
Abstract
Background
A sedentary lifestyle and psychosocial factors such as hopelessness and depression increase cardiovascular risk. Cross-sectional evidence suggests positive effects of physical exercise on psychological well being, but the time order of the relationship between physical activity and hopelessness has not been addressed.
Design
Population-based prospective cohort study with 630 middle-aged men participating in the 4-year follow-up and 509 men in the 11-year follow-up.
Methods
We investigated the association of leisure-time physical activity (LTPA) with the development of hopelessness during the follow-up. LTPA and hopelessness were quantified with questionnaires.
Results
In cross-sectional analyses, LTPA was inversely associated with hopelessness, independently of depression. Among men who did not have feelings of hopelessness at baseline, those who reported engaging in at least 2.5 h/week of moderate-to-vigorous physical activity had a lower risk (odds ratio 0.65, 95% confidence interval: 0.39–1.09, P for the trend = 0.047) to feel hopeless than sedentary men 4 years later after adjustment for age, smoking, alcohol consumption, cardiovascular disease and socioeconomic status. Furthermore, this relationship was not explained by body mass index or maximal oxygen uptake. Adjustment for depressive symptoms slightly weakened the association (odds ratio 0.66, 95% confidence interval: 0.39–1.11, P for the trend = 0.060). After 11 years, men who reported being physically active at baseline were still less likely to feel hopeless, after adjusting for age. However, after further adjustment for other confounding factors the association was no longer significant.
Conclusion
Moderate-to-vigorous physical activity seems to prevent development of hopelessness in middle-aged men. This protective effect may diminish over time.
Introduction
A physically active lifestyle contributes to mental health [1]. The evidence comes mainly from cross-sectional studies focusing on exercise and depression [2].
Prospective studies are scarce. Although a few large cohort studies suggest that physical activity protects against depressive symptoms [3–7], others do not [8–10]. In earlier studies psychological outcome has ranged from clinical depression to depressive symptoms and mood. It is plausible that physical exercise has a stronger impact on certain depressive or mental symptoms than on other symptoms.
Hopelessness is a cluster of negative expectancies concerning a person and his or her future. Hope is an important determinant of subjective well being [11]. Lack of hope is associated with various manifestations of psychological morbidity [12]. Although hopelessness is a major symptom of depression, it is nonetheless a distinct entity. The prevalence of hopelessness was 11.4% in a general population in Finland [13]. After excluding those with any self-reported mental disorder diagnosed or treated by a physician during the preceding year the prevalence of hopelessness was still as high as 7.8% [13]. Thus, although feelings of hopelessness and futility are common features of depression, hopelessness often exists in the absence of depression. Hopelessness, independent of depression, is associated with the metabolic syndrome, the incidence of hypertension and myocardial infarction, accelerated progression of carotid atherosclerosis and cardiovascular and overall mortality [14–19].
We showed earlier that low level of leisure-time physical activity (LTPA) was associated with hopelessness in a cross-sectional study [20]. Our findings raise the possibility that physical activity may also protect against feelings of hopelessness in the future. Therefore, we investigated the association of LTPA with the risk of developing hopelessness in middle-aged men during 11 years of follow-up in a population-based study.
Methods
Participants
The Kuopio Ischemic Heart Disease Risk Factor Study is a prospective population-based cohort study in middle-aged men in eastern Finland. Baseline data were collected between 1984 and 1989 from 2682 male participants aged 42–60 years. The Research Ethics Committee of the University of Kuopio approved the study. All study participants gave written informed consent.
The individuals were invited to participate in a follow-up study 4 and 11 years later. There were 630 men at the 4-year follow-up and 509 men at the 11-year follow-up who had complete data on LTPA and depressive symptoms. To study new-onset hopelessness, men in the highest tertile of hopelessness at baseline were excluded from the prospective analyses.
Assessment of leisure-time physical activity
The validated Kuopio Ischemic Heart Disease Risk Factor Study 12-month LTPA Questionnaire was used as described earlier [21, 22]. Low-intensity LTPA was defined as less than 4.5 metabolic equivalents (METs). At least moderate LTPA (≥ 4.5 METs) included brisk walking, skiing, jogging, bicycling, ball games and forestry. Vigorous LTPA was defined as ≥ 7.5 METs. The durations of LTPA were calculated in minutes/week.
Assessment of cardiorespiratory fitness
A graded symptom-limited exercise test was performed on a cycle ergometer. Maximal oxygen uptake (VO2max) was measured directly with respiratory gas analysis as described earlier [21].
Assessment of hopelessness and depressive symptoms
Hopelessness was assessed by two items included in psychological questionnaires administered both at baseline and at the 4-year and 11-year follow-ups [17]. The items measuring hopelessness were ‘the future seems to be hopeless, and I cannot believe that things are changing for the better’ and ‘I feel that it is impossible to reach the goal I would like to strive for’. Participants responded using a five-point scale (0 = absolutely agree, 1 = somewhat agree, 2 = cannot say, 3 = somewhat disagree, or 4 = absolutely disagree). Hopelessness score, with a range of 0–8, was created by reverse coding and summing the items.
The Human Population Laboratory Depression Scale was used to assess depressive symptoms, as described in detail previously [13]. The Human Population Laboratory Depression Scale is highly correlated with the Beck Depression Inventory (r = 0.66) [23].
Other assessments
Biochemical measures, body mass index (BMI), waist circumference and blood pressure were measured as described earlier [14]. Medical history, adult socio-economic status, smoking and alcohol consumption were assessed by self-administered standardized questionnaires [14, 24].
Statistical analysis
At baseline, men with a hopelessness score in the highest tertile, that is, those with ≥ 4 points were excluded from the prospective analyses. Men who scored ≥ 4 points after follow-up were defined as having developed hopelessness. Differences in characteristics at baseline between men who developed hopelessness during the 11-year follow-up and those who did not were assessed with Student's t-test for continuous variables and the χ2 test for categorical variables. The association between LTPA and risk of developing hopelessness at the 4-year and 11-year follow-ups was estimated using logistic regression analysis adjusting for covariates. Variables with skewed distributions are presented as medians (inter-quartile ranges) and analyzed using log-transformed values. Other data are presented as means ± standard deviations or simple percentages. Statistical significance was considered to be P value less than 0.05. All statistical analyses were performed with SPSS 14.0 for Windows (Chicago, Illinois, USA).
Results
Baseline characteristics
Table 1 presents the characteristics of the study population. Men who developed hopelessness at the follow-up had lower socioeconomic status and were more often smokers at baseline than the less hopeless men. There were no significant differences in baseline characteristics between the hopelessness groups at baseline. Men who were hopeless after follow-up were more physically active, but the difference was not statistically significant.
Leisure-time physical activity and hopelessness
We showed earlier that total, vigorous and moderate-to-vigorous LTPA was strongly associated with feelings of hopelessness at baseline [20] Similarly, cross-sectional analyses at 4 years and 11 years of follow-up showed that LTPA and hopelessness were connected (e.g. 4-year follow-up, model 2, total LTPA: odds ratio (OR): 0.65, 95% confidence interval (CI): 0.45–0.94, P = 0.015; vigorous LTPA: OR: 0.70, 95% CI: 0.48–1.02, P = 0.037; moderate-to-vigorous LTPA: OR: 0.67, 95% CI: 0.47–0.95, P = 0.008; 11-year follow-up, model 2, total LTPA: OR: 0.76, 95% CI: 0.50–1.17, P = 0.188; vigorous LTPA: OR: 0.66, 95% CI: 0.43–1.01, P = 0.042; moderate-to-vigorous LTPA: OR: 0.52, 95% CI: 0.33–0.80, P = 0.003). Low-intensity LTPA was not associated with hopelessness at any of the time points.
Baseline characteristics of the 509 middle-aged men according to categories of hopelessness at 11-year follow-up
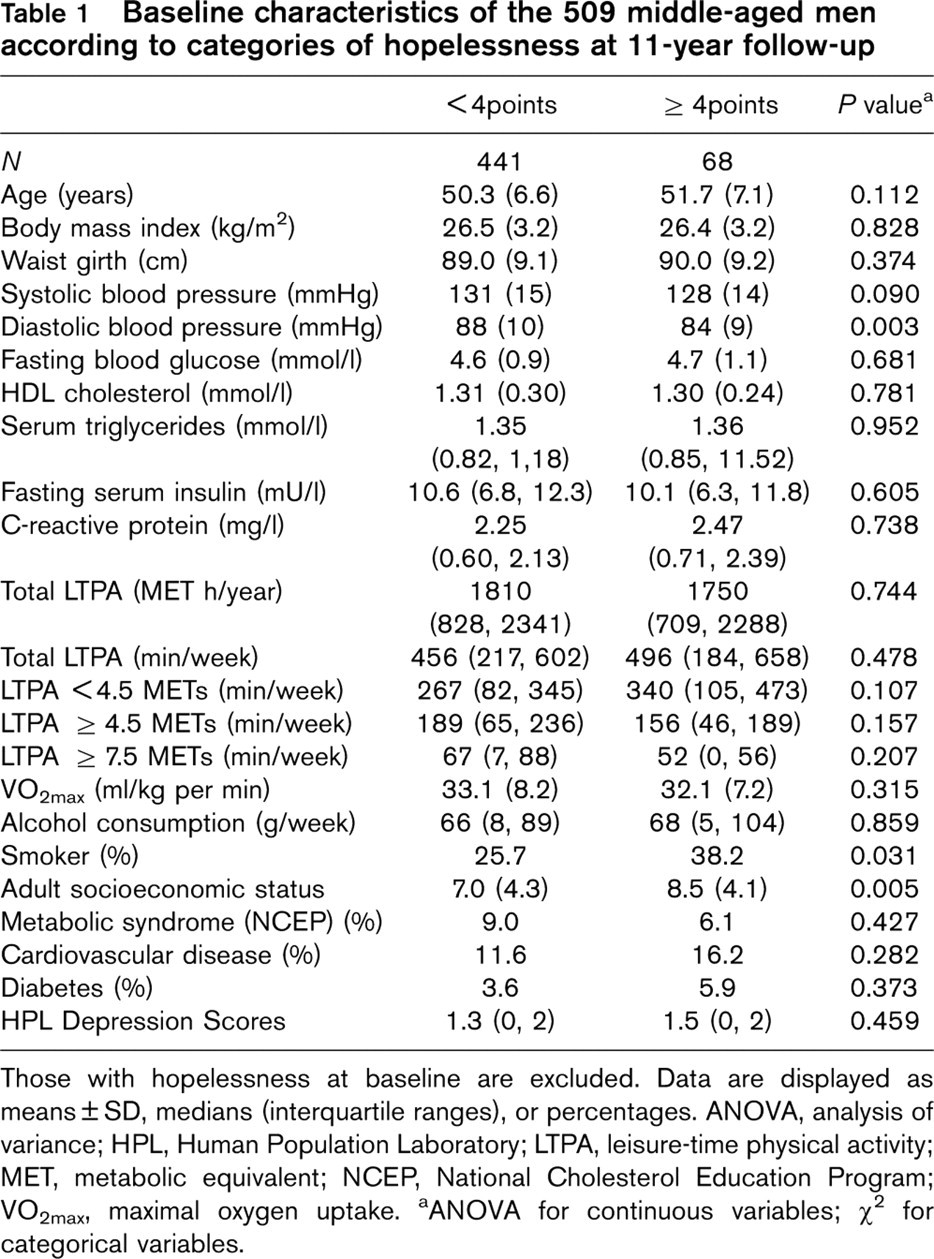
Those with hopelessness at baseline are excluded. Data are displayed as means ± SD, medians (interquartile ranges), or percentages. ANOVA, analysis of variance; HPL, Human Population Laboratory; LTPA, leisure-time physical activity; MET, metabolic equivalent; NCEP, National Cholesterol Education Program; VO2max, maximal oxygen uptake.
aANOVA for continuous variables; χ2 for categorical variables.
Leisure-time physical activity and the risk of developing hopelessness during 4-year follow-up
Men who reported at least 2.5 h of moderate-to-vigorous LTPA per week were almost half as likely (Model 1, OR: 0.58, 95% CI: 0.35–0.96, P for trend = 0.023) to feel hopeless 4 years later than sedentary men adjusting for age (Table 2). The association weakened slightly after further adjustment for smoking, alcohol consumption, cardiovascular disease and adulthood socioeconomic status (Model 2) as well as after additional adjustment for depressive symptoms (model 4). Further adjustment for VO2max and BMI had no effect on the association.
Total LTPA, vigorous LTPA, and low-intensity LTPA did not predict hopelessness at the 4-year follow-up (Table 2). Furthermore, VO2max was not associated with the development of hopelessness during the 4-year follow-up.
Leisure-time physical activity and the risk of developing hopelessness during the 11-year follow-up
An age-adjusted logistic regression model showed that moderate-to-vigorous LTPA at baseline protected from feelings of hopelessness 11 years later (Table 3: Model 1, OR: 0.53, 95% CI: 0.29–0.99, P = 0.049). After controlling for confounding variables (Model 2) the trend remained similar (OR: 0.59, 95% CI: 0.32–1.12), but the association was no longer significant (P = 0.108). Vigorous LTPA was similarly associated with hopelessness, but total LTPA and low-intensity LTPA did not predict hopelessness at the 11-year follow-up. VO2max also was not associated with the development of feelings of hopelessness at the 11-year follow-up.
Furthermore, in the association with emergence of hopelessness there was no interaction between moderate-to-vigorous LTPA and diabetes (P = 0.21), cardiovascular disease (P = 0.12) or the metabolic syndrome (P = 0.29 for the interaction). There was also no interaction between high-intensity LTPA and these variables for the association with development of hopelessness.
Hopelessness and the risk of becoming sedentary during follow-up
Men who were hopeless at baseline were not at risk for becoming sedentary during the 4-year follow-up (for ≥ 2.5 h/week vs. < 1 h/week, moderate-to-vigorous LTPA, Model 1: OR: 0.70, 95% CI: 0.42–1.15, P for trend 0.15, Model 2: OR: 0.89, 95% CI: 0.52–1.51, P = 0.58) or during the 11-year follow-up (Model 1: OR: 0.57, 95% CI: 0.29–1.11, P for the trend 0.14, Model 2: OR: 0.79, 95% CI: 0.39–1.61, P = 0.64). Those men already exercising less than an hour per week of moderate-to-vigorous physical activity at baseline (n = 951, 36%) were excluded from this analysis. Moreover, there was no association between changes in LTPA and changes in hopelessness scores during the follow-up period (data not shown).
Odds ratios (95% confidence intervals) for having feelings of hopelessness in 4-year follow-up according to categories of baseline physical activity in 630 middle-aged men
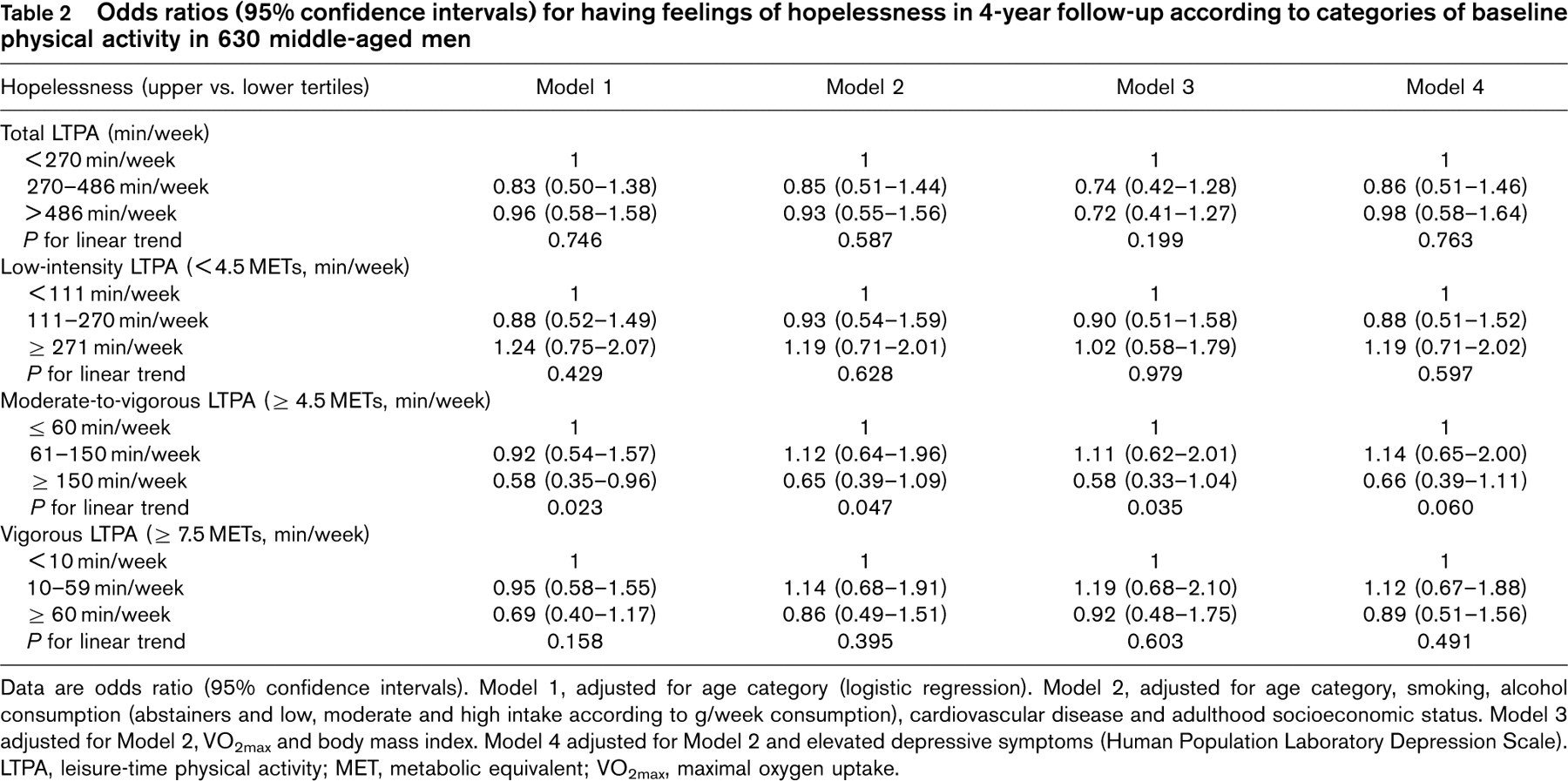
Data are odds ratio (95% confidence intervals). Model 1, adjusted for age category (logistic regression). Model 2, adjusted for age category, smoking, alcohol consumption (abstainers and low, moderate and high intake according to g/week consumption), cardiovascular disease and adulthood socioeconomic status. Model 3 adjusted for Model 2, VO2max and body mass index. Model 4 adjusted for Model 2 and elevated depressive symptoms (Human Population Laboratory Depression Scale). LTPA, leisure-time physical activity; MET, metabolic equivalent; VO2max, maximal oxygen uptake.
Odds ratios (95% confidence intervals) for having feelings of hopelessness in 11-year follow-up according to categories of baseline physical activity in 509 middle-aged men
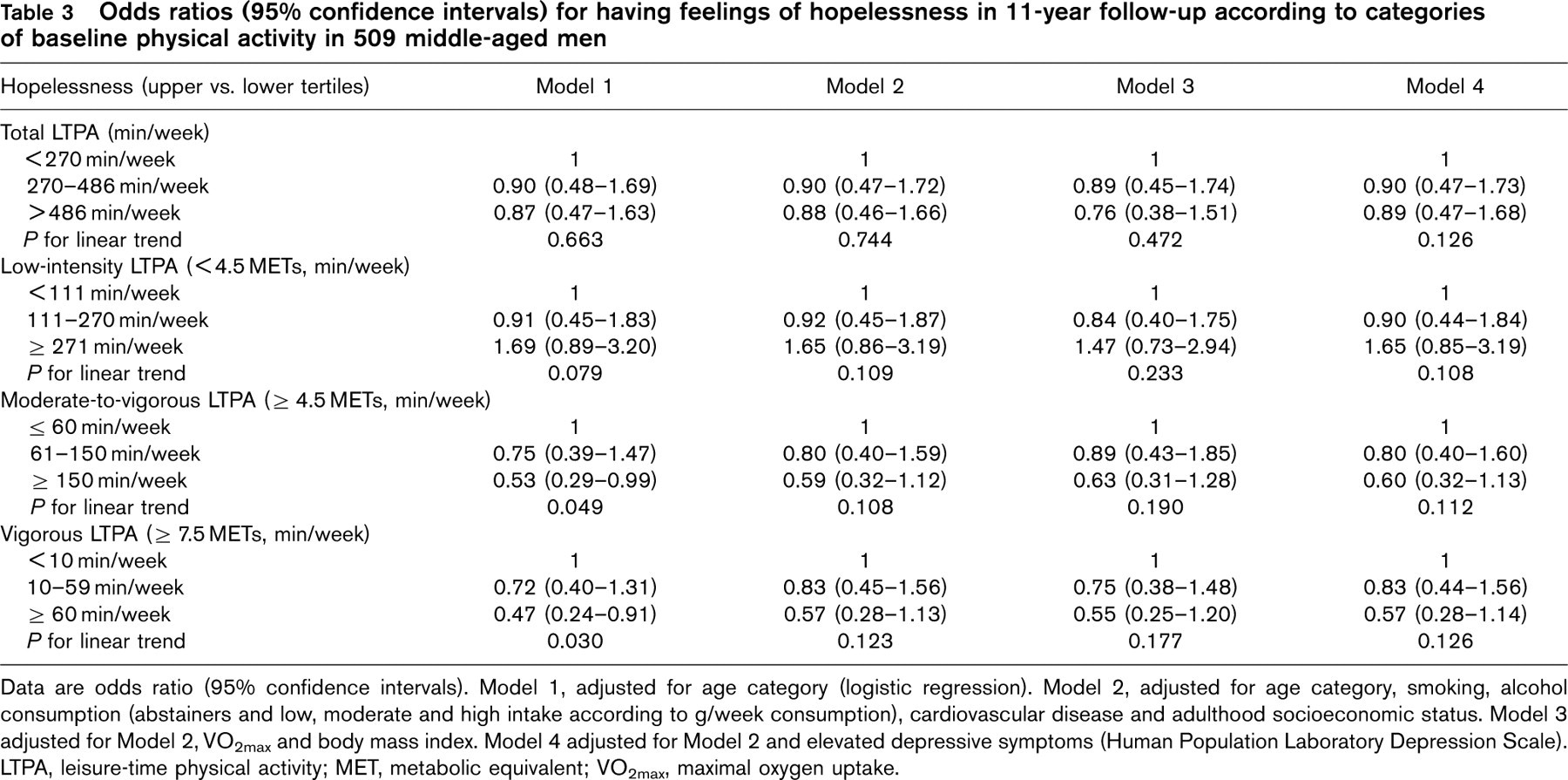
Data are odds ratio (95% confidence intervals). Model 1, adjusted for age category (logistic regression). Model 2, adjusted for age category, smoking, alcohol consumption (abstainers and low, moderate and high intake according to g/week consumption), cardiovascular disease and adulthood socioeconomic status. Model 3 adjusted for Model 2, VO2max and body mass index. Model 4 adjusted for Model 2 and elevated depressive symptoms (Human Population Laboratory Depression Scale). LTPA, leisure-time physical activity; MET, metabolic equivalent; VO2max, maximal oxygen uptake.
Leisure-time physical activity, hopelessness and depressive symptoms
Depression and hopelessness at baseline correlated moderately (r = 0.38, P < 0.001). The average depression score at baseline was higher in hopeless men than in other men, although the difference was not significant (Table 1). LTPA did not predict development of depressive symptoms (data not shown).
Discussion
This prospective population-based cohort study shows for the first time that moderate-to-vigorous LTPA is associated with a lower risk for developing hopelessness. Importantly, this association was not explained by BMI, VO2max or other confounding factors. However, depressive symptoms slightly attenuated the association at the 4-year follow-up.
After adjusting for potential confounding factors, men engaging in moderate-to-vigorous LTPA at least 2.5 h/week had 35% lower risk to feel hopeless about their future and reaching goals 4 years later than sedentary men at baseline. After 11 years the trend was still similar, indicating protective effect of LTPA. However, the association was no longer significant. Vigorous LTPA was associated with a lower risk for hopelessness at the 11-year follow-up in age-adjusted analyses, but not after further adjustment. Total and low-intensity exercise did not predict feelings of hopelessness at the 4-year or 11-year follow-up. Cardiorespiratory fitness was not associated with the development of hopelessness, suggesting that moderate-to-vigorous LTPA per se rather than fitness protects against progression of feelings of hopelessness.
Importantly, hopelessness at baseline did not predict sedentary lifestyle 4 or 11 years later. Earlier we showed the association between LTPA and hopelessness in a cross-sectional study [20]. The results of this study suggest that sedentary lifestyle predisposes to hopelessness, rather than vice versa. The protective effect of LTPA can still be seen after 4 years. However, it diminishes over time, and after 11 years the association is no longer independent of confounding factors.
In this study depression and hopelessness scores were correlated and depressive symptoms seemed to attenuate the association of LTPA with progression of hopelessness to some degree. However, depression did not explain the relationship entirely, and LTPA was not associated with depression. Although hopelessness and depression overlap, they are still considered distinct phenomena. The importance of hopelessness itself on physical and mental health has been recognized. In earlier studies, hopelessness has been found to predict various cardiovascular outcomes, independently of depression [14–19]. Psychological factors associated with hopelessness in the general population include depression, suicidal ideation and alexithymia (poor ability to recognize and verbalize emotions) [12]. Some studies suggest that hopelessness might be even a more powerful risk factor of suicidality than depression [25, 26]. Hopelessness has been seen as a trait that reflects person's attitude and increases vulnerability to react to certain environmental stimuli with depression [27]. These stimuli include unemployment, poor financial situation [28], poor general health, dissatisfaction with life [12] and stress [29], which are all associated with hopelessness in the general population.
Our findings raise the question of underlying mechanisms explaining the association between LTPA and hopelessness. Regular physical activity is suggested to have positive influences on brain health in humans, with respect to both brain structure and function [30, 31]. The mechanisms behind these adaptations are not known, but several neurogenerative, neuroadaptive and neuro-protective processes have been suggested in animal models, including increased expression of brain growth factors, stimulation of growth and development of brain cells and protection from neurotoxic damage [30]. Other possible biological pathways include activation of the hypothalamic–pituitary–adrenocortical system [32], increased neurotransmissions of central dopaminergic, noradrenergic and seratonergic systems [33], increased biosynthesis of neurotransmitters such as monoamines, catecholamines and endorphines [6]. In addition, several psychosocial factors may be involved in the positive effect of exercise on mental health. These include improved self-esteem and self-efficacy, decreased social isolation, increased self-image and self-worth [34], distraction, a sense of mastery and changes of self-concept [2]. How hopelessness relates to these mechanisms is not yet known. Nevertheless, the positive effects of exercise on brain and cognition may enhance optimism and subjective well being.
The strengths of this study include its large population-based design and long follow-up period. We also assessed in detail different psychosocial factors and potential confounding factors. Furthermore, VO2max was measured directly by a maximal symptom-limited cycle ergometer test with analysis of respiratory gas exchange, an accurate and highly reproducible measure of cardiorespiratory fitness [35]. Physical activity was not assessed using physical activity monitors, but the questionnaire used to measure LTPA is valid and repeatable [22]. Our hopelessness scale is fairly simple and it has not been compared with other hopelessness scales. However, it has been well validated and in earlier studies it has predicted various cardiovascular outcomes [14, 17–20]. The cohort of this study includes only middle-aged white men. Therefore, we caution against overgeneralization of the findings.
This study agrees with growing evidence that regular LTPA contributes to mental health. The new finding of this study is that physically active lifestyle helps people to maintain or gain more optimistic perspective on the future and oneself. This is especially timely considering the economic challenges people are facing throughout the world. Following the recommended physical activity guidelines may help to confront challenges in life and to enhance optimism and subjective well being.
Footnotes
Acknowledgements
The authors thank the staff of the Research Institute of Public Health, University of Kuopio, and Kuopio Research Institute of Exercise Medicine for data collection in the KIHD study. The KIHD study was supported by grants from the Academy of Finland (grants 118551, 41471, 1041086 and 2041022), the Ministry of Education of Finland (grants 167/722/96, 157/722/97, 156/722/98), and the National Heart, Lung and Blood Institute of the USA (grant HL44199). M.V. is supported by LIKES Research Center for Sport and Health Sciences and by grants from the Onni and Hilja Tuovinen Foundation, Orion Farmos Foundation and Yrjö Jahnsson Foundation.
Conflict of interest: none declared.