
Abstract
Background
Methods
Results
Conclusion
Introduction
Serum C-reactive protein (CRP) is a sensitive indicator of inflammation [1] and is actually considered a new marker of increased risk of cardiovascular events [2–8]. Consistent results from clinical studies indicate that high CRP levels predict recurrent instability in patients with acute coronary syndrome [9, 10] or undergoing coronary angioplasty [11, 12], and are a strong predictor of hospital readmission in patients with heart failure [13]. Furthermore, an increase in CRP is a common finding in the acute phase reaction after a surgical trauma, and serial measurements seem to be useful for quantifying the degree of tissue damage, the invasiveness of the procedure, and the early detection of surgical complications, especially infective [14–18].
In cardiac surgery, CRP is involved in the systemic inflammatory response syndrome [19, 20], a complex reaction that occurs during the first week after surgery, and despite it increasingly being used as a reliable marker for stratification, the results are still controversial. Although in some studies preoperative levels of CRP seemed to be predictive of postoperative outcome and complications [21–24], in others they did not provide predictive information [25–27]. Most of these studies, however, included patients with different clinical conditions, in the immediate postoperative period, with different lengths of follow-up and different outcomes, using various measurement methods and cutoff values of CRP. One of the reasons for this inconsistency is that the data supporting the significance of CRP after (cardiac) surgery were derived from populations at two extremes: individuals with signs or symptoms of infection, which are common complications in the postoperative period, and patients with a ‘lone’ increase in CRP in the absence of signs or symptoms of infection. We hypothesized that in the latter group a CRP increase may represent a biomarker due to distressed or injured tissue in response to surgery stress, with a favorable prognosis. On the basis of these concepts, we sought to determine the prevalence, clinical characteristics, time course, and prognostic value of the ‘lone’ increase in CRP in cardiac surgery patients referred to a Cardiac Rehabilitation program.
Methods
Seven hundred and thirty seven consecutive patients referred to our cardiac rehabilitation unit 8 ± 5 days after cardiac surgery were considered potentially eligible for this investigation. Patients with either fever (> 37.2°C), elevated white blood cell count (> 11000/ml), neutrophilia (> 70%), cardiac surgery in the setting of an acute coronary syndrome, perioperative myocardial infarction defined by WHO criteria [28], any inflammatory, infection or malignant disease were excluded. In addition, patients using corticosteroids or other anti-inflammatory drugs except aspirin (100 mg) were excluded.
Blood samples were obtained within 24 h of admission and at discharge. White blood cell counts and biochemical measurements were determined by standard laboratory methods. Plasma CRP levels were measured with a high-sensitive latex-enhanced nephelometric assay (Dade Behring, Deerfield, Illinois, USA) using Dade-Behring BN 100 autoanalyzer. The lower detection limit of this test was less than 0.30 mg/dl.
CRP values were analyzed according to the following variables: age, sex, diabetes mellitus, renal failure (serum creatinine > 1.5 mg/dl), specific type of surgery performed [coronary artery bypass graft (CABG), valve surgery, thoracic aorta replacement, combined surgery], postoperative atrial fibrillation, presence of pericardial or pleural effusion, and length of hospital stay.
Follow-up data were obtained from routine follow-up visits in the outpatient cardiac clinic, or from a telephone interview with the patient conducted by a staff cardiologist. We determined the specific occurrence of cardiac events defined as all-cause death, cardiac death, and readmission to hospital for cardiac reasons (acute coronary syndromes, worsening heart failure, endocarditis, revascularization procedures). Only the first event was considered for each patient. The hospital institutional review board approved the study and informed consent was obtained for all patients.
Statistical analysis
All analysis were performed by using SPSS for Windows (version 12.0.1, SPSS Inc., Chicago, Illinois, USA.). Continuous variables are expressed as mean ± SD, median, and interquartile ranges, as appropriate. CRP value was not normally distributed; consequently, non-parametric tests were used for comparison of CRP levels between dichotomic variables (Mann-Whitney U-test) and according to surgical procedure (Kruskal-Wallis test). Spearman's correlation coefficient was calculated to examine the association between length of hospitalization and CRP value. Patients were also grouped into quartiles according to CRP and differences in clinical variables and events among quartiles were calculated by a contingency χ2 test. Event-free survival was analyzed by the Kaplan-Meier method and the log-rank was used for comparison among curves.
Results
C-reactive protein on admission and at discharge
Among the 737 eligible patients, 550 were excluded. Reasons for exclusion were the presence of fever (n = 196), elevated white blood cell count (n=238), neutrophilia (n = 343), cancer (n = 3), rheumatoid arthritis (n = 2), positive culture results and/or antibiotic therapy on admission for sepsis in the early postoperative period (n = 44). Many patients presented more than one exclusion criteria. Thus, the remaining 187 patients constituted the study population. The demographic and clinical characteristics of the study patients are reported in Table 1.
On admission, CRP levels were above the upper normal limits in all except one patient, with a median value of 4.23 mg/dl (interquartiles range: 2.68-6.64). The mean hospitalization length was 16 ± 5 days. CRP at discharge was available for 173 patients (reasons for unavailability: intentional early discharge in six patients, urgent referral to cardiac surgery for pericardial tamponade in one patient, logistic reasons in seven patients), and only six out of 173 patients (3.5%) had normal CRP levels. As shown in Fig. 1, CRP levels at discharge were significantly lower than those measured on admission (median: 1.55 mg/dl, interquartiles range: 0.84-2.37, P < 0.001). Only in 10 patients (eight males, two females) CRP levels at discharge were higher than those obtained on admission, although this difference was not statistically significant.
Clinical characteristics of the study population
CABG, coronary artery bypass graft.
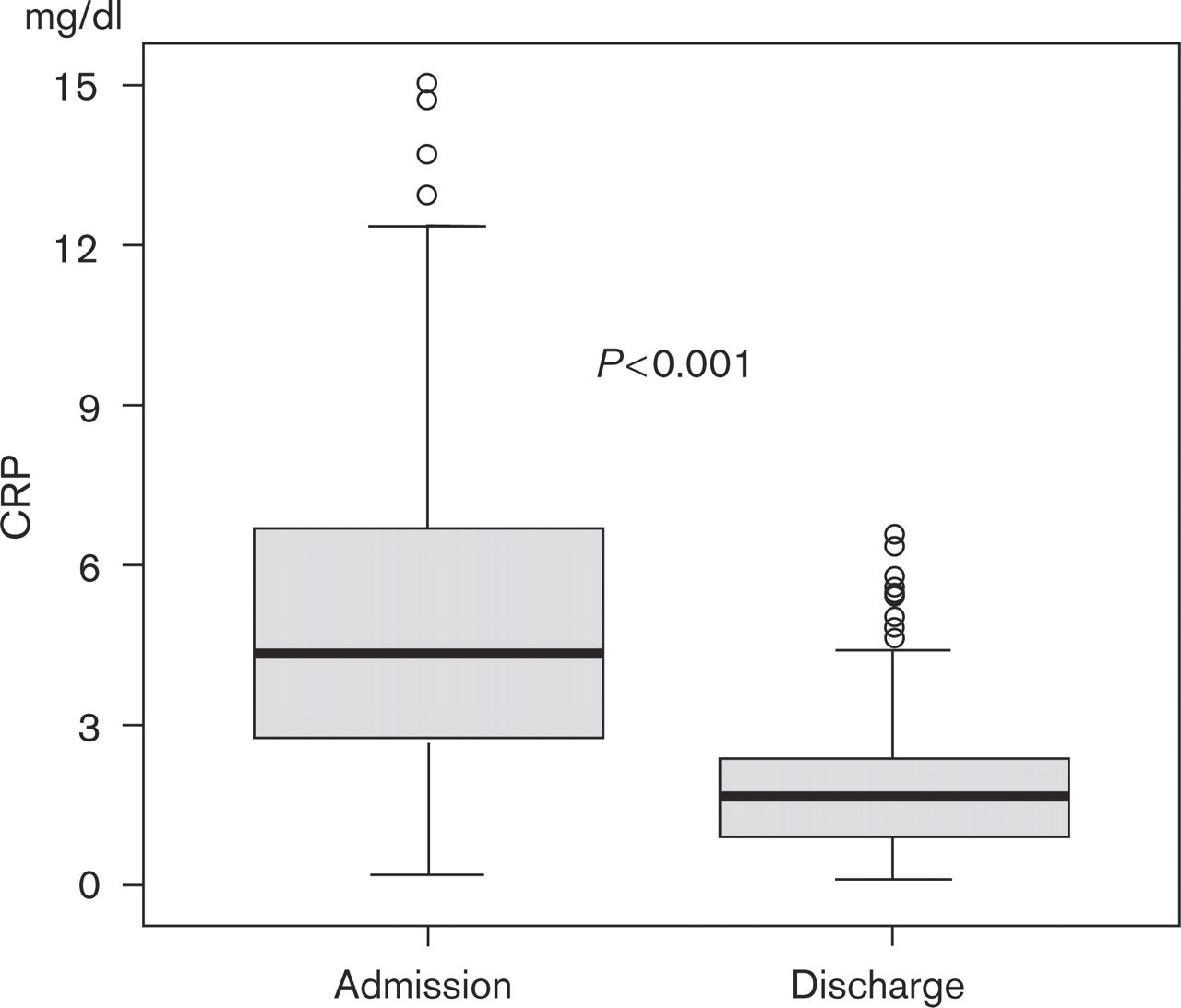
C-reactive protein (CRP) levels on admission and at discharge in the study population.
C-reactive protein and clinical variables
The relationship between CRP and the clinical variables considered is reported in Table 2. No significant difference was found in CRP values (median, interquartiles range) related to age, sex, presence of diabetes mellitus, renal failure, postoperative atrial fibrillation, and pleural or pericardial effusion either on admission or at discharge. Moreover, the length of hospitalization was independent of CRP levels either on admission or at discharge (Spearman's ρ = 0.032 and 0.036, respectively, NS). Even when considering the 10 patients with a CRP increase at discharge, no significant correlation was observed with the clinical variables considered. In this subgroup, we found only a trend toward a higher prevalence of pleural and pericardial effusion, compared with patients with a decrease in CRP levels from admission to discharge (90 vs. 76%; 50 vs. 32%, respectively, NS).
C-reactive protein (CRP) levels on admission and at discharge compared with clinical data
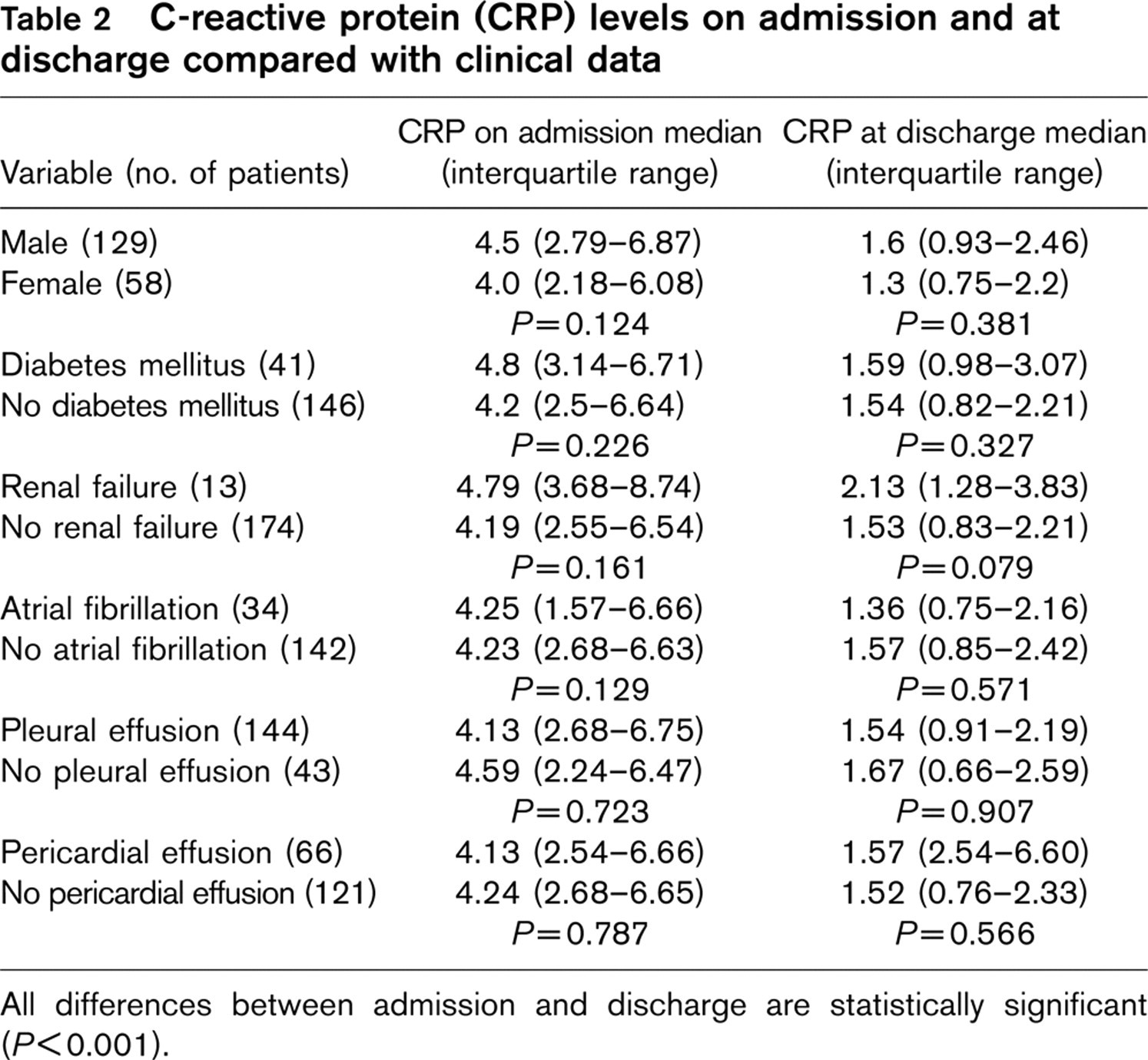
All differences between admission and discharge are statistically significant (P < 0.001).
C-reactive protein (CRP) levels on admission and at discharge compared with surgical data
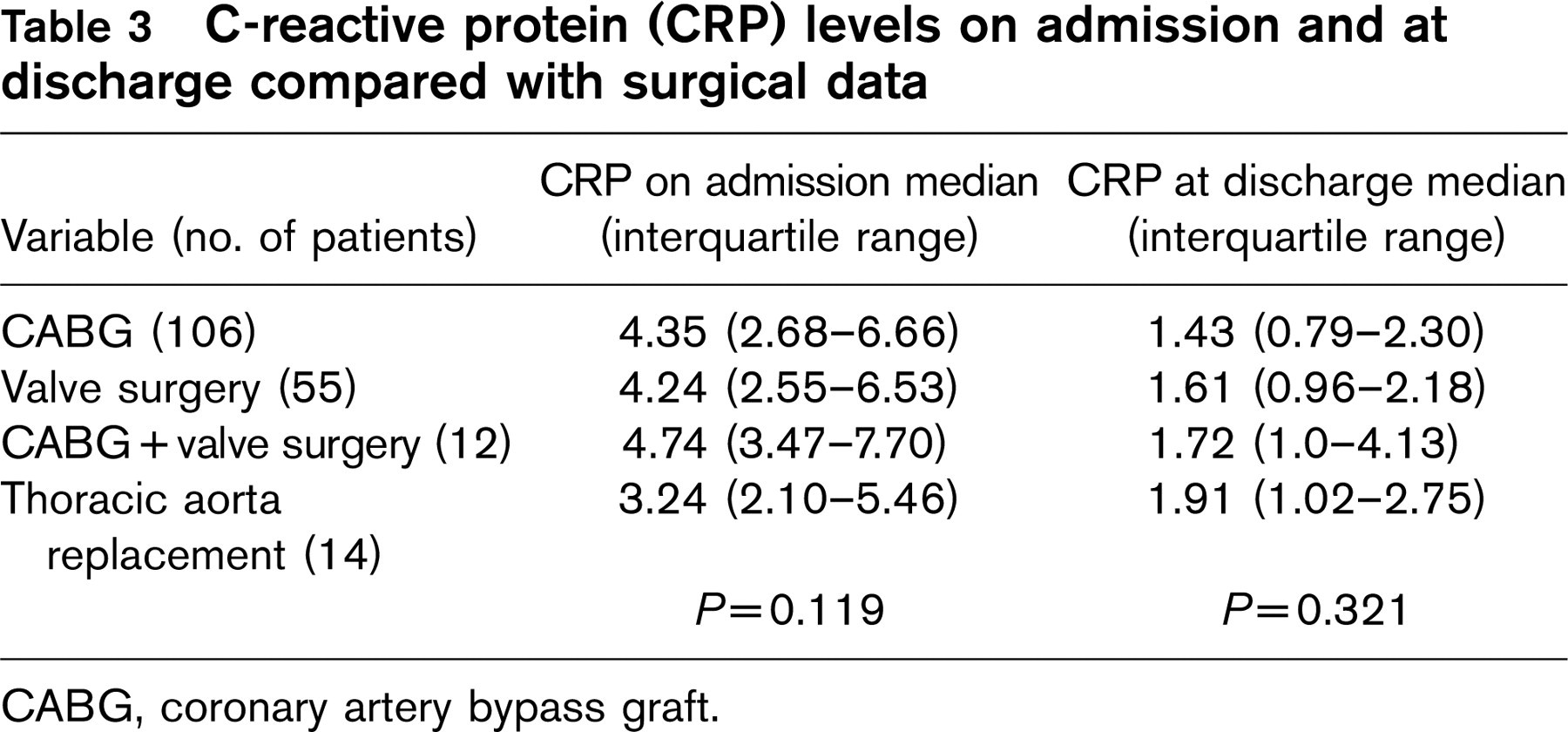
CABG, coronary artery bypass graft.
The impact of the type of cardiac surgery on CRP values is reported in Table 3. Although patients with combined CABG and valve surgery had the highest CRP levels on admission compared with patients who underwent cardiac surgery for other reasons, these differences were not statistically significant. In addition, in the subgroup of patients who underwent CABG (n = 106), CRP values were similar between patients who underwent on-pump as compared with off-pump surgery (median: 4.5, interquartiles range: 2.68-6.63, vs. 4.02, 2.41-7.05, respectively, NS).
Patients were divided into four groups according to CRP quartiles defined as less than 2.68 mg/dl, 2.68-4.23 mg/dl, 4.24-6.64 mg/dl, and greater than 6.64 mg/dl. When considering the CRP quartiles, the four groups were similar as for the clinical variables analyzed.
Follow-up
Follow-up was available for 176 patients (94%). The mean length of follow-up was 23 ± 8.5 months (range: 3-39 months). Overall, 19 events (10.8%) occurred: noncardiac death (malignancy, n = 2) and hospital readmission (n=17). Reasons for rehospitalization were acute coronary syndrome (n = 8), heart failure (n=7), coronary angioplasty (n = 1), and endocarditis (n = 1).
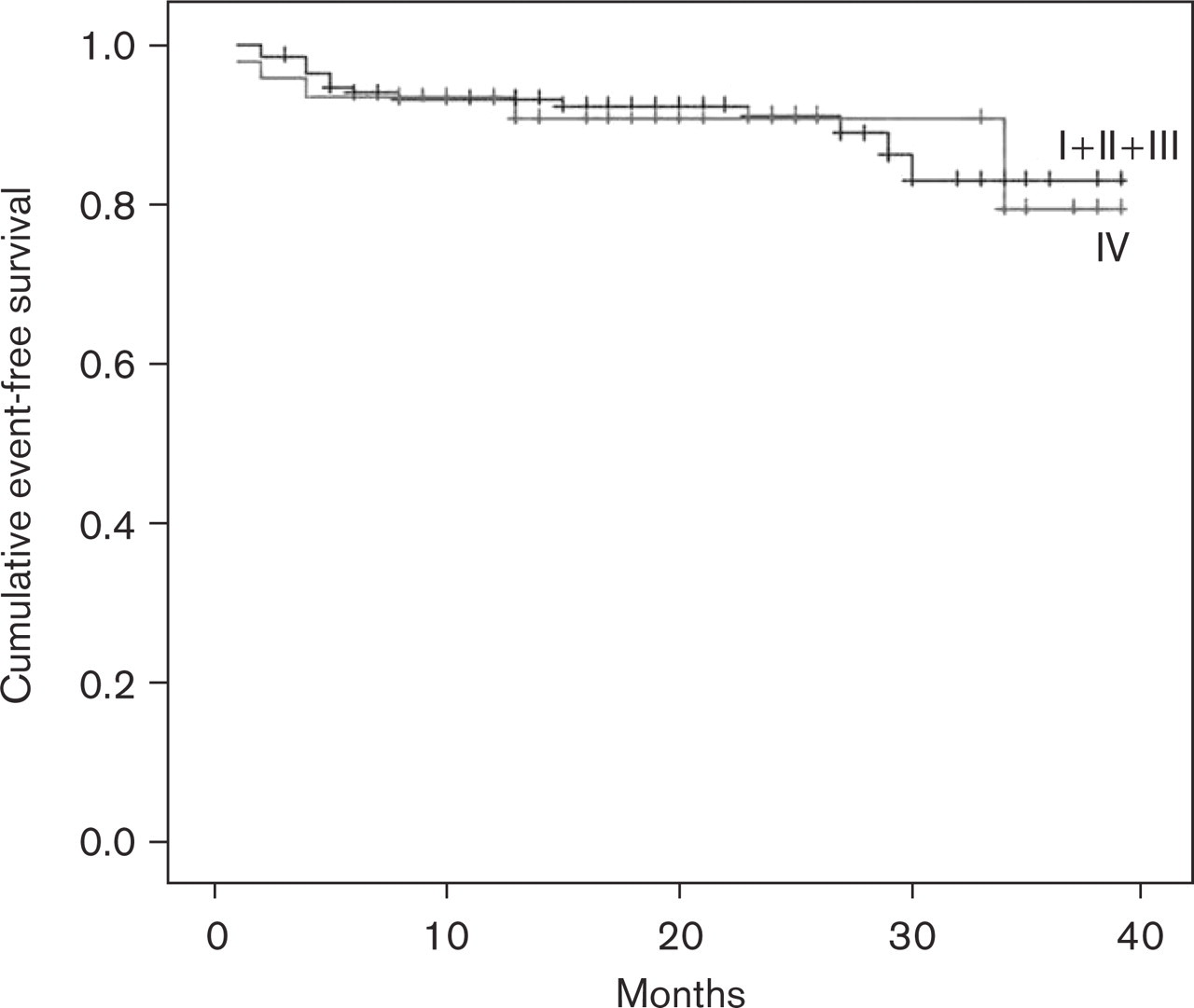
Event-free survival curves of patients in the highest quartile (IV, >6.64 mg/dl, n = 45) compared with those in the other three quartiles combined (I + II + III, n = 131).
CRP levels were similar in patients with or without events [4.2 (1.74-7.87) mg/dl vs. 4.27 (2.7-6.6) on admission and 1.55 (0.76-3.84) vs. 1.56 (0.84-2.17) at discharge]. Patients in the highest quartile (> 6.64 mg/dl, n = 45) and those in the other three groups combined (n = 131) did not differ with respect to event rate (11.1 vs. 10.7%, NS) (Fig. 2).
Discussion
Prognostic value of C-reactive protein
CRP, named for its capacity to precipitate the somatic C-polysaccharide of Streptococcus pneumoniae, is an acute phase reactant that has long been considered a classic marker for inflammation [1]. Consistent results from earlier studies have demonstrated a strong and independent association between CRP concentrations and cardiovascular end points, including acute coronary syndrome, stroke, and progression of peripheral arterial occlusive disease both in healthy participants [3, 29] and in secondary prevention [2, 8]. Increased CRP levels were also shown to predict recurrent instability in patients admitted with an acute coronary syndrome [9, 10], or undergoing invasive procedures [11, 12], such as percutaneous transluminal coronary angioplasty, stenting, or bypass grafting [23], and in other high-risk groups [30–32].
In general surgical procedures [14, 15], CRP concentrations are best related to the presence of early surgical complications, especially infective [16], and have also been used for monitoring the response to therapy and predicting the outcome of disease [17, 18]. CRP, however, may also reflect a nonspecific inflammatory response to the operative procedure due to perioperative tissue damage, independent of infection, and to this aim it has been used to quantify surgical trauma experienced by individual patients [14–16]. Thus, infection may be a confounding factor in understanding the significance and prognostic value of CRP after surgery.
C-reactive protein in cardiac surgery
Owing to the extensive body of evidence on the role of CRP in patients with atherosclerotic diseases and/or undergoing surgical procedures, CRP has been evaluated in patients undergoing cardiac surgery [19, 20], a particular scenario where the systemic inflammatory response represents an extremely complex process. For instance, ischemia-reperfusion injury, endotoxemia, contact of the blood components with the artificial surface of the bypass circuit and surgical trauma per se exert synergistic effects in this process, which make a comprehensive interpretation of the clinical significance of this biomarker difficult in this specific clinical setting [32, 33]. Thus, although an increase in proinflammatory cytokines such as CRP has been associated with an unfavorable outcome after cardiac surgery [21–24], the results available in the literature are still controversial [25–27]. This may be ascribed to different factors: study population (different type of surgery), timing of CRP samples (mostly unique preoperative measurements that do not reflect the inflammatory process throughout the time course), laboratory methods, cutoff values, and different outcomes. As a consequence, high preoperative CRP levels have inconsistently been related to mortality, postoperative complications, low cardiac output syndrome, and early graft occlusion. Thus, the significance and prognostic value of postoperative CRP after cardiac surgery remain to be elucidated. In addition, the main confounding effect on the clinical and prognostic significance of CRP after cardiac surgery is related to the high incidence of infective complications in this clinical setting, which may explain the activation and the subsequent release of CRP [17, 18, 24]. In this respect, we believe that cardiac surgery patients may be categorized according to the presence or absence of signs or symptoms of infection. While an increase in CRP levels in patients with (sub)clinical infection represents a surrogate marker, the ‘lone’ increase in CRP observed in absence of infection may stand for a biomarker of a nonspecific systemic inflammatory response to surgery-related stress [32, 33], which portraits a benign long-term prognosis.
Findings of the present study
In this study, we aimed at assessing the intrinsic significance of a ‘lone’ increase in CRP after cardiac surgery. To this goal, the study was designed to avoid the potential confounding effect of specific infections on CRP release: patients with clinical findings and/or biochemical markers of infection were not selected, patients with CABG in the setting of an acute coronary syndrome were excluded, CRP samples were obtained on admission and at discharge, and follow-up was available for prognostic verification.
Our data demonstrate that a ‘lone’ increase in CRP levels is a consistent finding after cardiac surgery, with a significant decrease at discharge, albeit elevated values are still present in the vast majority of patients, independent of clinical or surgical variables. These findings suggest that, despite improvements in surgical techniques and the biocompatibility of the extracorporeal circuits, the surgical procedure per se induces a systemic inflammatory response. At follow-up, the event rate was low and independent of CRP values. Even in patients with a CRP increase from admission to discharge (a finding that might herald future cardiac infections), long-term prognosis is good. In this respect, only one patient developed infective endocarditis on a prosthetic aortic valve after 17 months, which required re-do surgery. In this patient, CRP levels were 4 mg/dl on admission and 0.83 mg/dl at discharge.
Study limitations
Measurements of preoperative CRP levels were not available. This makes the comparison with most of the earlier studies difficult. Although CRP is the most common biomarker of inflammation for clinical purposes, additional markers have been proposed that might improve diagnostic accuracy. Nonetheless, laboratory tests for CRP have the advantage of being easily available and less costly than cytokine tests. We did not sample systematically serum concentration of Troponin I, which made unfeasible to correlate the values of postoperative myocardial damage markers with CRP.
Practical considerations and conclusion
An increase in CRP levels is a very frequent finding in cardiac surgery patients even in the absence of signs or symptoms of infection. The in-hospital course indicates a significant decrease in CRP levels at discharge. What are, then, the practical implications of this finding? We believe that a CRP increase after cardiac surgery is a nonspecific inflammatory biomarker, leading to a favorable prognosis provided that patients do not present with a clinical or biochemical profile suggestive of infection. Thus, in this population, additional diagnostic work-up as well as a longer hospitalization are usually redundant, resulting in a significant cost reduction.
Footnotes
Acknowledgements
The authors thank Mrs Paola Luciolli for her help and support to reviewing the English manuscript.