
Abstract
Objective
To investigate whether cardiovascular mortality related to obesity could be modified by physical activity.
Design
Mortality follow-up.
Setting
Population study.
Participants
Participants in a health survey: 34 868 women and 32 872 men free from known cardiovascular disease or diabetes at baseline.
Main outcome measures
Total cardiovascular mortality.
Main results
During 16 years of follow-up, 3026 women and 3526 men had died from cardiovascular causes. In middle age, obesity [body mass index (BMI) of 30 or higher] was associated with increased risk of cardiovascular death, but the association weakened with age. After 70, there was no association between BMI and cardiovascular death. At all ages, a lower level of physical activity was associated with a higher cardiovascular mortality. In women with high physical activity, indicated by at least 30 min of moderate to vigorous activity more than once a week, cardiovascular mortality was only slightly higher in the obese compared to lean women (adjusted relative risk, 1.27; 95% confidence interval, 0.80–2.00). In men with high physical activity, cardiovascular mortality was, however, significantly higher among the obese (relative risk, 1.62; 95% confidence interval, 1.09–2.40). In both genders cardiovascular mortality was substantially higher in obese people who reported no regular physical activity compared to obese people with a high level of physical activity.
Conclusion
In obese women, being highly active may, to a large extent, compensate for the risk-increasing effect of being obese, whereas in obese men who engage in a high level of physical activity, the risk of cardiovascular death may be higher than in lean and equally active men.
Introduction
The increasing prevalence of obesity and physical inactivity poses major public health concerns, not only in Western countries, but also on a global scale [1, 2]. In the United States [3], two-thirds of the adult population are classified as overweight and the situation in some European countries is equally alarming [2, 4, 5]. There is convincing evidence that obesity increases the risk for cardiovascular disease [6], whereas physically fit individuals appear to be protected [7]. It has been suggested that obese people who exercise regularly may also benefit from the protection provided by physical activity; thus, their cardiovascular risk may not differ from that of lean people with a similar level of physical activity.
Whether physical activity compensates for the higher risk of cardiovascular disease that is associated with obesity remains a controversial issue and therefore, we assessed the associations of body mass index and physical activity with cardiovascular mortality in a large prospective study of the general population. In particular, we examined whether high physical activity in obese people may provide protection against cardiovascular death.
Materials and methods
In Nord Trøndelag County in Norway, adults 20 years of age and older were invited to participate in a health survey (the HUNT Study) in 1984. Among 85 100 eligible individuals, 75 058 (88.2%) accepted the invitation. They filled in a questionnaire that was included with the invitation and subsequently attended a clinical examination, where they received a second questionnaire that was to be returned from home. The study has been described in detail elsewhere [8]. Briefly, information included past and present smoking, self-reported physical activity and the clinical examination included standardized measurements of blood pressure, body height and body weight.
We excluded 6719 participants who had a history of myocardial infarction or stroke, known angina pectoris, or known diabetes mellitus. In addition, 387 participants were excluded due to missing information on height or weight. Thus, 67740 (34 868 women and 32 872 men) participants were included in the analysis of body mass index and cardiovascular mortality. Information on physical activity was collected from the second questionnaire, and among the 67 740 participants who were followed up for cardiovascular mortality, 54 284 (27 769 women and 26 515 men) had responded to the questions on physical activity.
The mortality follow-up was approved by the regional committee for ethics in medical research and by the Norwegian Data Inspectorate.
Body mass index
Body mass index (BMI) was calculated as body weight (in kg) divided by the square of the height (in metres). BMI was further subdivided into five categories: less than 18.5 (extremely lean), 18.5–20.9 (very lean), 21–24.9 (lean), 25–29.9 (overweight) and 30 and higher (obese).
Physical activity
The participants were asked about their average frequency of physical exercise in a week, with five response choices (0, < 1, 1, 2–3, ≥ 4 times). Those who reported exercising once a week or more were also asked about the average duration (four categories: < 15, 15–30, 30–60, > 60 min) and intensity (three categories: light, moderate, vigorous) of the activity, and a composite score of frequency, duration and intensity was constructed [9] and found to correlate well with physical fitness [10]. Based on the score, participants were divided into four separate categories. One group consisted of those who reported no regular physical activity, and the others were divided into three groups of equal size depending on their activity score. The level of physical activity in these groups was classified as low, medium or high.
End points
The mandatory reporting of deaths to the Cause of Death Registry in Norway constitutes the basis for the coding of underlying cause of death. Mortality follow-up is virtually complete [11]. In this study, the primary end point was deaths caused by cardiovascular disease [International Classification of Diseases (ICD) 9: 390–459; ICD 10: I 00-I 99]. Specific emphasis was given to deaths from ischaemic heart disease (ICD 9: 410–414; ICD 10: I 20-I 25) and stroke (ICD 9: 430–438; ICD 10: I 60-I 69).
Statistical analysis
BMI was used as a measure of obesity and the participants were grouped into the five categories mentioned above. Person-years were calculated from the date of attendance until the date of death, or until the end of follow-up, 31 December 2003, whichever came first. Relative risks were calculated as the rate of death among participants within a given BMI category compared with the rate of death in the reference category (BMI between 21.0 and 24.9). Similarly, we calculated the rate of death among participants within a given level of physical activity compared with the rate of death in the reference category (high physical activity). In relation to BMI, we first examined the association with cardiovascular mortality and, specifically, with deaths from ischaemic heart disease and stroke. We used the Cox proportional hazards model to adjust for age (5-year categories) and other potentially confounding factors, including smoking status (never, former, current), ever use of blood pressure medication, use of alcohol (frequency in the past 2 weeks), marital status, and level of education (three levels).
For the combined effect of BMI and physical activity on cardiovascular mortality, we grouped physical activity into the four categories indicating activity level: high, medium, low or no activity, and BMI into four categories (less than 21, 21.0–24.9, 25.0–29.9 and 30 and higher). In the combined analysis, lean participants (BMI between 21.0 and 24.9) who reported high physical activity were used as reference, and we compared the death rates from cardiovascular disease in combinations of BMI and physical activity to that in the reference group.
Statistical analyses were conducted with the use of SPSS software, version 13.0 (SPSS Inc., Chicago, Illinois, USA) and all reported P values are two-sided.
Results
During 16 years of follow-up (more than 1 million person-years), 3026 women and 3526 men had died from cardiovascular disease. In women, 1202 deaths were caused by ischaemic heart disease and 994 were caused by stroke; in men, 1923 died from ischaemic heart disease and 771 from stroke.
Body mass index and cardiovascular mortality
The association between BMI and cardiovascular mortality displayed similar age-dependent patterns in men and women (Tables 1 and 2). In the age group younger than 60 years at baseline, the adjusted relative risk of cardiovascular death among obese men (BMI, 30 or higher) was 2.37 (95% confidence interval 1.88–2.98), compared to lean men (BMI, 21.0–24.9). In women, the corresponding relative risk associated with obesity was 2.60 (95% confidence interval 1.86–3.65).
In the older age groups (60–69 years and 70 years and older), the association with obesity was substantially weaker (Tables 1 and 2). Compared to lean men, the adjusted relative risk of cardiovascular death among obese men 60–69 years of age was 1.54 (95% confidence interval 1.28–1.86), and in women the corresponding relative risk was 1.37 (95% confidence interval 1.14–1.66).
Among obese men 70 years and older (Table 1), the relative risk of cardiovascular death was 1.14 (95% confidence interval 0.96–1.36), and in women 70 years and older (Table 2) there was no association with cardiovascular deaths (relative risk, 0.97; 95% confidence interval, 0.85–1.10) related to obesity.
At the lower end of BMI (extremely lean; less than 18.5), cardiovascular mortality was consistently higher than in the reference group. It is possible that a low BMI could be a result of serious pre-clinical disease and that the results could reflect so-called ‘reversed causality’. We explored this possibility by excluding the first 5 years of follow-up, but the estimates remained nearly unchanged. After excluding the first 10 years, however, the increased risk related to very low BMI was fully attenuated in women, but not in men (data not shown).
Physical activity and cardiovascular mortality
We examined the association between level of physical activity and risk of dying from cardiovascular causes (Table 3). In both men and women, and in all age groups, those who reported no physical activity had a higher risk of cardiovascular death than those who reported a low, medium or high level of physical activity. The risk increase displayed a gradual pattern from the most to the least physically active. This was apparent not only for total cardiovascular mortality, but also for deaths specified as due to ischaemic heart disease and stroke.
In men who reported no physical activity, the multi-variable relative risk of cardiovascular death was 1.32 (95% confidence interval 1.18–1.48), compared to men in the high activity group. Moreover, the results showed a gradual increase in cardiovascular mortality with decreasing level of physical activity (P trend < 0.001). Among women who reported no physical activity, the adjusted relative risk was 1.43 (95% confidence interval 1.25–1.63), compared to women with high physical activity.
Body mass index (BMI) in men and relative risk (RR) of cardiovascular death (CVD), and specifically, deaths from ischaemic heart disease (IHD) and stroke during 16 years of follow-up
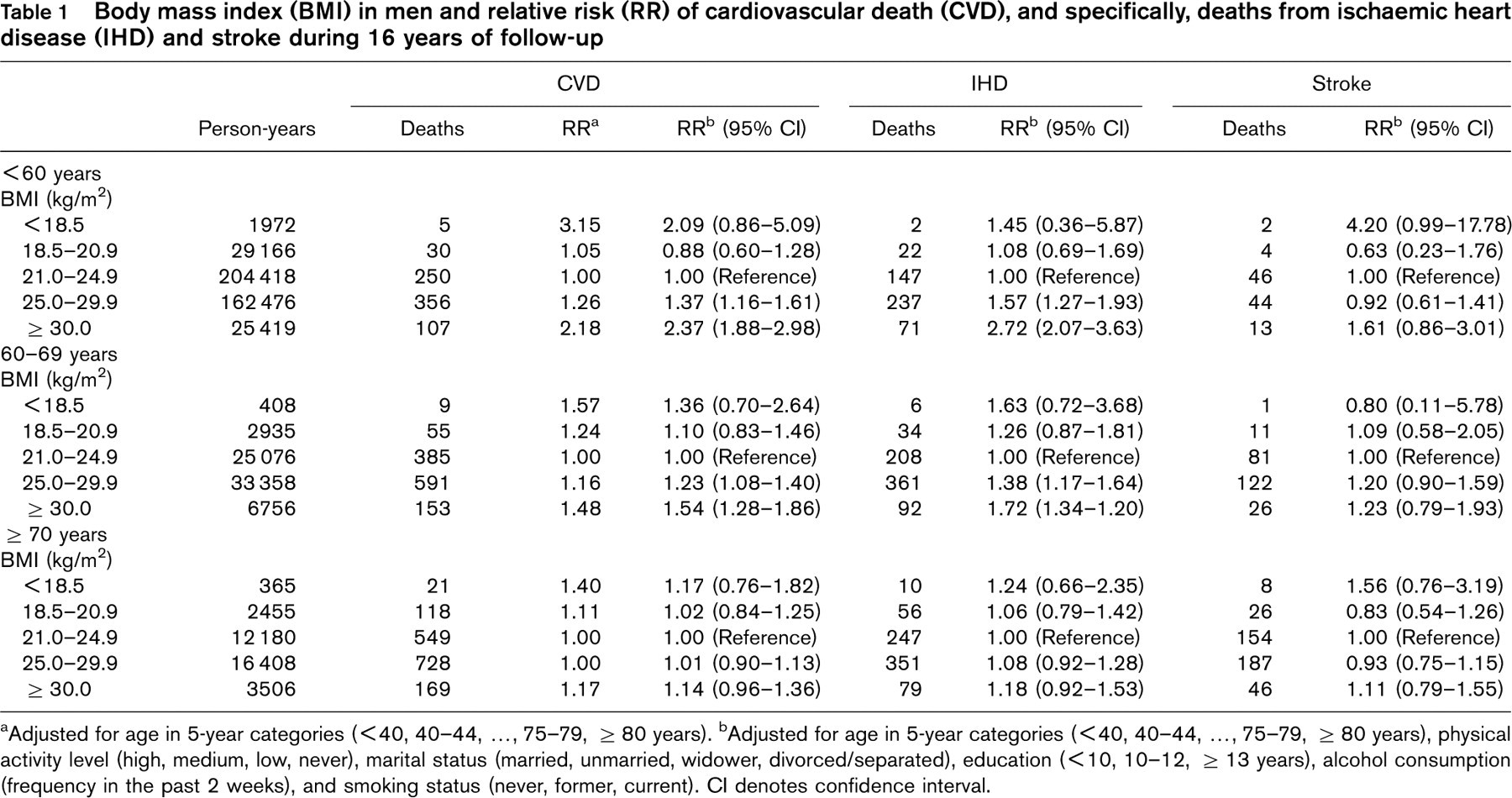
aAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years).
bAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years), physical activity level (high, medium, low, never), marital status (married, unmarried, widower, divorced/separated), education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency in the past 2 weeks), and smoking status (never, former, current). CI denotes confidence interval.
Body mass index (BMI) in women and relative risk (RR) of cardiovascular death (CVD), and specifically, deaths from ischemic heart disease (IHD) and stroke during 16 years of follow-up
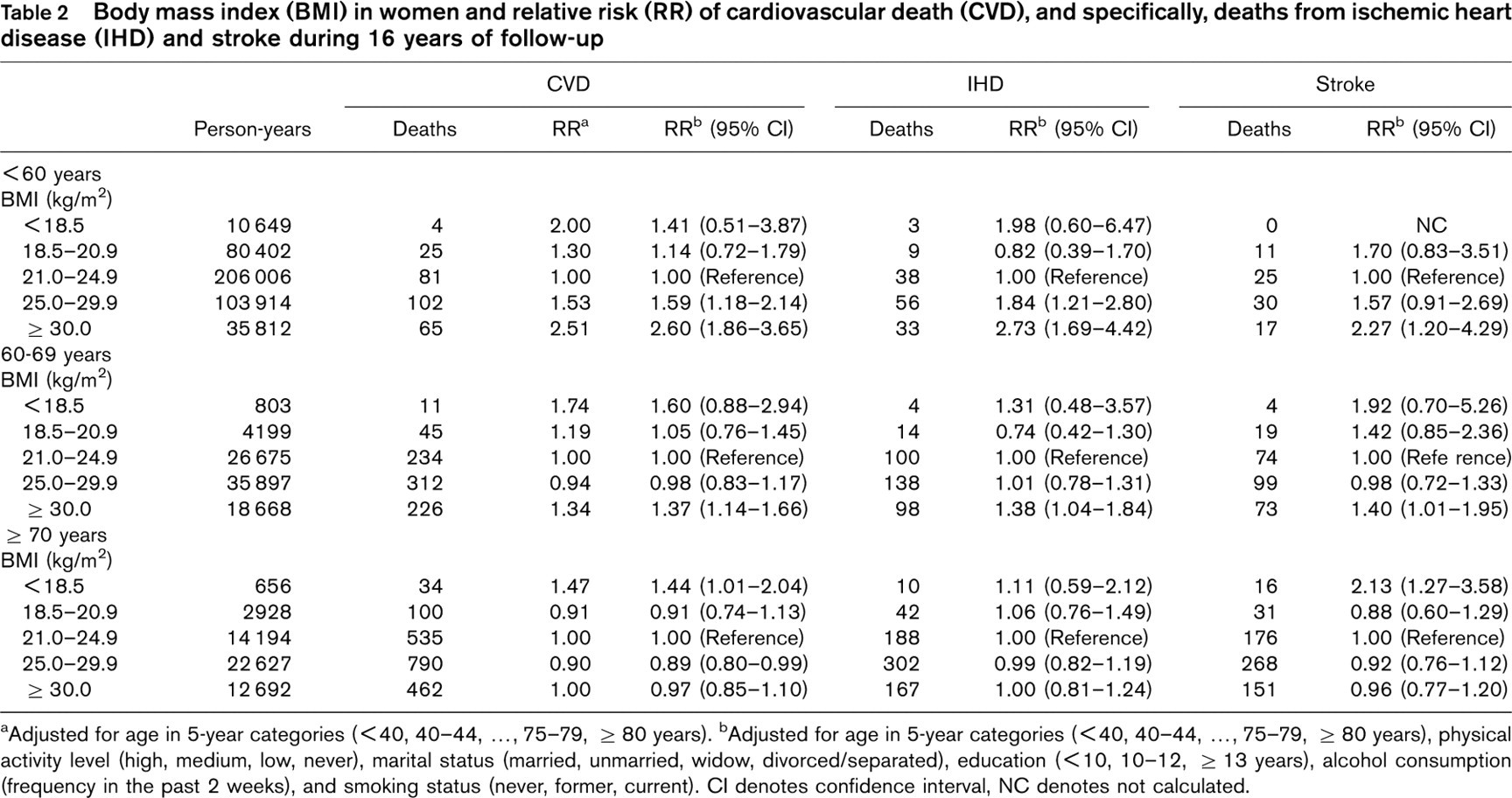
aAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years).
bAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years), physical activity level (high, medium, low, never), marital status (married, unmarried, widow, divorced/separated), education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency in the past 2 weeks), and smoking status (never, former, current). CI denotes confidence interval, NC denotes not calculated.
Level of physical activity in men and women and relative risk (RR) of cardiovascular death (CVD), and specifically, deaths from ischemic heart disease (IHD) and stroke during 16 years of follow-up
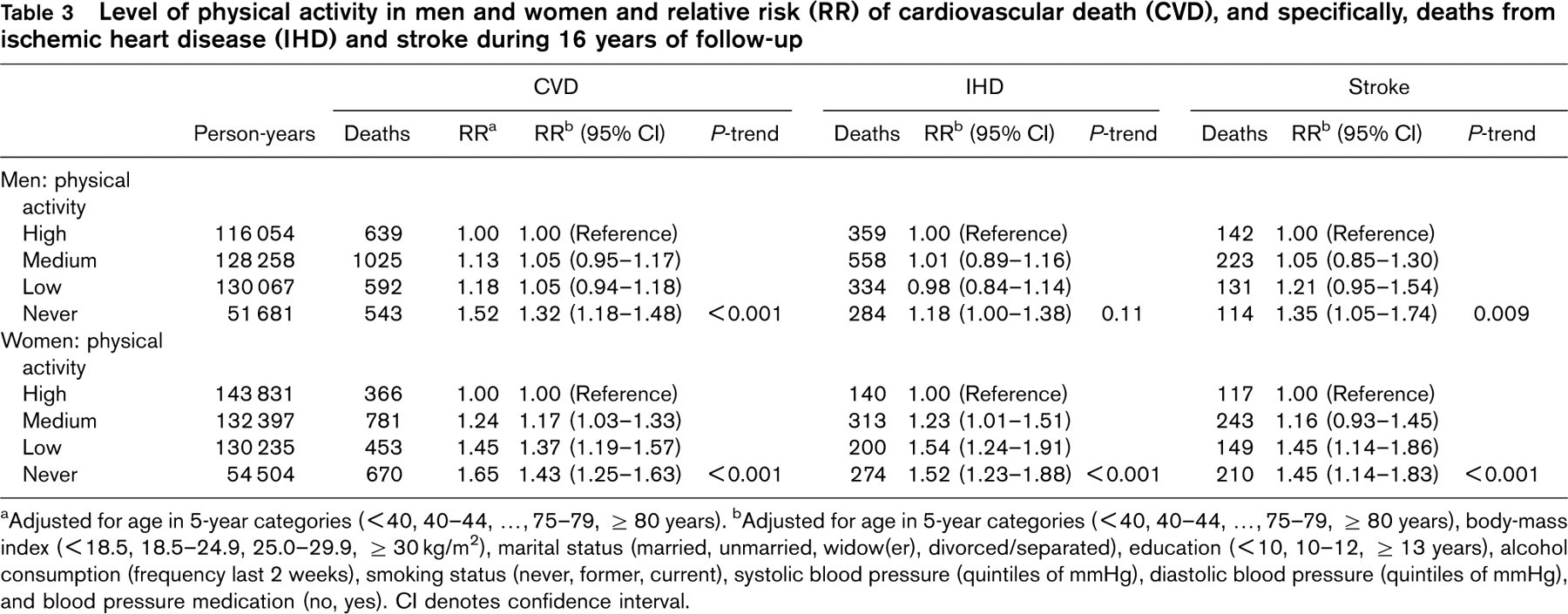
aAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years).
bAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years), body-mass index (< 18.5, 18.5–24.9, 25.0–29.9, ≥ 30 kg/m2), marital status (married, unmarried, widow(er), divorced/separated), education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency last 2 weeks), smoking status (never, former, current), systolic blood pressure (quintiles of mmHg), diastolic blood pressure (quintiles of mmHg), and blood pressure medication (no, yes). CI denotes confidence interval.
Also in women, the association of physical activity and cardiovascular mortality displayed a linear trend (P trend < 0.001).
Combined effect of obesity and physical activity
We examined the combined effects of BMI and physical activity on total cardiovascular mortality (Table 4). Since there was no association between obesity and cardiovascular mortality among individuals who were 70 years of age or older, this analysis was restricted to those who were younger than 70 years of age.
Among women who reported a high level of physical activity, cardiovascular mortality was fairly similar at all levels of BMI. Compared to the reference group of lean women with high physical activity, the risk of cardiovascular death in obese women with high physical activity was only slightly higher (adjusted relative risk 1.27, 95% confidence interval 0.80–2.00). In men who reported high level of activity, the corresponding pattern differed from that of women. Compared to lean men with high physical activity, cardiovascular mortality increased with increasing BMI, and in obese men who also reported high physical activity, the relative risk of cardiovascular death was 1.62 (95% confidence interval 1.09–2.40).
On the other hand, cardiovascular death in obese men and women with high physical activity was substantially lower than among other obese people who reported no physical activity. The results showed that increasing BMI combined with decreasing level of physical activity was associated with a consistently higher risk of cardiovascular death (Table 4).
Multivariable a relative risks of cardiovascular death according to joint categories of body mass index (BMI) and physical activity. Men and women 20–69 years of age at baseline
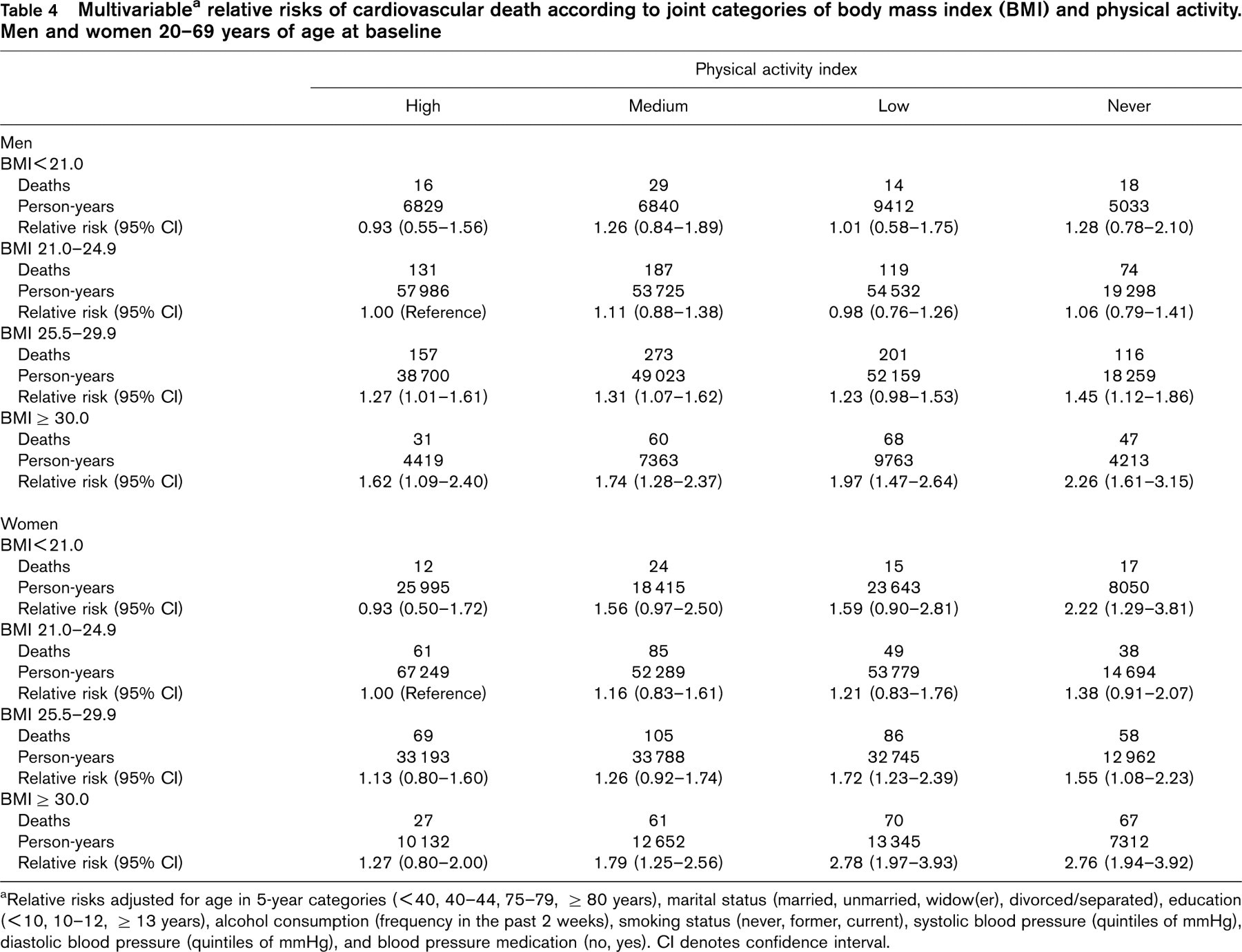
aRelative risks adjusted for age in 5-year categories (< 40, 40–44, 75–79, ≥ 80 years), marital status (married, unmarried, widow(er), divorced/separated), education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency in the past 2 weeks), smoking status (never, former, current), systolic blood pressure (quintiles of mmHg), diastolic blood pressure (quintiles of mmHg), and blood pressure medication (no, yes). CI denotes confidence interval.
Discussion
In this general population of adults 20 years and older, obese women younger than 70 years of age, who reported high level of physical activity, had a risk of cardiovascular death that was only slightly higher than that of lean women with a similar high level of activity. However, the risk of cardiovascular death in obese men who reported high activity was moderately but significantly higher than that of lean, equally active men.
The results of another prospective study suggested that physical fitness could remove completely the excess cardiovascular mortality associated with being overweight [7]. A report from the Lipids Research Clinics Study [12], however, showed that high BMI and low physical activity were independently associated with higher cardiovascular mortality, but the results did not support the possibility that high physical activity may counteract the risk-increasing effect of being obese. A similar conclusion was drawn in a report from the Nurses' Health Study [13]. In that study, the investigators found that women who engaged in regular physical activity at a relatively moderate level (brisk walking for 30 min/day) had lower total mortality than those who reported no physical activity. However, obese women who reported a high level of physical activity had an excess risk of cardiovascular death compared to lean women with similar level of activity. In the Cancer Prevention Study II [14], the investigators reported similar results for mortality from all causes: obese men and women who reported high activity were at higher risk of dying than lean men and women who also reported high activity. In another prospective study based on Norwegian data, obese men who were physically active had an excess mortality from all causes compared to lean, physically active men [15]. However, results on cardiovascular mortality were not specified in that study.
Our results also showed that the association between obesity and cardiovascular mortality strongly depended on the age of the participants. Obesity in age groups younger than 60 years at baseline was strongly associated with higher risk of cardiovascular death, both in men and women, but the strength of the association declined with increasing age. Thus, the association with obesity was substantially weaker in the age group 60–69 years, and for those who were 70 years or older at baseline the association was absent in both men and women.
In men younger than 60 years of age, obesity was associated with an increase in stroke mortality, but the association was not statistically significant. In older age groups of men, there was no clear association between obesity and stroke. In women younger than 70 years of age, the results showed a clear positive association between obesity and stroke mortality, but in the age group 70 years and older, there was no association between obesity and deaths from stroke in women. Similar results have previously been reported from another Norwegian cohort study [16].
The Cancer Prevention Study II in the USA showed that the strength of the association between obesity and mortality from all causes declined with age, but the associations remained positive, but moderate, in older age groups [6]. In a previous study of that population [17], the strength of the association between BMI and cardiovascular mortality also declined with age, in a similar manner as for deaths from all causes. In two other large cohort studies from Norway the optimal BMI related to total mortality increased with increasing age of the participants [18, 19].
Attempts to interpret these findings have listed many different possibilities [20]. One example is selective survival, where individuals with low tolerance for obesity tend to die before they reach old age. Another possibility could be effects related to different birth cohorts: the results could be attributed to different conditions or lifestyles associated with the time of growing up [21]. However, it is also possible that excess fat may have less effect on mortality in older than in younger people and, also, residual confounding by other factors cannot be excluded.
In relation to cardiovascular disease, BMI and blood pressure may exert their effects along related causal pathways and therefore, we did not adjust for blood pressure in the statistical analyses. However, in a separate analysis, we observed that additional adjustment for blood pressure substantially attenuated the association between obesity and cardiovascular deaths. A similar observation was made in another large cohort study in Norway [16], where the investigators showed that adjustment for systolic blood pressure attenuated the positive association between BMI and cardiovascular mortality. These results confirm that effects on cardiovascular mortality related to obesity may, at least partly, be mediated by blood pressure.
In this study, we constructed a physical activity index based on the responses to three questions. One was related to usual frequency (in a week) of physical activity, the second to duration (in minutes) and a third question was related to intensity (light, moderate or vigorous) of the physical activity [10]. We found that physical inactivity was associated with increased risk of cardiovascular death and, specifically, with deaths from ischaemic heart disease and stroke, in both men and women. The association displayed a gradual pattern, with increasing risk with decreasing level of physical activity. A high level of physical activity in these data was indicated by a frequency of more than once a week, usual duration of at least 30 min, and moderate to vigorous degree of intensity. Nonetheless, the major difference in cardiovascular mortality was between people who reported a low to moderate level of physical activity and those who reported no activity. These results are supported by several studies that have shown that those who engage in physical activity are at reduced risk of premature death from cardiovascular causes compared to those who report no activity, and by convincing evidence that cardiorespiratory fitness is a strong predictor for cardiovascular health [7, 12, 13, 15, 22].
In conclusion, cardiovascular mortality in obese women with a high level of physical activity was only slightly higher than that of lean, physically active women, suggesting that high activity in women, to a large extent, may compensate for the risk-increasing effect of being obese. In obese men who engage in high level of physical activity, the risk of cardiovascular death was, however, moderately higher than in lean and equally active men. The results support the hypothesis that cardiovascular health in obese individuals will benefit from physical exercise, and that, to some extent, physical activity may counteract the adverse effects of obesity.