preparticipation’ as keywords, combined with ‘sports’, ‘sports medicine’, ‘athletic injuries’, ‘exercise’ and ‘athletes’. Restrictions were English language and human subjects. To be overinclusive, there were no restrictions concerning age, sex, or study methodology. The keyword search yielded MeSH headings, which were exploded before they were combined. For study and data selection, we reviewed the results of the search and selected and grouped all studies reporting on SCD (reported cases) and the use of PPSP. Sudden death in athletes by other causes such as neurovascular, heat and doping were excluded and will not be discussed.
The initial search identified 2866 articles (SCD 1493 plus PPSP 1532) after duplicates were removed.
Sudden cardiac death
A total of 1493 articles were identified by the initial search; 124 were relevant to SCD in athletes, and were available, after review of all the titles and abstracts. We focused on athletes under 35 years of age, as the causes of SCD change past 35 years, atherosclerotic coronary artery diseases becoming much more frequent (84 versus 2% before 35 years) [5, 12–18]. Content experts within the medical profession were contacted as well as the relevant sports organizations to identify studies missed by electronic searches.
We used the following criteria to select the articles relevant to our study: articles reporting cases of SCD in athletes, aged up to 35 years, exercise-related, and in the absence of evidence of drug abuse.
SCD is defined as a death occurring within 1 h of the onset of symptoms in a person without a previously recognized cardiovascular condition that would appear fatal. An athlete is defined as a person participating in an organized team or individual sport that requires systematic training and regular competition against others, and that places a high premium on athletic excellence and achievement [19, 20].
There were 47 articles left after this final selection (Table 1), which we analysed.
Preparticipation screening protocols
A total of 1532 articles were identified by the initial search; 108 were relevant to PPSP in athletes, and were available, after review of all the titles and abstracts. Content experts within the medical profession were contacted as well as the relevant sports organizations to identify studies missed by electronic searches.
We used the following criteria to select and group the articles relevant to our study: (i) articles describing the PPSP procedure (cardiovascular part) and using it (± reported cases; Table 2); (ii) articles describing the PPSP procedure (cardiovascular part) but not using it (no reported cases; Table 3); (iii) articles about PPSP, specifically electrocardiography (ECG) or echocardiography [21–29]. Thirty-one articles were selected, with 11 in (i), 11 in (ii), and nine in (iii), and were analysed.
These groupings were reviewed and approved by an ad hoc consensus meeting of the IOC working group on Sudden Death in Athletes including several authors of the primary studies included and the Medical and Scientific Director of the IOC Medical Commission.
Outcomes of the studies were summarized for strength of evidence. The definitions of outcome of the authors of the studies included were accepted.
Results
Sudden cardiac death
Forty-seven articles were analysed and are represented in Table 1. The references of the articles were noted (classified in alphabetical order according to the last name of the first author), the type of article, the number of reported cases, the age and sex of the cases, the activity when SCD occurred, the eventual presence of previous symptoms and clinical data, whether an autopsy was carried out, and finally the cardiovascular diagnosis.
Selected articles on sudden cardiac death (SCD)
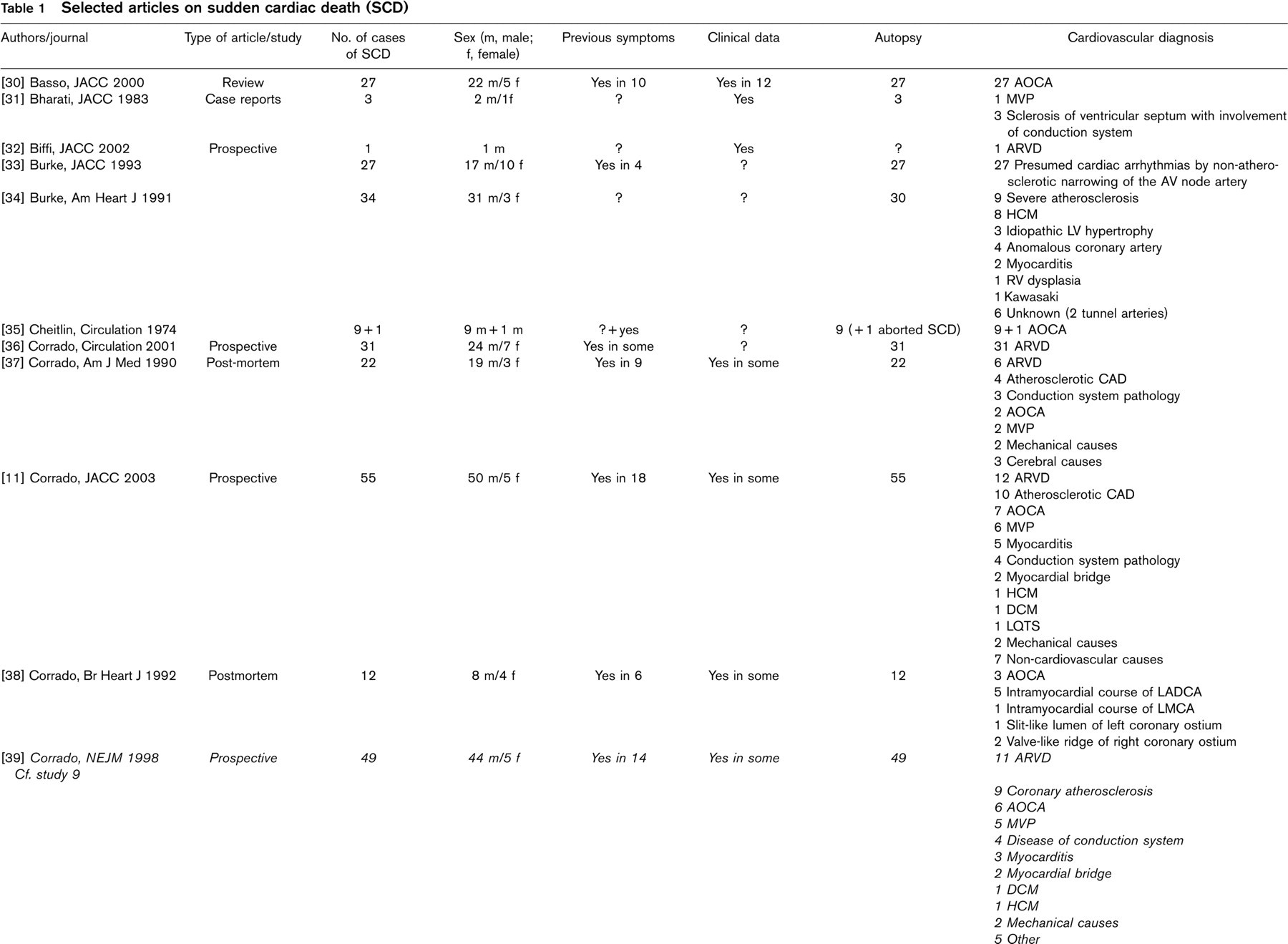
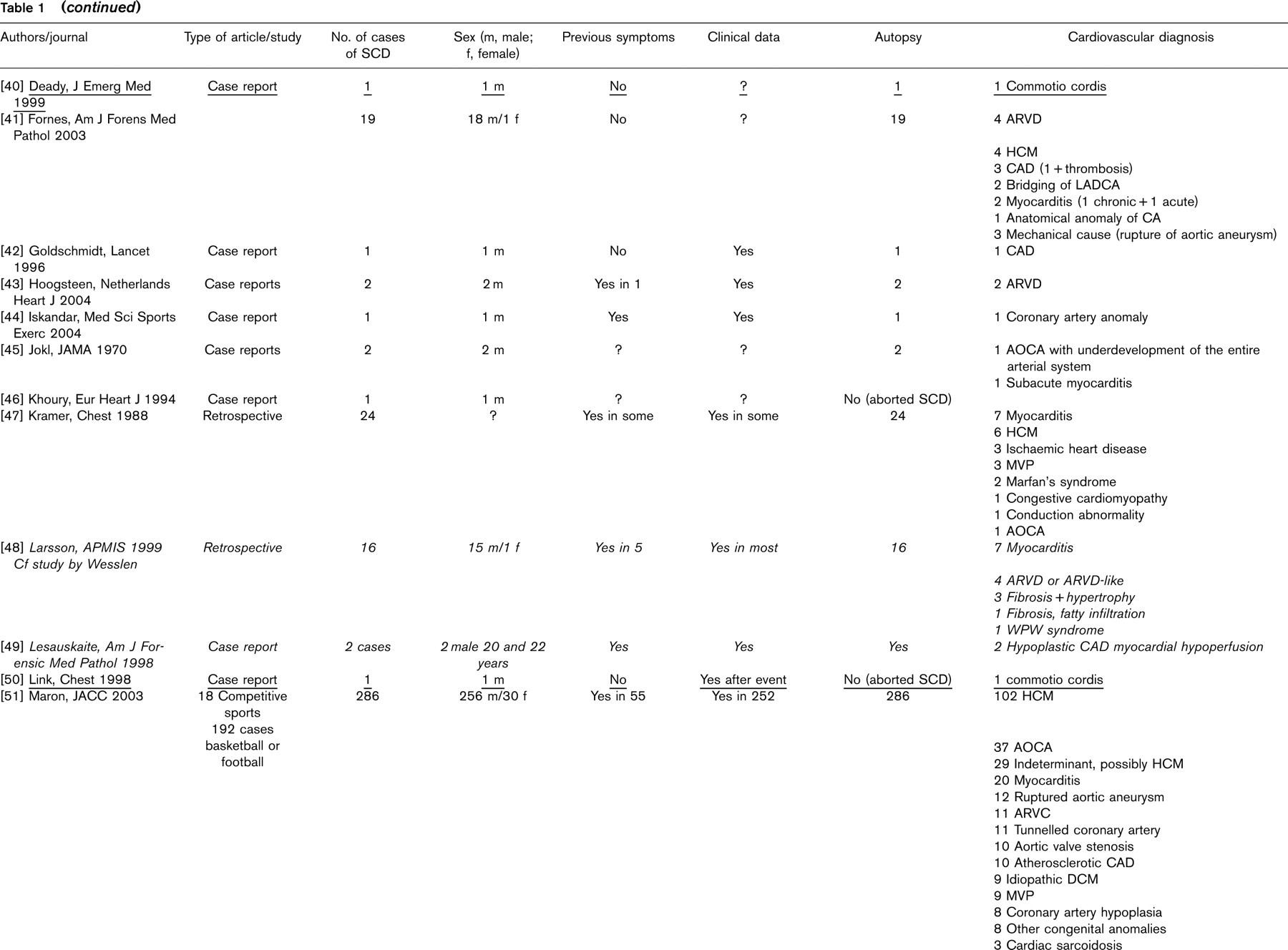
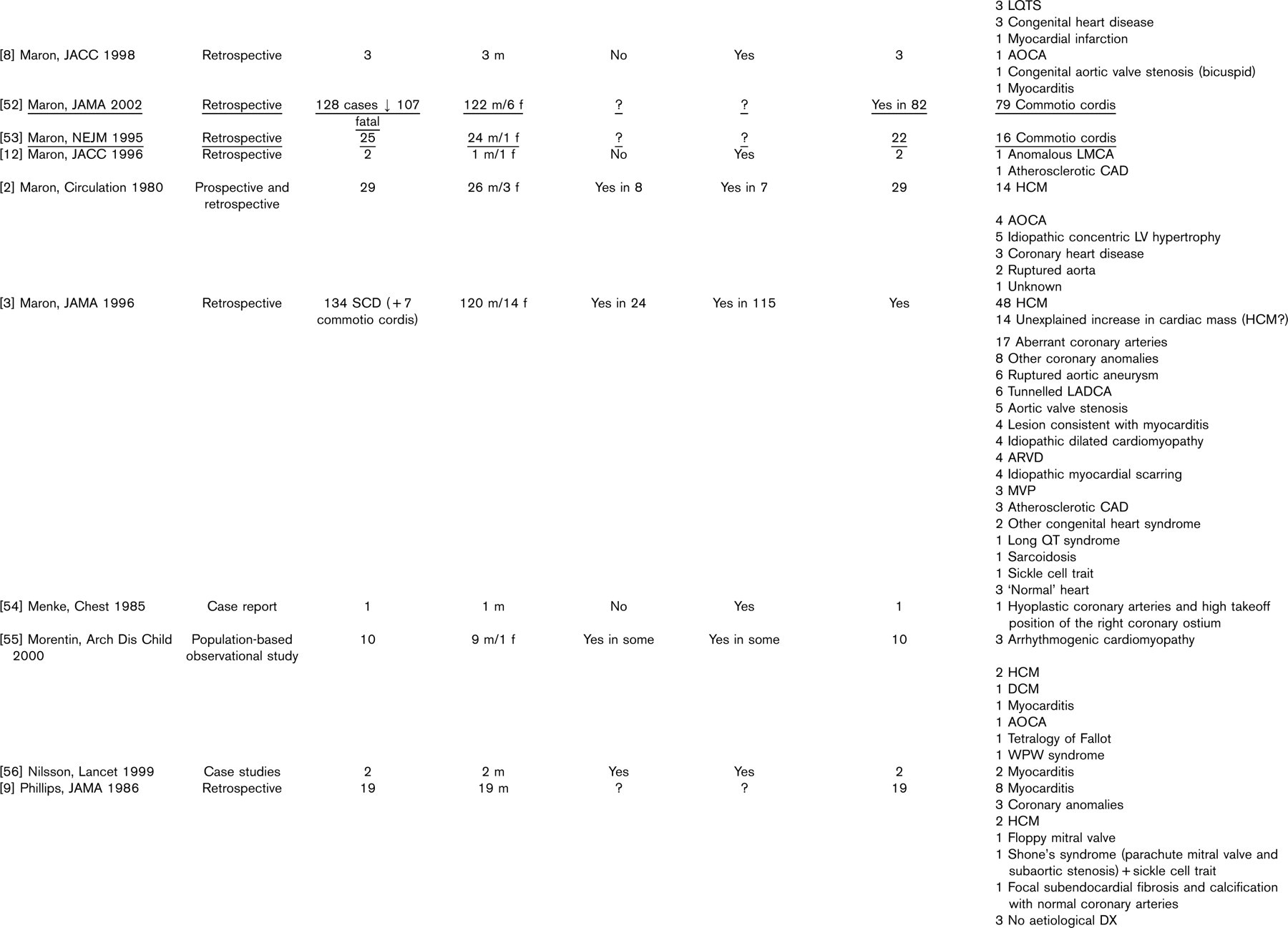
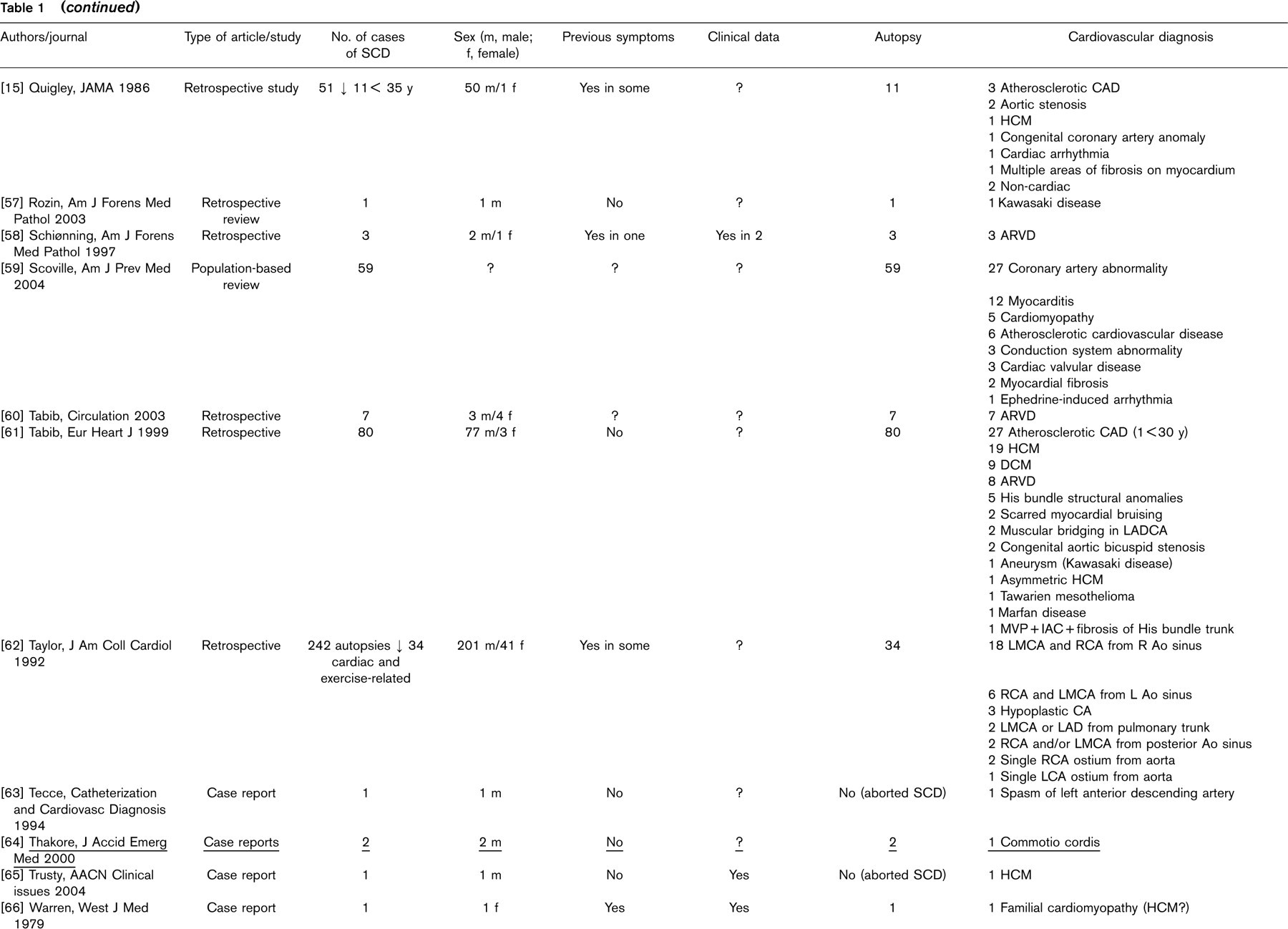
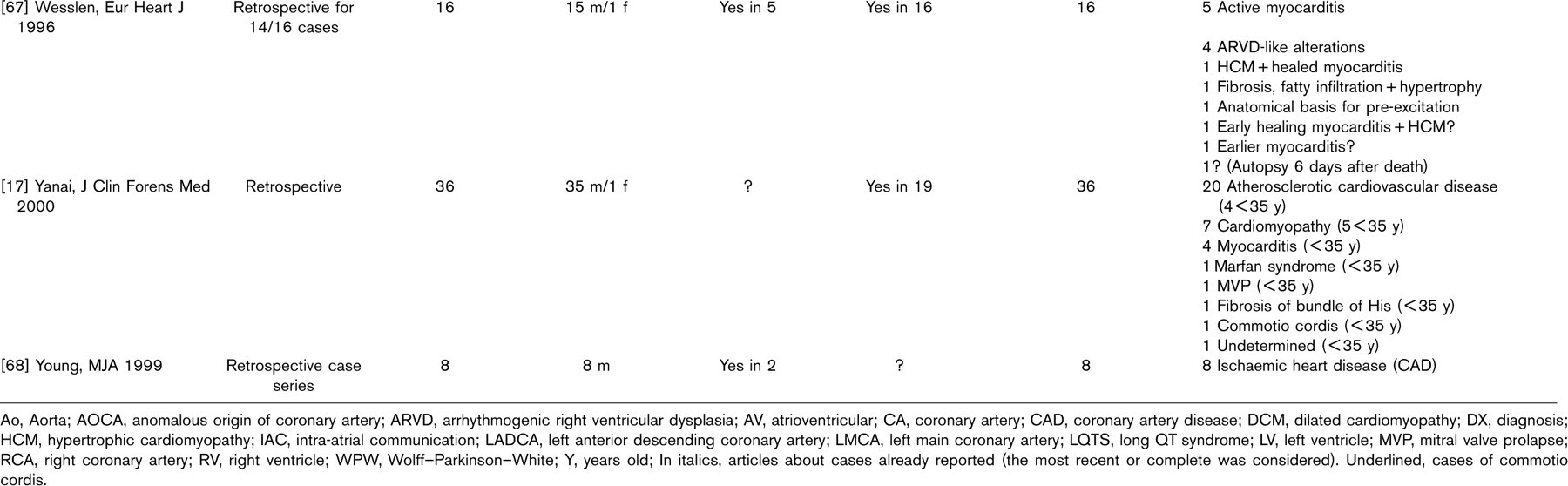
Ao, Aorta; AOCA, anomalous origin of coronary artery; ARVD, arrhythmogenic right ventricular dysplasia; AV, atrioventricular; CA, coronary artery; CAD, coronary artery disease; DCM, dilated cardiomyopathy; DX, diagnosis; HCM, hypertrophic cardiomyopathy; IAC, intra-atrial communication; LADCA, left anterior descending coronary artery; LMCA, left main coronary artery; LQTS, long QT syndrome; LV, left ventricle; MVP, mitral valve prolapse; RCA, right coronary artery; RV, right ventricle; WPW, Wolff–Parkinson–White; Y, years old; In italics, articles about cases already reported (the most recent or complete was considered). Underlined, cases of commotio cordis.
The articles were either case reports, relating the death of one or several athletes, or larger retrospective, sometimes prospective, studies. They were published between 1970 and 2004. The total of reported cases of SCD in athletes is 1101 cases (articles reporting the same cases are excluded, and appear in italics). This total includes the 103 cases of commotio cordis (blunt trauma to the chest, not particularly violent, that causes arrhythmias potentially followed by death) found in the articles (underlined).
The 1101 cases were grouped after pathology, according to the cardiovascular diagnosis, into 10 groups and 31 subgroups, as shown in Table 4. Coronary artery anomalies, half of them being anomalies of the origin of the coronary artery, the other half anomalies of the course of the coronary artery, and hypertrophic cardiomyopathy (HCM) are the two largest groups, with 262 and 261 cases, respectively. Traumatic cases of SCD being excluded (103 cases), there are 998 remaining cases, as shown in Fig. 1.
Focusing on the youngest athletes, 80 out of 199 were under 18 years of age, which represents as much as 40% of the cases, and 67 were under 16 years, 20% of the cases, with all types of underlying cardiac pathologies.
The cases were also grouped according to the sports the athletes were engaged in when sudden death occurred (Fig. 2). In 388 cases the sport practised when SCD occurred was mentioned. Deaths by commotio cordis (103) are not included in this figure.
Preparticipation screening protocols
A total of 108 articles were considered, and 31 articles were examined more closely, separated into three groups. (i) Articles describing the PPSP procedure (cardiovascular part) and using it (± reported cases): 11 articles. The articles were classified in Table 2, by alphabetical order of the first author. We looked at the population screened, where the PPSP was produced and when, who was performing the PPSP, at what frequency, what was the content of the PPSP (medical history, physical examination, non-invasive tests), the number of athletes screened, the number of athletes disqualified by the PPSP and the number of SCDs. (ii) Articles defining the PPSP procedure (cardiovascular part) but not using it; no reported cases: 11 articles. The articles were classified in Table 3, by alphabetical order of the first author. We looked at the origin of the protocol, the persons performing the PPSP, the frequency of screening and the content of the protocol. (iii) Articles about PPSP, specifically ECG or echocardiography: nine articles [21–29]. We focused on the utility of the test for diagnosing underlying cardiovascular diseases, the indications for using the test, the cost-effectiveness, and the opinion of the author on the test.
Articles describing the preparticipation screening protocols procedure (PSPP) and using it
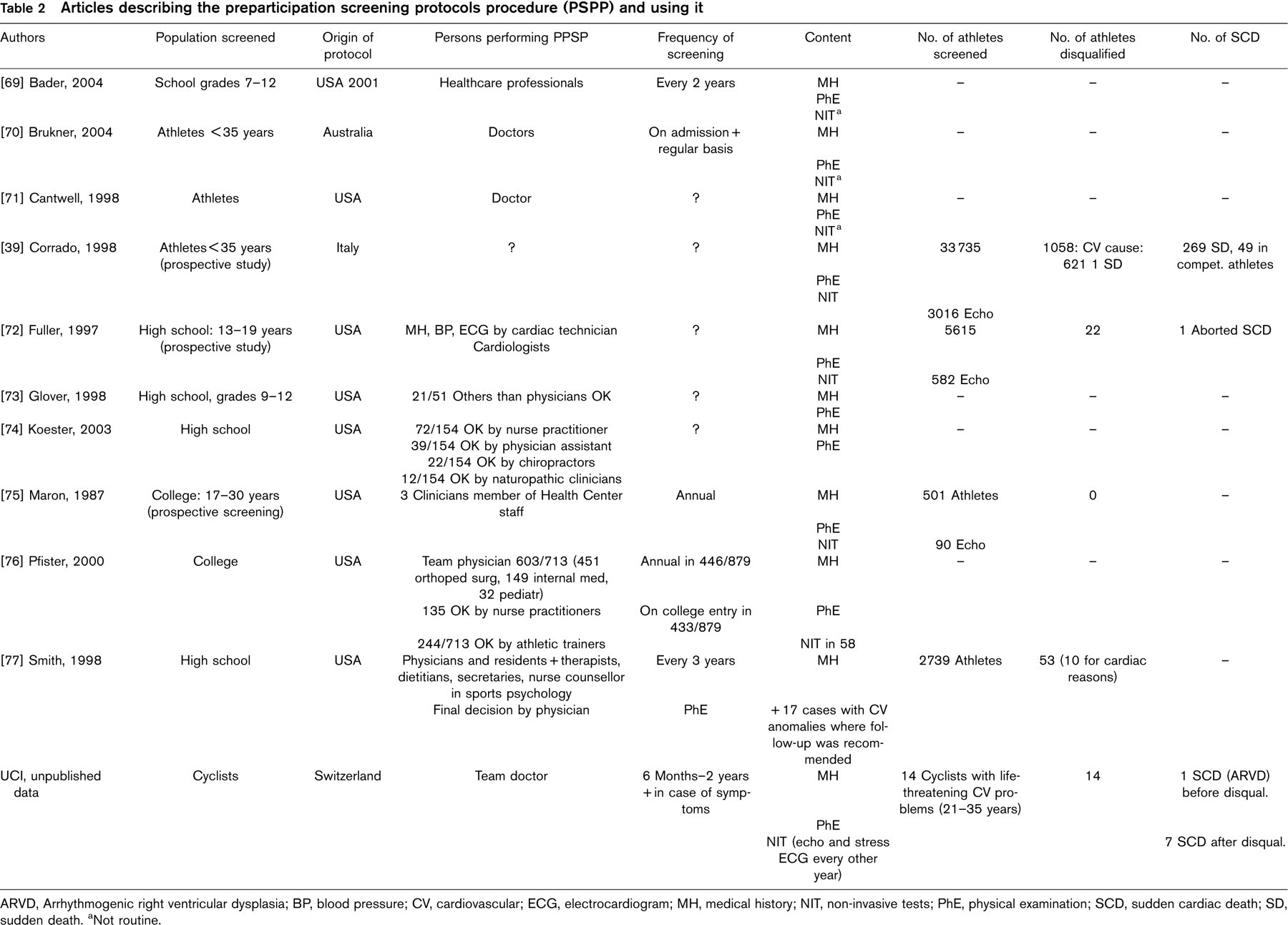
ARVD, Arrhythmogenic right ventricular dysplasia; BP, blood pressure; CV, cardiovascular; ECG, electrocardiogram; MH, medical history; NIT, non-invasive tests; PhE, physical examination; SCD, sudden cardiac death; SD, sudden death.
aNot routine.
Articles describing a preparticipation screening protocols procedure, without using it
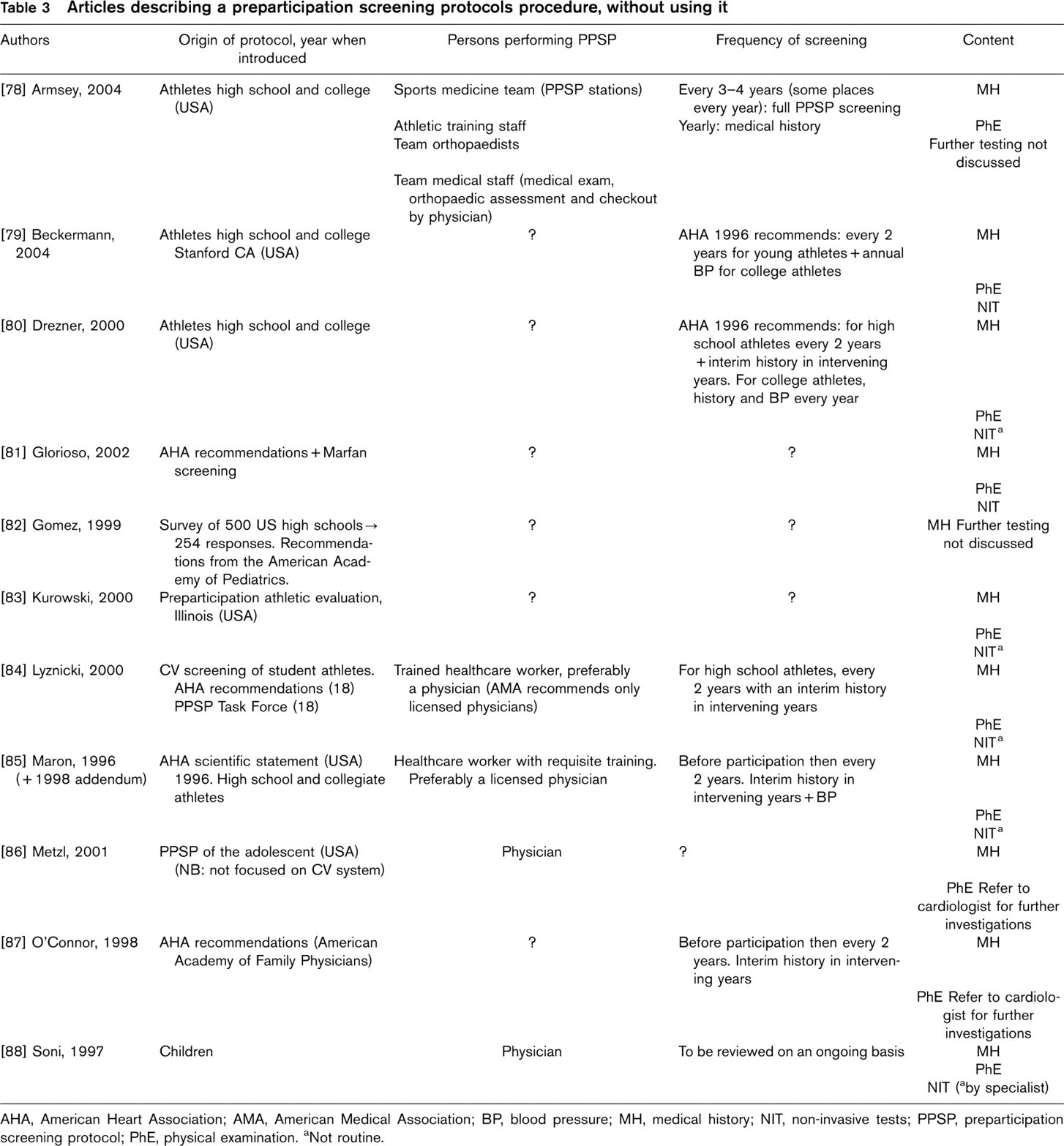
AHA, American Heart Association; AMA, American Medical Association; BP, blood pressure; MH, medical history; NIT, non-invasive tests; PPSP, preparticipation screening protocol; PhE, physical examination.
aNot routine.
Discussion
Physical activity is promoted and encouraged in society. It is considered healthy, with positive effects on the body and the mind. Healthcare and educational systems incite the population to be active in sports. The increased risk of exercise-related sudden death [10, 62, 89] might pose an irrelevant question mark on this statement, which is not justified because the positive effects of regular physical activity far outweigh the negative effects. Exercise-related sudden death can have many causes, such as cardiac, asthma or other pulmonary conditions, heat stroke (hyperthermia and dehydration), cerebral embolism or ruptured cerebral artery, trauma of the spine or head, drug abuse and doping. Doping is often considered to be the main cause of sudden death by the media and lay people [90], which seems unlikely, as underlying cardiac diseases account for approximately 90% of exercise-related sudden deaths [5–7].
Causes of sudden cardiac death
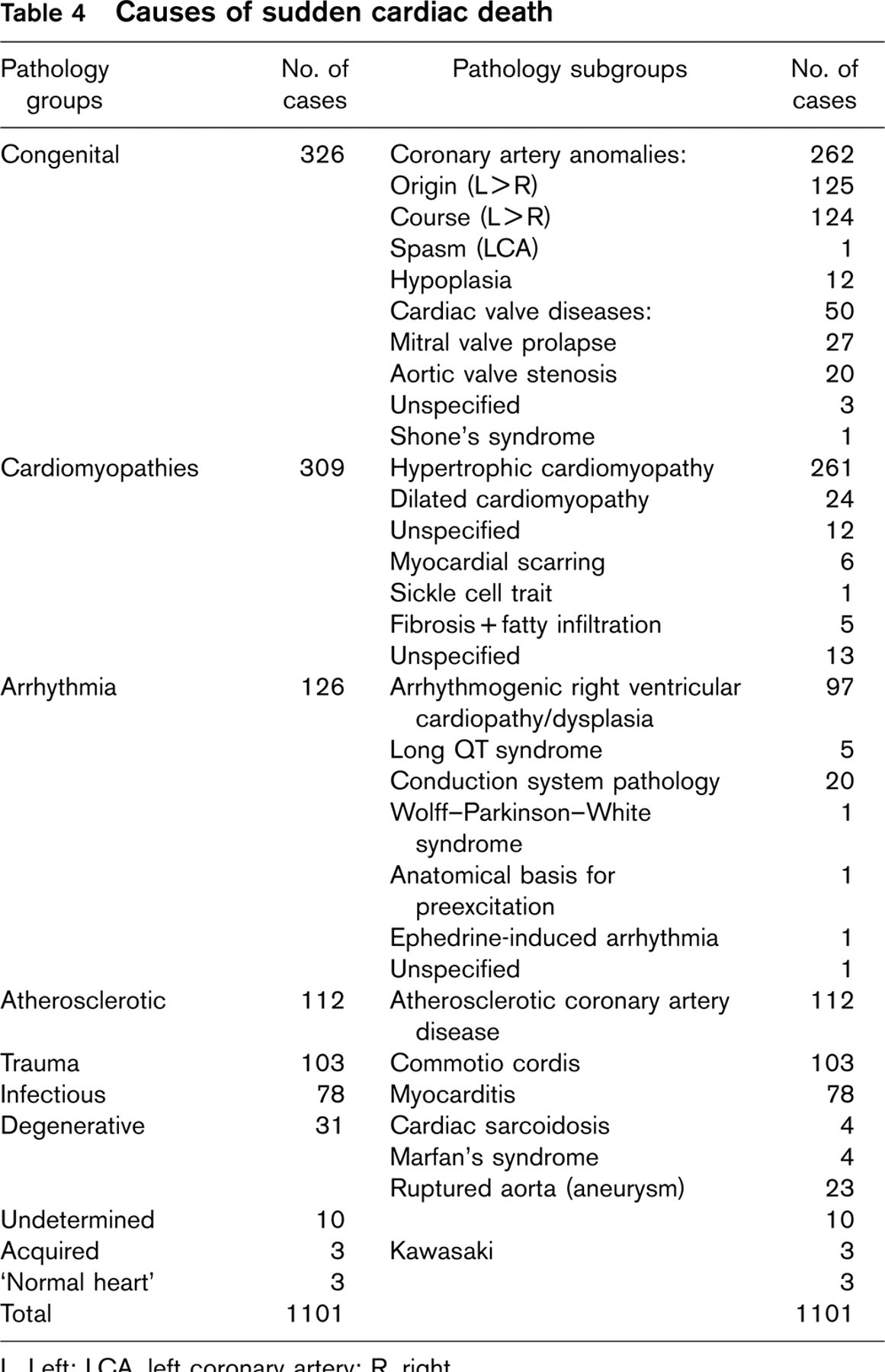
L, Left; LCA, left coronary artery; R, right.
The incidence of SCD in young athletes is 0.5–2/100 000 per year [6, 8–10]. Although the underlying forms of cardiac pathology are infrequent, they are represented in the athletic population as they are in the general population. The intense physical training and competition, with the accompanying higher cardiovascular demands, enhances the risk of athletes suffering serious consequences from their underlying cardiovascular disease [2, 3]. The identification of the pre-existing pathology suggests that sport itself is not per se the cause of the increased mortality; it rather acts as a trigger upon underlying cardiovascular diseases, predisposing to life-threatening ventricular arrhythmias during physical exercise.
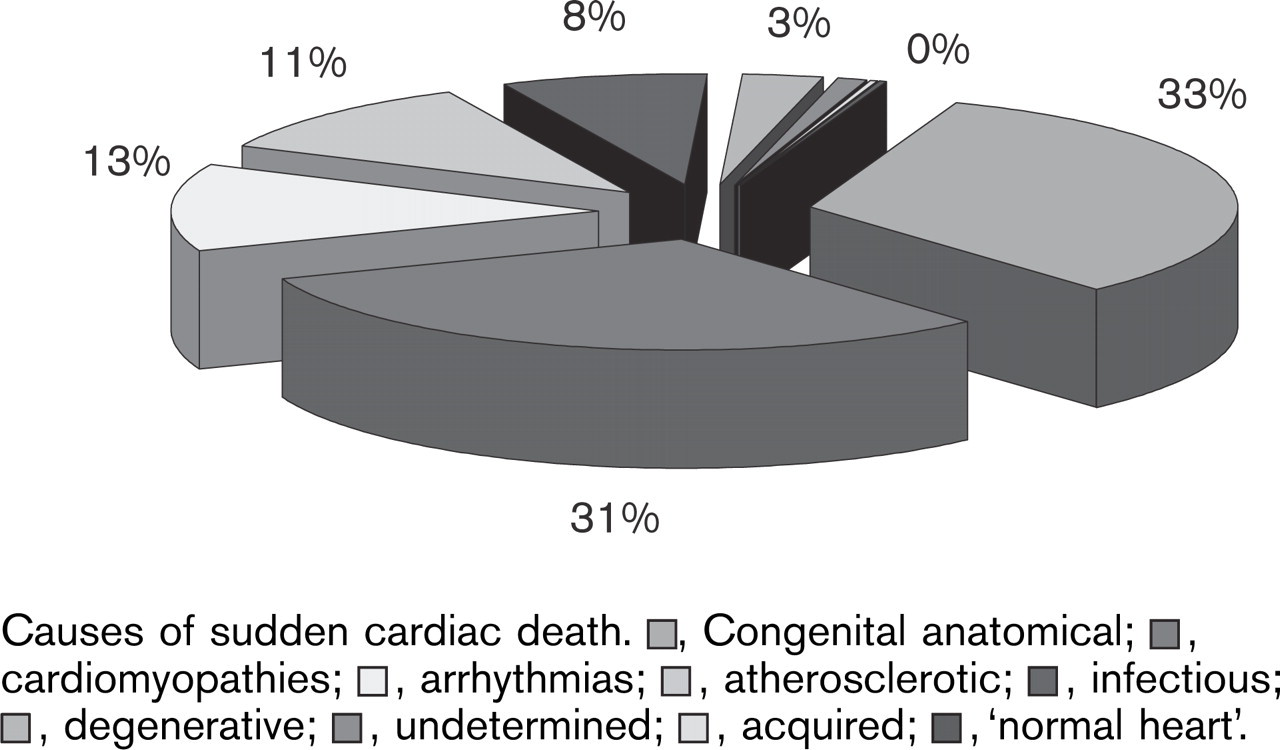
Causes of sudden cardiac death. ▪, Congenital anatomical; ▪, cardiomyopathies; ▪, arrhythmias; ▪, atherosclerotic; ▪, infectious; ▪, degenerative; ▪, undetermined; ▪, acquired; ▪, ‘normal heart’.
The unfortunate absence of national or international registers, which could provide precise data, suggests that SCD, although the present numbers are already impressive, is probably under-reported. The absence of precise data makes our/any analyses of reasons for SCD fragile and probably biased. For example, coronary artery diseases and HCM are the leading causes of SCD but are also the easiest to find; more difficult to find causes such as arrhythmias and arrhythmogenic right ventricular dysplasia may be under-represented. Cardiac causes of sudden death in the cases reported are listed in Table 4. Congenital coronary anomalies, such as abnormal origin and abnormal course of the coronary arteries and HCM are the leading causes of SCD [3, 4, 6, 7, 17–19, 91]. The reported leading causes of SCD, however, vary greatly from author to author. Corrado et al. [11] reported coronary artery anomalies (atherosclerotic and non-atherosclerotic) as by far the leading group with 30% of cases, whereas HCM accounts for only 7% [36, 38, 39]. Hoogsteen et al. [43] reported 38% of cases caused by HCM, with 26% of coronary artery anomalies.
The low proportion of SCD with a normal heart at pathological examination is another point of interest, which probably has to do with the interest of the pathologist or cardiologist to report on clearcut pathology rather than normal conditions, together with the fact that in our study we excluded all potential doping-related events.
A remarkable point is that atherosclerotic coronary artery disease already plays an important role in SCD in the young athlete; this premature form of atherosclerosis accounts for 2–20% of the cases of SCD depending on the study, and has long been overlooked.
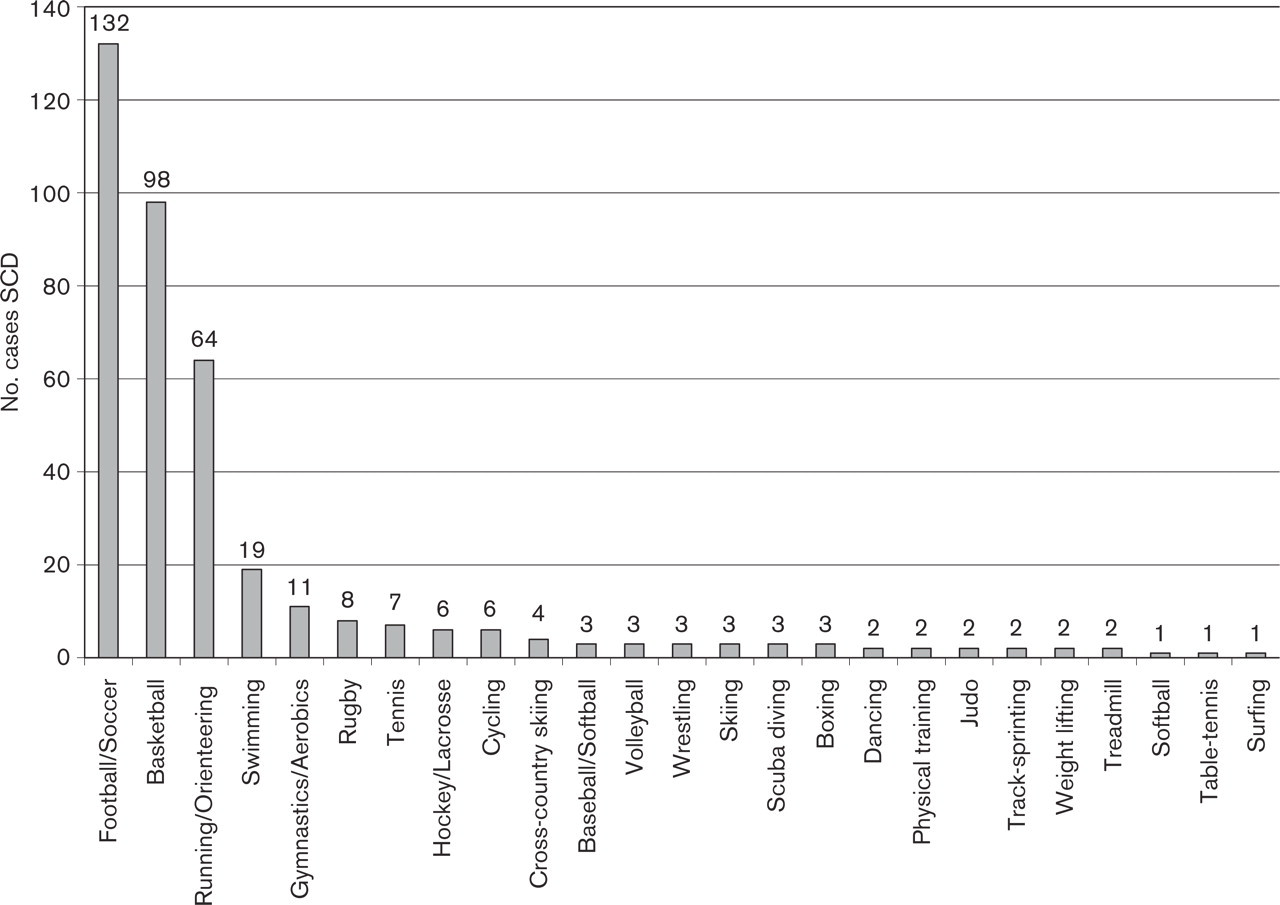
Number of cases of sudden cardiac death (SCD) by sport.
Classification of sports

Congenital anatomical heart diseases, cardiomyopathies and atherosclerosis represent 75% of the cases of SCD reported, if traumatic causes (commotio cordis) are excluded (Fig. 1). The various percentages of cardiopathic causes can be explained by the different incidences of the cardiopathies, HCM having an incidence of only 1/500 [4, 6, 92, 93], whereas anatomical anomalies of the coronary arteries have an incidence of 0.3–1/100 [5, 62].
A strikingly high percentage of very young athletes suffer from SCD. We found that approximately 40% of the total of SCD, in which the age was specified, occurred in athletes under 18 years of age, 80 of 199 athletes (out of the total 998 cases), 67 of these were even younger than 16 years. In the remaining 799 (998–80) the age was not specified.
To assess the risk of SCD, sports can be classified depending on the dynamic (isotonic) and static (isometric) work (Table 5). We grouped the reported cases by sport in Fig. 2, which shows that football/soccer, basketball and running/orienteering are the largest but not necessarily the most dangerous groups. They probably encompass the largest population of sports participants, because of their popularity. This does not mean that although these sports provide the largest number of SCD they necessarily are the sports with the highest risks. The sports with the highest cardiovascular demands and the highest isotonic work remain therefore to be more at risk of SCD, but because of a smaller number of participants have a smaller absolute number of SCD. This does not mean that the mentioned examples of sports per se represent a risk of SCD.
Lausanne Recommendations: sudden cardiovascular death in sport. Preparticipation cardiovascular screening. Under the umbrella of the International Olympic Committee Medical Commission, 10 December 2004
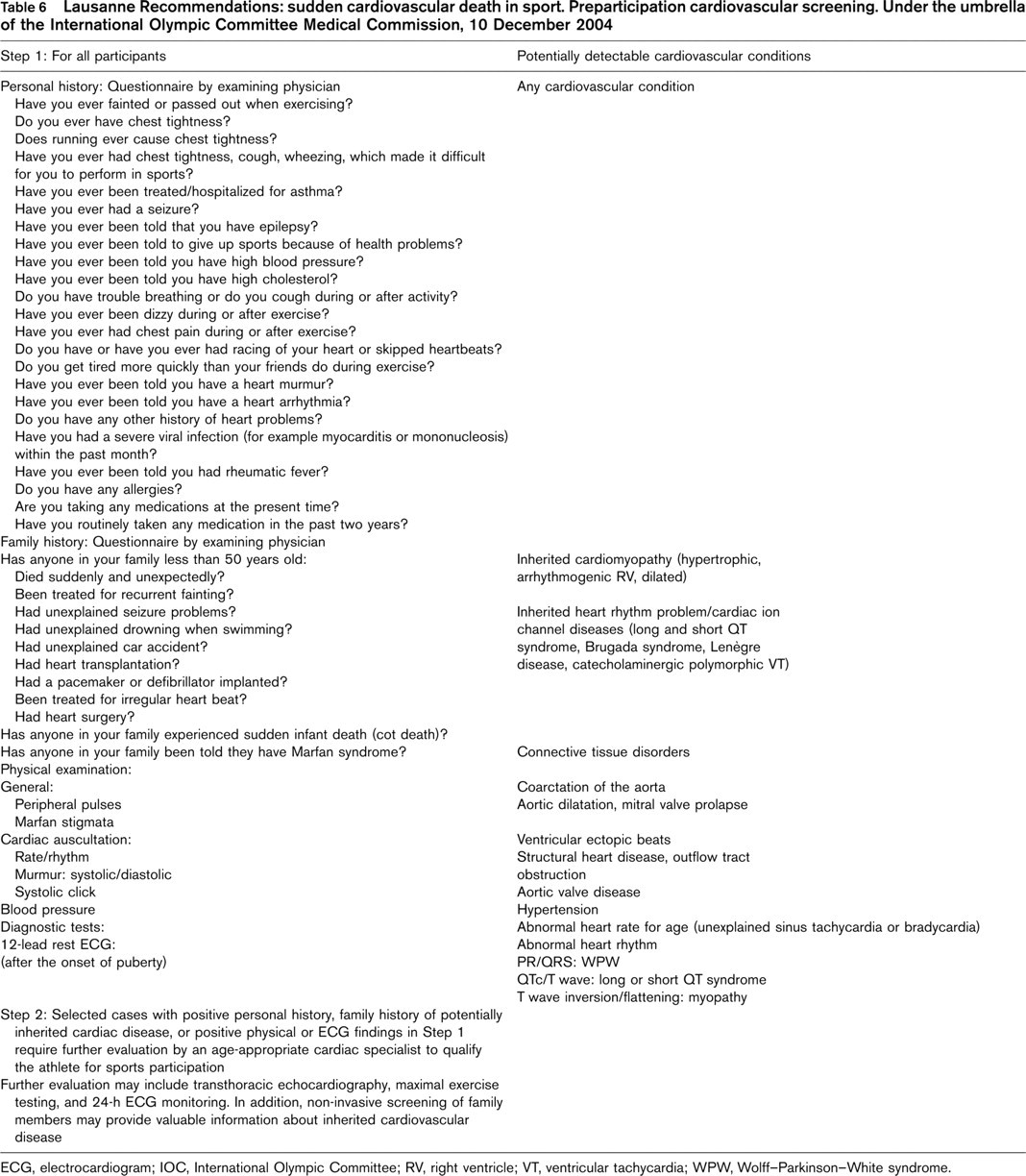
ECG, electrocardiogram; IOC, International Olympic Committee; RV, right ventricle; VT, ventricular tachycardia; WPW, Wolff–Parkinson–White syndrome.
After reviewing the causes of SCD and the sports with the highest risk of a cardiac event, the PPSP was considered. The studies reviewed reveal that the protocols are often considered as recommendations, and are only partly used. Some are considered inadequate for cardiovascular evaluation and contain four or fewer items recommended by the American Heart Association. The existing protocols all include a medical history and a physical examination, in some cases diagnostic tests, of varying content. The person performing the screening is also variable, some places allowing non-physicians [19, 69, 72, 73, 74, 76, 77, 78, 84, 85] to conduct the examination, which decreases the chances of positive findings. One wonders what the results will be when technicians, nurses, chiropractors, or athletic trainers perform the cardiovascular screening.
Even if a general consensus concerning the need for screening did exist, cost-effectiveness and the fact that it is not possible to prevent all deaths constitute a major problem. The Italian screening programme, consisting of history, physical examination and ECG seems to be cost-effective and efficient. Abnormal ECG lead to further investigations (often echocardiography) to detect cardiovascular diseases at risk of sudden death in athletes. As only 9% are false positives, the low cost of the ECG justifies this small percentage of unnecessary echocardio-graphies. As sport is a voluntary activity, death should not occur or at least be prevented as much as possible. Knowing the amount of money spent on top sports, the budget should also allow for the most efficient screening, to be performed by professionals.
The articles studied in the PPSP parts (i) and (ii) show a striking lack of uniformity, considering both quantity, the number of questions and tests, and quality. Although the protocols studied are aimed at detecting underlying cardiovascular diseases, in some the application of the recommendations is so limited that the usefulness of such screenings is questionable. The quality of the screening will not change its cost, as far as medical history and physical examination are concerned.
When it comes to the diagnostic tests, there are varying approaches, depending mostly on the population screened. Mass screenings in high schools and colleges most often do not comprise routine diagnostic tests, but in some places an ECG is included [39, 72, 75, 79, 88]. Suspect cases are referred to specialists for further investigations. In screening protocols for elite athletes, ECG and echocardiography at least are often routine [94]. This is the case for example in the programme of obligatory examinations of the International Cycling Union.
ECG and echocardiography each have their strong and weak points, and uniformity is not reached here either. ECG can often be abnormal in well-trained athletes [4, 21, 95–97], with patterns resembling those found in cardiovascular diseases such as HCM, which is the origin of many false positives. Despite this disadvantage, it is still considered a valuable screening tool because of its high negative predictive value and its low cost. Echo-cardiography on the contrary is expensive, but can reveal the pathologies most frequently encountered in SCD.
Our meta-analysis aims to provide a well furnished literature basis and form a platform for a generally accepted PPSP. The cooperation with the IOC and the consensus meeting on SCD in athletes organized by the Medical Commission of the IOC provided a tool to come to a generally acceptable screening procedure adopted by the IOC as the Lausanne Recommendations.
The Lausanne Recommendations (Table 6) are aimed at preventing SCD. We have assembled elements from the various existing protocols and studies that will help us best detect underlying cardiovascualr diseases that could cause SCD in athletes. It is a stepwise approach.
Step 1 is the basic screening that should be offered to every athlete. It is focused on detecting underlying cardiovascular diseases and includes a detailed personal history, a family history, a physical examination and a 12-lead ECG. The questionnaire consists of preconceived closed questions, in which a ‘yes–no’ answer has to be given. Any ‘yes’ requires further enquiry. The family history is focused on cardiovascular diseases, either congenital or acquired, and premature sudden death. It is important that the physician performing the screening is trained to focus on the possible cardiac problems of intense sport, and that he/she can read the 12-lead ECG.
Step 2 follows step 1 in case of positive findings in the medical history (personal or family history) or in the diagnostic tests of the first step. These further evaluations and investigations are the concern of a cardiologist. The tests in step 2 are chosen according to the type of positive finding.
These Recommendations should be offered to the athletes with an explanation of the tests performed and the results that can be expected, and it should be clear that it is a voluntary participation for the athlete. Therefore his/her participation in the screening should be preceded by the signing of a form stating the written and informed consent and his/her right not to know should be respected in the case of refusal. Most recently, shortly after the acceptance of the Lausanne Recommendations, both the European Society of Cardiology [98] and the American Heart Association [99, 100] published their recommendations. The European Society of Cardiology report recommendations coincide with the Lausanne recommendations (including the use of a 12-lead ECG), whereas the Bethesda Conference discussed the use of an ECG, but felt it was currently inappropriate to advise for use in the United States.
Limitations of the study
Several limitations in this study need to be specified. The definition of an athlete is very vague, without any quantitative values. Competition does not have a quantitative definition either.
The most important limitation however is that SCD in young athletes as reported in the published and studied papers is certainly underestimated. Most of the events occur in youth potentially involved in sports activities, which are not reported in the literature. SCD is therefore likely to have comprised more than the 1101 athletes in the 38-year period across the world, which we reported. The lack of national or international registers and the uncertainty of the number of athletes involved forms the basis of this problem. An effort to inventory all cases of SCD in the future seems mandatory.
A bias resides in the fact that some articles do not give the precise age of every case reported, but sometimes only an age range for the whole group considered.
Certain sports are under-reported in the articles studied, such as cycling and rowing/canoeing. There are newer articles on cycling [101], which show significant numbers as reported to the smaller groups concerned. The International Cycling Union Cardiology Subcommission reports 14 competitive cyclists with major life-threatening cardiovascular problems. The athletes had trained and participated in competition for at least 5 years. They all seem to have developed an acquired form of right ventricular electrical instability.
Despite these limitations, this article tries to report facts and draw conclusions and cannot provide a final answer, but may provide a uniform format to help diminish this mortality. Further studies of efficacy are needed.
Conclusion
Sudden death in athletes is a serious problem that requires serious attention. The vast majority of these sudden deaths are caused by underlying cardiovascular diseases. Therefore, the general idea that most sudden deaths in sports are related to doping is contradicted by the large numbers of sudden deaths related to underlying cardiovascular diseases.
The importance of the group of athletes suffering SCD under 18 or even 16 years of age is to be noted, and a serious screening should be offered to teenagers training and competing at a high level.
Premature atherosclerosis in young athletes leads to death in a surprisingly large group of competitive athletes, when it was long thought to be a cause of death almost exclusively concerning older athletes.
The large variety of PPSP and the variability of persons using them prevent a serious evaluation of their efficacy. This evaluation would benefit from unified preparticipation recommendations, for which we propose the Lausanne Recommendations.
Footnotes
Appendix
Members of the IOC ad hoc working group on Sudden Cardiac Death in Athletes:
Dr P. Schamasch, IOC Medical and Scientific Director, Lausanne, Switzerland
Dr. E.J. Meijboom, Professor of Congenital Cardiology, CHUV, Lausanne, Switzerland
K. Bille, Resident Pediatrics, Thesis on SCD in Athletes, CHUV, Lausanne, Switzerland
Dr J. Brenner, Professor of Pediatric Cardiology, Johns Hopkins, Baltimore, USA
Dr D. Corrado, Director of Cardiology Laboratory, Padua, Italy
Dr J. Dvorak, FIFA Chief Medical Officer, Zurich, Switzerland
D. Figueiras, Department of Sports Sciences, Lausanne, Switzerland
S. Greinig, IOC Manager of Medical Program, Lausanne, Switzerland
Dr J. Hoogsteen, Head of Training Centre Sports Cardiology, Veldhoven, the Netherlands
Dr L. Kappenberger, Professor of Cardiology, Head of Department, Lausanne, Switzerland
Dr W. McKenna, Professor, Director of Heart Hospital, London, UK
Dr F.J. Meijboom, Cardiologist, Thoraxcentre, Rotterdam, the Netherlands
D. Oswald, Lawyer, Director of International Centre for Sports Studies, Neuchâtel, Switzerland
Dr L. Rivier, Toxicologist, Lausanne, Switzerland
Dr P. Sangenis, Cardiologist, IOC MC Director Institute in Sports Medicine, Buenos Aires, Argentina
D. Sprumont, Lawyer, Director Institute of Health Law, Neuchâtel, Switzerland
Dr G. Theine, Professor of Pathology, Director Institute of Pathological Anatomy, Padua, Italy
Dr M. Zorzoli, International Cycling Union Health Manager, Aigle, Switzerland.