
Abstract
Background C-type natriuretic peptide (CNP) is structurally related to cardiac natriuretic peptides and is currently considered as an endothelium-derived hyperpolarizing factor. Endothelial dysfunction, commonly observed in chronic heart failure (HF) patients is positively affected by physical training.
Methods To evaluate the effect of aerobic physical training on the expression of CNP, 90 HF patients on optimal pharmacological treatment (age 62±2 years, mean±SEM), randomly assigned in a 3:1 ratio to either control group (C, 19 patients) or home-based aerobic exercise-training program group (T, 71 patients), completed the protocol. Plasma assay of CNP, brain natriuretic peptide or B-type natriuretic peptide (BNP), and norepinephrine; echocardiogram; and cardiopulmonary-stress test were performed in all patients at enrollment and after 9 months.
Results At baseline, in both groups, CNP plasma level was significantly related to BNP (R = 0.50), ejection fraction (R = 0.43), and peak oxygen uptake (Vo2, R = 0.43, all P [ 0.001). After 9 months, trained patients showed an improvement in peak Vo2 (P [ 0.001) and ejection fraction (P [ 0.05), whereas norepinephrine (P [ 0.05), BNP (P [ 0.001), and CNP (P [ 0.001) decreased. No changes occurred in group C in group T, the decrease in CNP was significantly related to the increase in peak Vo2 (R = 0.31, P [ 0.01), and the relation between CNP and BNP was preserved at the end of the program (R = 0.41, P [ 0.001).
Conclusion Clinical and functional improvement after physical training in HF patients is associated with a decrease in adrenergic activation and in both CNP and BNP concentration. Changes in CNP plasma concentration after physical training might reflect an improvement in endothelial function.
Introduction
C-type natriuretic peptide (CNP), first isolated from porcine brain in 1990 [1], is mainly produced by the endothelium [2] and holds vasodilator properties, counteracting the action of endothelin and angiotensin II [3]. It is currently considered to be an endothelium-derived hyperpolarizing factor [3], and shares structural and physiological properties with the atrial (ANP) and brain (B-type) natriuretic peptides (BNP), but has a shorter half-life [4]. Both ANP and BNP, as well as shear stress, induce its production and release [5]. Similar to ANP and BNP, which have an established diagnostic and prognostic relevance [6], CNP plasma level increases in chronic heart failure (HF) patients, in relation to clinical severity [7].
Impaired endothelium-dependent vasodilatation is a common finding in HF [8,9], and is associated with vasoconstrictor influences by neurohormonal activation, namely, the sympathetic, renin-angiotensin, and endothelin systems. Physical training can reduce neurohormonal activation [10–12] and improve endothelium-dependent vasodilation [13,14] independently of pharmacological treatment. The aim of this study was to evaluate whether physical training could result in changes in CNP secretion in HF patients.
Methods
Patients
We screened 148 consecutive patients with a diagnosis of systolic HF from July 2003 to September 2005 at our institution. Inclusion criteria were impaired left-ventricular systolic function [ejection fraction (EF) [ 45%] and exercise capacity [peak oxygen uptake (Vo2) [ 25 ml/min/kg]. Exclusion criteria were the presence of New York Heart Association (NYHA) class IV, acute coronary syndrome up to 6 months before enrollment, exercise-limiting diseases, and severe pulmonary and renal disease (i.e. glomerular filtration rate [ 60 ml/min, calculated with the ‘modification of diet in renal disease’ equation). Of the 148 patients, 40 did not match these criteria, and 11 refused to participate. Ultimately, 97 patients (83 men and 14 women; mean age, 61 ± 1 years) were enrolled. All patients were on stable (i.e. > 1 month) optimal pharmacological treatment (Table 1), and did not present any sign of infection/inflammation. A change in treatment (only a ± 25 mg furosemide change was allowed) or hospitalization resulted in withdrawal from the study.
Study design and protocol
This was a prospective, randomized, controlled study. Patients were randomly assigned in a 3: 1 ratio to either the training group (T, 73 patients) or the control group (C, 24 patients). The two groups did not differ as to age, sex, NYFIA class, EF pharmacological treatment, or HF etiology (Table 1). Within the same morning, patients underwent clinical evaluation, blood sampling, an echocardiographic study, and a maximal cardiopulmonary exercise test with gas exchange, upon enrollment and after 9 months.
Blood samples were withdrawn between 08:00 and 09:00 h from an antecubital vein, after a 20-min period of supine rest. Plasma samples for CNP and BNP were collected into ice-chilled disposable polypropylene tubes containing aprotinin, (500 KIU/ml) and EDTA (1 mg/ml), to prevent the proteolytic breakdown of the peptides. Plasma samples were rapidly separated by centrifugation for 15 min at 4°C, and then stored in aliquots frozen at –20°C. CNP assay was carried out using a modified commercial radioimmunoassay (Phoenix Pharmaceuticals, Belmont, California, USA) after a preliminary extraction step on activated Sep-Pak C18 cartridges (Waters Associated, Milford, Massachusetts, USA), as described elsewhere in detail [7] (normal reference value [3.5 ng/l). BNP was measured by a two-site immunoradiometric assay (Shionogi, Japan), and norepinephrine by automated high-pressure liquid chromatography (HCL-725 CA, Tosoh Corporation, Tokyo, Japan).
Peak Vo2 (the highest value at the end of exercise, as a 20-s average) and ventilatory efficiency on exercise (estimated by linear relationship between ventilation and production of carbon dioxide before isocapnic buffering, VE/Vco2 slope) were determined. A single physician performed all the cardiopulmonary tests and the echocardiograms, and was unaware of the results of blood sampling.
Group T patients underwent a 9-month home-based aerobic training program on a bike, as described in detail elsewhere [12]: the training program consisted of cycling on a bike at 65% of peak Vo2 for a minimum of 3 days/week, 30 min/day; the exercise load was adjusted after 3 months by repeating a cardiopulmonary test, to achieve a progressive training effect. Compliance to the training program was assessed monthly by the physiotherapist during the inhospital training session. Group C patients continued their usual lifestyle, physical activity, and treatment. The investigation conforms to the principles outlined in the Declaration of Helsinki, and was approved by the local ethical committee. Informed consent was obtained from all the patients enrolled in the study.
Statistics
Skewness and kurtosis tests were used to determine whether the data were normally distributed. As CNP and BNP values were not normally distributed, natural logarithmic transformation of data was used for the parametric statistical analysis. The χ2 test and unpaired t-test were used to evaluate differences between the two groups. Paired t-test was used to assess differences within groups at enrollment and at the end of the follow-up. Linear regression analysis was used to assess the relationships between the variables. Results are expressed as mean ± SEM, and P values were considered significant when [ 0.05.
Results
Two patients in group T did not complete the program because of significant changes in treatment, and five patients in group C either because of hospitalization for decompensation or because of treatment changes. A total of 90 patients completed the protocol (71 in group T, 19 in group C).
At baseline, functional capacity and ventilatory efficiency (VE/Vco2) were both reduced: they were associated with plasma BNP and norepinephrine elevation in both groups to a similar extent. CNP concentration was similarly increased in both groups with respect to the reference value (Table 1).
At baseline, on the whole, CNP was inversely correlated with peak Vo2 (R = 0.43, P [ 0.001), maximum workload (R = 0.40, P [ 0.05), VE/Vco2 (R = 0.22, P [ 0.05), and EF (R = 0.44, P [ 0.001); a direct relationship was also observed between CNP, BNP, and norepinephrine plasma values (R = 0.50, P [ 0.001 and R = 0.31, P [ 0.01, respectively) (Fig. 1).
Effects of physical training on left-ventricular ejection fraction, functional capacity, and natriuretic peptides
In group T, EF had slightly increased before the visit at 9 months (from 35.1 ± 1.1 to 37.8 ± 1.0%; P [ 0.05); no change occurred in group C.
At the ninth month, group T increased in functional capacity (P [ 0.001) and maximum workload (P [ 0.001), whereas no changes were observed in group C. By the end of follow-up, the VE/Vco2 slope had not changed in either of the two groups (Table 2).
Baseline characteristics of the study patients in the training (T) or control (C) groups
No significant differences were found for any of the variables. Values are mean ± SEM unless otherwise specified. ACE, angiotensinogen-converting enzyme; ARB, angiotensin-receptor blocker; BMI, body mass index; GFR, glomerular filtration rate by ‘modification of diet in renal disease’ equation; LVEF, left-ventricular ejection fraction; NYHA, New York Heart Association functional class.
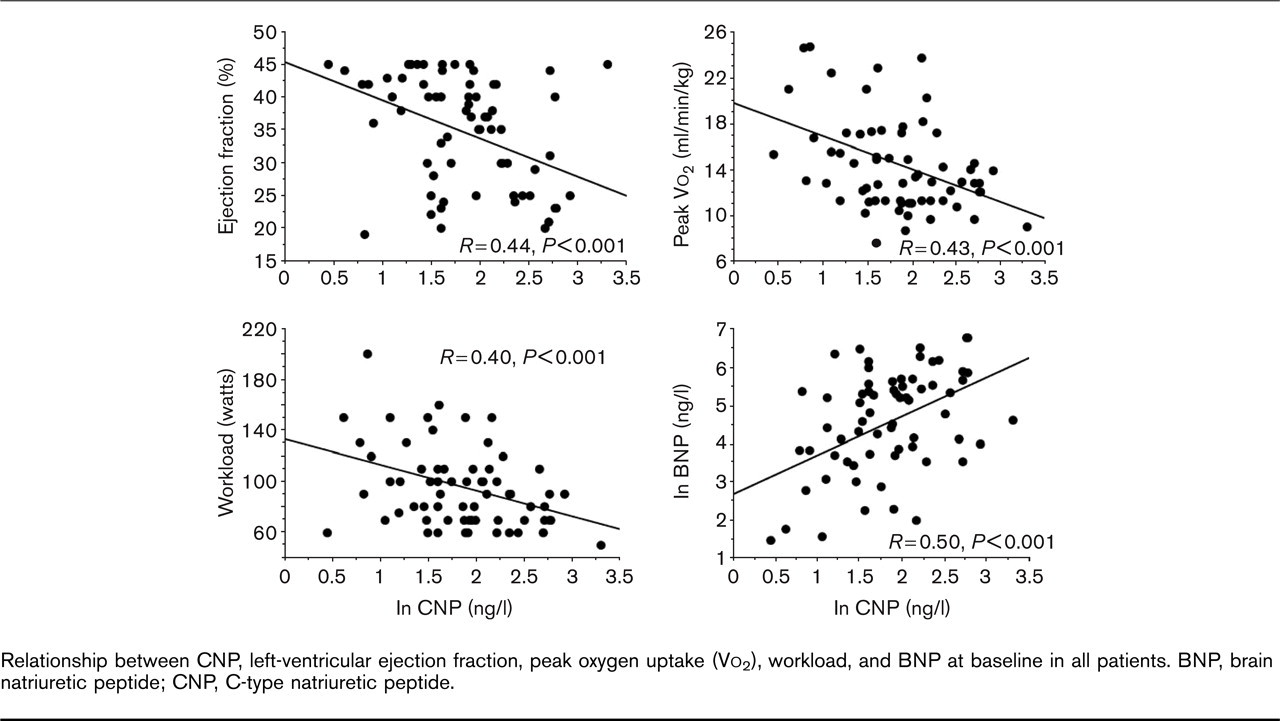
Relationship between CNP, left-ventricular ejection fraction, peak oxygen uptake (Vo2), workload, and BNP at baseline in all patients. BNP, brain natriuretic peptide; CNP, C-type natriuretic peptide.
Patients on stable pharmacological treatment (group C) did not show significant changes in plasma neurohormone levels, whereas norepinephrine (P [ 0.05), BNP (P [ 0.001), and CNP (P [ 0.01) decreased in group T (Fig. 2 and Table 2). The increase in peak Vo2 at the end of the program was correlated with the decrease in CNP plasma concentration (R = 0.31, P [ 0.01). In group T, the relationship between BNP and CNP was intact, although slightly reduced, at the end of the period of training (R = 0.41, P [ 0.001), and the absolute variations between the two hormones were weakly correlated (0.23, P [ 0.01). The relationship between CNP and norepinephrine, found at baseline, was lost at the end of the training program.
Baseline and ninth-month cardiopulmonary and neurohormonal data in the training (T) or control (C) groups
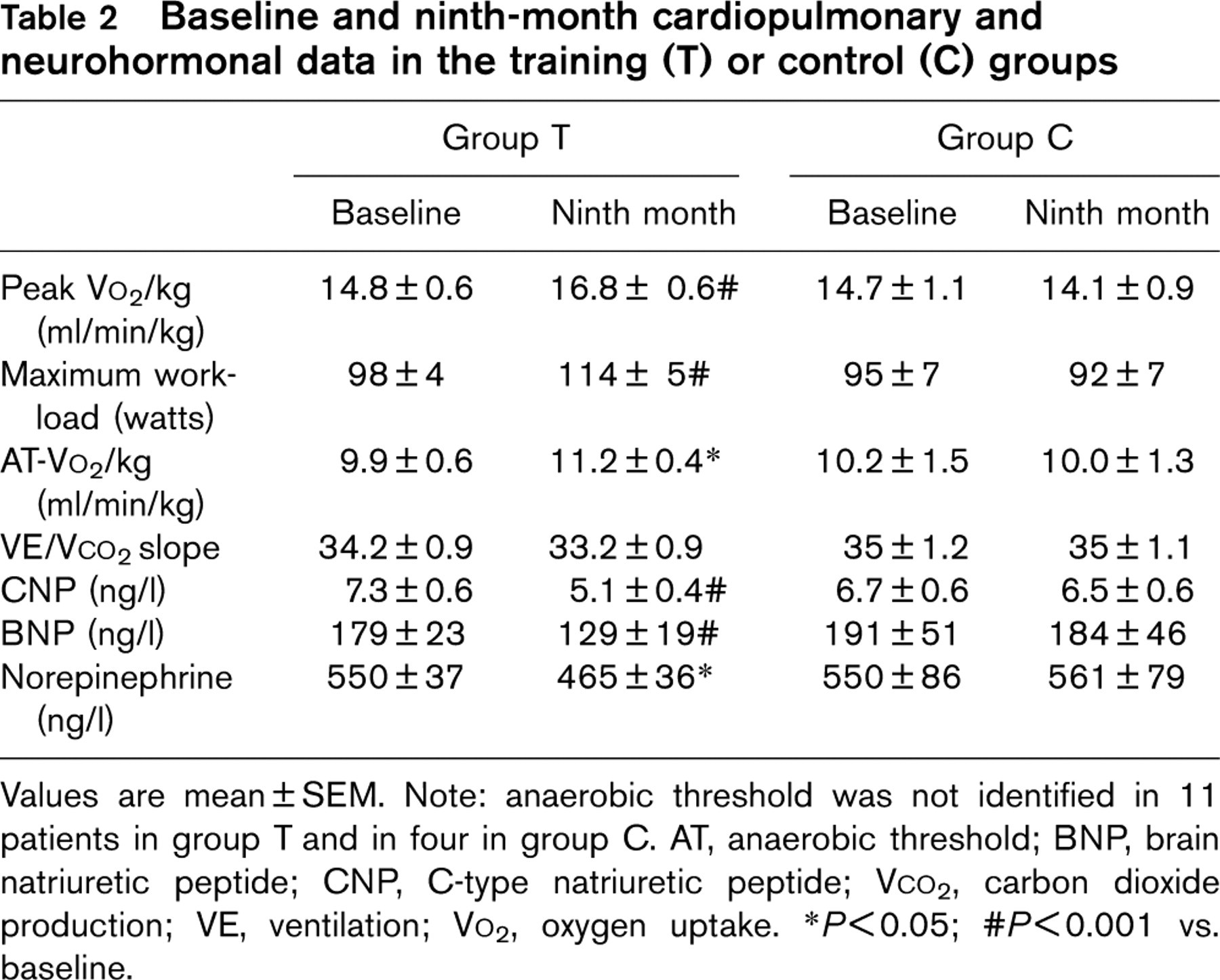
Values are mean ± SEM. Note: anaerobic threshold was not identified in 11 patients in group T and in four in group C. AT, anaerobic threshold; BNP, brain natriuretic peptide; CNP, C-type natriuretic peptide; Vco2, carbon dioxide production; VE, ventilation; Vo2, oxygen uptake.
∗ P[0.05; #P[0.001 vs. baseline.
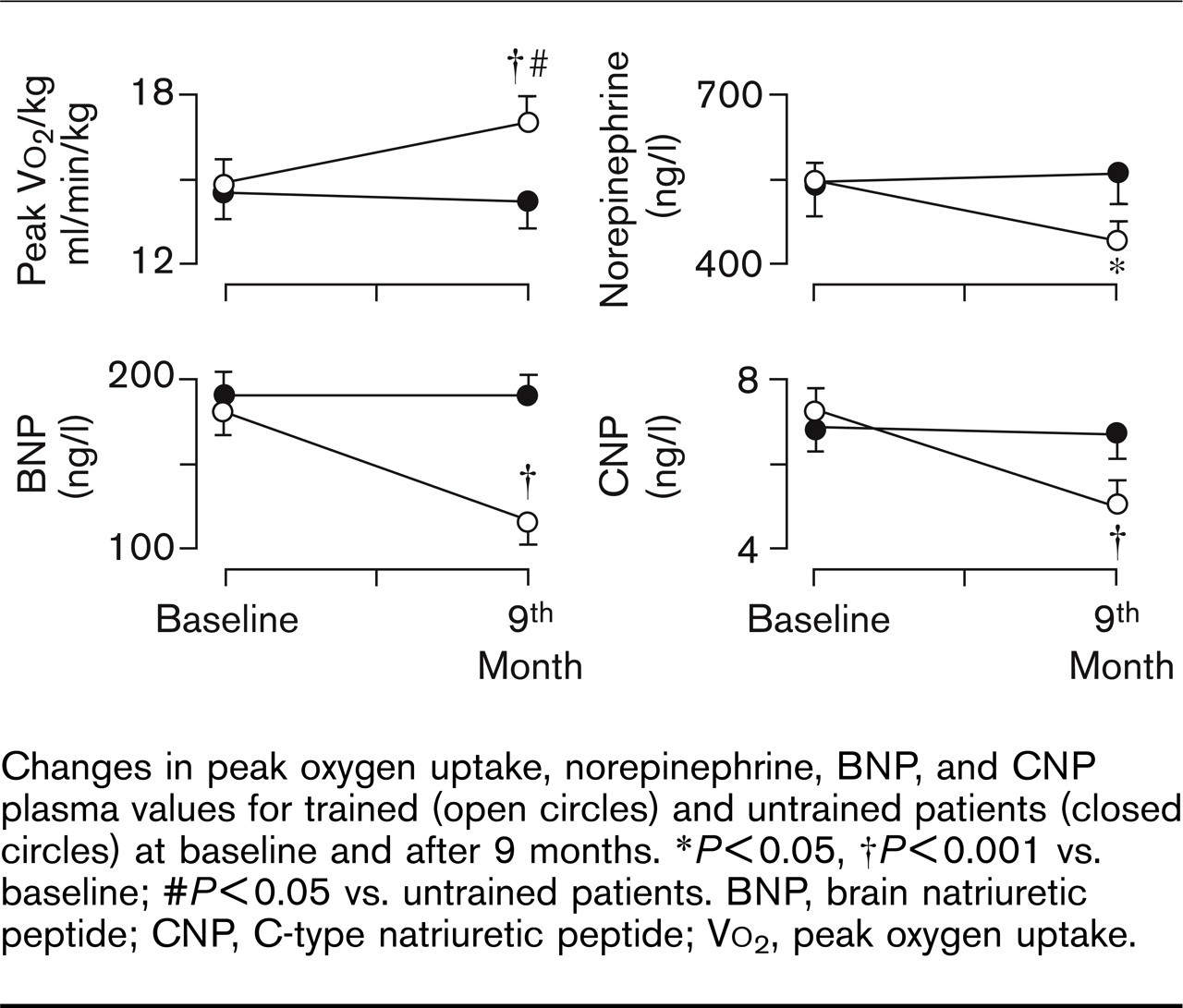
Changes in peak oxygen uptake, norepinephrine, BNP, and CNP plasma values for trained (open circles) and untrained patients (closed circles) at baseline and after 9 months. ∗P[0.05, †P[0.001 vs. baseline; #P[0.05 vs. untrained patients. BNP, brain natriuretic peptide; CNP, C-type natriuretic peptide; Vo2, peak oxygen uptake.
Effects of the etiology of left-ventricular dysfunction on the C-type natriuretic peptide response to training
Patients in group T were divided according to etiology into two groups (i.e. 32 idiopathic vs. 39 ischemic). Despite the ischemic patients being older and with more severe symptoms than the idiopathic patients (age: 64 ± 2 vs. 56 ± 2 years, P [ 0.01; NYHA class: 2.1 ± 0.1 vs. 1.8 ± 0.1, P [ 0.05; EF: 34.0 ± 1.4 vs. 36.6 ± 1.4%, P = NS; peak Vo2: 13.2 ± 0.4 vs. 16.9 ± 1.0 ml/min/kg, P [ 0.001; and BNP: 215 ± 35 vs. 130 ± 26 ng/l, P [ 0.05), the effect of physical training on plasma CNP levels was similar: from 8.8 ± 0.8 to 5.9 ± 0.5 ng/l (P [ 0.01) in ischemic patients and from 6.3 ± 0.7 to 3.8 ± 0.4 ng/l (P [ 0.001) in idiopathic patients.
Discussion
This is the first study demonstrating that CNP plasma concentration can be positively affected by a therapeutic intervention, such as physical training, in HF patients. The results of this study confirm previous reports [10–12] of the positive effects exerted by progressively adjusted aerobic physical training on adrenergic activation and on cardiac endocrine function (i.e. BNP expression), in addition to the recognized beneficial effects on functional capacity and left-ventricular function. The reduction in natriuretic peptide expression has been attributed to exercise-induced improvement in hemodynamic conditions, tissue oxygenation [6,12,15], and restored sympathovagal balance [11].
The observed decrease in CNP plasma concentration after physical training was independent of the etiology of HF, and might be an expression of the same mechanisms: indeed, a clear relationship between CNP, clinical severity, and cardiac function has been previously demonstrated [7]. Moreover, paracrine secretion of CNP is elicited by both ANP and BNP [5]: a reduction in their production and secretion after physical training could directly affect CNP plasma concentration. Loss of the correlation between norepinephrine and CNP after the period of physical training in group T and the weak relationship between the exercise-induced changes in BNP and CNP, however, suggest that other mechanisms could contribute to the decrease in plasma CNP.
Endothelial dysfunction is a rather common finding in patients with HE as evidenced by attenuated vasodilation in response to acetylcholine and reduced ischemic vasodilation during reactive hyperemia [8,9]. A partial correction of endothelial dysfunction can be achieved after an aerobic exercise-training program [13,14,16,17], in patients with HF: intermittent chronic shear stress is a postulated mechanism contributing to the beneficial effect of aerobic physical training on endothelial function, in HF. Experimental data have demonstrated that increased shear stress increases nitric oxide synthase gene expression in endothelial cell cultures [18], and that a training program increases vascular nitric oxide production and nitric oxide synthase gene expression [19]. These observations support the idea that repetitive increases in shear stress by physical training can induce the enhanced synthesis and release of nitric oxide through an upregulation of the nitric oxide synthase [13], resulting in an improvement of endothelial function in patients with HF. The improvement of the endothelial function could therefore result in a diminished stimulus to CNP secretion, leading to a decrease in plasma concentrations of the hormone at the end of a period of aerobic training. Further studies are, however, required to assess the direct link between plasma CNP concentration and endothelial function.
Limitation of the study
The low prevalence of women in this population does not allow the extending of the results of this study to patients of both sexes. As CNP is a recognized local mediator with a half-life of few minutes [4], CNP circulating levels might not reflect the tissue concentration. Furthermore, until a clear relationship between CNP plasma levels and endothelial function is established, changes in CNP plasma levels cannot be assumed to be expressions of changes in endothelial function.
In conclusion, CNP plasma level progressively decreases after physical training, whereas functional and neurohormonal improvement takes place in HF patients. Changes in CNP plasma concentration after physical training might be expression of an improved endothelial function after physical training, suggesting the potential use of CNP assay for follow-up in HF patients.
Footnotes
Acknowledgements
The authors thank Ms Maristella Maltinti and Mr Guido Nassi for their technical support and Mr Luc Zyw for statistical advice.
Conflict of interest: none declared.