
Abstract
Background
Design
Methods
Results
Conclusions
Keywords
Introduction
Research has indicated that participation in a regular exercise program is an effective intervention to maintain and enhance multiple aspects of physical and psychological functioning across the lifespan. Beneficial effects of exercise on cognitive function could be explained by possible cardiovascular mechanisms. Aerobic exercise results in an increase in cerebral blood flow [1] and aerobic exercise influences components of cardiovascular fitness [2–10]. These components of cardiovascular fitness (vascular risk factors) have been related to a reduction in cognitive performance [11, 12]. Current evidence for the link between physical activity, cardiovascular fitness and cognitive function in older individuals is provided by several cross-sectional studies and randomized controlled trials, although the results are inconsistent [13–25]. Recent meta-analyses [26, 27] report that aerobic fitness training enhances the cognitive vitality of healthy adults aged 55 years and older. A similar effect was found in demented and cognitively impaired older adults [28]. The results of the previous studies on the effect of physical activity on cognitive function are difficult to compare as a result of different methodological issues. In most studies the total time spent on and the intensity of physical activity were rarely presented separately. Moreover, these studies focused mainly on supervised physical activity discarding a possible association between leisure time or unsupervised exercise and cognitive function, and did not account for the effects of variation in activities on prevention of cognitive decline [23].
This study aimed to investigate the association between the time spent on physical activity as well as the average intensity of these activities and cognitive function, the latter evaluated with a comprehensive neuropsychological test battery, in a large, healthy middle-aged population in the Netherlands.
Methods
Study population
Data from the Doetinchem Cohort Study were analysed in 2004. The baseline measurements for the Doetinchem Cohort Study were carried out from 1987 to 1991 in a cohort of 7 769 men and women aged 20-59 years. Response in participants aged 45 years and older was 61%. A first follow-up measurement was carried out from 1993 to 1997. Each respondent was reexamined 6 years after the baseline measurement. The second follow-up measurement was done from 1998 to 2002, 5 years after the first reexamination, the respondents now being 31-70 years of age. Response during follow-up was 75-80%. In 1995 cognitive assessment was introduced for respondents aged 45 years and older. During 1995-2000 all respondents aged 45 years and older were tested once, so cognitive testing was spread over two rounds of follow-up [29]. Response rate for participation in the cognitive tests, for those participating in the study was over 90% and a total of 1927 men and women were examined. See earlier publication for exact information on recruitment of the study participants [29].
The study was approved by the Medical Ethics Committee of the Organization for Applied Scientific Research-Zeist, the Netherlands. All participants signed an informed consent before enrolment in the study.
Assessments
For all examinations, participants received a self-administered questionnaire at home and were invited to come to the research centre for medical examinations. The questionnaire contained items on demographic variables, lifestyle factors, (family) history of diseases, medication use and perceived health.
Education was assessed as the highest level achieved and was classified into three categories: low, middle and highly educated. In the research centre various cardio-vascular risk factors, including body mass index [weight (kg) divided by height (m) squared], waist and hip circumference (cm) and blood pressure (random-zero sphygmomanometer) were determined. Furthermore, plasma total and high-density lipoprotein cholesterol and glucose were determined. The participant's customary alcohol intake and smoking habits were estimated from self-report. Full descriptions of these methods are found in a previous paper [29].
Assessment of physical activity
Physical activity was assessed over the year before cognitive measurements with an extended version of the validated European Prospective Investigation into Cancer and nutrition (EPIC) physical activity questionnaire [30]. The questionnaire included questions on time (h/week) spent on leisure time activities for summer and winter separately, and questions on sports irrespective of season. Leisure time activities included walking, bicycling, housekeeping, doing odd jobs and gardening. Spearman's correlation coefficients for reproducibility of the EPIC questionnaire ranged from 0.47 to 0.89 in men and from 0.49 to 0.81 in women. Spearman's correlation coefficients for relative validity between the short questionnaire and a 3-day activity diary were between 0.32 and 0.81 for men, and 0.28 and 0.72 for women [30].
All activities were coded and given a specific metabolic equivalent (MET) value (1 MET = 3.51 × O2/kg/min) for intensity varying between 1 and 12 METs [31]. Subsequently, total MET hours were calculated as the sum of total time × MET for each activity. The weighted average intensity of all activities was then calculated by dividing the total MET hours by the total amount of time spent on those weekly activities (METs). Variation in weekly activities (ranging from 0 to 8) was calculated by summing up all possible leisure time physical activities; walking, bicycling, housekeeping, doing odd jobs, gardening and sports activities.
Assessment of cognitive function
Cognitive function was assessed using a battery of tests that measures specific cognitive domains, including processing speed, memory function, cognitive flexibility (time needed for higher order information processing) and overall cognitive function. Included were the Dutch versions of the (Visual) Verbal Learning test (subtest of the Wechsler Adult Intelligence Scale (WAIS) [32], immediate and delayed recall), the Concept Shifting Task, The Stroop Colour Word test, the Letter Digit Substitution test (WAIS) and a Word Fluency test (animals). These tests are known to be sensitive to calendar age (so called Do not Hold tests) detecting age-related cognitive impairment, and have no ceiling effect, as the Mini-Mental State Examination (MMSE) would have in this specific age group [33]. Detailed descriptions of all used cognitive tests are found in neuropsychological literature [34].
As a result of a lack of time, the Concept Shifting Task was excluded from the test battery from January 2000 and onward. In total, 1927 participants completed the cognitive measurements, of whom 1667 performed the Concept Shifting Task.
Statistical analysis
As stroke can have a profound effect on cognitive performance, all participants with this condition were excluded from the statistical analyses (N = 38 and 19 cases of missing data on stroke).
The timed cognitive tests (Stroop Colour Word test and the Concept Shifting Task) were not distributed normally and were log transformed before further analysis. The cognitive data were made comparable by transforming them to standardized z scores [2] and recalculated to compound scores according to reports in previous studies [29]. Compound scores for memory function were calculated by averaging the z scores of the subtests of the Verbal Learning test. For processing speed, the average of the z scores of subtests A and B of the Concept Shifting Task, subtest I of the Stroop Colour Word test and the Letter Digit Substitution test was calculated. Compound scores for cognitive flexibility were calculated by averaging the z scores of the subtest C of the Concept Shifting Task and the third subtest of the Stroop Colour Word test. As a reflection of overall cognitive function, the average of the z scores of the Letter Digit Substitution test, the Word Fluency test, the total and delayed recall score of the Verbal Learning test and subtest III of the Stroop Colour Word test was calculated. For tests in which a higher score denotes a better performance (Verbal Learning test, the Letter Digit Substitution test and the Word Fluency test), the sign was reversed before calculation of a pooled z score. We explored the possibility of linear relationships between the physical activity measures (time spent on activities and average intensity of activities) and the cognitive data.
We performed multiple linear regression analyses in which each regression coefficient represented the difference in the standardized cognitive score (z score) per cognitive function according to, either the time spent weekly on activities or the weekly weighted average intensity, or the weekly variation in activities. Each regression was adjusted for smoking status and alcohol consumption besides adjustments for age, sex and education. Final adjustments were made for cardiovascular risk factors; blood pressure, glucose, total cholesterol, high-density lipoprotein -cholesterol and body mass index. Five alcohol consumption groups were entered as dummy variables, smoking status was entered as two dummies (former and current smokers vs. never smokers) [29]. Education was defined as ‘low’ (primary school), ‘middle’ (high school) or ‘high’ (professional education or university) and entered as two dummy variables. Our calculation of weighted average intensity makes it partially dependent on the total variation in physical activities reported. To elucidate effects of this variation on cognitive function, we ran the described multiple regression analyses, according to the variety in all weekly physical activities (ranging from 0 to 8 possible activities). Exclusion of outliers in the cognitive data did not alter the results of the regression analysis, and so these outliers were retained in the analyses. All analyses were performed in SPSS version 12.0 (SPSS Inc. Chicago, Illinois, USA, 2004) [35].
Results
Table 1 presents the characteristics of the study population. Overall, participants spent 30 h/week on activities with an average intensity of 3.5 MET.
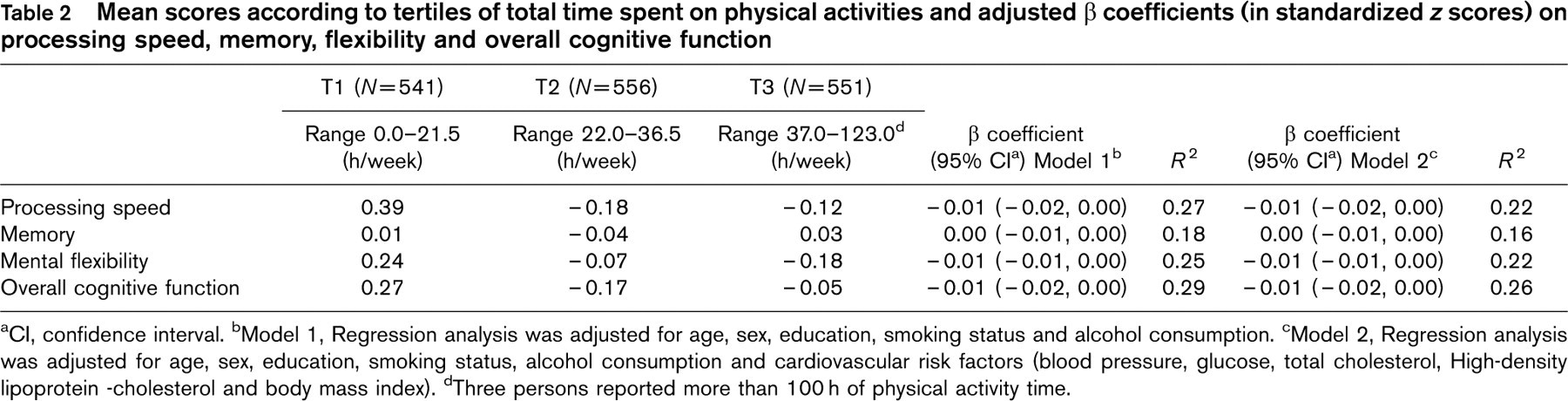
Although potentially 1870 individuals were left in analyses, the number of truly analysed participants was influenced by missing data on cognitive tests due to the exclusion of the Concept Shifting task and individual problems on the tests. Analysis on speed includes 1600 cases, on memory 1858, on flexibility 1596, and on global function 1839 cases. Comparing baseline descriptives of missing participants with the group of included participants with an independent samples t-test comprised 48 comparisons. Owing to the large number of statistical tests, the odds were that several of the comparisons would result in statistically significant differences. Indeed, five comparisons showed statistically significant differences between both groups. Multiple linear regression analyses showed no significant associations between the total time spent on physical activity and the cognitive parameters. The associations of weekly weighted average intensity were determined with multiple linear regressions. Participants with higher levels of weekly weighted average intensity scored significantly better on processing speed (β 0.46, P < 0.01), memory (β 0.16, P < 0.05), mental flexibility (β 0.16, P < 0.05) and overall cognitive function (β 0.17, P < 0.01). The results of the regression analyses are presented in Tables 2 and 3. As an association between weekly weighted average intensity of all activities could partially be explained by the variation in physical activities, we performed a multiple regression analysis according to the variation in all possible activities. The results in Table 4 show significant associations between the variation in activities and processing speed (β 0.14, P < 0.05), memory (β 0.06, P < 0.05), mental flexibility (β 0.09, P < 0.01) and overall cognitive function (β 0.22, P < 0.01). Final adjustments for cardiovascular risk factors did not alter the results of the regression analyses.
Characteristics of the study population, Doetinchem Cohort Study, The Netherlands, 1995-2000
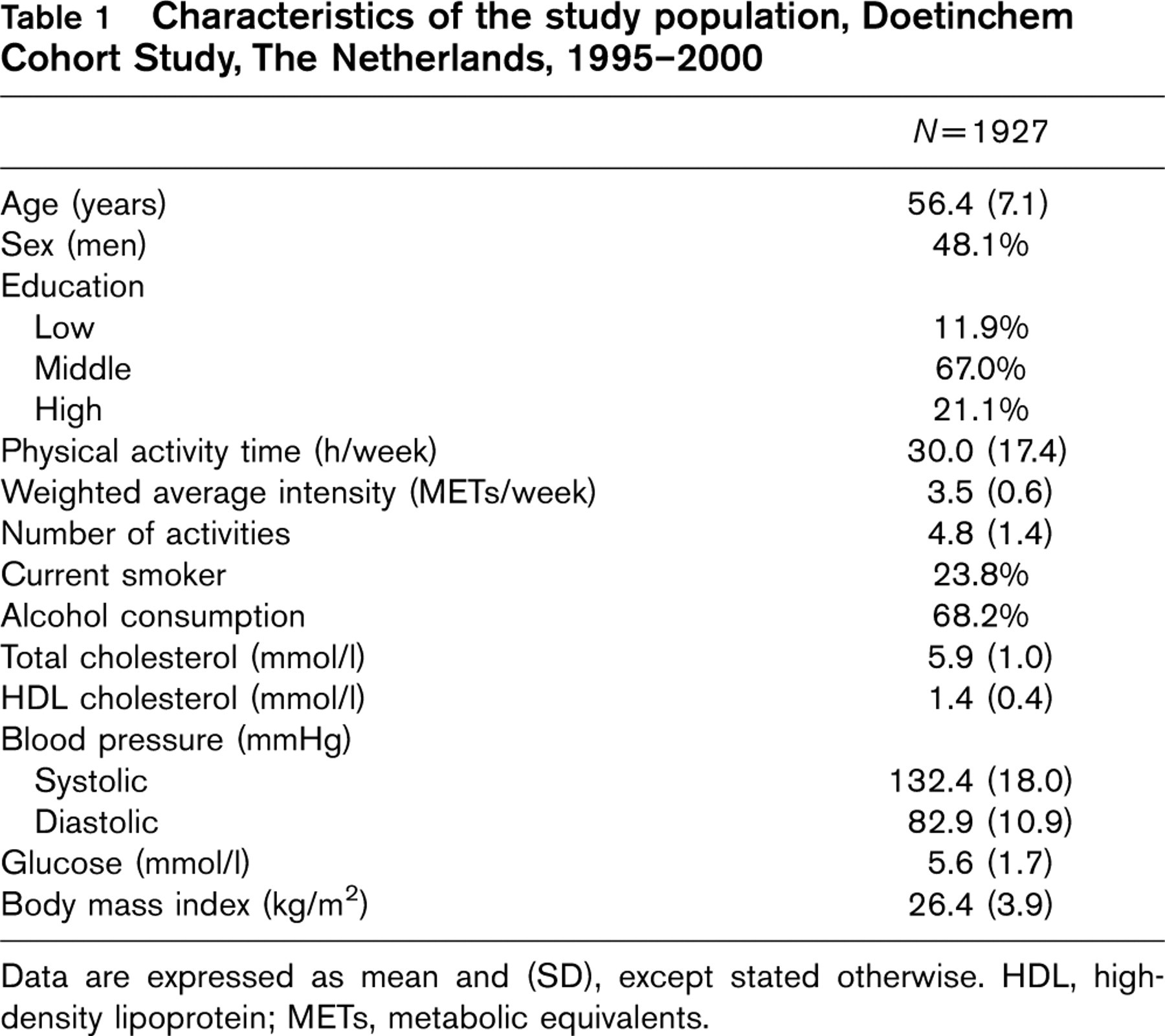
Data are expressed as mean and (SD), except stated otherwise. HDL, high-density lipoprotein; METs, metabolic equivalents.
Discussion
In this cohort study of 1927 healthy middle-aged men and women, weighted average intensity of weekly physical activities and variation in activities are positively and significantly associated with performance on processing speed, memory and mental flexibility as well as performance on overall cognitive function. In this cohort there were no significant associations between the total time spent on these weekly activities and cognitive capacity.
This study reports the separate effects of the time spent on, and the weighted average intensity of, unsupervised, usual, leisure time physical activities on cognitive function in a middle-aged healthy population. Other studies reporting the effects of physical activity on cognitive function use composite physical activity indexes in which duration and intensity of activities are intertwined [13, 16, 18, 23] or studies tend to report the effects of specific training programs in the elderly [19–21, 24, 25]. Furthermore, our study used a sensitive neuropsychological test battery, which can detect small cognitive differences even in middle age in contrast to the widely used MMSE.
Several cross-sectional studies, randomized controlled trials and meta-analyses stress the relation between physical activity and cognitive performance, although the results are inconsistent [13–25]. Regular physical activity is reported to decrease the risk of dementia [13, 15, 16, 18] or can enhance cognitive capacities [19–21, 26, 27, 36]. Consistent with our data, higher levels of intensity of leisure time activities [15, 16, 18] or training programs based on diversity of exercises [19, 21, 37] have been associated with reduced risks of cognitive impairment or enhancement of capacities. Higher intensity of activities results in boosting the cardiovascular system which results in an increase in cerebral blood flow and increased oxygen transport to the brain. In contrast, reduced cognitive function is correlated directly with reductions in cerebral blood flow in patients with multi-infarct dementia and dementia of the Alzheimer's type [11, 12]. At the same time our data showed no relation between the total time spent on physical activity and cognitive function. A large prospective population study on 4055 participants confirms our data by reporting that more hours of physical activity is associated with a small significant beneficial effect on cognitive decline over 6 years, but this association was lost after adjustment for cognitively stimulating activities [23]. Training programs in the randomized controlled trials that describe no effects [24, 25] of exercise tend to be monotonous; participants jog or cycle indoors. The possible effects of variation in exercises or cognitive stimulation by alternating environments are lost. At the same time these intervention groups are compared with groups of yoga, flexibility/strength training or memory training which could imply more variation and stimulation. Cognitive performance has been related to cardiovascular risk factors and disease [7–10]. A possible mechanism by which physical activity could improve cognitive function is through an effect on cardiovascular risk factors, such as blood pressure or serum cholesterol levels [3]. Our adjustment for all cardiovascular risk factors, however, did not alter the results of the regression analysis.
Mean scores according to tertiles of total time spent on physical activities and adjusted β coefficients (in standardized z scores) on processing speed, memory, flexibility and overall cognitive function
CI, confidence interval.
Model 1, Regression analysis was adjusted for age, sex, education, smoking status and alcohol consumption.
Model 2, Regression analysis was adjusted for age, sex, education, smoking status, alcohol consumption and cardiovascular risk factors (blood pressure, glucose, total cholesterol, High-density lipoprotein -cholesterol and body mass index).
Three persons reported more than 100 h of physical activity time.
Mean scores according to tertiles of weighted average intensity on physical activities and adjusted β coefficients (in standardized z scores) on processing speed, memory, flexibility and overall cognitive function
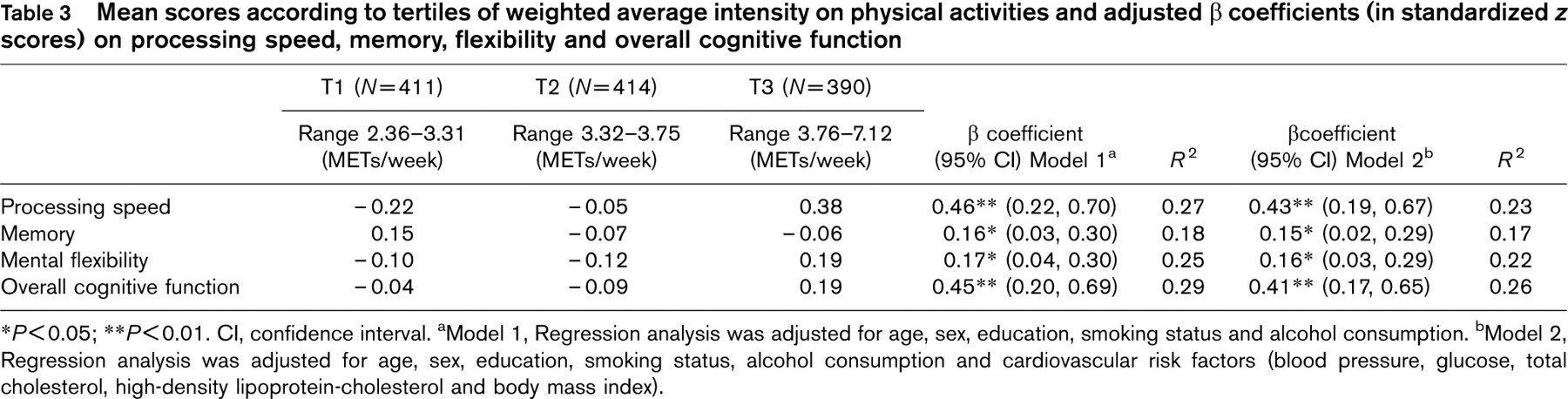
P < 0.05;
P < 0.01. CI, confidence interval.
Model 1, Regression analysis was adjusted for age, sex, education, smoking status and alcohol consumption.
Model 2, Regression analysis was adjusted for age, sex, education, smoking status, alcohol consumption and cardiovascular risk factors (blood pressure, glucose, total cholesterol, high-density lipoprotein-cholesterol and body mass index).
Adjusted β coefficients (in standardized z scores) on processing speed, memory, flexibility and overall cognitive function according to variation in all activities
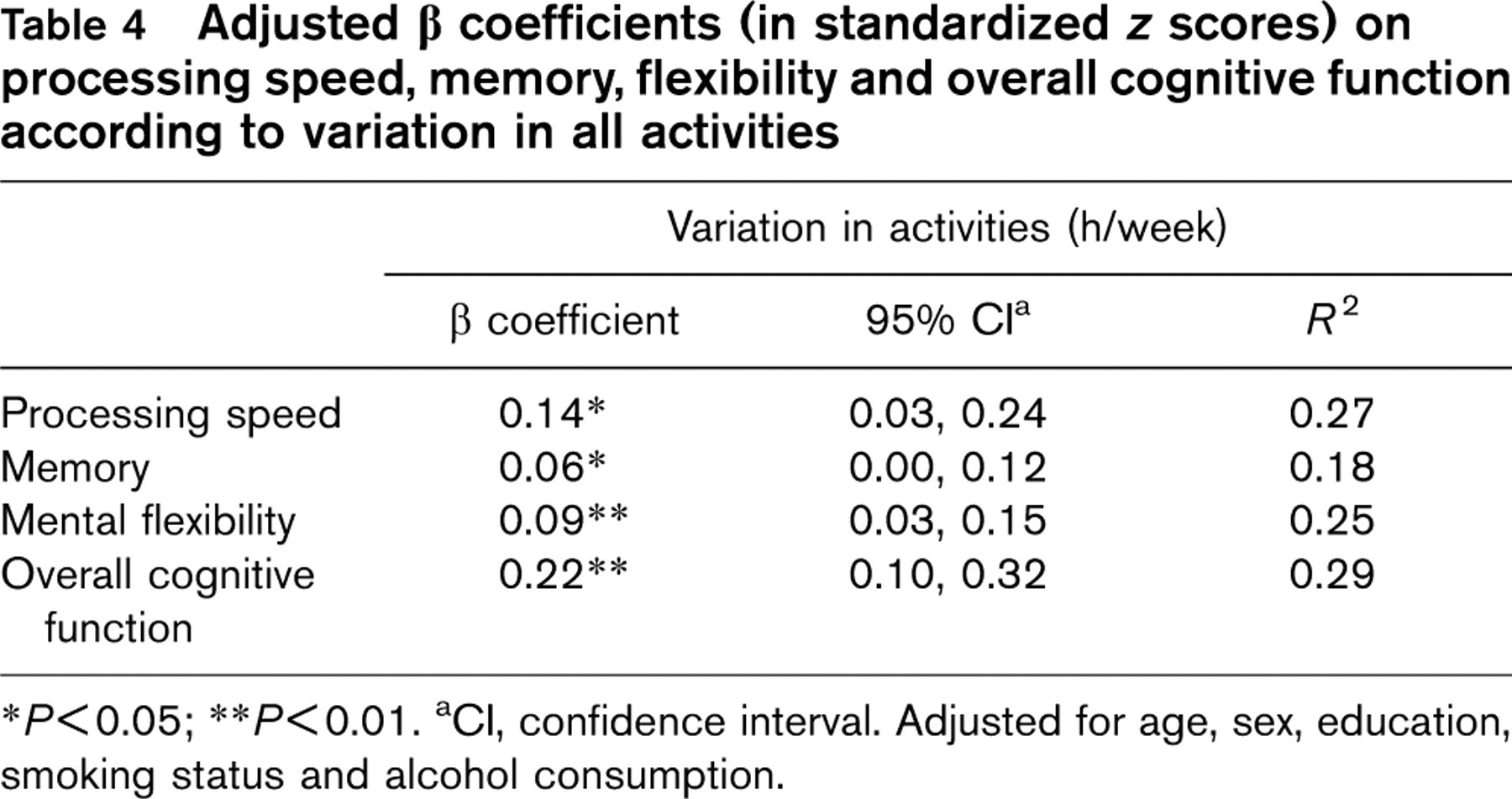
P < 0.05;
P < 0.01.
CI, confidence interval. Adjusted for age, sex, education, smoking status and alcohol consumption.
The strength of this study was the use of a neuropsychological test battery, which contained several tests sensitive to cognitive differences even in the middle age. Clinically significant cognitive deficits are seldom seen among the middle aged, thus sensitive, standardized neuropsychological tests are needed to assess performance differences, in contrast to screening on gross cognitive impairment with short forms, such as the MMSE. One of the limitations of this study is that physical activity was assessed by a questionnaire. Although questionnaires assess usual physical activity over a lengthy period, questionnaires are subjective methods and could result in an overestimation of the amount of physical activity, as people tend to give a socially acceptable answer [38]. Furthermore, the MET values (although categorized conform the classification of energy costs of human physical activities [31]) were estimates and not measured with objective methods in our study. All the variables including cognitive function were measured only once in the entire cohort. It would have been more informative to have data on changes in physical activities and cognitive function over a period of time as changes in the total time spent on, and the intensity of physical activity, might result in changes in cognitive capacity [15], and these data are being collected now. Short-term effects of physical activity on cognitive capacity were probably not assessed in our study. Finally, the cross-sectional nature of the analyses renders it possible that diminishing cognitive abilities (in the older participants of our study) influenced physical activity recall.
New research should focus on the possible mechanisms by which physical activity may be beneficial for cognition, possibly through a mediating role of aerobic factors [39]. Randomized controlled studies, which are directed at changes in cellular and molecular mechanisms and better performance on a neuropsychological test battery in relation to increased physical activity, may enable researchers to determine a possible causal link. At the same time, these studies should account for a possible role of stimulating activities [23] or variation in activities. To prove the causal nature of the latter, longitudinal data are needed.
In conclusion, weighted average intensity of weekly physical activities and variation in activities are positively and significantly associated with performance on processing speed, memory and mental flexibility as well as performance on overall cognitive function in this healthy, relatively young middle-aged population.
Footnotes
Acknowledgements
The authors express their gratitude to the epidemiologists and field workers of the Municipal Health Services in Doetinchem for their contribution to data collection. The Doetinchem Cohort Study was financially supported by the Ministry of Health, Welfare and Sports of the Netherlands and the National Institute for Public Health and the Environment, Bilthoven, the Netherlands.
Potential conflict of interest: none.