
Abstract
Purpose
The purpose of this study was to examine knowledge, attitude, and barriers toward care planning documentation practices with standardized nursing languages (SNLs) of nurses and nursing students at a midwestern healthcare system, comparing student and nurse responses.
Methods
Cross-sectional surveys were given over a 2-month period with nurses and nursing students at different sites in a midwestern healthcare system, using convenience sampling. The Knowledge, Attitude, and Barriers to Using Standardized Nursing Languages and Current Practices Survey was adapted for use and re-tested for validity/reliability (Content Validity Index 0.81–1.00; Cronbach alpha = 0.82–0.99) with 28 Likert scale items measuring knowledge, attitude, and barriers. Descriptive statistics, composite scores, correlations, t-tests, and multiple regression were used to analyze the concepts of the tool.
Findings
134/400 RNs responded (34%); 109/116 students responded (93.9%). Data analyses indicate adequate to superior levels of knowledge related to SNLs and NANDA International, Nursing Interventions Classification (NIC), and Nursing Outcomes Classification (NOC), collectively referred to as NNN (NANDA, NIC, & NOC), positive attitudes toward SNLs/NNN and for adopting SNLs/NNN into documentation practices, but moderate to great barriers for implementation in practice. Barriers included lack of financial resources for change, lack of mentors, and lack of mandates to use SNLs. Students scored significantly higher than nurses in attitude only.
Conclusions
Perceptions of nurses and student nurses for current documentation indicate awareness of inadequacy in existing systems and willingness to change existing systems for standardized languages, with perceived barriers to change/implementation of SNLs. Students were more positive about SNLs than nurses.
Implications for nursing practice
Major implications for nursing are to reevaluate electronic documentation systems and determine how to insert and easily apply SNLs in these systems, such that nursing care documentation is standardized, interoperable, effective, time-saving, and attainable.
INTRODUCTION
Accurate nursing documentation is not only important for communication between nursing and other healthcare staff but is also an important source of information about patients’ needs and potential nursing actions to address those needs (DeGroot et al., 2020). Since nurses are responsible 24 h each day for continuously identifying care issues as well as implementing and adjusting care prescribed by themselves and other providers to achieve desired patient outcomes (Macieira et al., 2019), the electronic health record (EHR) could and should provide a means to enhance both healthcare worker communication efforts and patient care quality and be perceived as useful by nursing personnel.
As an information repository with data stored in digital form, the EHR contains retrospective, concurrent, and prospective patient information, which in turn can support continuing, efficient, and quality integrated healthcare (Häyrinen et al., 2010). Unfortunately, EHRs serve multiple purposes and have become a maze of legal notations, checkmarks, numerical entries, and test results, with no clear indication that “the big picture” or the progression (or lack thereof) of that patient's healthcare journey has been duly noted and routinely addressed by anyone who has regular contact with the patient. Compounding the problem is the lack of standardized, interoperable nursing data required for conducting research, which also raises the issue of whether these current documentation systems meet the unique needs of nurses.
BACKGROUND
Recent research in the area of nursing electronic documentation has revealed several key issues: Standardized nursing languages (SNLs) will improve the quality of nursing documentation, assist in the fulfillment of the legal requirements of documentation, and facilitate the use of an EHR (Johnson et al., 2018; Müller-Staub et al., 2006, 2008; Saranto et al., 2014); SNLs include better, safer, and more efficient care while underpinning statistical reporting, decision making, performance and outcomes measurement, and cost analyses (Teixeira et al.,2015; Østensen et al., 2020); most EHRs in the United States do not incorporate any of the SNLs recognized by the American Nursing Association (ANA) (Keenan, 2014; Rutherford, 2008; Staggers, 2013; Westra et al., 2015); the lack of SNLs in EHRs results in inability to use nursing data to determine if nursing interventions or actions lead to improved patient outcomes (Jones, 2016; Staggers, 2013; Wagner et al., 2023); and inability to connect nursing interventions (actions) to patient outcomes hinders the ability of nurses to determine and apply evidence-based practice (Alderden & Cummings, 2016; McCormick et al., 2015; Saranto et al., 2014; Scherb et al., 2013; Wagner et al., 2023). More importantly, lack of evidence of nursing planning and nurse critical thinking in the form of nursing SNLs leads to inability to determine important patient needs and outcomes, such as nursing intensity, patient length of stay, and patient acuity (Sanson, 2023). In fact, recent research indicates the use of SNLs increases ability to predict patient complexity, length of stay, and nursing care requirements in the Intensive Care Unit (Castellan et al., 2016; D'Agostino et al., 2017; Sanson et al., 2019).
Research is lacking, however, in detailing the perceptions of the nurses related to the current state of nursing documentation, specifically the inclusion of SNLs in the EHR. Although two surveys were administered from 2009 to 2011 by Schwirian and Thede (2012) and Thede and Schwirian (2013a, 2013b, 2013c, 2014, 2015), and the results indicated that a majority of the surveyed nurses were familiar with and comfortable in using some of the nursing SNLs, it should be noted that EHRs were relatively new at that time and vendors had not begun to routinely dictate nursing documentation practices through their products.
Despite these promising findings, more recent research demonstrated that the vendors of documentation systems are increasingly creating their own nursing languages and unique documentation systems. Staggers (2013) in her testimony to the Office of the National Coordinator (for Health IT) stated that every site starts its own EHR from scratch and is encouraged by vendors to do so. This makes sharing content across sites unwieldy with interoperability of the data very low. This is problematic for nursing departments as nursing documentation needs are often overshadowed by the need for legal requirements and financial billing needs. This has resulted in nursing documentation in EHR systems that focuses on flowsheets with check-boxing tasks and assessments, making the intellectual and critical thinking work of nurses to identify patient problems, plan interventions, and measure outcomes of those interventions largely invisible in our current EHRs (Wagner et al., 2023).
Internationally, DeGroot et al. (2020) surveyed 667 Dutch nurses and found that EHRs did not have user-friendly designs and that staff did not feel supported by the EHRs. DeGroot et al. (2020) attributed this to the inconsistent and variety of ways in which software developers have integrated standardized terminologies, similarly to Staggers (2013) and Keenan (2014) in their findings.
Schools of nursing report that accurate electronic documentation is a necessary method of addressing the requisite knowledge of nursing in the new millennium (Clingerman, 2000). According to Clingerman (2000), when SNLs have been integrated into such areas as clinical assignments, discussion groups, papers, projects, and plans of care, students are able to identify and describe discrete differences in concepts, are able to learn to develop a plan of care related to the provision of healthcare in a variety of community-based and acute care settings, and are able to bring a new sensitivity to their patient assessments. Hansen and Bratt (2015) reported increased student comprehension of essential nursing concepts of care when using SNLs. Eardley et al. (2018) noted that using a case study assignment requiring electronic documentation with SNLs to guide the nursing process allowed for a higher level of content mastery.
In view of this information, it is apparent that nurses need to be using SNLs in their daily practice. Furthermore, nursing students need to have SNLs in their curricula.
PURPOSE OF THE STUDY
The purpose of this study was to determine perceptions and experiences of nurses and nursing students related to SNLs and their usefulness in nursing documentation systems. The inclusion of student nurse perceptions adds to the richness and uniqueness of this study. Study objectives included: Describe the level of nurse and student nurse knowledge of SNLs in their current practice, using the NANDA-I (NANDA International [formerly the North American Nursing Diagnosis Association {NANDA}]), the Nursing Interventions Classification (NIC), and the Nursing Outcomes Classification (NOC), collectively referred to as NNN (NANDA, NIC, & NOC). Describe nurses’ and student nurses’ attitude toward and perception of usefulness of SNLs and NNN. Describe perceived barriers for nurses and student nurses to implement NNN into nursing documentation. Determine relationships and differences between knowledge, attitude, and perceived barriers between and among nurses and student nurses. Determine relationships between demographic data and knowledge, attitude, and perceived barriers for nurses and for student nurses.
This study will focus on NNN, as research has demonstrated that NNN are the most comprehensive classifications and the only classifications with a sound taxonomic nursing structure (Herdman et al., 2021; Müller-Staub & Rappold, 2017; Müller-Staub et al., 2007) that have the highest familiarity with nurses for any of the ANA approved SNLs (Thede & Schwirian, 2012) and are the most frequently found in publications and research studies (Macieira et al., 2019; Tastan et al., 2014).
METHODOLOGY
Study design and scope
Using a descriptive tailored survey with a cross-sectional data collection plan, nurses and nursing students at a mid-level midwestern integrated health system with its associated accredited college of nursing (baccalaureate and master's degree) were recruited to participate. The scope of the study was limited to practicing nurses and student nurses as follows: Practicing nurses were recruited at three of the hospital sites of the health system and were contacted during a mandatory health fair that occurred at each site for a period of one to two days. This recruitment period lasted for 3 months, ending when the health fair ended. All nurses attending the mandatory health fair were solicited to participate. The student nurses were recruited during a 1-month period where researchers solicited participation before and after mandatory large group classes that occurred twice weekly. All student nurses attending the classes during that time frame were solicited to participate. Each participant was consented and then asked to complete the instrument described in a subsequent section.
Participants
Sampling for this study included nurses from all areas of patient care in three separate sites of a mid-level midwestern health system attending a mandatory health fair at each site. Although all possible efforts were made to allow all Registered Nurses an equal chance of participating, it was not possible to contact all the eligible staff because many worked very infrequently or were working during the mandatory health fairs. Inclusion criteria were Registered Nurses working any shift and any unit for all sites. Exclusion criteria were those not holding a Registered Nurse license.
Student nurses were recruited at the school site during class sessions that were mandatory for all nursing students. Each session was comprised of either junior or senior level baccalaureate nursing students. Masters’ classes had not started yet so those in the masters’ programs were not recruited. Inclusion criteria were any nursing student currently enrolled in the school. Exclusion criteria were non-nursing students enrolled in the school (the school has radiology, health sciences, and medical laboratory programs).
Instrumentation
The School Nursing Documentation: Knowledge, Attitude, and Barriers to using SNLs and Current Practices Survey (SND), was created by Yearous (2011), uses words that are well defined to minimize misinterpretation of questions, ensures that each question measured a single idea, and uses the Diffusion of Innovations theory (Rogers, 2003) as a guiding framework. The sections of the survey are as follows: (1) demographics (items 1–15), (2) knowledge (items 16–22), (3) attitude (items 23–34), (4) barriers (items 35.1–35.9), and (5) current documentation practices (items 37–54). The various sections of the survey were developed by Yearous using focus groups, literature reviews, concepts from Rogers (2003) Diffusion of Innovations theory, standards of nursing documentation, expert opinions, and reliability and validity testing that included pilot testing of the instrument. Likert responses were developed for each section of the survey based on recommendations from Fowler (1995) and DeVellis (2003).
Methods to measure validity and reliability of the initial SND survey occurred in several phases, included content validation by experts, use of vignettes, and several iterations of reliability and validity testing in pilot tests of the instrument. Various iterations of the instrument were trialed and rated using item-objective congruence forms and ratings. The Scale-Content Validity Index (CVI) scores were 0.81 for knowledge section, 0.94 for attitude section, 1.00 for barriers section, and 0.92 for documentation practices section. The multiple phase testing and various iterations of the instrument resulted in a final instrument deemed to be reliable and valid (Yearous, 2011). In applying the instrument in her study, Yearous found adequate reliability for the instrument, obtaining Cronbach's alpha scores for the three areas of the instrument ranging from 0.81 to 0.88 (Yearous, 2011, p. 85).
The instrument was adapted slightly from its school nurse references and questions related to the school nursing functions to those references familiar to acute care nursing staff and nursing students. The adapted instrument was renamed the Knowledge, Attitude, and Barriers to Using Standardized Nursing Languages and Current Practices Survey. The majority of the adaptations were to the demographics section of the instrument or with minor adaptations to the survey section, such as removing the word “school” in questions where it noted “school nurse” or removing questions related to school nurse activities (e.g., “have you ever accessed the NASA position statement”). The adapted questionnaire had 38 questions, including Yearous’ section on documentation practices. The adaptations were approved by Yearous (now Dr. Sharon Guthrie) (personal communication, March 28, 2018). Nonetheless, the altered content was validated by nursing experts to assure the adaptations did not alter the questions in such a manner as to compromise the characteristics that the original instrument was designed to measure. A group of three nurse educators reviewed both the original and adapted instrument and determined that the adapted questions remained relevant and inclusive of all important topics. These educators used an item-objective congruence evaluation form to rate whether each survey item from the adapted instrument was relevant to the corresponding objective of the survey. The rating scale provided three options: +1 (definitely a measure of objective), 0 (undecided), and −1 (definitely not a measure of objective). Ideally the CVI scores should be 1.00 when there are five or fewer experts “to be considered a reasonable representation of the universe of possible ratings” (Lynn, 1986, p. 383). The CVI scores were 1.00 for the knowledge section (questions 1–6), 0.94 for the attitude section (questions 7–18), and 1.00 for the barriers section (questions 19–27). The CVIs were nearly identical to the original CVIs reported by Yearous (2011). Finally, internal consistency was verified with the use of Cronbach alpha on the data from the adapted instrument (knowledge = 0.87–0.94, attitude = 0.91–0.97, barriers = 0.83–0.99), which was consistent with Yearous’ original alphas (knowledge = 0.87, attitude = 0.88, barriers = 0.81).
Data collection
Staff nurse solicitation for participation occurred during a mandatory health fair that was provided at the three separate locations and on several different days during the months of May and June of 2018 for all nurses that attended the health fair. An attractive posterboard presentation was created to entice interest, and a brief presentation was provided. Seating at nearby tables allowed for quiet and private completion of the questionnaires and consents. A researcher was present throughout each health fair to field questions, provide consents and questionnaires to interested persons, and collect completed consents and questionnaires.
Students were solicited after attendance at lectures, examinations, or clinical skill checks in the lobby of the nursing school using the attractive posterboard and a short presentation. Seating at nearby tables and a lounge area allowed for quiet and private completion of the questionnaires and consents. A researcher was present throughout each solicitation to field questions, provide consents and questionnaires to interested persons, and collect completed consents and questionnaires.
Data analysis
Data were analyzed based on the individual objectives and following the analysis patterns of Yearous (2011). Initially, a general analysis began with calculations of descriptive information for the samples and including frequencies and percentages for item responses. Data sampling occurred to check for reliability of data entry, missing data, and accurately entered data. To analyze, compare, and determine relationships among and between nurses and student nurses, the responses in each section of the knowledge, attitude, and barriers constructs were examined for normalcy and combined to create composite scores for each construct (composite knowledge, composite attitude, and composite barrier), as recommended by Yearous to facilitate statistical analyses (2011, p. 65).
For composite knowledge scores, the option “none (do not know)” was the lowest value, which converted to numeric coding so it did not skew composite scores. For regression models that included composite attitude scores, the category “not enough knowledge to have an opinion” was re-coded to equal the neutral category, “have enough knowledge but neither agree nor disagree” so those without enough knowledge were not negatively affecting the overall attitude composite values. This substitution was controlled for using a dichotomous variable scored one for respondents who did not have enough information to answer and zero for respondents who did. Composite barrier score was determined by adding the sum of the nine barrier items.
Regression analysis was used to determine if there are certain variables that predict the knowledge level and adoption of SNLs. For aims with dependent variables that were continuous, multiple regression was used. For aims with dependent variables that were categorical, logistic regression was used. Multiple regression was used to determine relationships among and between the nurses and student nurses for the variables of interest. Composite scores between nurses and student nurses were also compared using t-tests where appropriate. Some correlations between demographic data and the three constructs were computed using chi-square analyses, due to non-normalcy of these data fields.
Study objective #1
Describe the level of nurse and student nurse knowledge of SNLs in their current practice, using NNN. Descriptive statistics including frequencies and percentages were used to analyze the data obtained from the knowledge sections of the questionnaire.
Study objective #2
Describe nurses’ and student nurses’ attitudes toward and perception of usefulness of SNLs and NNN. Descriptive statistics including frequencies and percentages were used to analyze the data obtained from the attitude sections of the questionnaire.
Study objective #3
Describe perceived barriers for nurses and student nurses to implement NNN into nursing documentation. Descriptive statistics including frequencies and percentages were used to analyze and describe the data obtained from the barrier sections of the questionnaire. Graphs were used to display and compare barriers for nurses and student nurses.
Study objective #4
Determine relationships and differences between knowledge, attitudes, and perceived barriers between and among nurses and student nurses. Multiple regression was computed with a model using composite knowledge score as the dependent variable and, for nurses, composite attitude, composite barriers, age, educational level, and total years practiced as a nurse as the independent variables. For student nurses, composite knowledge score was the dependent variable, and composite attitude, composite barriers, age, and average clinical hours were the independent variables. Next, multiple regression was computed as described above, but interchanging composite attitude score as the dependent variable and adding composite knowledge as one of the independent variables. Next, multiple regression was computed as described above, but interchanging composite barrier score as the dependent variable and using composite knowledge and composite attitude as independent variables, along with the abovementioned demographic variables. Independent t-tests were used to determine significant relationships or the lack thereof, with multiple regression used to determine strength of relationships when present.
Study objective #5
Determine relationships between demographic data and knowledge, attitude, and barriers for nurses and for student nurses. Chi-square analyses and Pearson correlations were used to determine predictor variables for any of the constructs in the demographic data, with multiple regression models computed as described above.
Ethical aspects
Permission to conduct the study was obtained from the Institutional Review Boards (IRBs) of both the school of nursing and from the healthcare system. Assurances of confidentiality were made. Volunteers were not paid for participation, although refreshments were provided. Participants were given the option to return a blank questionnaire or mark it refused if they did not wish to participate. There were no identifying names or numbers on the questionnaires.
Findings
The findings of this study are presented in three subsections. The first section describes the demographics of the subjects that participated in this study, separated into the two groups. The second section addresses findings for each of the study's specific aims. The third section briefly provides the results of the additional statistical analyses related to reliability of the survey tool adapted for this study.
Demographics and characteristics of the samples
Four hundred RNs signed log-in sheets for the health fairs and 134 completed a questionnaire for a 34% response rate. There were 116 student nurses contacted and 109 completed a questionnaire for a 93.9% response rate. Descriptive statistics derived from the demographic data analyses are presented in Table 1.
Demographic data.
Abbreviation: BSN, Bachelor of Science in Nursing.
Study objective #1 knowledge of NNN
The majority of nurse participants noted adequate to superior knowledge of NANDA-I, NIC, and NOC (ranges 48%–51%). Nurses reported lower NANDA-I knowledge than NIC or NOC knowledge overall (48% for NANDA-I vs. 51% for both NIC and NOC). The mean and mode of the nurse responses corresponded to the adequate knowledge selections for NIC and NOC (μ = 2) but were slightly less for NANDA-I (μ = 1.75).
The majority of student nurses noted adequate to superior knowledge of NANDA-I, NIC, and NOC (ranges 49%–61%). Student nurses reported lower NOC knowledge than NANDA-I or NIC knowledge overall (49% NOC vs. 53% NIC and 61% NANDA-I). The mean and mode of the student nurse responses corresponded to the adequate knowledge selections for NANDA-I and NIC (μ = 2) but were slightly less for NOC (μ = 1.66). Descriptive statistics for the nurse and student nurse knowledge data are presented in Table 2.
Knowledge data analysis.
Abbreviations: NANDA-I, NANDA International; NIC, Nursing Interventions Classification; NOC, Nursing Outcomes Classification.
Study objective #2: attitude and perception of usefulness of NNN
A majority of the nurses (61% or >) noted that they completely agreed or generally agreed with SNL use in documentation and that they were willing to change to use NNN in their current documentation (73%). Additionally, large majorities (76% or >) of the nurses noted that they recognized the advantages of NNN and that NNN were consistent with nurse values and needs. Specifically related to NNN, 77% were agreeable to change to NANDA-I, 74% to NIC, and 73% to NOC. Overall, the attitudes of the nurses toward SNLs and NNN were positive, with the dispersions of the data for each question demonstrating a right skew.
A majority of the student nurses (75% or >) noted that they completely or generally agreed with SNL use in documentation and that they were willing to change to use NNN in their current documentation (75%). Additionally, large majorities (87% or >) of the student nurses noted that they recognized the advantages of SNLs and that SNLs were consistent with nurse values and needs. Specifically related to NNN, 87% were agreeable to change to NANDA-I, 78% to NIC, and 75% to NOC. Overall, the attitudes of the student nurses toward SNLs and NNN were positive, with the dispersions of the data for each question demonstrating a right skew. It is of interest to note that neither nurses nor student nurses selected “completely disagree” for any of the attitude construct questions. Descriptive statistics for the nurse and student nurse attitude data are depicted in Table 3.
Attitude and perceived usefulness of NANDA, NIC, & NOC (NNN).
Note: 5 = completely agree, 4 = generally agree, 3 = neither a/d, 2 generally disagree. 1 = lack knowledge, no completely disagree selected.
Abbreviations: NANDA-I, NANDA International; NIC, Nursing Interventions Classification; NOC, Nursing Outcomes Classification; SNL, standardized nursing language.
Objective #3: perceived barriers for NNN implementation
Both groups noted most of the barriers listed in the survey were moderate to great barriers. The barriers perceived as greatest for RNs were lack of mentors, lack of a mandate from administration, lack of time to learn a new system, and lack of financial resources. Students perceived the greatest barriers as lack of knowledge of SNLs, lack of financial resources, lack of time to learn a new system, and lack of a mandate from administration. Table 4 depicts descriptive statistics for the barrier constructs, and Figures 1 and 2 graphically depict barrier comparisons.
Perceived barriers for NANDA, NIC, & NOC (NNN) implementation in current organization.
Abbreviations: NIC, Nursing Interventions Classification; NOC, Nursing Outcomes Classification; SNL, standardized nursing language.
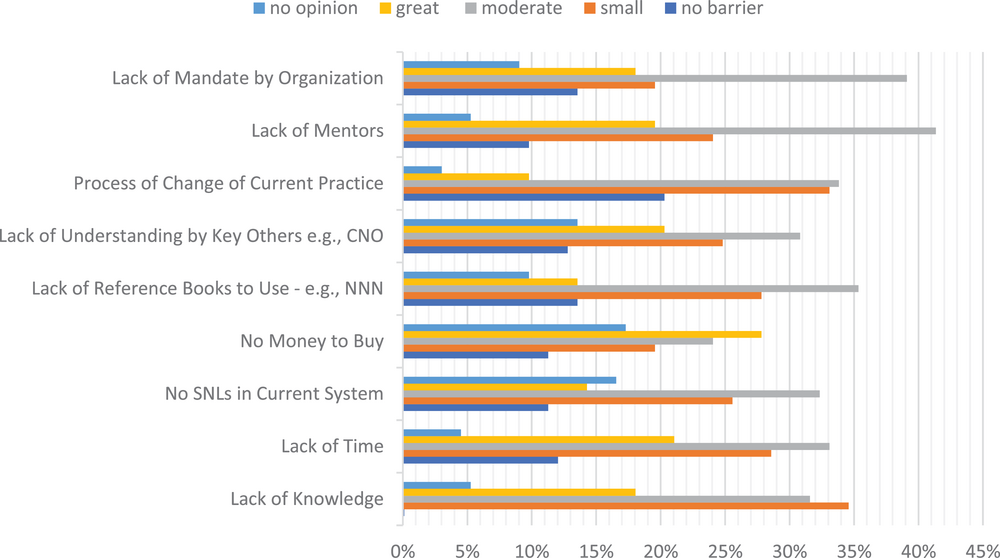
RN perceptions of barriers to standardized nursing language (SNL) adaptation. NNN, NANDA, NIC, & NOC.
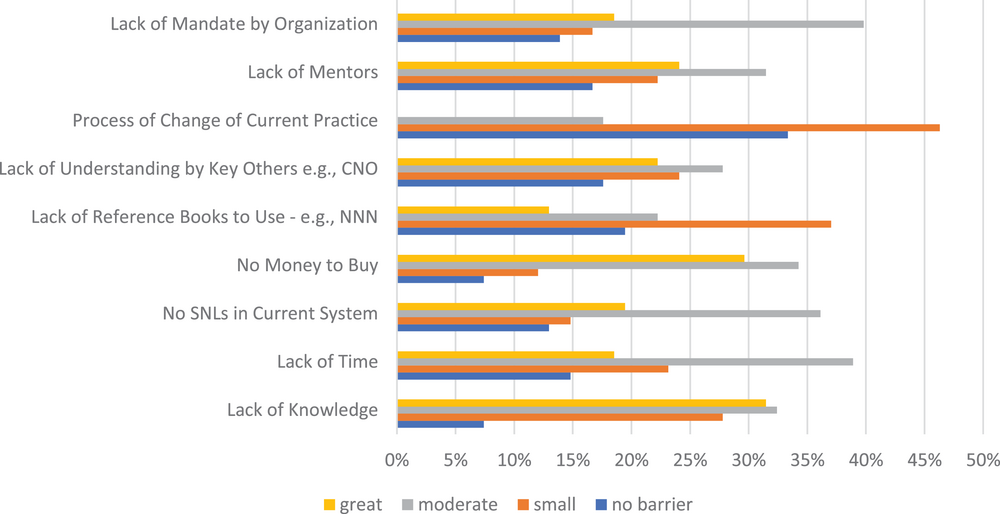
Student perceptions of barriers to standardized nursing language (SNL) adaptation. NNN, NANDA, NIC, & NOC.
Objective #4: relationships and differences between constructs, nurses, and student nurses
For nurses, analyses indicated that there were significant correlations between the constructs of the knowledge, attitude, and barriers. The relationships and the models were significant (see F significance values in Table 5), but predictability was low (see R 2 values in Table 5). For example, for nurses, the attitude and barrier constructs had a positive linear relationship with the knowledge construct (p = 0.0031, 0.0038), but the R 2 was 18%. Trialing various independent demographic variables in the model did not prove fruitful, with the variables as noted in Table 5 demonstrating the strongest model. For attitude, total years as RN also had a positive linear relationship with the attitude construct (p = 0.019), along with the barrier and knowledge constructs (p = 0.037, p = 0.00026), and R 2 was 15.1%. For the barriers construct in nurses, only the knowledge construct had a positive linear relationship that was significant (p = 0.0038). The R 2 was 18.9%.
Relationships between constructs, nurses, and student nurses.
Statistically significant.
For student nurses, the attitude construct and age had a positive linear relationship with the knowledge construct (p = 0.0063; p = 0.0206), with an R 2 of 22%. For the attitude construct, only the knowledge construct had a significant p value (p = 0.0063) indicating a positive relationship, with an R 2 of 9%. For the barriers construct in student nurses, only the knowledge construct had a positive linear relationship that was significant (p = 0.0046). The R 2 was 8.5%.
There were significant differences in attitude scores between student nurses and RNs, with the students having significantly higher (or more positive) attitude scores than the RNs. There were no significant differences in knowledge or barrier scores between student nurses and RNs.
Objective #5: relationships between demographic data, constructs, nurses, and student nurses
As noted in Table 5, there were two statistically significant findings. Years as an RN were statistically significant, along with knowledge and barrier scores, for explaining a respondent's attitude about SNLs, and in the students, attitude score and age were statistically significant in explaining knowledge about SNLs.
There were no correlations between the nurse demographic data and the three constructs of the scale when examined independently using Pearson's correlation and chi-square where indicated, although a weak negative correlation appeared between years as a nurse and knowledge of NANDA-I, as well as a weak correlation between age and gender (male) and knowledge of NANDA-I. These 3 weak correlations were all statistically significant. There were no correlations between the student demographic data and the three constructs of the scale, although a weak correlation that was statistically significant appeared between hours worked and some of the individual questions related to willingness to change documentation practices.
Reliability of the instrument
This use of the instrument provided the opportunity to further explore the reliability of the survey instrument. In addition to the content validity using expert opinions as noted above, confirmatory analyses using Cronbach's alpha were calculated for each of the composite variables (knowledge, attitudes, and barriers) in each of the data sets for nurses and student nurses to assess the reliability of the composite variables (Table 6).
Reliability of the instrument.
DISCUSSION
Demographics
Demographic data are representative of the population of this Midwestern area for nurses and nearly that of the United States in general (F = 82% and M = 12% in the U.S.) (National Council of State Boards of Nursing [NCSBN], 2020). Male nurses and nursing students occur in lower numbers, like national norms (NCSBN, 2020), and Caucasian race is the most common, although minorities, particularly African American, occur in higher numbers nationally (11%) (NCSBN, 2020). Average nurse age is slightly lower than the national average (44 years) (NCSBN, 2020) with numbers of nurses with Bachelor of Science in Nursing education level slightly lower than the national average (42%). Since the school of nursing is a completion degree program, maintaining cooperative agreements with nearby community colleges, students are not admitted to the nursing program until they have finished pre-nursing courses and are considered junior level entry. Thus, third- and fourth-year students are representative of the total population of the school of nursing.
Knowledge
Both groups had a majority of participants reporting adequate to superior knowledge of SNLs and NNN in general, although neither group scored significantly higher than the other in any of the knowledge areas of the questionnaire. This was surprising as students regularly create patient care plans using NANDA-I and some NIC and NOC in their coursework and clinical activities, whereas the staff nurses used the pre-developed care plans that were selectable in their EHRs and which applied only to the 10 most common complaints and/or safety risks for patients (e.g., pain, falls, knowledge, skin condition, activity tolerance). Due to the more focused use and cognitive applications for students in designing care plans, student knowledge of care planning and NNN was expected to have higher scores. Knowledge and attitude were highly positively predictive of each other, which seems logical as the more understanding one has about a topic the more positive one's attitude may be about that topic.
Attitude
The attitude scale reflected considerable willingness to adapt and change documentation practices to include SNLs and/or NNN. The self-reported attitude levels about NNN are more favorable than not in all attitude questions, which was a surprising finding but not an unwelcome one. RNs and students seemed aware that SNLs in EHR documentation are good and useful for nurses. The willingness to change to use any of the SNLs and/or NNN was also surprisingly high, ranging from 73% to 77% for RNs and from 75% to 83% for students. It is encouraging that nearly three quarters of the respondents indicated they would be willing to change their documentation practices. In addition, 79.0% of the RN respondents and 90% of the students recognize the relative advantage of SNLs, whereas 76% of the RN respondents and 87% of the student respondents reported that SNLs are consistent with nursing values and needs (compatibility). As student nurses scored significantly higher than the nurses (p = 0.0068), this reflects considerable willingness to adapt and change documentation practices to include SNLs and/or NNN, compared to the RNs, which may be an indication of students wanting workplaces that mirror what they learn in school (i.e., they use SNLs in school and would like to see them in clinical areas). Research is limited in this area and does not include student nurse documentation issues.
Barriers
For all participants, all listed items were more likely to be perceived as moderate to great barriers (range 52%–63%) except the items pertaining to having NNN resource books or having NNN in documentation systems (See Figures 1 and 2). For the nurses, the greatest barriers reported in this study were lack of mentors, lack of a mandate from administration, lack of time to learn a new system, and financial resources to pay for necessary equipment. For the students, the greatest barriers were lack of knowledge related to SNLs, financial resources to pay for necessary equipment, lack of time to learn a new system, and lack of a mandate from administration. Aside from mentors and lack of knowledge of SNLs, the barriers were very similar between the groups, although not significantly correlated.
Both RNs and students felt finances were a moderate to great barrier. One is reminded of the widely perceived belief among nurses (whether practicing or students) and healthcare workers in general that hospital systems do not have adequate money, as propagated by the frequent and often unnecessary staff reductions (Robbins et al., 2022). Interestingly and recently, a New York Times research study found that several health systems routinely lay off staff to increase profits, often at the expense of safe patient care and nurse well-being, telling staff that money is scarce yet reporting profits in the millions or billions (Robbins et al., 2022). While this information may not be widely known, it certainly calls into question the commonly held nurse and student perceptions that healthcare systems cannot afford to upgrade to better nursing documentation systems that include SNLs.
Both groups also noted time to learn a new system of documentation as a moderate to great barrier, which corresponds to a recently studied phenomenon known as documentation burden. Over the past decades, health care has experienced wide-spread, rapid-paced implementation of the EHR focused on receipt of government financial incentives (Harmon et al., 2020). Often there was not adequate pre-implementation planning or a systematic assessment of the organization's workflows and needs (Harmon et al., 2020). Post-EHR implementation research has provided evidence of unintended consequences due to this rapid EHR implementation, including extra or duplicate documentation for provider convenience, conflicts between electronic and paper-based systems, and unfavorable changes in communication, all known as documentation burden (Padden, 2019).
The other moderate to great barrier with a high selection rate by both groups was lack of a mandate from administration. This could have several implications and meanings, discussed in the implications section below.
In the findings related to comparisons between groups, it seems apparent that both students and nurses were knowledgeable about and value SNLs and became more so with age and experience. Although it is difficult to find substantiating research on this topic (e.g., current nurse developing perception of care plans), it may indicate that as nurses become more indoctrinated to EHRs with increased experiences, they value having a plan of care as well as welcoming SNL additions that result in ease of use of those care plans in EHRs.
LIMITATIONS
Limitations of the study include the fact that this research focused on the use of NNN although other SNLs exist. Responses might be different for different SNLs. The survey did not access nurses and student nurses nation-wide but focused on a circumscribed area of the Midwest. Thus, nurses in other areas of the country might have differing responses. The survey used self-reported subjective ratings of knowledge and not a method to measure actual knowledge and application of using NNN through application questions. Self-reports can involve over- or under-estimating one's abilities. Finally, the original questionnaire was adapted to remove school nurse references and allow for any nurse and/or nursing student to respond. Thus, although validated through this work, the adapted tool is relatively new and needs more applications to assure its reliability and validity.
CONCLUSIONS AND IMPLICATIONS FOR NURSING PRACTICE
The high levels of knowledge and attitudes toward SNLs (specifically NNN) that appear to be present in both RN and student responses (Objectives 1 & 2) suggest that these nurses and soon to be nurses may be ready for different nursing documentation methods, particularly the addition of SNLs such as NNN. This implies that additional research needs to be completed for nurse satisfaction with current documentation system. Although there are several previous studies (many of which are noted above), there are not any recent studies done in the United States and none that study student nurses’ documentation satisfaction.
The barriers to adding SNLs to existing systems (Objective #3) suggest that RNs and student nurses perceive similar difficulties in implementing SNLs, such as adequate time for implementation and mandate from administration. This reinforces the idea that systems must be planned and added strategically and not hastily adopted, and indicates nurses realize these changes must come from upper levels of administration. Adding SNLs to current EHRs must be implemented with nursing expertise and not rely on non-nursing vendor recommendations. Simply adding legal requirements or creating a system that ignores nursing needs and does not use standardized languages for nursing documentation is not adequate. A prudent pathway would include adding the expertise of a nurse informaticist as well as following an effective change strategy such as the Systems Development Life Cycle (McGonigle & Mastrian, 2022), which has been used successfully for documentation changes multiple times by organizations incorporating nurse informaticists.
But more importantly, this study provides much food for thought as to the current state of nursing documentation systems in healthcare and its impact on the delivery of that nursing care. When one recalls that the backbone of nursing education involves creation of a plan of care addressing patient concerns and needs, and the ability of the nurse to adequately create that needed plan in the current documentation systems is not easily accomplished, it begins to shed light on some of the issues occurring now in healthcare and nursing education.
For one, it highlights the rising concern of nursing administrations over the increasing lack of clinical judgment in nurses, particularly new nurses. Tanner (2006) researched clinical judgment in nurses and produced a model that portrays how nurses “think when they are engaged in complex, underdetermined clinical situations that require judgment. It also identifies areas in which there may be breakdowns where educators can provide feedback and coaching to help students develop insight into their own clinical thinking” (p. 209). As noted by Tanner (2006) the model formation indicated that “educational practices must…. act on a responsible vision for excellent care of those patients ……. Clinical reasoning must arise from this engaged, concerned stance, always in relation to a particular patient and situation and informed by generalized knowledge and rational processes” (pp. 209–210). The model indicates that nurses must have a vision or plan to respond to patient needs and achieve outcomes. Tanner (2006) also noted that educational reflection on this plan when taught in schools of nursing can help students to achieve a higher level of critical thinking ability.
It is of note that lack of ability for nurses to provide an accurate portrayal of the care they provide or plan to provide (i.e., care planning) may be a source of the recent uptake in reports of missed care (Bragadóttir et al., 2020; Cho, et al., 2020; Jones, et al., 2015) and nurse concerns related to that care (Jones et al., 2015; Ogboenyiya, 2019). Recent research seems to indicate missed care can be linked to lack of adequate time or resources to formulate or carry out nursing care plans (Papathanasiou et al., 2024). Empirical findings demonstrate associations between patients with missed nursing care, decreased quality of care, and patient safety, resulting in increased rates of patient mortality, errors, and dissatisfaction (Ball et al., 2018; Jones et al., 2015; Recio-Saucedo et al., 2017). When nurses are not able to adequately develop via SNLs, the detailed and targeted nursing care plans to plan the care that addresses patient needs (as they are taught in basic nursing training) communication becomes disjointed, vital information can be scattered across different patient records and databases, or reliance on verbal handoffs that might be misheard, misunderstood, or forgotten arises (Patiraki et al., 2017). Nursing care plans using SNLs are essential to determine patient needs, provide necessary care, and ensure correct patient outcomes (Herdman et al., 2021), and to accurately document that care.
Therefore, nursing academicians and nursing organizational leaders would be well advised to obtain more information about incorporating SNLs into nursing schools and nursing documentation systems. They need to become knowledgeable about these topics to adequately address these apparent documentation needs. Furthermore, nursing administrations in both the practice and educational settings need to be aware of the current issues with nursing documentation and the usefulness of data collection for nursing research. More emphasis and value should be placed on obtaining ease of documentation for nurses, as well as the generation of meaningful patient care data for nurse collaborative communication and research of best practices in nursing. Since nursing administrations in both the practice and educational settings have much influence on documentation practices, they would need to be a driving force for any change. Notably, if healthcare organizations were made more accountable, through such things as governmental mandates and policy-making supported by nurse administrators and deans of nursing school, to responsibly add new or update current EHRs to include the much desired and needed nursing documentation changes (e.g., care plans incorporating SNLs), the resultant positive changes in nursing provision of care, nursing critical thinking ability, and patient outcomes would enable nurses to do what they do best: care for their patients.
Nursing care plans with SNLs have been successfully used for the delivery of high-quality nursing care, but the use of SNLs in current EHRs or electronic nursing care plans is not common. The benefits of the use of SNLs in nursing care plans and documentation systems have been demonstrated in multiple studies (DeGroot et al., 2019). This study builds on previous knowledge and adds additional unique information from student nurses and nurse perceptions. The findings demonstrate a willingness of nurses and student nurses to embrace and add SNLs to their documentation. As such, it encourages the adoption of SNLs to the current EHRs. Once SNLs are adopted and utilized by healthcare organizations, ongoing research can more easily be conducted to monitor the effectiveness of interventions based on patient outcomes, which in turn will add to the required body of evidence-based practice in nursing. Major implications for nursing practice, including research, education, policy, and clinical applications, are to reevaluate nursing documentation systems to determine how to insert and more easily apply SNLs in the current systems, such that nursing care documentation is standardized, interoperable, effective, time-saving, and attainable.
AUTHOR CONTRIBUTIONS
Cheryl Wagner led on research creation and article writing and revisions and critical review of final draft of article. Karen Cummins and Megan Dean assisted with data collection and analysis and critical review of final draft of article.
CONFLICT OF INTEREST STATEMENT
The authors declare no potential conflicts of interest.
FUNDING INFORMATION
The authors received no specific funding for this work.
ETHICAL STATEMENT
Permission to conduct the study was obtained from the Institutional Review Boards (IRBs) of both the school of nursing and from the healthcare system.