
Abstract
Background
Evidence for the proper management of ischemic heart disease (IHD) in the general population is well established, but recommendations for physical activity and competitive sports in these patients are scarce. The aim of the present paper was to provide such recommendations to complement existing ESC and international guidelines on rehabilitation and primary/secondary prevention.
Design and methods
Due to the lack of studies in this field, the current recommendations are the result of consensus among experts. Sports are classified into low/moderate/high dynamic and low/moderate/high static, respectively.
Results
Patients with a definitive IHD and higher probability of cardiac events are not eligible for competitive sports (CS) but for individually designed leisure time physical activity (LPA); patients with definitive IHD and lower probability of cardiac events as well as those with no IHD but with a positive exercise test and high risk profile (SCORE>5%) are eligible for low/moderate static and low dynamic (IA-IIA) sports and individually designed LPA. Patients without IHD and a high risk profile + a negative exercise-test and those with a low risk profile (SCORE<5%) are allowed all LPA and competitive sports with a few exceptions.
Conclusions
Individually designed LPA is possible and encouraged in patients with and without established IHD. Competitive sports may be restricted for patients with IHD, depending on the probability of cardiac events and the demands of the sport according to the current classification.
Scope of the article
Evidence for the proper management of ischaemic heart disease (IHD) in the general population is well established. However, recommendations for physical activity and participation in competitive sports for people with IHD are relatively scarce.
The targets of these recommendations (termed ‘active individuals with IHD’ throughout) are: (1) individuals with IHD engaged in regular exercise training, including those participating in official sports competitions (competitive sports); but also (2) those being physically active in leisure-time activities, including recreational sports.
Classification of sports (adapted and modified after [8])
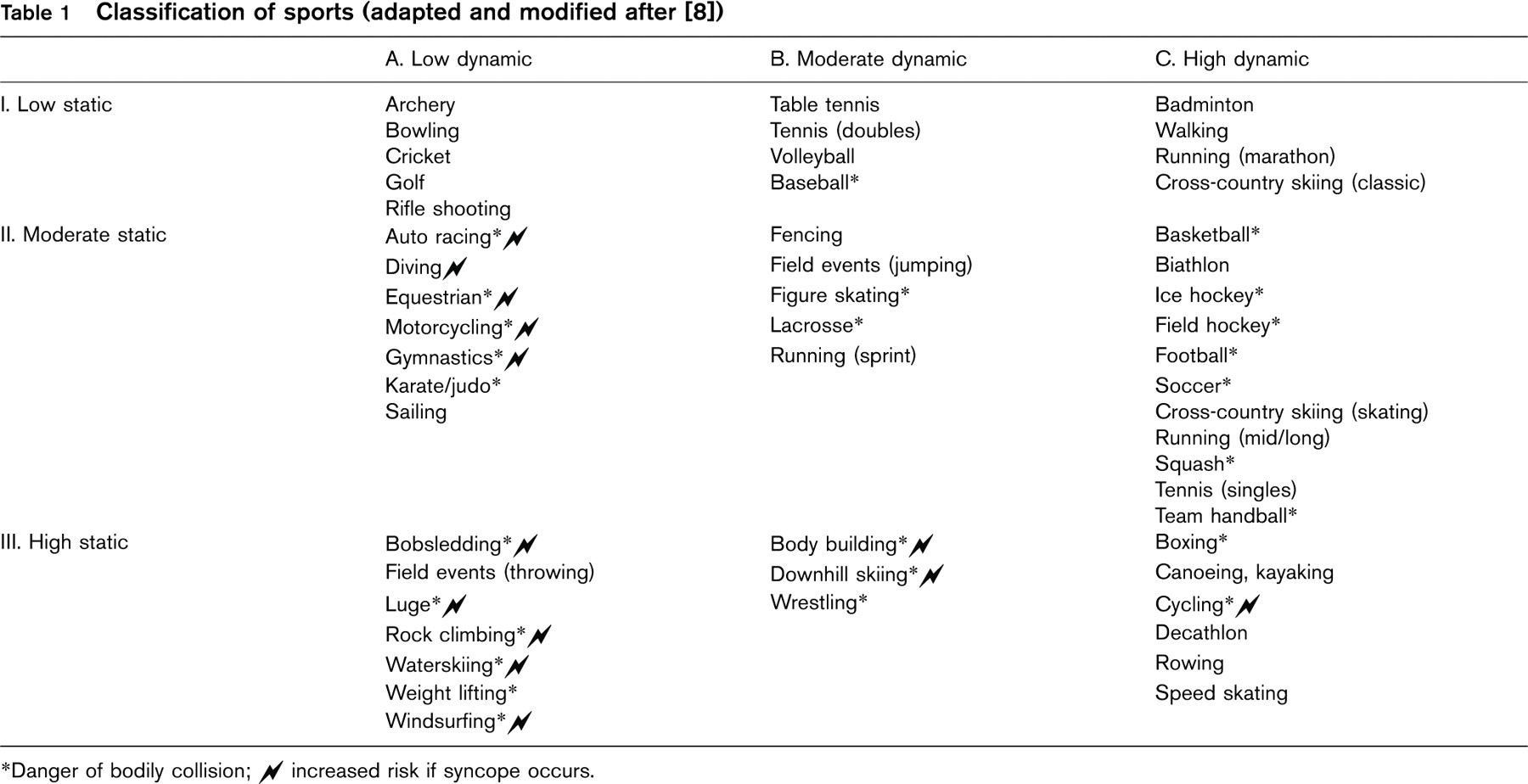
∗Danger of bodily collision; N increased risk if syncope occurs.
These recommendations aim to complement the current European Society of Cardiology (ESC) recommendations on cardiac rehabilitation [1], primary/secondary prevention [2] and also the ESC recommendations [3] and the Bethesda recommendations [4], both specifically targeting athletes.
Medical treatment of ischaemic heart disease falls outside the scope of this article, and is included in the guidelines for treatment of stable angina from the ESC [5]. Due to the prevalence of cardiovascular diseases, athletes are commonly described as ‘young athletes’ (< 35 years) and ‘older athletes’ (≥ 35 years). To comply with the majority of other cardiovascular literature, we are using the cut-off point of 35 years. However, in competitive sports the term ‘Master athletes’ is used, and refers to the age of 40 years and older [6].
Please note that due to lack of studies in this field, the level of evidence for these recommendations are low (level of evidence C) with a few exceptions (unstable angina) and are the results of consensus among experts [7].
Also please note that we have used the classification of sports used in the Bethesda recommendations (Table 1) [8] and in the ESC recommendations [7], published in 2005.
Introduction
Epidemiology
Ischaemic heart disease (IHD) is the leading cause of death in the Western world [9]. The prevalence of IHD increases with age (for men 7% at ages 40–49 years, 13% at ages 50–59 years and 16% at ages 60–69 years; and in women 5, 8 and 11%, respectively) [10]. Premature IHD in young subjects is uncommon, with a prevalence of about 2% below 40 years of age according to the GISSI data [11, 12]. In addition, the prevalence of clinically asymptomatic IHD (silent ischaemia) is estimated to be 2–4% in the general population and 10% in individuals with two or more risk factors for IHD [13].
IHD also accounts for most exercise-related sudden deaths [14], typically above the age of 35 years. In fact, sudden cardiac death (SCD) is often the initial coronary event in patients with either silent or symptomatic IHD [15].
Various data suggest a future increment in the incidence of IHD, as risk factors for IHD, such as obesity and diabetes mellitus, are increasing rapidly [16], even in younger populations. Efforts to educate the general population to lifestyle changes may contribute to a more active population. More people suffering from IHD therefore could potentially take part in sports activity in the future. Thus, physicians will need more knowledge of effective training programmes for subjects with coronary abnormalities, including the effects of these programmes on current and emerging risk factors for cardiovascular disease. An attempt to make recommendations for the management of active subjects with IHD and/or classical risk factors for IHD therefore seems warranted.
Pathophysiology
Ischaemic heart disease is typically caused by progressively developing atherosclerosis. It is due to a combination of several risk factors closely related to lifestyle and familial disposition. Classical non-modifiable risk factors include age, male gender and family history of IHD. Major modifiable risk factors are smoking, diabetes mellitus, hypertension (> 140/90 mmHg), hyperlipidaemia (total cholesterol > 5.2 mmol/l or 200 mg/dl), physical inactivity (less than 3 × 1 h/week of brisk walking) and stress. Predisposing risk factors are also obesity in childhood/young adulthood and psychosocial factors [17].
The patient eventually may develop symptoms due to progressive disease, namely angina pectoris, but many patients with IHD also remain symptom-free [18], that is, have silent ischaemia. However, a considerable number of myocardial infarctions are not the consequence of a significant stenosis of the coronaries, but are instead caused by rupture of an unstable coronary plaque, possibly during exercise. Another possible cause of SCD in patients with IHD, is exercise-induced ventricular arrhythmias. These are frequently observed during exercise testing, and have been shown to be independent predictors of cardiovascular mortality [19]. Novel risk markers for early detection of atherosclerosis and/or increased risk are now emerging. However, markers such as high-sensitivity C-reactive protein, homocysteine and plasminogen activator inhibitor-1 (PAI-1) are still not routinely recommended.
Non-coronary causes, such as myocardial bridging [20] or drug/substance abuse/doping [21], might be associated with the clinical syndrome of unstable angina, and may cause SCD in athletes/active individuals.
Risks/benefits of exercise
Potential risks of exercise and IHD
The risk for triggering fatal/non-fatal coronary events increases transiently during vigorous physical activity [6]. Several factors potentially contributing to myocardial ischaemia, may be specifically related to the athlete and a high level of competition. However, physical activity at relatively lower intensities may trigger a coronary event in an individual with IHD.
Primarily, the events occur during or after physical activity [14]. Proper warm-up and cool-down phases (5 min of light activity at a reduced intensity) may have an anti-anginal and possibly cardioprotective effect [22].
A circadian periodicity for the time of onset of myocardial infarctions, with a peak in the early morning hours, is well established [23] and is attributed to the similar circadian rhythm of physiological (hypercoagulability and coronary vasoconstriction) and biochemical parameters (early morning rises of plasma catecholamines, cortisol and platelet aggregability) [23]. But overall, the risk associated with regular exercise is relatively small, particularly if that exercise approximates to, or is below, the ventilatory threshold.
Strenuous exercise (corresponding to activity above an individual's ventilatory threshold) increases the release of catecholamines and could induce platelet adhesion/activation [24] with possible thrombotic complications.
Ventricular ectopic beats and tachycardia during exertion may increase myocardial ischaemia and fatal/non-fatal ventricular arrhythmias in active individuals with a underlying IHD.
Thermal stress, for example a hot shower after prolonged exertion, may result in an increased heart rate and arrhythmias [25]. Equally strenuous and/or prolonged physical exertion in the heat, accompanied by an inadequate intake of appropriate fluids, may cause localized sub-endocardial ischaemia, adverse changes in blood coagulation and possibly infarction [26]. In contrast, exercising in cold climates decreases peripheral circulation while increasing metabolic rate and in active individuals with underlying IHD unstable cardiac function may be the result.
In addition, exercising at altitude can carry an increased risk for pulmonary oedema and tachycardia in individuals with underlying IHD [27].
Strenuous exertion may also lead to electrolyte disturbances, for example elevated potassium levels, which can induce fatal or non-fatal ventricular arrhythmias by enhancing cardiac irritability [28].
The abuse of various drugs can be a factor contributing to SCD [21]. Alcohol may cause sudden death by acute respiratory failure or cardiac arrhythmia. Cocaine abuse may cause coronary spasm [29], thrombosis [30] or increased myocardial oxygen consumption [29] by stimulation of alpha-adrenergic receptors, contributing to acute cardiac events [31]. Case reports also describe sudden death in young athletes with no previous known heart disease but who were taking androgenic anabolic steroids [32, 33]. Cardiac hypertrophy or myocarditis were here found at autopsy. However, it is difficult to establish causality in these sporadic cases. The clinical importance of haemostatic system activation shown in confirmed steroid users, with regard to risk of thrombosis, is unclear [34].
Benefits of exercise for IHD
Increasing physical activity is universally recognized as a desired lifestyle modification for improving cardiovascular health. Changing lifestyle with risk factor modification is associated with reduced mortality and morbidity [2]. Specifically, regular aerobic exercise at moderate intensity reduces the risks for fatal and non-fatal coronary events [35–39]. This effect is mediated by effects on most of the classical risk factors, including the components of the metabolic syndrome. Physical activity for a minimum of 30 min three times a week can reduce hypertension and glucose intolerance, improve lipid profile and reduce weight [36, 40].
In addition, regular physical activity at moderate intensity, has specific benefits on the autonomic nervous system and blood coagulation. In patients with IHD, regular physical activity increases maximal physical performance while decreasing the rate—pressure product at identical sub-maximal work intensities, thereby lifting the ischaemia threshold for a given work load. In addition, coronary artery size changes in humans are limited to a small number of recent studies showing angiographic regression relative to controls, but most of these studies have included statins, making it difficult to assess the independent effects of exercise [41, 42]. The effects of exercise on endothelial dysfunction (coronary and peripheral), on the other hand, are highly consistent, and recent studies in this area have brought about a new paradigm on the benefits of regular exercise for patients with ischaemic heart disease [43, 44]. Acute exercise tends to increase thrombogenesis (thrombotic tendency), but regular, chronic exercise of moderate intensity seems to reduce platelet aggregability [45] and decreases the overall risk of thrombosis [46]. The risk of SCD during vigorous physical exertion is lower for those who exercise regularly (at least three times a week for 30 min on each occasion) [47]. However, regular physical exercise, even in highly trained athletes, is not an absolute guarantee for ‘healthy’ coronary arteries.
Summary: safety of exercise
The benefits of regular physical activity by far outweighs the increased relative risk of triggering a coronary event during the exercise session [48]. Thus, the prospective physicians’ health study found that habitual exercise diminished the risk of SCD during vigorous exercise [49].
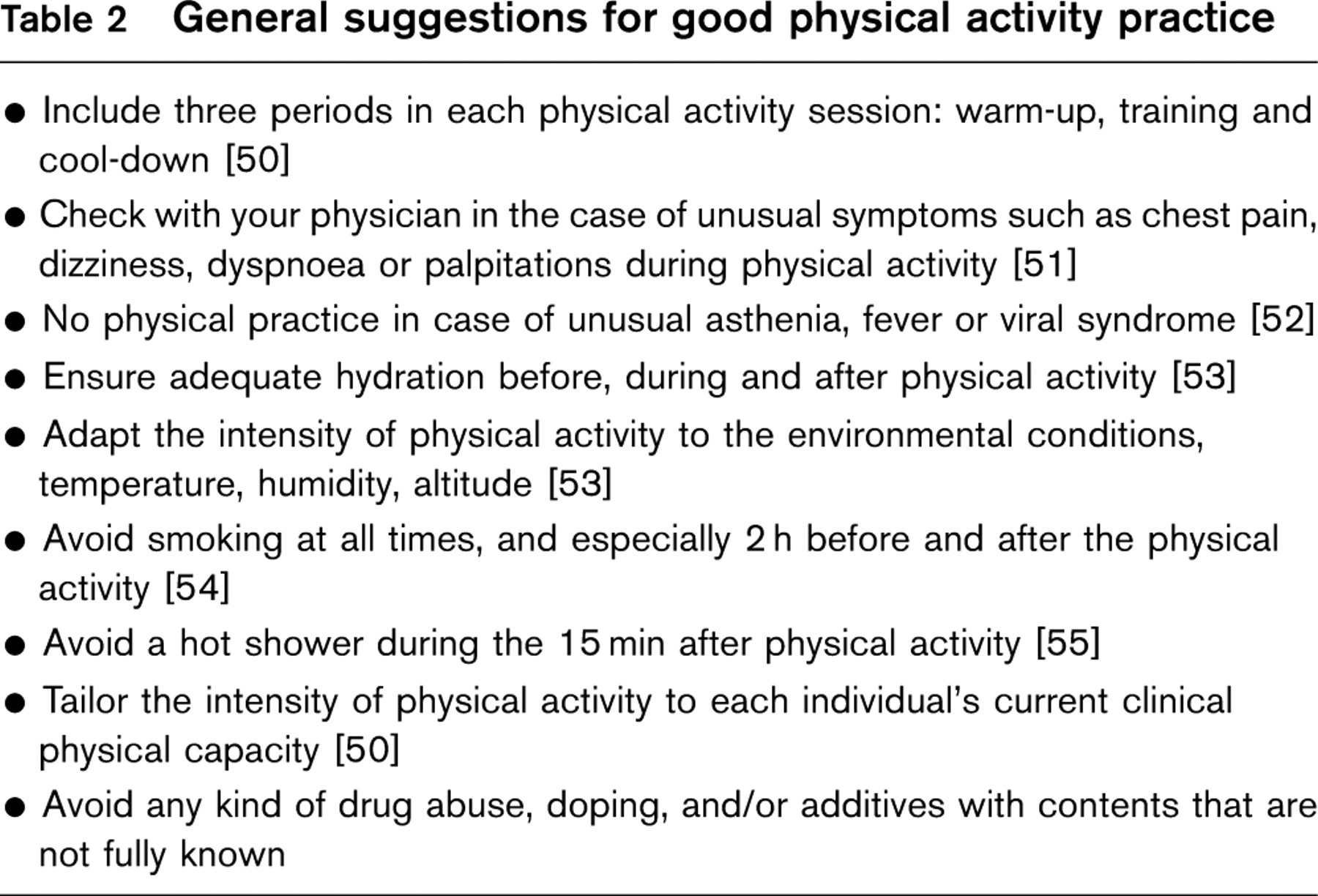
Different types/intensities of physical activity have different effects on the autonomic tone, which may reflect the net results of these activities. The positive benefits of regular physical activity are largely associated with moderate intensity activity that increases vagal tone. In contrast, the potentially negative effects of exercise (as listed previously) are almost exclusively related to high-intensity activity, which typically stimulates sympathetic tone and increases adrenaline, with an increased risk of dysrhythmia in patients with underlying IHD. Consequently it is essential to give instructions to the individual with IHD, who wishes to participate in competitive sports or leisure-time sport activity, on how to be physically active at a safe level of intensity. To minimize risks during physical activity, some general ‘suggestions for good physical activity practice’ should also be applied to each activity session (Table 2) [50–55].
General suggestions for good physical activity practice
Prescription of exercise
It is recommended that exercise is tailored to each athlete/individual in terms of their physical condition, aerobic/anaerobic fitness and local muscular condition. This can vary in athletes/individuals when comparing preseason/off-season condition with that in the competitive season. It is also important that exercise is suited to each individual in terms of its intensity, duration and volume. Individuals and athletes who have not undertaken training for 3–6 months, must physically condition themselves before practising more rigorous physical activity. The activity should be linked to other lifestyle modifications to minimize the cardiac risk. Adequate pre- and post-exercise medical evaluations (follow-up) are essential.
Exercise intensity
As exercise above an individual's ventilatory threshold increases the risk for complications [56], different methods to determine, or rather approximate, the appropriate training intensity may be used. The most widely used methods are measuring aerobic capacity (VO 2 max), heart rate (%HRmax) or rating of perceived exertion (RPE) using the Borg scale [57]. The use of the % of HRmax is dependent on the assumption that the relationship between VO 2 and % of HRmax is linear [22]. The most frequent intensity levels proposed as training guidelines to increase cardiorespiratory fitness (training zone) are 40–85% VO 2 max, corresponding with 64–93% of HRmax [22, 58]. Table 3 outlines the relationship between VO 2 max, %HRmax and RPE [59].
However, the percentage of VO 2 max may vary considerably in relation to an individual's ventilatory threshold, even though the ventilatory threshold is higher in ‘fit' individuals. In established IHD, training should not be above the individual ventilatory threshold, which typically corresponds with 85% of age-related HRmax, but may in fact vary between 50 and 90% of HRmax. Low-fit individuals may demonstrate increases in cardiorespiratory fitness even at exercise intensities at the low to medium end of the proposed training range (i.e. below 70% of HRmax) [22]. In sport activities requiring more strenuous efforts, training may need to be above the ventilatory threshold, moving well into anaerobic metabolism [60]. In individuals with a high level of fitness who need to train and perform at higher intensities, testing at these intensities is vital to ensure safety while minimizing risk. Knowledge of ventilatory and potentially higher anaerobic thresholds is important. The ventilatory threshold may be determined by different methods, including respiratory exchange ratios, measuring blood lactate accumulation and the ‘heart rate deflection point’ [61], during maximal exercise testing [62].
The relationship between percentage of HRmax, rate of perceived exertion (RPE) and %VO 2 max for defining physical activity intensity (adapted from [59])
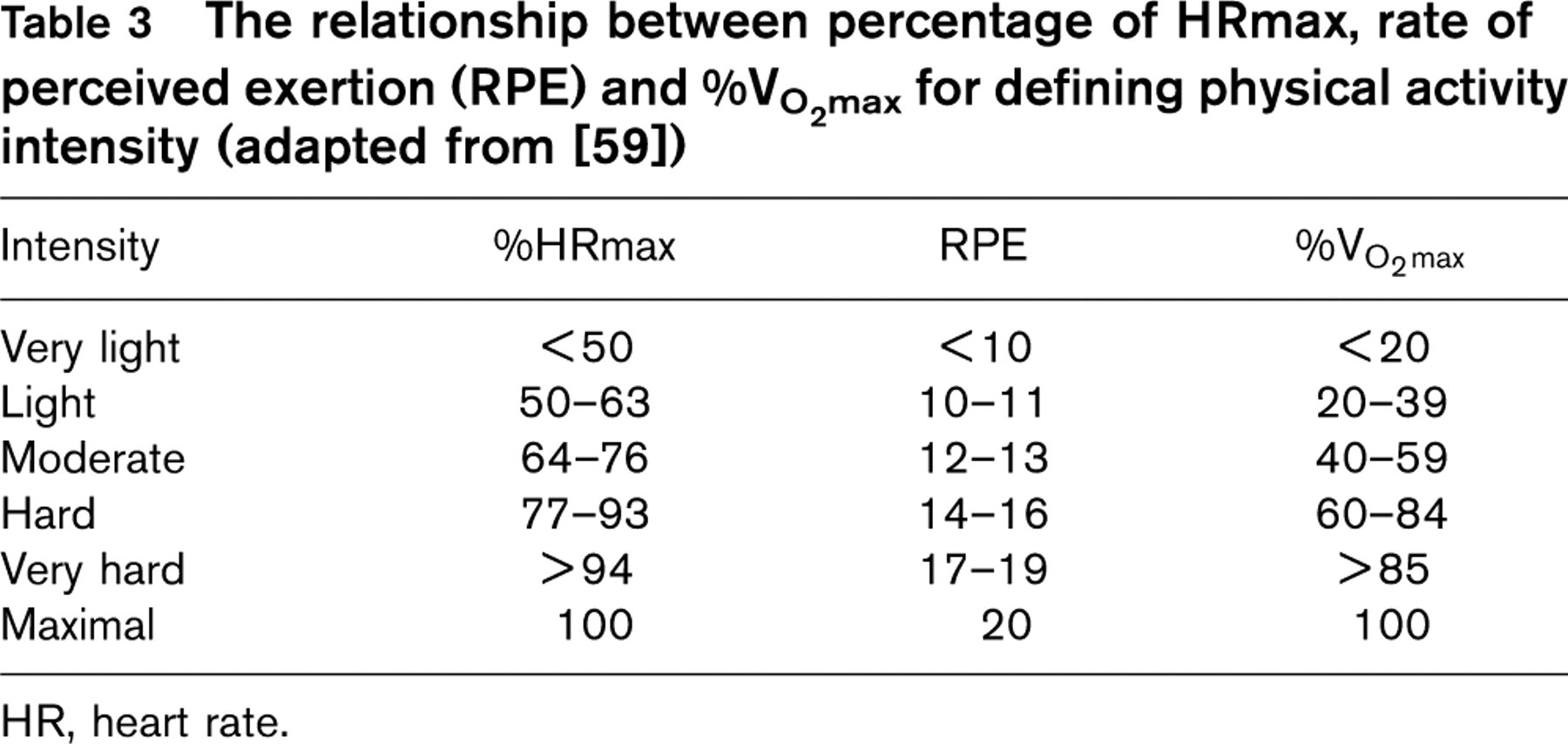
HR, heart rate.
In addition, the evaluation of HR recovery (time and percentage drop in heart rate) may also give valuable information regarding both fitness and indications to alter training regimes. However, in addition to being a marker of training status, faster HR recovery has been shown to be an independent prognostic marker in patients with cardiovascular disease [63, 64].
Blood pressure (systolic) normally increases as exercise intensity increases but often there is minimal change in diastolic pressure. Both heart rate and blood pressure (double product = blood pressure × heart rate) may be monitored during exercise in certain instances. This is especially valuable when there is a need to avoid sudden surges in myocardial O2 demand, reflected by a sharp increase in the double product.
Beta-blockade and exercise
Special consideration has to be given to the patients with IHD on beta-blockade treatment, especially after myocardial infarction. Some studies show that beta-1 selective beta-blockade is associated with decreases of up to 10% in both HR and VO 2 max [65]. Beta-blockade may also change the relationship between HR and VO 2 max [66], but usually the relationship remains linear. Hence, heart rate based on an exercise test while on beta-blockade may generally be applied to prescribe training intensity. As it is recommended for IHD patients to exercise below the ventilatory threshold, it is advisable to determine an individual's ventilatory threshold and then modify the prescribed upper ‘heart rate limit’ to reflect this parameter. Often this heart rate will be lower than expected due to the effect of certain selected beta-blocking agents. An additional option is to use the Borg scale of perceived exertion (RPE) as this parameter appears to be less affected by beta-blockade use. It is recommended that careful note be taken of an individual's RPE rating as it coincides with the appearance of ventilatory threshold during testing. This will allow a more accurate guide towards selecting the correct ‘safe’ exercise intensity.
In addition, in patients with established IHD, the heart rates associated with ischaemia, silent ischaemia, angina and arrhythmia thresholds should be noted from the exercise tests and used to help guide safer exercise prescriptions. It is important that individuals be encouraged to exercise up to 10 beats below the heart rates that correspond with these thresholds. The value of using heart rate monitors to guide individuals towards these safer exercise levels should not be underestimated [22].
In summary, exercise intensity should be prescribed in relation to an individual's cardiorespiratory fitness, his or her intended level of sport activity and their training goals. However, the intensity should be below the ventilatory threshold determined by RPE or %HRmax, and/or kept 10 beats below the anginal/ischaemic/arrhythmia threshold.
Clinical evaluation/risk stratification/recommendations
Listed below are broadly available diagnostic and/or evaluation methods for IHD. For further information we recommend the ESC Guidelines on management of stable angina [5].
Personal history: confirm any family history of IHD/SCD, the presence of symptoms of stable or unstable angina, risk factors for IHD, the type and intensity of physical activity to be undertaken and the measured responses to physical exercise.
Resting 12-lead electrocardiogram (ECG) for detection of ischaemia, arrhythmias and cardiac hypertrophy. Note that ECG interpretation may not be straightforward in individuals trained to a high level.
Physical exercise test, using treadmill or bicycle, for evaluation of symptoms, ST segment changes, arrhythmias, ischaemia and anginal thresholds, exercise capacity and blood pressure/heart-rate responses, including double product [67], as well as prognosis [68].
Echocardiography for evaluation of left ventricular function, structural abnormalities or regional wall motion abnormalities.
Physical or pharmacological (adenosine, dipyridamol, dobutamine) stress with single photon emission computed tomography (SPECT), for detection of regional perfusion defects of the myocardium.
Maximal physical or pharmacological stress with echocardiography or magnetic resonance imaging (MRI), for detection of reversible regional wall motion abnormalities, as a sign of reversible ischaemia.
Coronary angiography for evaluation of luminal coronary stenosis or occlusion in one or more of the main branches or left main stem, coronary flow disturbances or abnormal coronary anatomy.
Twenty-four-hour or longer (Holter) electrocardiographic monitoring for detection of electrical instability or ST—T changes.
Additional, emerging methods of non-invasive assessment of the presence of IHD, such as electron beam computed tomography for detection of coronary calcification [69] or MRI, are not yet in routine clinical practice.
Patients with known IHD
This includes individuals with unstable angina, stable angina, after myocardial infarction (MI), after coronary artery bypass grafting/percutaneous coronary intervention (CABG/PCI) and silent ischaemia.
Risk stratification (adapted from [6, 70])
A subgroup of the low-risk group with a slightly higher risk (intermediate probability for exercise-induced events) has been proposed in earlier guidelines for patients post-MI [70]. However, in the present recommendations the groups are put together into the low-risk group, to comply with the newly published recommendations on sports participation from the ESC Study Group of Sports Cardiology [3], and because the recommendations for sports and leisure-time activity are similar for both groups. Please note that in absolute terms both these groups have a low risk for cardiac-induced events.
Lower-risk group (all below)
Normal exercise capacity on testing, for age and sex, as well as for type of intended activity;
absence of exercise-induced ischaemia during stress testing;
ejection fraction > 50% on echocardiography at rest;
absence of complex ventricular arrhythmias at rest and during 24-h Holter monitoring;
absence of significant coronary stenosis of main coronary arteries following coronary angiography (if performed);
fewer than two risk factors, under control; and
< 55 years of age.
Patients with poor exercise capacity during testing, for age and sex, as well as for type of intended activity; earlier myocardial infarction; absence of exercise-induced ischaemia on stress testing; ejection fraction > 50% on echocardiography at rest; absence of complex ventricular arrhythmias at rest and during 24-h Holter monitoring; absence of significant coronary stenosis of main coronary arteries during coronary angiography (if performed), but possible occluded vessel due to previous MI; and multiple risk factors under control, represents the ‘intermediate’ subgroup.
Higher-risk group
Exercise-induced ischaemia (>1 mm ST depression) on physical exercise test; or
exercise-induced anginal pain, pathological dyspnoea (angina equivalent) or syncope; or
ejection fraction < 50% on echocardiography; or
complex ventricular arrhythmias at rest, at stress or under Holter monitoring; or
significant coronary stenosis of main coronary arteries (> 70%) or left main stem (> 50%) on coronary angiography (if performed);
or poor left ventricular (LV) function on ventriculography, regardless of risk-factor status.
Patients with unstable angina
Defined as recent-onset angina; progressive angina (in frequency, intensity and/or duration); angina at rest; or directly associated with a myocardial infarction [71, 72].
Patients with known IHD and unstable angina have a high risk for future cardiovascular events.
Recommendations Patients with unstable angina are not eligible for competitive sports or any other regular physical activity (level of evidence A).
Patients with stable angina
Angina pectoris is considered as stable if not deteriorating over a prescribed time period (normally several weeks). It typically occurs with increased myocardial oxygen consumption, for example during exercise, temperature changes, emotional stress or hypercirculation [72].
These subjects should be risk stratified as outlined above for known IHD.
During exercise testing, it is important to reach the ventilatory threshold and/or 70–85% of the predicted maximal heart rate for individuals on medical treatment (see previous discussion on beta-blockade), and to aim for the maximal predicted heart rate in others.
Recommendations
Patients with stable angina and a high probability for exercise-induced events are not appropriate for competitive sports. However, after optimal medical and interventional therapy they may be re-evaluated (see PCI/CABG group below).
Patients with stable angina and a low probability for exercise-induced events are eligible for competitive sports requiring low/moderate static and low dynamic types of sports (IA–IIA, see Table 1), for example, bowling, cricket, golf, rifle shooting, archery and equestrian.
Leisure-time physical activity, including recreational sports, should be encouraged and individually prescribed for patients with stable angina. The exercise intensity should be kept 10 beats below the anginal threshold and/or below the ventilatory threshold (see above) [57]. As a level of intensity indicator, the rating of perceived exertion (RPE < 14) is a clinically relevant alternative, especially in patients taking beta-blockade.
Regular, annual clinical follow-up and stress testing to assess any developing IHD is necessary in athletes with stable angina and is advised in non-athletes.
Patients with silent ischaemia
Silent ischaemia (SI) is defined by the presence of unequivocal evidence of ischaemia on stress testing, but without clinical symptoms of angina [18]. SI may be encountered during routine pre-participation screening or as a direct result of evaluating active individuals with increased risk factors (see below). Many athletes with a positive exercise test with no symptoms do not suffer from coronary artery disease (false-positive tests) [73]. These individuals should go through all the necessary diagnostic steps, including additional stress testing, appropriate non-invasive assessment (MRI, myocardial perfusion imaging) to rule out/confirm IHD, and if such test results still prove inconclusive, coronary angiography may have to be considered.
The physician supervising stress testing should be aware that some athletes have an increased threshold/tolerance to pain [74], and also of atypical symptoms, possibly denial of symptoms and lack of prodromal symptoms.
Silent ischaemia increases the risk for cardiac arrest during physical stress to the same extent as symptomatic IHD [75]. If coronary angiography has shown significant coronary atherosclerosis, and/or stress testing shows unequivocal signs of ischaemia, these patients should be risk stratified similarly to the athletes with known IHD.
Patients with SI should be subsequently treated according to the ESC guidelines on stable angina [5].
Recommendations
Patients with silent ischaemia and a high probability for exercise-induced coronary events are not eligible for competitive sports.
Patients with low probability for exercise-induced events are eligible for low/moderate static and low dynamic types of competitive sports (IA–IIA, see Table 1), following optimal medical treatment.
Leisure-time physical activity, including recreational sports, at intensities below the ischaemia threshold, should be encouraged. The optimal intensity should be determined by heart-rate monitoring. Rating of perceived exertion (RPE) is an alternative, especially for patients on beta-blockade, while the lack of anginal symptoms in SI hinders the use of the angina threshold.
Regular, annual follow-up and serial stress testing to gauge potential progression of ischaemia is necessary in active individuals with silent ischaemia.
Patients after PCI/CABG
Once PCI and/or CABG are performed and out-patient care starts, this group needs special attention with regard to conditioning programmes.
Physical (or pharmacological) stress testing must be performed in patients after successful PCI/CABG before they resume sports activity again. If no evidence of myocardial ischaemia is found after the individual outpatient cardiac rehabilitation [50] is completed (typically after 3–4 months), patients may resume individually tailored activity under the supervision of a qualified physician.
In the case of left ventricular dysfunction and/or electrical instability, the risk of an adverse coronary event increases during training and/or competition.
Recommendations
Patients with previous revascularization and a low/intermediate probability for exercise-induced coronary events are eligible for low dynamic and low to medium static types of competitive sports (IA–IIA, see Table 1), after 12 event-free and symptom-free months.
In patients with a high probability for exercise-induced events, competitive sports are not recommended.
Leisure-time physical activity, including recreational sports, is encouraged due to multiple positive effects (as outlined above), at a safe level, in line with the recommendations for stable angina.
Special cases of single-vessel disease with low probability for events and other contributing factors (e.g. dehydration) probably have less risk. Recommendations regarding activity in these cases are difficult due to lack of evidence. Subsequently, the recommendations are as outlined above (IA–IIA), but more activity may be allowed in certain cases on individual prescription.
Periodical, serial re-assessment, at least every 12 months, is recommended.
Patients after myocardial infarction
Out-patient cardiac rehabilitation [50] usually starts 2–6 weeks after an unequivocal MI (>1 mm ST elevation in the inferior leads or 2 mm ST elevation in two or more other leads on the ECG), with or without symptoms, and/or with troponin- and/or creatinine kinase (CK)-MB elevation within the first 24 h [76, 77], and/or reduced TIMI flow during coronary angiography if performed in the acute phase.
Patients must be treated optimally according to the guidelines for MI, including taking beta-blockers and aspirin [72, 78]. Risk assessment post-MI should be performed before discharge from hospital prior to in/out-patient cardiac rehabilitation, and again after completion of rehabilitation, typically after 3–4 months. Thereafter, recommendations for further physical activity can be given (Fig. 1) [70].
The incidence of SCD after symptomatic and silent MI is comparable [79]. Patients with a high risk for future events [80] are those with persistent or recurrent myocardial ischaemia at rest or on minimal exertion; or persisting heart failure with a poor LV function; and/or electrical instability (e.g. ventricular tachycardia, frequent and polymorphic ventricular premature beats). Coronary angiography must be performed in SCD survivors and high-risk patients after myocardial infarction. Unless coronary angiography is performed during the acute phase of the MI, coronary angiography is not indicated per se.
For risk assessment and sports eligibility, exercise testing and echocardiography are mandatory.
Recommendations
Patients with a high risk of cardiovascular events after MI are not eligible for competitive or recreational sports, and should be considered for coronary angiography or invasive treatment on clinical grounds.
Post-MI and with a low risk for cardiovascular events, patients are eligible for competitive sports class IA/IIA, and recreational sports at a safe level (10 beats below anginal/ischaemic threshold) and/or RPE < 14.
In the special case of patients with impaired LV function post-MI (ejection fraction <50% on echocardiography) and often accompanying poor exercise capacity (who, by definition, are high-risk patients for cardiovascular events), 24-h Holter monitoring may aid in identifying those who could be eligible for sports. If no clinically significant arrhythmias, including ventricular tachycardia (VT) and high-degree atrio-ventricular (AV)-block are present, the patient may be eligible for competitive sports class IA/IIA as well as recreational sports at a safe level. If ventricular arrhythmias are detectable, the recommendation remains as for high-risk patients (see above).
Initially, the exercise test should be repeated after 3 months and then at prescribed regular intervals (as often as every 3 months), based upon individual prognosis.
Leisure-time physical activity should always be encouraged and be moderately intensive (up to the ventilatory threshold and/or 70–85% of age-related maximum heart rates, the latter not being subject to the effects of medication, e.g. beta-blockade).
Patients without evidence of IHD, but with one or more classical risk factors for IHD
The European Society of Cardiology (ESC) recently issued new guidelines on cardiovascular disease prevention in clinical practice [2]. According to the SCORE system, in asymptomatic, apparently healthy subjects, the total IHD risk level can be estimated from the presence of the major risk factors, namely age, sex, smoking, blood pressure, and total cholesterol level, together with diabetes [2].
The high risk profile for developing a fatal cardiovascular event is defined as follows:
the presence of the various multiple risk factors, resulting in a 10-year risk > 5% now or if extrapolated to age 60 in the SCORE chart;
markedly raised levels of total cholesterol [>8 mmol/l (320 mg/dl)], low-density lipoprotein (LDL)-cholesterol [>6 mmol/l (240 mg/dl)] or blood pressure (> 180/110 mmHg);
diabetes mellitus type 2 or type 1 with micro-albuminuria, as individuals with diabetes mellitus have the same risk as patients with stable angina for a future coronary event [81].
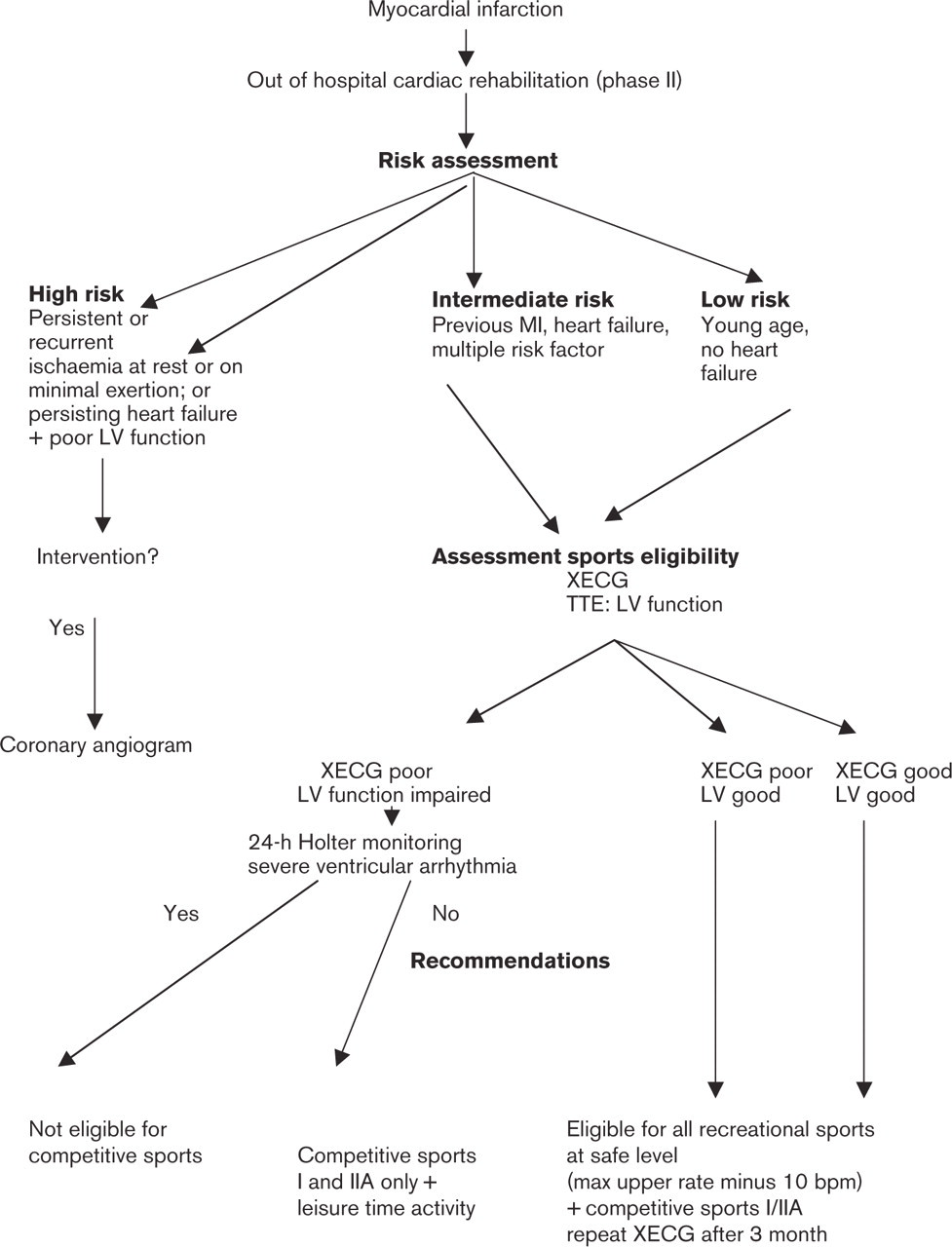
Risk assessment and recommendations for sports eligibility after myocardial infarction (adapted from [70]). LV, left ventricular; MI, myocardial infarction; XECG, exercise electrocardiogram (exercise test); TTE, transthoracic echocardiography; bpm, beats per minute (heart rate).
Individuals with a strong family history of premature cardiovascular disease [82, 83] in first-degree relatives < 50 years old, should also be added to this group. This risk factor may be more prominent in young MI-patients, < 45 years of age [11].
The low risk-factor profile for developing a fatal cardiovascular event is defined as active individuals with fewer risk factors according to SCORE (< 5% risk) [2].
The degree of preparticipation screening for individuals with risk factors for IHD, but without previous diagnosis of IHD will depend on the intended level of physical activity and its proposed intensity (competitive sports versus leisure-time activity, and high versus low/medium intensity). The additional burden of known risk factors should also be taken into consideration.
Patients with a high risk-factor profile for future cardiovascular events (>5% according to SCORE)
These patients should be further evaluated to rule out silent or symptomatic ischaemia, by extensive symptom evaluation (especially ask for atypical symptoms), and by maximal physical stress ECG if competitive sports are intended. For recreational sports/leisure-time activity, stress ECG is recommended only on an individual basis. Stress ECG remains the most regular screening test used to evaluate ischaemic thresholds in patients with high risk factors [84], and the exercise test may be useful when combined with the SCORE system to risk-stratify asymptomatic individuals in a screening programme [85]. However, exercise ECGs have proven weaknesses (false-positive and negative results).
Alternatively, stress scintigraphy or stress echocardiography (especially in women) may be superior to stress ECG in doubtful cases, but the costs are higher [73]. Physical stress with SPECT [86] or positron emission tomography (PET) [87] are not sufficiently evaluated for primary detection of IHD in this group of athletes [84], but may be indicated to confirm true ischaemia, in some cases with a positive exercise test. According to the results of the stress test we can then stratify further.
Negative stress testing The absolute risk of a major event during physical activity is small in asymptomatic patients without evidence of cardiac disease [6]. However, among active subjects who have high risk scores but no evidence of cardiac disease, future risk of a cardiac event is nevertheless elevated.
Recommendations
The patients with a high risk-factor profile and no signs of ischaemia are eligible for most competitive sports, unless resting blood pressure or other risk factors indicate otherwise (see separate recommendations for physical activity in patients with hypertension [88]). Restrictions may apply for extreme sports, for example scuba diving, flying and mountaineering (often on an individual basis).
Leisure-time, non-athletic activity is encouraged and has been shown to confer positive effects on the most traditional risk factors of IHD (blood pressure, total cholesterol, glucose levels).
Regular screening according to SCORE (every year, and sooner in the case of symptoms) should be performed in these patients because of their possible future risk, together with possible changes to that risk over time (deterioration or improvement).
Exercise testing should be applied every second year in young competitive athletes (< 35 years old) and yearly in older competitive athletes (> 35 years old).
Patients with a positive exercise test These patients need further evaluation by stress echocardiography/myocardial scintigraphy, but realizing that, in rare cases, these tests may produce a false-negative (or false-positive). Coronary angiography may be needed in conflicting cases to confirm/exclude the presence of IHD. Several studies have established an increased risk for future coronary events in asymptomatic populations with coronary risk factor(s) and a positive exercise test (Multiple Risk Factor Intervention Trial (MRFIT) [89], Kupio Study [90]). If IHD is confirmed, these athletes should be risk stratified as for known IHD.
Recommendations See recommendations for known IHD, above.
Patients with a low risk-factor profile (<5% according to SCORE)
Regular use of exercise testing in healthy asymptomatic athletes, < 35 years old for men and < 45 years for women, without classical risk factors is not recommended [6, 84, 91]. These athletes are considered as having a low risk during physical activity.
Recommendations
Asymptomatic patients with a low risk-factor profile are eligible for all types of competitive sports as well as leisure-time activity.
No further evaluation by stress testing is needed in asymptomatic athletes with a low risk-factor profile, unless the risk-factor profile deteriorates. Periodical risk factor evaluation by a qualified health care professional is recommended every 1–3 years.
Other entities associated with myocardial ischaemia
Myocardial bridging
This is defined as the presence of a segmental intramyocardial course of one of the major coronary arteries, most commonly the left anterior descending coronary artery (LAD). This condition usually has limited clinical significance at rest, but has been linked to myocardial ischaemia and even SCD [20, 92, 93].
Myocardial bridging should be considered in young athletes with exertional angina, signs of antero-septal ischaemia and no coronary risk factors. The diagnosis may be made by coronary angiography and/or MRI. Only a few patients show signs of ischaemia on exercise tests [94]. Myocardial bridging may be more common in athletes with hypertrophic cardiomyopathy, consequently echo-cardiography is recommended.
Risk stratification and recommendations Risk stratification and recommendations for this condition are difficult due to lack of scientific evidence. However:
if ischaemia is confirmed on stress testing, the athlete should be evaluated according to athletes with known IHD, see above;
if hypertrophic cardiomyopathy is present, athletes should be evaluated in exactly the same way as other patients with cardiomyopathy.
Recommendations for participation in competitive sports and leisure-time physical activity in patients with ischaemic heart disease (IHD)
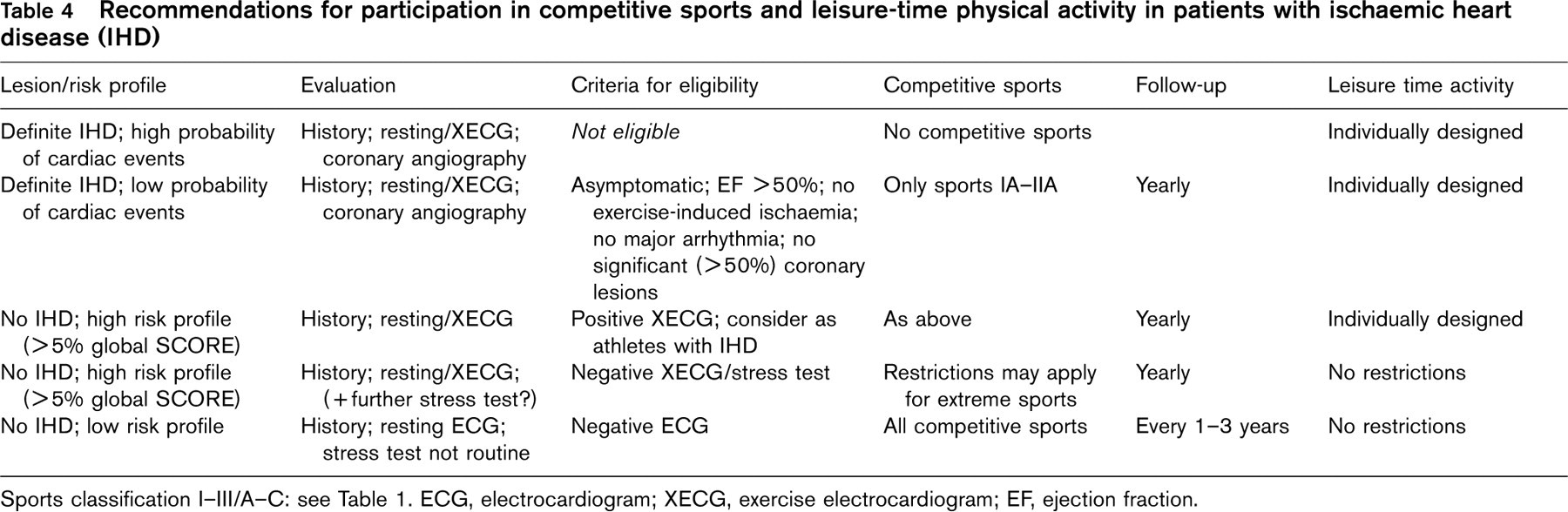
Sports classification I–III/A–C: see Table 1. ECG, electrocardiogram; XECG, exercise electrocardiogram; EF, ejection fraction.
Spasm angina
Spasm angina is defined as a transient marked reduction of the coronary artery lumen leading to myocardial ischaemia, in an either normal or atherosclerotic vessel [95]. These patients are typically younger and without classical risk factors for IHD. Precipitating factors may be hyperventilation, dehydration, tobacco, drug abuse (cocaine) [29], autonomic imbalance [96] or endothelial dysfunction [97].
Coronary angiography may or may not show signs of concomitant coronary artery disease.
Risk stratification The prognosis is good if coronary angiography is normal [98]. If IHD is present, the prognosis is dependent on the severity of the underlying disease.
Recommendations These are difficult due to a lack of scientific evidence. However, in the case of an underlying IHD, recommendations follow those outlined above for known IHD.
Syndrome X
Syndrome X is defined as symptoms of angina pectoris, with signs of ischaemia on testing, but with ‘normal’ coronary angiography, thus not showing any luminal narrowing [99, 100]. Some of these cases may also be due to coronary vasospasm of coronary microvessels, but other abnormalities, such as chest pain secondary to oesophageal dysfunction, may sometimes fulfil the criteria of this heterogeneous entity [101].
Patients with syndrome X should be further evaluated by echocardiography and exercise test if not already performed, and by an exercise stress test such as stress-echo or myocardial scintigraphy.
Risk stratification Showing a normal coronary angiogram, these patients have an excellent overall prognosis, with low risk for cardiovascular events [102]. However, the specific risk for these patients during exercise is largely unknown.
Recommendations
If both the stress-echo and/or scintigraphy are normal, the athlete may have no true ischaemia, and may be allowed to participate in competitive sports on an individual basis.
If the stress tests confirm ischaemia, the athlete is evaluated as for known IHD (above).
The above recommendations for participation in competitive sports and leisure-time physical activity by patients with IHD are summarized in Table 4.