
Abstract
Aim
This research quantitatively explored the prevalence of NANDA-I nursing diagnoses related to the care of patients experiencing heart failure.
Design
A systematic review and meta-analysis were conducted with the systematic review protocol registered in PROSPERO (registration number: CRD42022382565).
Methods
Systematic searches were performed between March and April 2022, including peer review for selection, quality assessment, data extraction, and analysis of all included studies. A subsequent meta-analysis was performed, focusing on the proportion of nursing diagnoses in patients with heart failure. The logistic random effects model with maximum likelihood estimation assessed the combined proportion, and heterogeneity between studies was evaluated using the I 2 statistic. The goodness-of-fit of the meta-analysis results was assessed using the leave-one-out method and by evaluating publication bias through contour-enhanced funnel plots.
Data sources
PubMed, SCOPUS, CINAHL, WOS, and Embase were used.
Results
Of the 11 studies that met the eligibility criteria, 44 nursing diagnoses were identified as most frequently occurring in patients experiencing heart failure, and only 16 diagnoses appeared in more than one publication. The combined mean proportion was 35.73% (95% CI = [26.67%; 48.56%]), indicating the presence of heterogeneity based on the I 2 value. However, no publication bias was observed.
Conclusion
The results of the meta-analysis suggest priority diagnoses in individuals with heart failure, such as deficient knowledge (00126). Additionally, secondary diagnoses, such as activity intolerance (00092), excess fluid volume (00026), and ineffective breathing pattern (00032), were identified as responses to decreased cardiac output (00029). Less prevalent nursing diagnoses were associated with deterioration of health status and the need for hospitalization.
Objetivo
Investigar cuantitativamente la prevalencia de diagnósticos de enfermería NANDA-I asociados con la atención de pacientes con insuficiencia cardíaca.
Diseño
Revisión sistemática y metanálisis. El protocolo de revisión sistemática quedó registrado en PROSPERO) número de registro: CRD42022382565).
Métodos
Se realizaron búsquedas sistemáticas entre marzo y abril de 2022, llevándose a cabo una revisión por pares sobre la selección, evaluación de calidad, extracción de datos y análisis de todos los estudios incluidos. Se realizó un metanálisis posterior centrado en la proporción de diagnósticos de enfermería en pacientes con insuficiencia cardíaca. El modelo logístico de efectos aleatorios con estimación de máxima verosimilitud evaluó la proporción combinada y la heterogeneidad entre los estudios se evaluó mediante el estadístico I 2. La bondad de ajuste de los resultados del metanálisis se evaluó mediante el método Leave-one-out y la evaluación del sesgo de publicación mediante gráficos de embudo (funnel plot), denominado Contour-Enhanced Funnel Plot.
Fuentes de datos
PubMed, SCOPUS, CINAHL, WOS, Embase.
Resultados
En los 11 estudios que cumplieron con los criterios de elegibilidad, se identificaron 44 diagnósticos de enfermería aunque sólo 16 diagnósticos aparecieron en más de una publicación. La proporción media combinada fue del 35,73% (IC del 95%) = [26,67%; 48,56%]), y el valor de I 2 indica la presencia de heterogeneidad, aunque no hay sesgo de publicación.
Conclusión
Los resultados de este metaanálisis indican que habría diagnósticos prioritarios en personas con insuficiencia cardíaca, como Conocimientos deficientes (00126). Además, se han identificado otros diagnósticos de enfermería como diagnósticos secundarios: Intolerancia a la actividad (00092), Exceso de volumen de líquidos (00026) y Patrón respiratorio ineficaz (00032), que sería la respuesta a Disminución del gasto cardíaco (00029). Además de diagnósticos de enfermeríaa menos prevalentes relacionados con el deterioro del estado de salud y la necesidad de hospitalización.
INTRODUCTION
Heart failure (HF) is a clinical syndrome caused by a structural or functional cardiac abnormality. There are elevated intracardiac pressures or inadequate cardiac output at rest or during exercise. HF is characterized by dyspnea and inflammation of the lower extremities, and it may also be accompanied by signs, such as elevated jugular pressure, pulmonary crackles, and peripheral edema (McDonagh et al., 2021).
The prolongation of the life span of cardiac patients, a consequence of therapeutic innovations, has led to an increasing prevalence of HF. In developed countries, the prevalence of known HF is generally estimated to be 1%–2% of the general adult population. The incidence in European countries and the United States ranges widely, from 1 to 9 cases per 1000 person-years (Groenewegen et al., 2020). Patients with HF often suffer frequent decompensations, which is a common cause of hospitalization (readmission at 60–90 days in 25%–30% of cases) with high rates of morbidity (4.7% of cases) and in-hospital mortality (at 60–90 days in 7%–11% of cases) (Farmakis et al., 2015; Gonzalez & Mena, 2022; Martinez et al., 2019).
Nurses interpret and treat signs and symptoms that arise due to the pathophysiological process. Additionally, they deal with human responses to this process, aspects inherent in a human being, which are destabilized due to admission, disease progression, and treatment (dos Santos et al., 2013; Pereira et al., 2015). These responses are described through nursing diagnoses (ND). Nursing diagnosis is defined as a clinical judgment concerning a human response to health conditions/life processes, or a vulnerability to that response, by an individual, family, group, or community. A nursing diagnosis provides the basis for the selection of nurse interventions to achieve the outcomes for which nurses have responsibility, approved at the ninth NANDA conference: modified in 2009, 2013, and 2019 (Herdman & Kamitsuru, 2021–2023).
The development and validation of NDs are based on diagnostic indicators: defining characteristics (DC), risk factors, and related factors. Diagnostic indicators provide decision support to nurses through information that is used to diagnose and differentiate one diagnosis from another. These include DC, which describe the manifestations of the diagnosis in terms of signs and symptoms, and risk factors and related factors, which describe causes, and allow the nurse to target interventions. In addition, in the 2018–2020 edition of NANDA-I, two new indicators have been added to help improve the accuracy of diagnostic identification, namely, the population at risk and associated problems. NANDA-I considers the degree to which scientific evidence and existing theories support the correct interpretation of each nursing diagnosis. To do this, it classifies diagnoses into three levels of evidence and their subsequent sublevels, which depend directly on the robustness of the scientific evidence that supports them (Herdman & Kamitsuru, 2018–2020).
In addition, ND is established in clinical practice as a result of critical thinking and analysis of the data obtained from the evaluation. Diagnostic reasoning requires the interaction of interpersonal, technical, and intellectual processes by the nurse, as well as the development of tolerance to ambiguity and the use of reflective practice as personal strengths, or to put it another way, it requires precision in diagnostic judgment (Lunney, 2013; Pereira et al., 2015). Accurate diagnosis is crucial as it involves the identification of appropriate care outcomes and the planning of specific nursing interventions, resulting in fewer decompensations in patients with HF, a better quality of life, and lower readmission and mortality rates. This means fewer adverse events, better quality of care, and therefore better health outcomes (Tian et al., 2023).
In recent years, several secondary studies have been conducted to summarize the available evidence on prioritized NDs for patients with HF. Cavalcanti et al. (2014) identified 8 prevalent ND, and de Almeida Neto (2017) identified 13 ND. Overall, only NDs 00298 (decreased activity tolerance), 00029 (decreased cardiac output), and 00026 (excess fluid volume) appear in both studies. No known evidence was found that provides data on the prevalence of ND in patients with HF, nor meta-analyses. In this sense, identifying the most prevalent ND and providing meta-analysis data in patients with HF would allow for the design of more precise care plans based on scientific evidence, facilitating better health outcomes, and avoiding the occurrence of adverse events.
Aim
This research quantitatively investigates the prevalence of NANDA-I NDs associated with the care of patients experiencing HF. The overarching goal of this research is to contribute to science (generate evidence) related to the care management of patients with HF and to provide the evidence base necessary for the NANDA-I terminology to contribute to the synoptic construction of the literature and clinical decision-making. This research will add to a standardized nursing language, which is vital for the documentation of nursing care related to decreasing the morbidity and mortality associated with HF.
METHODS
This systematic review and meta-analysis were guided and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021). The systematic review protocol for this meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO).
Search strategy
Systematic searches were conducted in the following electronic databases: MEDLINE through PubMed, SCOPUS, CINAHL, Web of Science, and Embase, between March and April 2022.
The search strategy followed the criteria of each database combined using Boolean operators AND and OR and the words (“HF,” “nursing diagnosis,” “ND,” “cardiac failure,” “heart decompensation,” “myocardial failure,” and “congestive HF”).
Criteria for study selection
The following inclusion criteria were applied: Studies using the NANDA-I Nursing Diagnoses Taxonomy for diagnosis. Studies in any sample size that identified NDs in patients with HF. Studies using data on diagnoses identified in absolute numbers or frequencies. Studies whose objective is to identify possible or certain NDs in patients with HF. Studies published between 2012 and 2022 in English, Portuguese, and Spanish.
The following exclusion criteria were considered: Unique case studies and abstracts submitted to congresses. Clinical validation studies of diagnoses, expert consensus studies, and integrative reviews. Studies using overlapping populations, that is, different publications from the same series of patients. Studies in which the results are not comparable to the rest of the studies included.
Study selection and data extraction
To ensure the reliability of the study selection process, it was carried out by two members of the review team independently (IPST and MRCC). Initially, the titles and abstracts of the studies were read, selecting them for full reading according to the eligibility criteria. In case of disagreement, an evaluation was requested from a third member of the review team (AMPG). However, if the abstract reading did not provide enough information, each of the researchers proceeded to read the entire article independently. Subsequently, disagreements were resolved through joint discussions and consensus (IPST, MRCC, RAC, and AMPG). The rejected studies were classified according to the reason for exclusion.
Finally, the same members of the research team conducted an inverse search, searching potentially eligible items in the reference lists of included studies, repeating the previous process. See the PRISMA flow diagram (Page et al., 2021) (Figure 1).
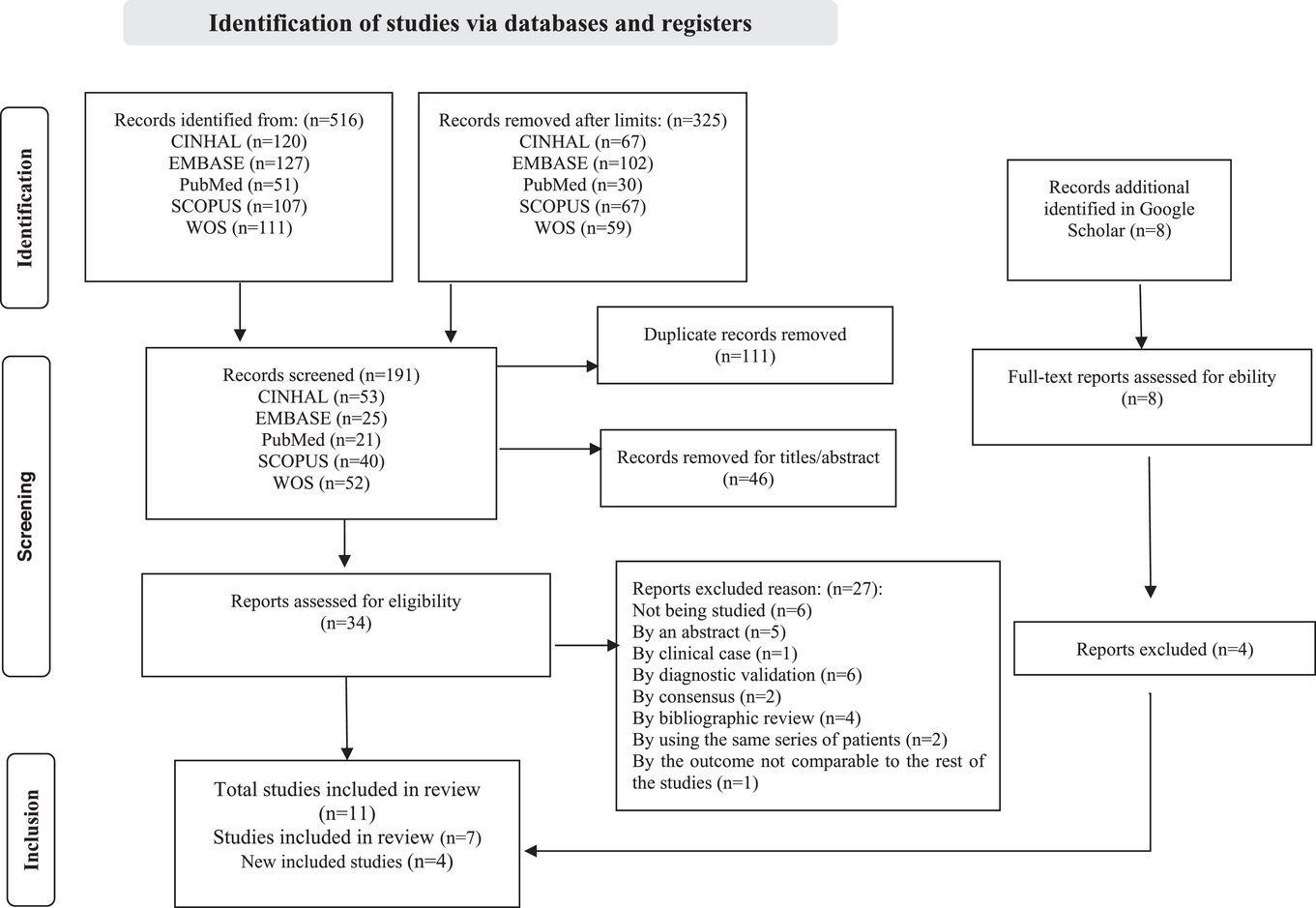
Flow diagram for study selection.
Quality assessment
For the study of methodological quality and evidence level of the studies that made up the final sample, the Johns Hopkins Nursing Evidence-Based Practice Guide was used (Dang et al., 2021).
Data analysis
Analyses were performed using R Commander (R Core Team, 2013), package metaphor (Viechtbauer, 2010), meta (Balduzzi et al., 2019), and dmetar (Harrer et al., 2019, 2021).
The selected outcome measure was the proportion (with logit transformation) of ND in patients with HF. For the estimation of the combined proportion, a logistic random-effects model with maximum likelihood estimation was used, as recommended by Stijnen et al. (2010) and Schwarzer et al. (2019). Heterogeneity between studies was assessed using an I 2 statistic, representing total variability due to heterogeneity (Higgins & Thompson, 2002).
The goodness-of-fit of meta-analysis results was evaluated by sensitivity analyses based on the leave-one-out method (Viechtbauer & Cheung, 2010) and the assessment of publication bias through contour-enhanced funnel plots (Peters et al., 2008).
Moderator analysis was applied to evaluate differences in the proportion of NDs in the hospital or primary care.
RESULTS
Search results and characteristics of included studies
A total of 191 titles and abstracts were examined for relevance, and 34 full-text publications were reviewed. Of these, 11 studies met the eligibility criteria for inclusion in the meta-analysis (Figure 1).
The 11 studies included 854 patients, 10 were conducted in Brazil and 1 in the USA: 8 in hospital units and 3 in outpatient clinics. They identified 44 most prevalent NDs in patients with HF; five studied the prevalence of NDs (activity intolerance (00092), decreased cardiac output (00029), excess fluid volume (00026), fatigue (00093), and ineffective health management (00078)) in patients with HF, and 6 the prevalence of possible diagnoses in the patient with HF. The latter six studies also identified the above diagnoses, except for ineffective health management (00078).
In these 11 publications, three analyzed risk factors and related factors and DCs from NDs in patients with HF (Carneiro et al., 2018; de Padua et al., 2019; Park et al., 2017;), although the latter 2 focused on analyzing such variables in diagnosis, ineffective health management (00078) and activity intolerance (00092), respectively; 3 studies identified DCs of specific NDs (de Souza et al., 2015; Pereira et al., 2016; Santos et al., 2020). De Souza et al. (2015) identified DCs of activity intolerance (00092), excess fluid volume (00026), and decreased cardiac output (00029), globally for the three NDs; Pereira et al. identified DCs of decreased cardiac output (00029); Santos et al. identified DCs for fatigue (00093); and one study identified related factors for eight diagnoses (da Costa et al., 2016) (Table 1).
Characteristics of included studies and participant.
Of the 44 NDs identified in the 11 studies, 16 are repeated in more than 1 publication and are the ones for which the meta-analysis was carried out.
Regarding the level of evidence (LOE) of each diagnostic label, all have minimum levels of 2.1, except decreased cardiac output (00029), and will be removed from the NANDA-I Taxonomy in the 2024–2026 edition unless the LOE 2.1 or higher is completed with additional work (Herdman & Kamitsuru, 2021–2023).
Most of the 16 NDs identified focus primarily on physiological problems. Thus, except for deficient knowledge (00126) and anxiety (00146) (domains perception/cognition and coping/stress tolerance of NANDA-I), the rest belong to the domains: activity/rest, safety/protection, nutrition, and comfort.
The 16 NDs identify related or very similar human responses. For example, ND activity intolerance (00092), the fifth most prevalent ND, currently labeled decreased activity tolerance (00298), would be related to others belonging to the same domain; thus, it is related to impaired physical mobility (00085) (with related factor decreased activity tolerance) or to self-care deficits (00108, 00109, 00102, 00110) (with related factor impaired physical mobility) (Herdman & Kamitsuru, 2021–2023). On the other hand, there are similar NDs that belong to the same domain with some related factors and matching CDs. Therefore, fatigue (00093), in addition to being an ND in the NANDA-I classification, is also described as a DC of activity intolerance (00092).
Quality assessment of studies
Evaluation of the LOE of the included studies, following the recommendations of the John Hopkins Institute of Medicine (Dang et al., 2021), produces the following results: 7 (63.6%) Level III A (high quality) and 4 (36.4%) Level III B (good quality). The results of the quality assessment of the selected studies are described in the last column of Table 1.
Results of the meta-analysis
The combined mean proportion takes a value of 35.73% (95% CI = [26.67%; 48.56%]). Figure 2 shows both the combined mean proportion and the proportions for each of the diagnoses, with a 95% CI. The heterogeneity measures I 2, τ 2, and heterogeneity test are also incorporated for the pooled proportion and by diagnosis, which indicates the presence of heterogeneity. However, although heterogeneity is high, the prediction interval for the pooled proportion (9%–96%) indicated that future studies will fall above 0.
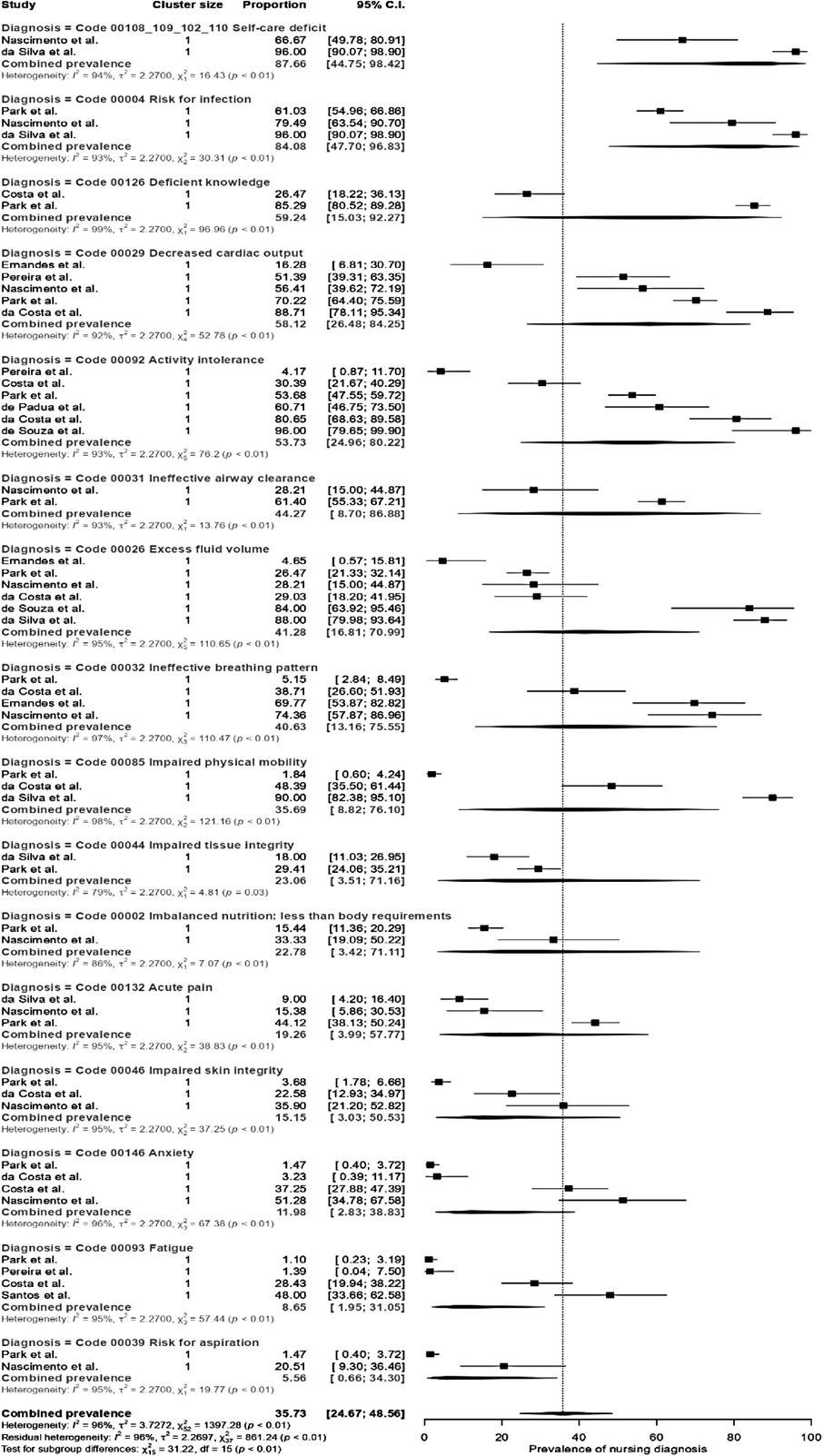
Forest plot.
On the other hand, the moderator analysis indicates that there are no significant differences between the prevalence of NDs used between hospital and primary care (Q (df) = 0.01 (1), p-value = 0.99), with a pooled proportion of NDs in hospital of 35.7% (95% CI = [24.01%, 49.2%]); and in primary care of 35.9% (95% CI = [9.3%; 75.5%]).
In the forest plot (Figure 2), each ND is ordered by prevalence. We could determine higher or lower prevalences for all NDs whose combined prevalence falls outside the confidence interval of the overall combined prevalence. That is, those with a prevalence below 24.97 (they are less prevalent) or above 48.56 (they are more prevalent). Thus, the most prevalent would include: decreased cardiac output (00029), activity intolerance (00092), excess fluid volume (00026), and ineffective breathing pattern (00032), which would correspond to typical symptoms caused by a structural or functional cardiac abnormality resulting in inadequate cardiac output at rest or during exercise (Hill et al., 2022). The less prevalent diagnoses would be: (impaired tissue integrity (00044), imbalanced nutrition: less than body requirements (00002), acute pain (00132), impaired skin integrity (00046), related to the deterioration of health status and the need for hospitalization.
Analysis of publication bias and sensitivity
Publication bias seems to be absent. The results of Peter's test (t(df) = 0.37 (51), p-value = 0.71 showed no funnel plot asymmetry.
Sensitivity analysis using the leave-one-out method does not indicate that there is any publication that has a particular influence on the measure of effect.
Heterogeneity
To try to reduce heterogeneity, a new variable is incorporated, which we will call a group, and which presents two categories: group A: studies that identify certain ND in patients with HF; group B: studies that identify possible ND, not predetermined. One way to reduce heterogeneity is to introduce variables into the meta-analysis model, perform what is known as meta-regression, and observe the change in the parameters τ 2 and I 2. Incorporating the different variables (without moderating variable, group, dx, group + dx, group + dx + country, group + dx + scope, and group + dx + country + scope) into the model reduces heterogeneity (τ 2) but reduces the parameter I 2 by very little, which always obtained values greater than 95%, indicating high heterogeneity.
DISCUSSION
This research quantitatively investigates the prevalence of NANDA-I NDs associated with the care of patients experiencing HF. Our meta-analysis aims to generate evidence for clinical decision-making in the identification of NANDA-I diagnoses in patients with HF. Additionally, with this systematic review and meta-analysis, we want to test whether the identified diagnoses are clinically useful for treating patients with HF.
Education and the promotion of self-care are key points in the management of this disease (MDConagh et al., 2021). In this regard, the diagnosis of poor knowledge (00126) has been identified in our meta-analysis as one of the most prevalent. To support its importance, the study by Silva et al. (2021) aims to develop a mid-range nursing theory on deficient knowledge in individuals with HF. The consensus study by da Silva Correia et al. (2021) also identifies this diagnosis. Furthermore, one integrative review (Cavalcanti & Pereira, 2014) points out how this ED can affect treatment adherence, which is one of the main causes of HF decompensation. In addition, other articles evaluated the effectiveness of education and promotion of self-care through the implementation of interventions from the Nursing Interventions Classification (NIC) and with the outcomes of the Nursing Outcomes Classification (NOC) in patients with HF (Carneiro et al., 2016; Oliveira et al., 2020). Finally, a systematic review and meta-analysis evaluated the effectiveness of health education interventions versus usual care for adherence to treatment and self-care in patients with HF (Tinoco et al., 2021).
In this sense, some NDs can be considered secondary because of their relationship with other NDs that could be considered a priority. This concept indicates that the diagnosis takes precedence over others for the achievement of the objectives, minimizing, interrupting, or preventing the development of others, and secondary NDs would be those that have the failure of the priority diagnosis as a causal factor (da Silva Correia et al., 2021). Thus, deficient knowledge (00126) (priority diagnosis) may lead to other secondary NDs such as activity intolerance (00092), excess fluid volume (00026), and ineffective breathing pattern (00032), which would be the patient responses to decreased cardiac output (00029). These NDs are less prevalent and related to the deterioration of health status and the need for hospitalization. In this sense, numerous publications also support such diagnoses in patients with HF, such as reviews (Cavalcanti & Pereira, 2014; de Almeida Neto, 2017; Vianna et al., 2021; de Souza Carneiro et al., 2017), consensus studies (Azzolin et al., 2012; da Silva Correia et al., 2021), precision (Pereira et al., 2015; Trojahn et al., 2020), and validity (Rojas Sánchez et al., 2017).
However, the diagnosis of anxiety (00146) identified among the least prevalent is the only one belonging to the coping/stress tolerance domain. This is even though manifestations of anxiety and other coping responses compromise adequate treatment adherence and self-care to cope with the disease (Dantas Cavalcanti et al., 2013; de Souza Carneiro et al., 2017). Regarding the quality level of the reviewed scientific evidence, high levels of evidence and good quality IIIA–IIB were obtained, which supports the robustness of the results of our meta-analysis (Dang et al., 2021).
The development of the ND is based on the diagnostic indicators: DC, risk factors, and related. However, of the 11 publications, only three look at related factors and DCs, another three studies identified only DCs, and only one study identified related factors. Identification of nursing diagnostic criteria should always be present in this type of study, which is the only possible way to advance diagnostic precision and is crucial to the development of ND.
Regarding the LOE, decreased cardiac output (0029) is the fourth most prevalent ND. Currently, related factors are pending development, since these had all disappeared in the 2018–2020 edition. In other words, we are dealing with a diagnosis that is considered prevalent in HF, with numerous publications supporting it, and which could be withdrawn from NANDA-I. However, the thinking might be that it does not have manageable related factors with independent nursing interventions, as HF is a clinical syndrome that results in inadequate cardiac output at rest or during exercise, closely related to the pathophysiology of the disease (MDConagh et al., 2021).
The results of this meta-analysis indicate the presence of heterogeneity, which would show that the individual results of the studies included in the meta-analysis differ from each other. Most of the studies were conducted in the hospital, but there were no significant differences between the prevalence of hospital NDs and consultation. In this type of meta-analysis, in which the measures collected show a high level of variability, it is common for there to be heterogeneity. There might have been a variable that could reduce it, but which is not present in these publications, as observed in the results of the meta-regression carried out. It is important to note, given the sensitivity study, that no study has a special influence on the estimated prevalence. Possible causes or sources of such heterogeneity as shown throughout this article would be the complexity of interpreting similar human responses that share domain/class, and the result is that some, others, or both are identified. In addition, not only have diagnoses related to HF been identified, but also those related to hospitalization and/or deteriorating health status. Finally, an important part of the differences could be due to the different study designs (retrospective, prospective, or cross-sectional).
One limitation is the fact that, of the 11 studies that met the eligibility criteria, all but one were in the same cultural context. However, this shows that this country actively participates in the search for a higher level of understanding in this area and that the literature elsewhere in the international arena is very scarce. Future studies should be implemented in other countries to increase scientific evidence on the prevalence of NDs in other cultures.
Implications for nursing practice, research, policy, and education
This meta-analysis focuses on the examination of the most prevalent NANDA diagnostic labels in the clinical setting of people affected by HF. The accumulated findings provide substantial evidence to rationalize the formulation of evidence-based standardized care plans while delineating key endemic gaps and challenges in this area of clinical knowledge.
These findings, by extension, are poised to empower nursing professionals in the discernment of diagnostic determinations and the judicious application of precision care plans based on the precepts of the most robust scientific evidence articulated through standardized languages. Furthermore, they facilitate proactive forecast interventions of maximum effectiveness, thus helping healthcare administrators make decisions regarding resource allocation that meet the nuanced care demands of the aforementioned patient cohort.
Moreover, the implications extend beyond the immediate clinical setting to positively influence the fields of research and education, thus substantially contributing to the evolving trajectory of nursing as a scientific discipline. Especially important for prospective research is the imperative validation of the diagnostic labels defined through this meta-analysis concerning patients with HF. Additionally, the discernment of fundamental diagnostic indicators emerges as an imperative prerequisite for conducting differential diagnostic analyses and ensuring the practical applicability of these findings in the clinical setting.
CONCLUSIONS
The results of this meta-analysis indicate that the priority and secondary diagnoses in patients with HF would be the following: deficient knowledge (00126), being secondary Intolerance to activity (00092), excess fluid volume (00026), and ineffective breathing pattern (00032), which would be the response to decreased cardiac output (00029), which we would not consider ND but a sign of HF. In addition, NDs are less prevalent related to deterioration of health status and the need for hospitalization.
Finally, nurses in HF pathology should recognize not only physiological changes but also emotional and psychosocial changes for holistic care. The importance of the emotional and psychosocial spheres in chronic conditions such as HF should be emphasized.
AUTHOR CONTRIBUTIONS
Conceptualization: Inmaculada Paneque-Sánchez-Toscano; María-Reyes Carrión-Camacho; Ana-María Porcel-Gálvez; Regina Allande-Cussó. Data curation: Inmaculada Paneque-Sánchez-Toscano; María-Reyes Carrión-Camacho; Regina Allande-Cussó. Methodology: Inmaculada Paneque-Sánchez-Toscano; María-Reyes Carrión-Camacho; Ana-María Porcel-Gálvez; Regina Allande-Cussó. Writing—original draft: Inmaculada Paneque-Sánchez-Toscano; María-Reyes Carrión-Camacho; Ana-María Porcel-Gálvez; Regina Allande-Cussó. Writing—review and editing: Inmaculada Paneque-Sánchez-Toscano; María-Reyes Carrión-Camacho; Ana-María Porcel-Gálvez; Regina Allande-Cussó.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
FUNDING INFORMATION
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
ETHICS STATEMENT
The study did not involve human beings so no Ethical Approval is required for this study.