
Abstract
Objective:
The objectives of this retrospective study were to characterize the clinical presentation, diagnostic findings, surgical approaches, intra-operative challenges and complications following the surgical treatment of cardiac myxoma in two of the largest referral hospitals in Jordan.
Methods:
Medical records of all patients presented to the cardiology department during the period between 1984 and 2016 were reviewed. Criteria for inclusion in the study were: (1) patients who were presented for cardiac evaluation due to symptoms suggestive of a primary cardiac problem, (2) completed medical records, including results of echocardiography suggestive of intra-cardiac occupying mass, (3) the surgical operation was undertaken and intra-operative data was available, (4) a histological diagnosis of myxoma was available and (5) the discharge status and follow-up data were available for at least 2 years after initial surgery.
Results:
A total of 27 patients fulfilled the criteria for inclusion in the study. The average age was 42 years. Thirteen of the patients were females and 14 patients were males. The most common clinical presentations were dyspnea (29.6%) and murmurs (22.2%). Non-specific signs, such as weight loss, fever, fatigue, arthralgia and anemia, were reported in 10 (37%) patients. Signs related to systemic embolization were reported in 9 (33.3%) of the patients, involving the upper and lower extremities (55.6%), brain ischemia and vision loss (54.4%). Tumors in all patients were successfully resected under cardiopulmonary bypass support. The tumor was pedunculated in 17 (62.9%) of the patients and the size of the tumors varied from 1 to 7 centimeters in diameter. The tumor was located in the left atrium in 21 patients (77.7%), in the right atrium in 4 patients (14.8%), in the right ventricular side of the septum in 1 patient (3.7%) and involving the tricuspid valve in 1 patient (3.7%). The left atrial approach was used in 3 patients, a right atrial approach in 4 patients and a bi-atrial approach in 20 patients. The most common concomitant cardiac pathology was coronary artery disease in 3 patients and an atrial septal defect in one patient. The most common intra-operative challenges were inter-atrial communication (2 patients), large defect in the tricuspid valve leaflet (1 patient) and involvement of the inter-ventricular septum (1 patient). In the post-operative period, 1 patient suffered a stroke. In the post-operative period, the most common complications were stroke (1 patient) and recurrence of the tumor (2 patients).
Conclusion:
The success rate after surgical removal of cardiac myxoma in this study was substantial and complications were rare.
Keywords
Introduction
In general, cardiac tumors are considered rare medical entities. Myxoma represents the most common primary cardiac tumor. Cardiac myxoma has been defined by the World Health Organization as a neoplasm composed of stellate to plump, cytologically bland mesenchymal cells set in a myxoid stroma. 1 Primary cardiac myxomas have been reported as the second most common primary cardiac tumors in children. 2 Cardiac myxoma more commonly affects the atria than the ventricles.3,4
The exact aetiology of the tumor has yet to be fully determined. However, heritability has been considered as a contributing risk factor in sporadic myxoma cases, especially in young patients. 3 Embryologically, the tumor is believed to originate from entrapped undifferentiated embryonic foregut. 5 Myxomas also could be part of the Carney complex, which is an autosomal dominant syndrome including several other clinical manifestations, such as abnormal skin pigmentation, endocrinopathy and endocrine and non-endocrine tumors.3-6 Microscopically, the tumor appears to be of low cellularity, scattered in a mucopolysaccaride matrix. The size of the tumor varies between 1 to 5 cm and is typically gelatinous in consistency. The tumor is frequently characterized as pedunculated, with a smooth, villous or friable surface. 6
The clinical manifestations of the tumor vary and are probably related to the size and location of the tumor. Most of the small myxomas are asymptomatic and are only diagnosed during autopsy or found incidentally during echocardiography for other reasons. However, larger tumors are reported to be associated with more pronounced cardiovascular symptoms, such as dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea, pulmonary oedema, cough, hemoptysis, oedema due to heart failure and fatigue. 7 Other non-specific signs, such as fever and weight loss, are reported in one third of cases. 7 Laboratory examination may reveal anaemia and elevation in erythrocyte sedimentation rate, C-reactive protein or globulin levels. 8
The clinical presentation and outcome following surgical treatment of myxoma in Jordan has not been characterized. Therefore, the main aims of this study reported here were to characterize the clinical presentation, diagnostic findings, surgical techniques used to remove the tumor, intra-operative challenges and complications following surgical treatment of cardiac myxoma in two of the largest referral hospitals in Jordan.
Materials and Methods
During the period between 1984 and 2016, 27 patients retrospectively fulfilled the following criteria and were included in the study: (1) presented for cardiac evaluation due to symptoms suggestive of primary cardiac problem, (2) complete medical records, including results of echocardiography suggestive of intra-cardiac occupying mass, (3) surgical operation was undertaken and intra-operative data available, (4) a histological diagnosis of myxoma was obtained and (5) discharge status and follow-up data available for at least 2 years after initial surgery. Patients with missing information or incomplete records were excluded from the study. The study was approved by the Institutional Research Board.
The clinical history, clinical symptoms, echocardiographic results and type of surgical intervention, intra-operative findings and complications were obtained from the medical records by the principle investigator (PI).
Results
Clinical presentation
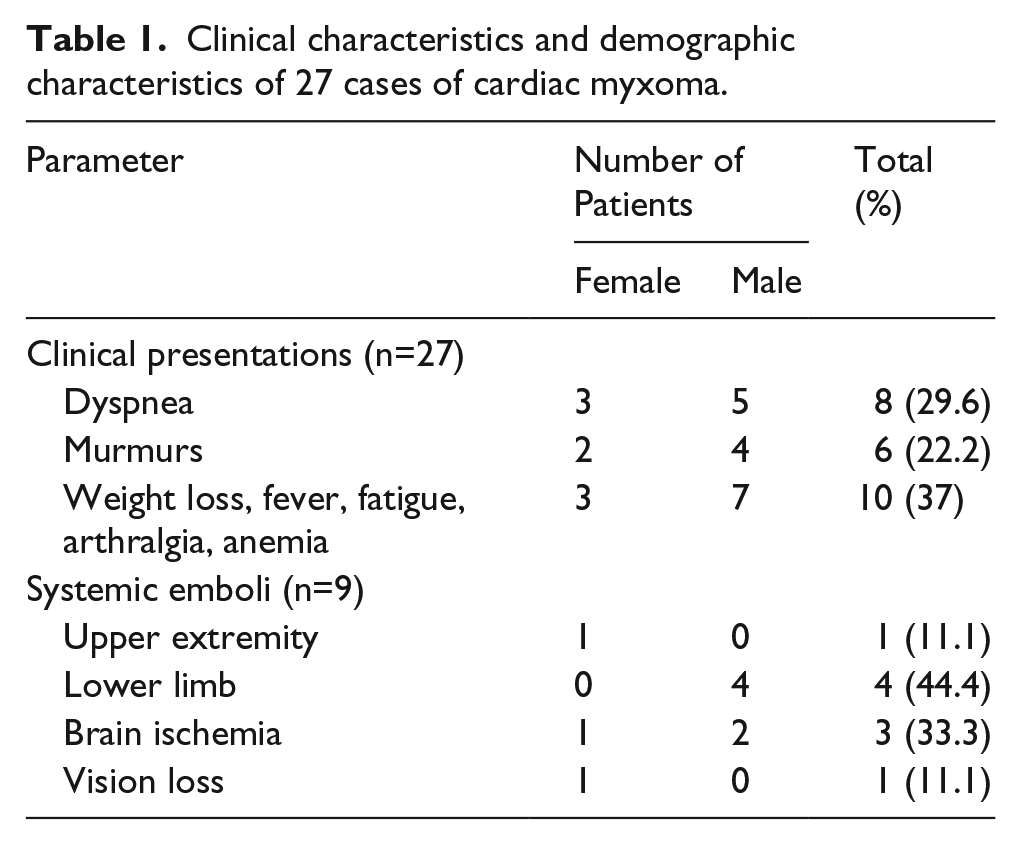
A total of 27 patients were included in the study. The most common clinical and demographic characteristics of the affected patients with cardiac myxoma in this study are presented in Table 1. The average age of the patients was 42 years (range 15-60). The patients consisted of 14 males and 13 females. The most common clinical presentations were dyspnea (29.6%) and murmurs (22.2%). Non-specific signs, such as weight loss, fever, fatigue, arthralgia and anemia, were reported in 10 (37%) patients. Signs related to systemic embolization were reported in 9 (33.3%) of the patients, involving the upper and lower extremities (55.6%), brain ischemia and vision loss (54.4%).
Clinical characteristics and demographic characteristics of 27 cases of cardiac myxoma.
Echocardiography
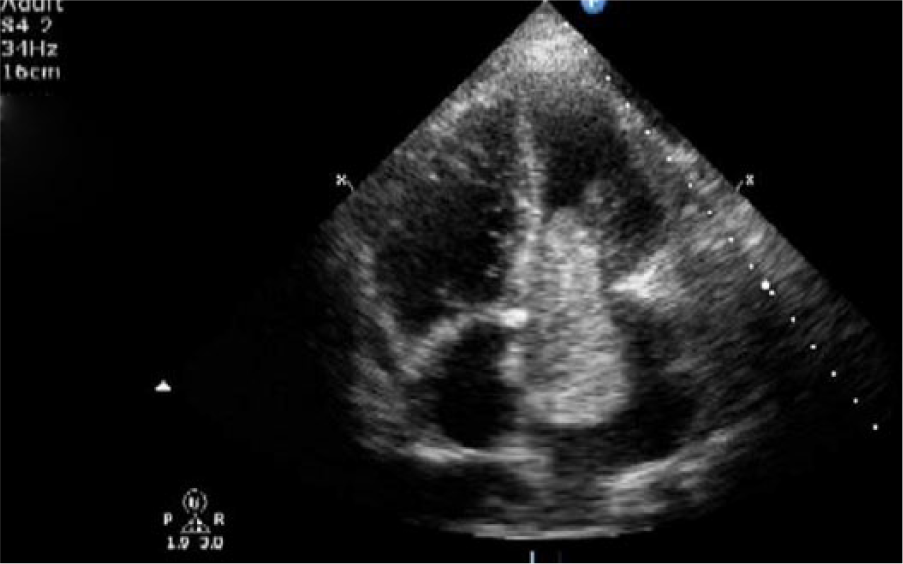
Transthoracic echocardiography was used in the diagnosis of cardiac myxoma in all cases (Figure 1). In addition, trans-esophageal echocardiography was used peri-operatively to determine the exact location of the tumor, its size and invasiveness (Figure 2).

Transthoracic echocardiographic image of a cardiac myxoma. Representative image of appearance of all patients.
Trans-esophageal echocardiogram for a patient with myxoma prolapsed through the mitral valve.
Operative treatment
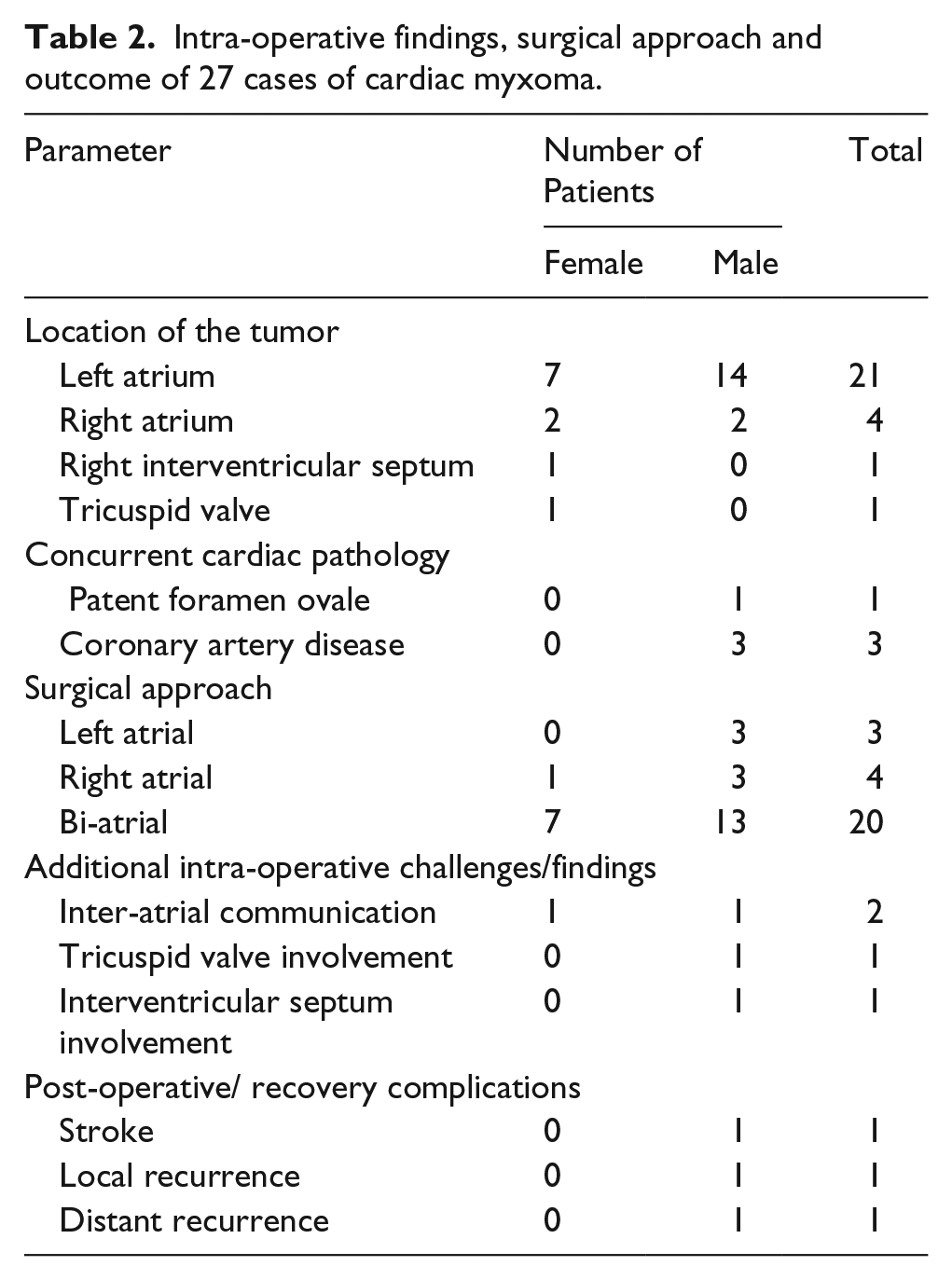
Tumors were successfully resected in all patients, under cardiopulmonary bypass. The different intra-operative findings, surgical approaches and outcomes associated with cardiac myxoma in this study are presented in Table 2. The tumor was pedunculated in 17 (62.9%) of the patients, with the size of the tumors varying from 1 to 7 centimeters in diameter (Figure 3). The tumor was located in the left atrium in 21 patients (77.7%), in the right atrium in 4 patients (14.8%), in the right ventricular side of the septum in 1 patient (3.7%) and involving the tricuspid valve in 1 patient (3.7%). The left atrial approach was used in 3 patients, right atrial approach in 4 patients and bi-atrial approach was used in 20 patients.
Intra-operative findings, surgical approach and outcome of 27 cases of cardiac myxoma.

A photograph of a cardiac myxoma.
Intra-operative challenges
In this study, intra-operative challenges were encountered and included inter-atrial communication in two patients due to the removal of a wide-base tumor, which involved a large area of the septum, which was repaired successfully using an autologous pericardial patch. The second challenge was resecting parts of a tricuspid valve leaflet which was then replaced using a prosthetic device and, finally, the involvement of the inter-ventricular septum which was repaired using an autologous pericardial patch.
The most common concomitant pathology was coronary artery disease in three patients and an atrial septal defect in one patient. Coronary artery bypass grafts were necessary for concurrent coronary artery disease and the atrial septal defect was repaired surgically using an autologous pericardial patch.
Post-operative care and complications
In the post-operative period, the mean post-operative intensive care stay was 2±0.5 days. Mean post-operative ventilation was 6±1.5 hours. One patient suffered a complete stroke in the region of the right middle cerebral artery immediately after surgery.
All patients remained on oral aspirin at 100 mg once per day and diuretics (furosemide at 20 mg orally twice per day) for six months.
Follow-up
Follow up evaluation using transthoracic echocardiography confirmed recurrence of the tumor in two patients during the first two years of follow-up. In the first patient, the tumor had a wide base involving the interatrial septum. The tumor was successfully resected again and an autologous pericardial patch was used in this patient. In the second patient, several inter-ventricular septal small nodules were noted on follow-up echocardiography after two years of the initial surgery. No surgery was planned for this patient, but follow-up examinations were recommended.
Discussion
Cardiac myxoma is a rare tumor, with a reported incidence rate of around 0.5 per million people. 8 In this retrospective study, we have characterized the clinical manifestations, surgical intervention, intra-operative surgical challenges and outcome in 27 cases confirmed to have cardiac myxoma. Primary cardiac myxomas are reportedly more common in older patients while familial myxomas are more common in pediatric patients. 9 No genetic or familial relationships were investigated in any of the cases in this study. Furthermore, myxomas in this study occurred almost at a similar frequency between males and females although, in the literature, it has been reported more frequently in females.8-12
Generally, cardiac myxomas are presented with non-specific clinical signs, making the diagnosis difficult unless other cardiac problems exist. However, larger myxomas, particularly those affecting the left atrium, are more likely to cause symptoms due to mechanical obstruction and systemic tumor embolization. 13 Similarly, in this study, clinical symptoms associated with systemic embolization accounted for about 33% of all clinical symptoms. High rates of embolization (30-40%) were reported in other studies worldwide. 14
Two-dimensional echocardiography is used most commonly for accurate diagnosis of the tumor.9-14 Transthoracic echocardiography is used to determine the location, size, shape, invasiveness and mobility of the tumor pre-operatively.9-14 In cases where coronary artery disease is suspected or the patient’s age is greater than 40 years, coronary arteriography must be performed to evaluate the coronary arteries.9-14 In this study, all cases were successfully diagnosed using transthoracic echocardiography.
The ideal surgical approach to achieve complete excision of an intracardiac myxoma is still controversial. It is believed that a surgical approach to atrial myxomas should allow minimal manipulation of the tumor, provide adequate exposure for complete resection of the tumor, allow inspection of the four heart chambers, minimize recurrence and be safe and efficacious. 15 Some surgeons recommend the use of a biatrial approach to myxoma while others consider the left atriotomy approach to be adequate, with reported low recurrence rates with this technique. 16 Furthermore, the trans-septal approach through a right atriotomy was suggested to provide good access to the myxoma with minimum handling and allows inspection of all the cardiac chambers. 16 In most cases, right atrium and right ventricle myxomas are approached through the right atrium. In any approach chosen, however, wide margins must be excised to minimize the risk of recurrence.
Recurrence of the tumor locally or at a distant site may occur due to inadequate resection or tumor embolization. 17 However, familial myxomas have an increased risk of recurrence. 18 In this study, the most common complications associated with myxomas were recurrence in two patients and stroke in one patient. Complications related to cardiac myxoma, such as congestive heart failure, sudden death, cardiac arrhythmias, infection and embolization, have been commonly reported. 18
In conclusion, this is considered the first clinical study to report myxoma in the population of Jordan. The clinical approach to diagnosis and treatment, in addition to intra-operative challenges and outcome following surgical treatment, were characterized. The study showed that the success rate after surgical removal of cardiac myxoma is substantially good, with rare complications.
Footnotes
Authors’ contributions
Mahmoud Abu Abeeleh, Moaath Alsmady, Amjad Bani Hani: Review of the cases, collection of the data and literature review; writing the manuscript.
Suhayl Saleh, Emad Alhaddad: Diagnostic echocardiography and interpretation of results
Musa Alshehabat, Zuhair Bani Ismail: Editorial assistance
Islam Massad, Sami Abu Halaweh: Clinical anaesthesiologists on the cases
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.