
Abstract
Introduction
Exercise therapy provides many benefits to people with chronic heart failure (CHF), while some information exists on the effects of exercise training on BNP levels in heart failure patients, 1 evidence may be equivocal due to the magnitude of the standard deviation measured for both brain natriuretic peptide (BNP) and the N-terminal portion (NT-pro-BNP). 2 – 4 Moreover a recent systematic review has shown both BNP and NT-pro-BNP to be modulated after exercise training although this conclusion was based on post-training data only and assumptions that participant groups were matched at baseline. 5 We therefore sought to establish, via an individual patient meta-analysis whether exercise training is able to modulate systemic BNP, NT-pro-BNP and functional capacity levels in heart failure patients. We also sought to examine the relationship between changes in BNP/NT-pro-BNP and peak VO2, patient characteristics and the volume parameters of exercise training regimes.
Methods
Following the acceptance for publication of a systematic review evaluating the effects of exercise training on BNP and NT-pro-BNP, 5 a collaborative group was coordinated from Bond University, Australia. Prospective data collection was agreed and a common dataset of collected variables was sent to the included study authors.
Search strategy
Potential studies were identified by a systematic review librarian (ST). The search was conducted of Medline (Ovid) (1950−January 2010), Embase.com (1974−January 2010), Cochrane Central Register of Controlled Trials and CINAHL (1981−January 2010). The search strategy included a mix of MeSH and free text terms for the key concepts heart failure, exercise training, and brain natriuretic peptide and these were combined with a sensitive search strategy to identify randomized controlled trials. Reference lists of papers found were scrutinized for new references. All identified papers were assessed independently by two reviewers.
Inclusions
Randomized, controlled trials of exercise training in heart failure patients, for a minimum of 12 weeks, with a primary or secondary outcome measure of BNP or NT-pro-BNP were included.
Exclusions
Animal studies, review papers and non-randomized controlled trials were excluded. Studies that did not have desired outcome measures (BNP or NT-pro-BNP) or participants who were non-heart failure or healthy in either treatment or control groups were also excluded. Authors were contacted to provide missing data or to clarify if data was duplicated in multiple publications by the same author or research group, and incomplete data or data from an already included study resulted in exclusion. Studies of physical therapy other than aerobic or strength exercise and acute exercise rather than training response studies were excluded.
Studies included in the review
We examined conference proceedings and the latest editions of relevant journals not yet available on electronic databases. Initial screening identified 126 potential reports; 94 were not randomized trials of exercise training in heart failure patients, four were animal studies, and nine were drug studies, leaving 19 full manuscripts for review. Two groups had reported information from the same trial in more than one publication, one study was excluded because only some patients had congestive heart failure. Five studies had used other types of physical therapy, e.g. electrical stimulation that were considered heterogeneous compared to exercise training. One study was excluded because of selective (incomplete) outcome reporting, leaving ten eligible trials. Two studies had conducted more than one similar trial. Individual patients were therefore combined into one dataset for these trials, yielding eight non-overlapping datasets meeting the eligibility criteria.
Selection and validity assessment
All principal investigators provided anonymized individual patient data for originally randomized patients. Datasets included age, gender, medication [beta-blocker, angiotensin-converting enzyme (ACE) inhibitor, angiotensin receptor blocker (ARB), spironolactone, diuretic] brand and dosage, ischaemic vs. non-ischaemic causes, New York Heart Association (NYHA) functional class, left ventricular ejection fraction, peak oxygen consumption, and exercise adherence.
Included datasets were randomized parallel group controlled trials assessing effects of exercise training on BNP and/or NT-Pro-BNP levels. Patients with left ventricular ejection fraction >50% or peak VO2 >24 ml O2/kg/min were removed from the database as these patients were deemed atypical of CHF patients. Datasets were checked for completeness and consistency with original publications. Queries were resolved by communication with principal investigators.
Data synthesis
Data relating to BNP and NT-pro-BNP, heart failure patient characteristics, and exercise training protocols were reviewed. Primary outcome measures following exercise training were post-exercise change in BNP, NT-pro-BNP, and peak VO2. Secondary outcome was exercise programme energy expenditure. Measures of study quality were also recorded such as interstudy variation in age, gender, functional status e.g. NYHA score, left ventricular ejection fraction (LVEF), and cardiac medications.
Subgroup meta-analysis of dichotomous end points
The effect of exercise training was also evaluated in pre-specified subgroups: ischaemic vs. non-ischaemic causes, gender, beta-blocker use, age (<60 and ≥60 years), body mass index (BMI) (<27 vs. ≥27), peak oxygen uptake (<14 ml/kg/min vs. ≥14 ml/kg/min), LVEF (<34% vs. ≥34%). The continuous variables were dichotomized. The BMI and LVEF criteria were selected because previous randomized trials and meta-analyses of heart failure exercise training studies have shown these to be mean values. 6 − 8 Subanalyses were also conducted according to change in peak VO2 as outlined by Balady et al. 9 So three categories were used, those who showed more than a + 5% change (positive responders) in peak VO2, neutral responders < ± 5%, and negative responders showed more than a 5% fall in peak VO2.
Exercise programme parameters
Where possible we calculated, using established methods, 10 work completed during exercise training (kcal) and mean weekly calorie expenditure, in order to determine a dose−response relationship with change in BNP or NT-pro-BNP, disease severity, and clinical characteristics of CHF participants.
Statistical analysis
SPSS version 17.0 was used to conduct meta-analyses for BNP, NT-pro-BNP, and peak VO2 following exercise training. As BNP and NT-pro-BNP data were not normally distributed, BNP and NT-pro-BNP were reported as median and interquartile range, all remaining data were reported as mean and standard deviation. We assessed inter- and intragroup differences in BNP and NT-pro-BNP using non-parametric statistics (Wilcoxon signed ranks). We analysed differences between baseline and post-intervention using repeated-measures ANOVA. If there was significant interaction from the ANOVA, paired t-tests calculated intragroup significance. Appropriate correlation coefficients were calculated for change (normally distributed for BNP and NT-pro-BNP) in primary outcome measures. We used a 5% level of significance and a 95% confidence interval to report outcome measure changes.
Results
Study characteristics
Ten randomized, controlled studies (eight discrete datasets, overlapping data was not duplicated) met our eligibility criteria, with an aggregate number of 565 subjects (313 exercise participants and 252 controls) 3 −4,11− 18 were included. Five studies measured BNP, six measured NT-pro-BNP, and one study measured NT-pro-BNP and BNP. BNP data from 230 patients, NT-pro-BNP data in 466 patients, and both BNP and NT-pro-BNP in 133 patients were available.
Participant characteristics
Baseline clinical, demographic, and pharmacological characteristics of exercise and control group patients
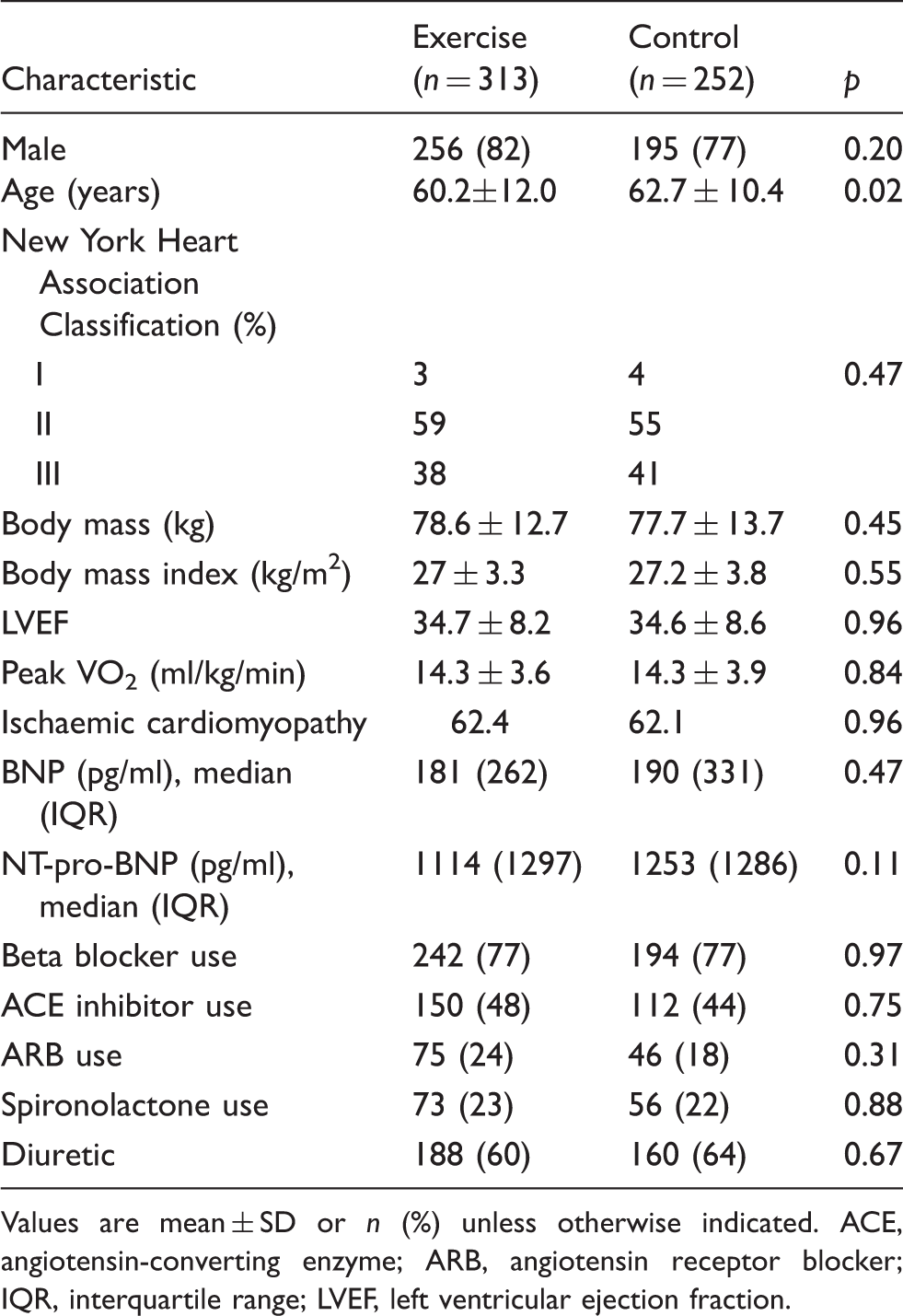
Values are mean ± SD or n (%) unless otherwise indicated. ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; IQR, interquartile range; LVEF, left ventricular ejection fraction.
Exercise programme parameters
All but one study utilized cycling as the exercise mode. 18 Training frequency was 2–7 weekly sessions, intensity 50–95% of peak VO2, 30–50 minutes per session, and 3–9 month duration. Energy expenditure calculations were possible in all but one study, 11 only the aerobic, not resistance, activity was calculated in one study. 14 Mean weekly energy expenditure was 457 ± 135 kcal/week and when multiplied by completed exercise sessions, the exercise participants were estimated to have expended 430 ± 127 kcal/week or 94% of target.
Change in BNP and NT-pro BNP
Baseline and post-intervention changes in peak oxygen consumption (VO2), brain natriuretic peptide (BNP), and N-terminal portion of BNP (NT-pro-BNP) in exercise and control group patients
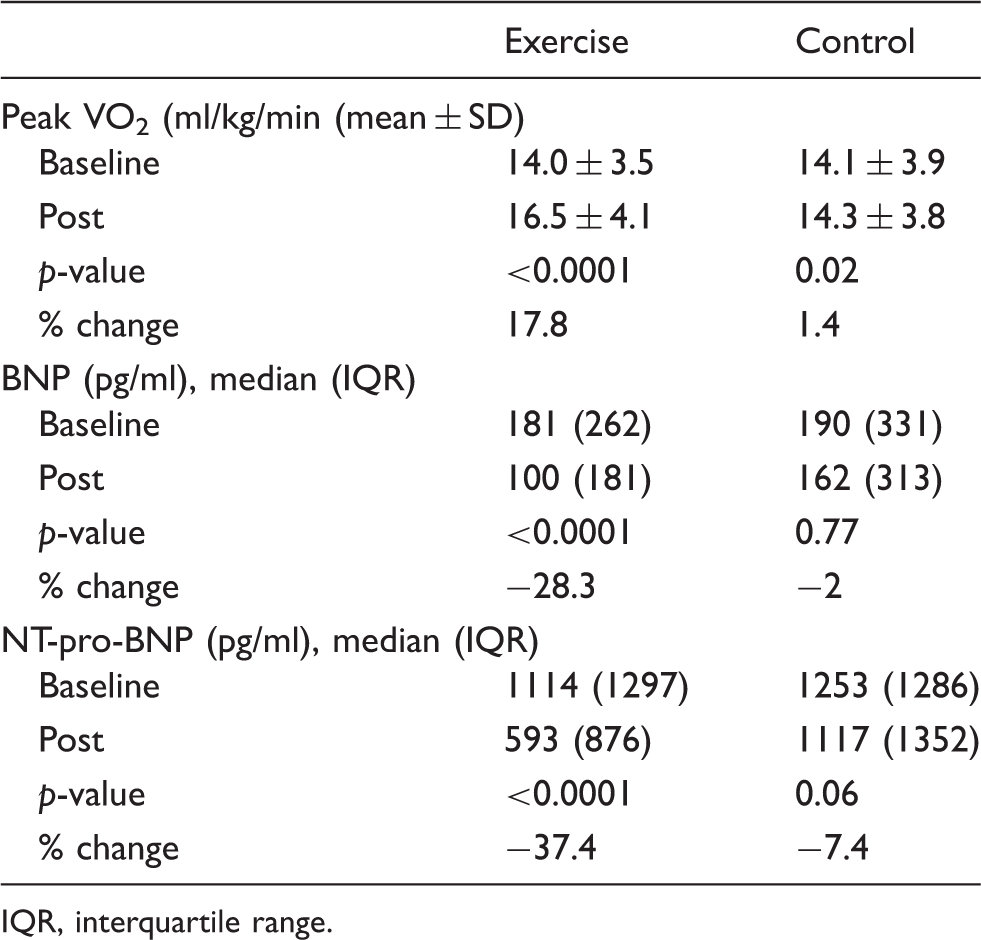
IQR, interquartile range.
Sensitivity analyses
We conducted sensitivity analyses, removing studies where we were unable to calculate exercise energy expenditure. After sensitivity analysis (removal of the two studies) significant changes in both BNP and peak VO2 remained; however, the increment of change was unaltered.
Correlates of baseline primary outcome measures in all patients
Baseline measures of peak VO2 and BNP (r = −0.33, p < 0.001) and NT-pro-BNP (r = −0.32, p < 0.001) were both inversely correlated.
Correlates of change in primary outcome measures in the exercise training group
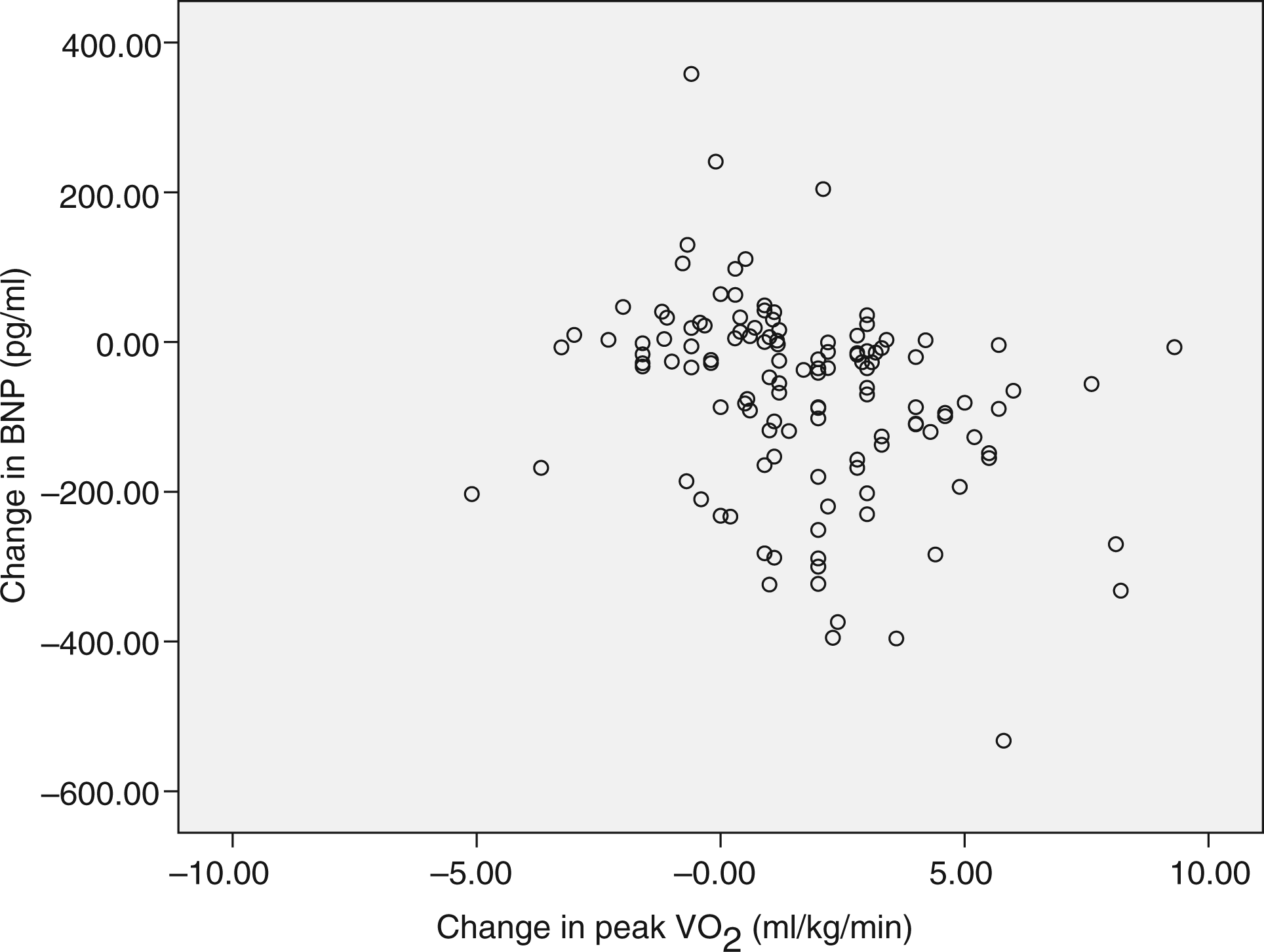
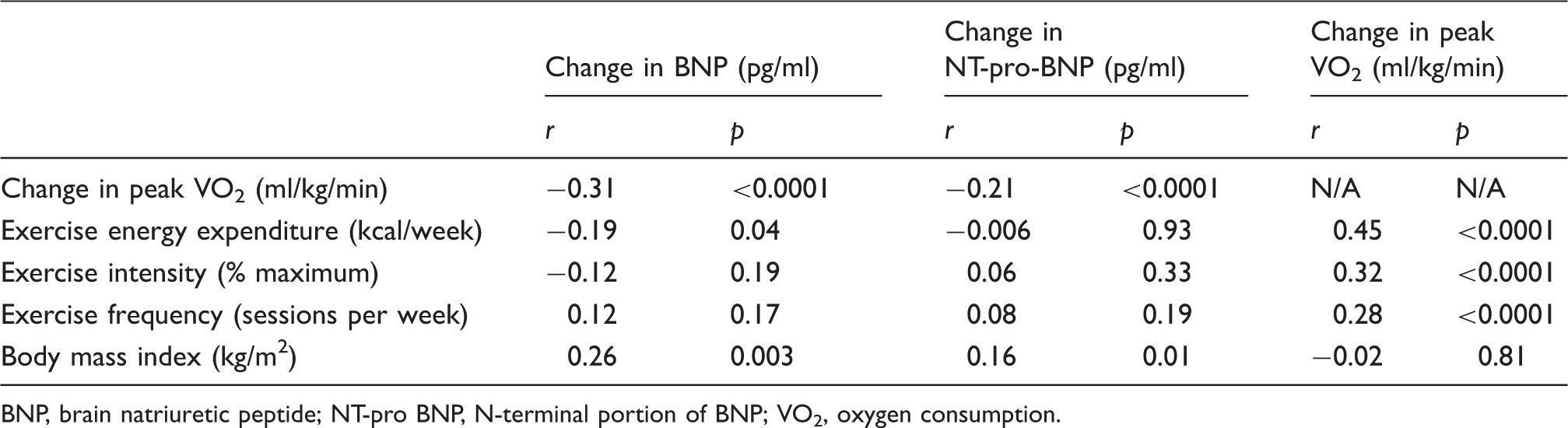
Correlation coefficients showed inverse relationships between change in peak VO2 and change in BNP (r = −0.31, p < 0.0001) and NT-pro-BNP (r = −0.21, p = 0.001): see Figures 1 and 2. Change in BNP was also related to exercise energy expenditure (r = −0.19, p = 0.04). Body mass index was correlated with both change in BNP (r = 0.26, p = 0.003) and NT-pro-BNP (r = 0.16, p = 0.01). Other correlation coefficients can be seen in Table 3.
Correlation of change in peak oxygen consumption (VO2) and N-terminal portion of brain natriuretic peptide (NT-pro-BNP). Correlation of change in peak oxygen consumption (VO2) and brain natriuretic peptide (BNP). Correlation between change in primary outcome measures and other markers of prognosis in patients undertaking exercise training BNP, brain natriuretic peptide; NT-pro BNP, N-terminal portion of BNP; VO2, oxygen consumption.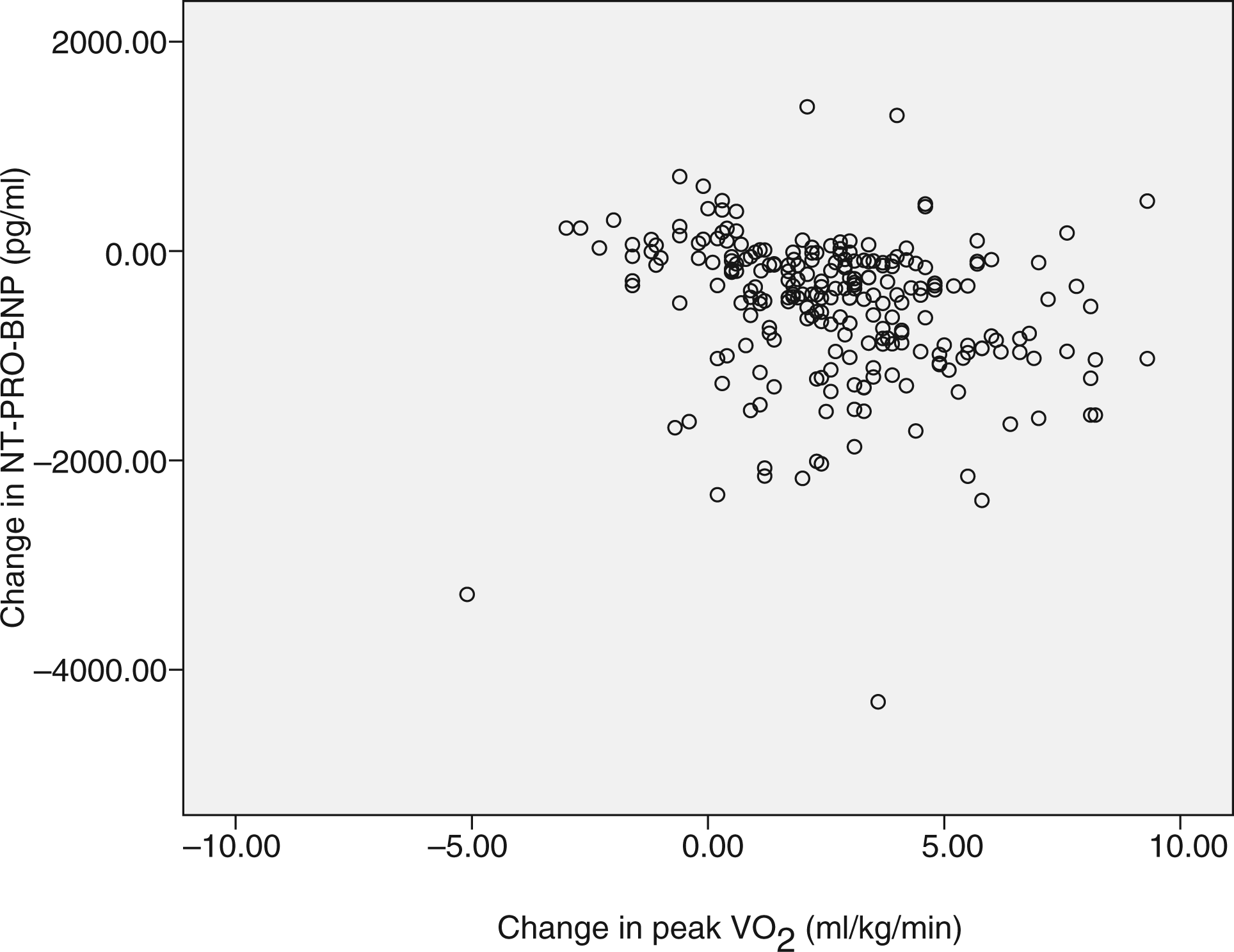
Training response
The exercise training group (n = 284) was further divided into 227 patients (80%) who exhibited a positive training response (5% or greater increase in peak VO2), 37 patients (13%) with ‘neutral’ response, and 20 patients (7%) showing a negative response. Those patients with a positive training response showed a greater reduction in both BNP and NT-pro-BNP compared to both neutral and negative responders (all p < 0.003).
Subanalyses
Subanalysis of predictors of change prognosis in patients undertaking exercise training
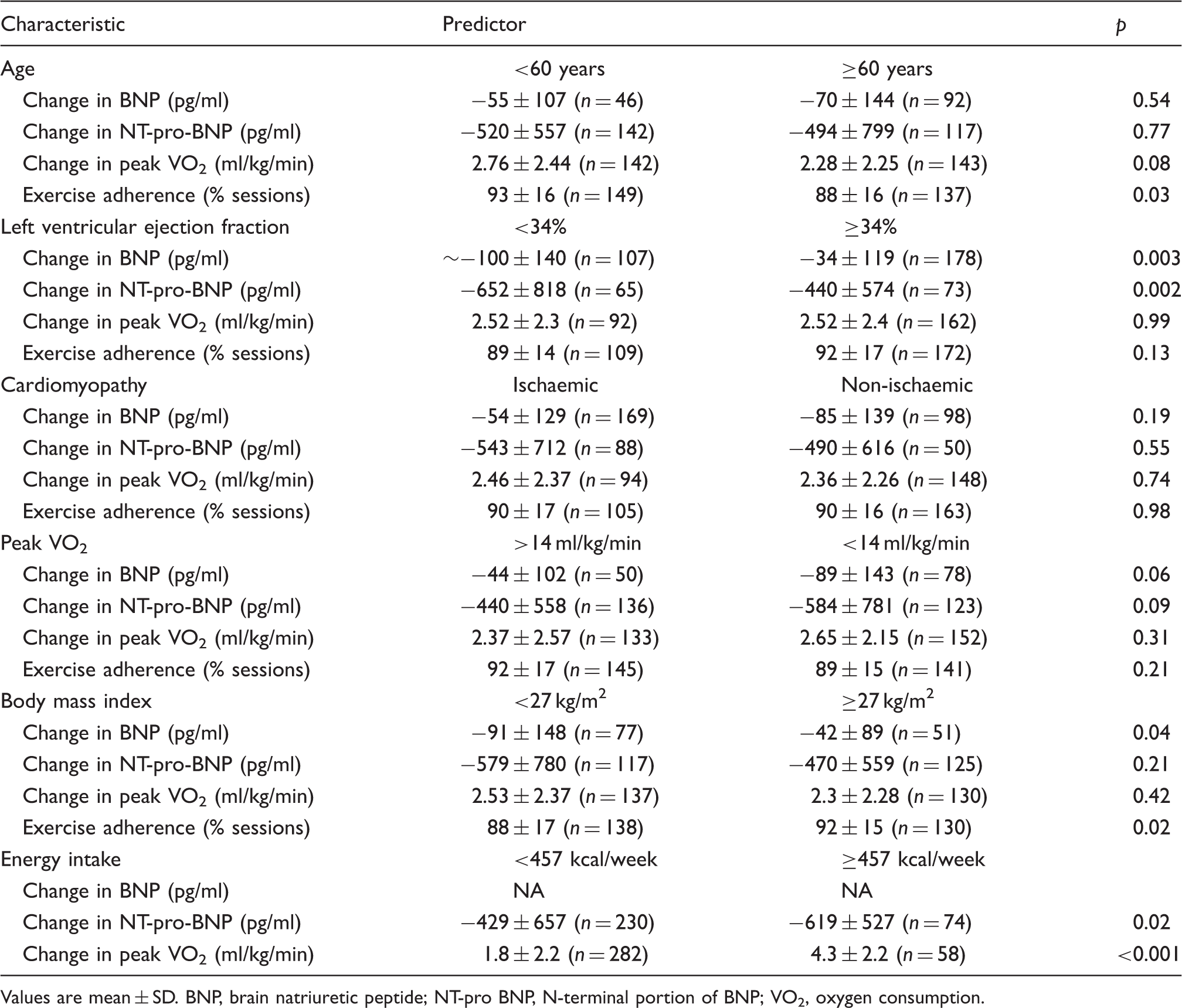
Values are mean ± SD. BNP, brain natriuretic peptide; NT-pro BNP, N-terminal portion of BNP; VO2, oxygen consumption.
Discussion
Ten published studies, with an aggregate of 565 subjects allowed an individual patient meta-analysis of the effect of exercise training on BNP and NT-pro-BNP in CHF patients. At baseline BNP and NT-pro-BNP values were both predictors of peak VO2. Analyses of BNP and NT-pro-BNP demonstrated overall reductions and an improvement in peak VO2 following exercise training. Statistical significance of these changes remained after conducting sensitivity analyses.
Participants were generally well matched at baseline for clinical, demographic and pharmacological characteristics. Previous data from exercise training studies in heart failure patients suggest the majority are male.6,8 One study used NYHA class I, as well as class II and III patients. Mean LVEF was 34%.
Both BNP and NT-pro-BNP showed an inverse relationship with peak VO2 at baseline. Baseline BNP and NT-pro-BNP can be considered additional criteria for selecting exercise training candidates and appear surrogates of peak VO2 in evaluating exercise training response and prognosis in heart failure. Recent work has shown NT-pro-BNP to predict peak VO2 in heart failure patients. 1 Change in BNP was 28% vs. 2% in the exercise vs. control groups, respectively. Similarly the change in NT-pro-BNP was 37 vs. 7% in the exercise vs. control groups, respectively. Both groups significantly improved their functional capacity (peak VO2) from baseline, although the magnitude of change was only 1.4% in the control group compared to 18% in the exercise group. One could speculate that the improvement in functional capacity in the control group could be attributed to habituation to the exercise test, degree of effort spent, 19 or effects of optimal medication. A net improvement of 16.6% in peak VO2 is consistent with previous reports. 8 Our data suggested that beta-blockade did not attenuate exercise training effects on BNP, NT-pro-BNP and functional capacity. Rosenberg reported that 6 months of ACE inhibition (enalapril), but not beta-blockade (carvedilol), lowers BNP levels in heart failure patients, 20 while other work reported that metoprolol causes plasma BNP/NT-pro-BNP to rise. 21
Change in both BNP and NT-pro-BNP were correlated with change in peak VO2 and BNP change was correlated with mean weekly exercise energy expenditure. Data from the heart failure action study (HF-ACTION) supports the notion that NT-pro-BNP is a strong predictor of peak VO2. 1 The two exercise training programmes yielding the lowest mean weekly energy expenditures did not show significant changes in BNP,11,14 while our analyses (Table 4) suggest about 460 kcal/week may be required to change BNP. The work by Wisloff et al. 18 reported that high intensity intermittent exercise was effective in significantly reducing NT-pro-BNP while a comparative group performing continuous moderate intensity exercise of isocaloric energy expenditure did not alter NT-pro-BNP levels. We calculated that mean weekly exercise energy expenditure of the participants of Wisloff’s 18 study was 505 kcal/week. It may be that the very small sample size (n = 9 for each group) and the relatively short study duration (12 weeks) may have precluded NT-pro-BNP changes in the moderate exercise intensity group. Our data did not suggest that 12 weeks was as effective as 39 weeks exercise training programme in eliciting BNP and NT-pro-BNP changes.
Previous work has suggested that reductions in BNP following exercise training may be due to blunted neurohormonal responses at rest. 3 It has been shown that exercise training ameliorates sympatho-vagal balance22,23 and reduces sympathetic outflow, plasma catecholamines, angiotensin II, vasopressin, and brain natriuretic peptides at rest. 24 Patients with ejection fraction <34% showed a greater improvement in both BNP and NT-pro-BNP, this is unsurprising as natriuretic peptides are released in response to myocardial stretch and those with lower ejection fraction have greatest improvement potential. Body mass index showed a positive correlation with change in both BNP and NT-pro-BNP, therefore lower body mass may be related to greater lowering of natriuretic peptides. Future short-term research might aim at linking changes in BNP and NT-pro-BNP with improved myocardial function, body composition, and blunted neurohormonal responses at rest. Longer studies, with larger sample size, may be able to demonstrate a link between exercise-induced BNP/NT-pro-BNP decrease and reduced morbidity, healthcare costs, and mortality in CHF patients.
Conclusions
Data from published studies, suggest exercise training has a favourable effect on BNP and NT-pro-BNP in heart failure patients; moreover, the changes in natriuretic peptides were related to functional capacity change. Baseline BNP and NT-pro-BNP can be considered additional criteria for selecting exercise training candidates and appear surrogates of peak VO2 in evaluating exercise training response and prognosis in heart failure. Exercise intensity and weekly minimum exercise energy expenditure around 460 kcal may determine the magnitude of change in BNP and the N-terminal portion of BNP in heart failure patients.
Footnotes
Funding
Ulrik Wisloff received funding from the KG Jebsen Foundation and Norwegian Research Council granting bodies. Jon Butterworth received equipment from ALERE, Australia.