
Abstract
In recent years, cities in North America have declared public health emergencies in response to opioid–related overdoses and fatalities. Municipalities are reacting with various interventions and degrees of urgency, whereas harm reduction organizations coordinate the street–level fight against death. Though drug use has long been concentrated in urbanized and downtown areas, these neighborhoods are being addressed with new national attention. This article draws on qualitative interviews with participants in the Downtown Eastside (DTES) in Vancouver and the Tenderloin in San Francisco. I highlight two interconnected themes: (1) the legacy of distrust between municipal officials and drug users and (2) the disconnection between “epidemics” as narrowly constructed public health emergencies and the needs of communities. Findings show ongoing struggles with “progressive” urban agendas. San Francisco minimized fatalities thanks to the early introduction of unregulated naloxone; however, new anti–homelessness legislation and police–led initiatives continue to create social upheaval for drug users. In comparison, the rollout of Vancouver's naloxone program arrived 10 years too late. Organizations are attempting to amplify access to safe injection and overdose prevention sites in the DTES. Using interurban analysis, overdose epidemics can be conceptualized as sociospatial fields of power, providing greater insight into urban marginality and health inequalities.
Municipalities across North America are reporting a significant rise in fatal overdoses. In 2013, 23,000 overdose deaths occurred in the United States; the Center for Disease Control and Prevention reports that from 1990 to 2006, the rate of overdose deaths tripled (Center for Disease Control 2017; Rowe et al. 2016). The Canadian Centre for Addictions estimates that opioid use in Canada has increased 203 percent from 2000 to 2010, second only to the United States (Canadian Centre for Addictions 2017). A statement from the Public Health Agency of Canada, released in June of 2017, stated that there were 2,458 fatalities from opioid–related overdoses in 2016, with the majority of deaths reported being in Western Canada (Public Health Agency of Canada 2017). With the influx of significantly stronger opioids, including fentanyl and carfentanil, overdoses and fatalities have reached the point of an “epidemic,” with cities declaring public health emergencies, as well as state, provincial and federal governments.
Urbanized and impoverished neighborhoods in North American cities have been some of the most impacted by drug use and the risk of overdose. For these areas, the prevalence of drug use and health epidemics is not simply a recent trend. In San Francisco, opioid use and mortality rates also peaked in the 1990s, concentrated in small, “high–poverty” areas of the city, such as the Tenderloin/Civic Center and South of Market (Visconti et al. 2015:758). Vancouver saw a similar statistical peak in the 1990s of a “dual epidemic” of overdoses and fatalities (Kerr et al. 2013). Jozaghi (2014) traces drug use in Vancouver to the densely populated “10–block neighborhood” of the Downtown Eastside (DTES), outlining its history of injection (and noninjection) drug use (p. 213). Misconceptions about intravenous drug use, such as the excess of syringes in the streets, rampant public drug consumption, and concerns over “street safety,” have long been cited as symbols of both Vancouver's DTES and San Francisco's Tenderloin neighborhood. The influx of gentrification in the DTES and the Tenderloin further contributes to the lines of spatial marginality.
Harm reduction efforts have emerged in these cities over the past several years, aiming to reduce opioid–related overdoses and fatalities, as well as HIV and hepatitis epidemics. In 2000, the San Francisco Health Commission officially adopted a harm reduction policy to address substance use in the city (San Francisco Department of Public Health n.d.). The City of Vancouver followed suit in 2005, introducing a drug policy prevention plan informed by harm reduction philosophy (City of Vancouver n.d.). Harm reduction strategies generally try to utilize “the social networks of drug users as sites and tools for intervention,” as discussed by Faulkner–Gurstein (2017:20). A harm reduction intervention includes a variety of tools and networks, such as methadone maintenance programs, needle exchanges and syringe programs, safe injection/consumption sites, and naloxone distribution programs (McCann 2011b). Prior to municipal and health authorities adopting official harm reduction policies, some of the first grassroots approaches were needle exchange programs (NEPs), providing clean syringes to drug users. Many of these programs were street–based initially and operated unofficially against state and federal law (Clarke et al. 2016). San Francisco's Prevention Point started in 1988, operating during a time when the possession of a syringe for injection drug use was illegal without a prescription (San Francisco Aids Foundation 2017). NEPs were opened in 1989 in both Vancouver and Toronto as part of pilot programs (Canadian Centre on Substance Abuse 2004). Peer–led organizations (namely, the Vancouver Area Network of Drug Users and the San Francisco Drug Users’ Union) also emerged in the late 1990s as radical responses to municipal neglect of their communities.
Strategies to fight overdoses have adapted and expanded in recent years. In Vancouver, the safe injection site InSite was founded in 2003. Larger foundations have adopted San Francisco's rogue NEPs, with the distributing over 2 million syringes in 2016 (San Francisco Aids Foundation 2017). In both cities, overdose reversal drugs (i.e., naloxone) have become another tool of local services. With increased public and political attention on cities experiencing overdose epidemics, dynamics among municipal authorities, formal organizations, and community members are shifting. Using the cases of Vancouver and San Francisco, this article addresses the regulation of addiction and poverty under public health emergencies and epidemics. The primary research sites include the DTES in Vancouver and the Tenderloin area in San Francisco; these neighborhoods have long been home to communities fighting the war on drugs, as well as ongoing efforts to combat economic and health inequalities. Qualitative interviews were conducted with individuals from organizations, coalitions, and alliances based in (or primarily serving) these neighborhoods. These groups included harm reduction and peer services, anti–poverty/homeless organizations, and health authorities that either had primary goals of reducing overdoses or, in recent months, adopted overdose prevention initiatives.
This article asks how do municipal and health authorities conceptualize drug–related epidemics compared to community members and front–line workers? How does the regulation of drug use in some of the poorest neighborhoods in North America change when overdose numbers hit the point of crisis? This article contributes to harm reduction literature and urban theory by identifying challenges and successes of overdose prevention in the DTES and the Tenderloin. This article discusses epidemics and the illusion of the “progressive city”—a municipality that is seen as being amenable to public health reform and innovations. The empirical findings detail how organizations continue to face municipal blockades to providing both emergency and continuous care. These barriers include explicit forms of social control, such as the introduction of anti–homelessness legislation and police–led sweeps, but also include regulatory bodies that approve or reject community solutions like naloxone programs. Despite the adoption of harm reduction policies by Vancouver and San Francisco, decentralized strategies (i.e., take home naloxone programs, overdose prevention sites, and safe consumption spaces) that best facilitate reversals often begin as unsanctioned efforts. Participants in each of the neighborhoods cite recent instances of mobilizing in the best interest of their communities, often circumventing current regulatory frameworks and municipal laws. This article disrupts the framing of opioid–related epidemics as temporary emergencies, arguing that truly effective and long–term overdose prevention must consider both urgent health needs and continuous urban displacement.
Addictive Streets? Public Health and the “Urban Crisis” of Drug Use
The history of harm reduction is entwined with narratives of urban crisis in the United States and Canada. Municipalities began introducing methadone maintenance programs as early as the 1960s, beginning with three New York City hospitals offering the treatment for opioid addicts (Courtwright 2001). With high rates of disease and increased fatalities affecting urban communities during the 1980s and 1990s, which researchers identify as one of the most significant decades for harm reduction advocacy, a shift began from purely punitive modes to discussions of addiction as a disease (Clarke 2016; Jozaghi 2014; McLean 2011; Roe 2005). NEPs were some of the most widespread harm reduction interventions due to a rise in the spread of HIV/AIDS and infection for both heroin and cocaine injection users. Evidence–based research during the 1990s and onward instead shows a significant drop in infection rates after the legalization of syringe access programs in many North American cities (Acker 2002; Clarke 2016; McLean 2011). Health departments were nonetheless concerned with misuse, or a “discourse of risk,” seeing “dangerous” behavior as a leading cause of the transmission of diseases and likelihood of overdose (McLean 2011:76). It is important to note that the increased involvement of public health authorities in drug–related epidemics did not deter drug crime convictions; as Gowan et al. (2012) illustrate, drug courts in the United States, emerging in 1989, incorporated mandatory treatment into the penal system. Over 1,600 courts operate in the United States, with over half of drug–related convictions being levied against Black men (Gowan et al. 2012). Gowan et al. (2012) highlight the prominence of rehabilitation centers in innercity neighborhoods, evidencing a shift toward “drug–treatment–as–crime–control” that targets specific populations of drug users (p. 71).
This brief summary of drug policy reveals two main patterns: (1) that states and municipalities at times acted independently of the federal of government by allowing specific programs and (2) that the criminalization of drug use is also associated with the criminalization of specific communities based on race and class. Bourgois’ (2003) comparative analysis of Canadian and American drug policy speaks to this overlap of control and treatment of drug users and what this means in terms of municipal governance. Bourgois (2003) states that while the blatant “carceral model” of the United States represents one kind of “policy world,” drug policy in Canada has also been subject to “neoliberal repression” that targeted the urban poor (p. 35). Bourgois (2003) describes how “opiate–based addiction” and crack use were “disproportionately concentrated on the blocks surrounding public housing, sex worker strolls, and on burnt out vacant lots” in both Canada and the United States (p. 32). The perception of urban (dis)order dominated policy decisions, leading to incoherent deliveries of support for “marginal, urbanized substance abusers” (Bourgois 2003:35). For example, Bourgois and Bruneau (2000) argue that there was a resistance by health authorities to understand the “cultural logics of street addicts” (p. 341). Reflecting on ethnographic work conducted in the center ville area of Montreal, they highlight how municipal and health authorities were overly concerned with operational issues, such as having syringes returned before they could issue new ones, rather than making services lower barrier.
The urban neighborhoods that Bourgois (2003) describes have been objects of investigation for both policy–makers and researchers with regard to drug use and poverty. Some researchers have taken more broad approaches to the city itself as a contested phenomenon, wherein “moral panics over the city” rewrite the actualities of urban life (Macek 2006:188). As Hall (1978) seminally argues, cultural concerns over “urban crime” in the 1970s (particularly the media's obsession with “mugging”) rendered certain spaces of the city as dangerous territories (p. 19). Drawing on case studies in Britain, Hall (1978) outlines the racialization of street crime and the hierarchization of urban decay, which portrayed “colonies” within cities as epicenters of deviant behavior (p. 305). The war on drugs of the late 80s was also a war on a dehumanized urban America, during which homelessness and/or drug use were seen as signs of social dissolution (Macek 2006). Smith (1996) argues that these anti–urban sentiments can be framed as a “revanchism of the city” or the retaliation against certain groups, spaces, and behaviors that were perceived as contributing to social ills (p. 207). Hall (1978), Smith (1996), and Macek (2006) present readings of the punitive cityscape.
Other urban sociologists are also concerned with the politics of the city but narrow their analysis to specific sites and how these areas become stigmatized. Wacquant's (2007) ideas regarding “advanced marginality” conjure images of bounded blocks within the city milieu, confined by the borders of the municipality (p. 67). Wacquant (2007) first suggests that there are marginalized groups that in fact have a strong collective identity; however, over time the “spatial redistribution” of production, resources, and capital have rendered these places as “spaces of mere survival” (pp. 69–72). Wacquant's (2009) states that “social insecurity” in the 1980s and 1990s drove the restructuring of the “urban order” (p. 303). State and municipal authorities have introduced “special measures” (be it orders to expel, surveil, etc.) to re–establish “urban order” (Wacquant 2007:69). Wacquant's (2007) more localized analysis of “dispossessed neighborhoods” and the severing of certain communities from the urban fabric stands in contrast with Hall (1978) and Smith's (1996) city–wide (and even state–level) discussions; however, each of these perspectives provides valuable insight into the ways in which meanings surrounding urban space are constructed (p. 66). What is gained from their discussions is an understanding of narratives surrounding urban crisis and “skid row” areas: the mythos of mugging, the construction of an anti–social underclass, and the assumed physical and moral decay of the postindustrial metropolis (Hall 1978; Smith 1996; Macek 2006).
There is a fictitious element to the “skid row district,” demonized as a magnet for the “crisis of street homelessness” and the birthing grounds for other forms of urban crime, including drug selling and consumption (Cloke et al. 2010:40/149). Drawing on Smith (1996), Cloke et al. (2010) argue that practices of urban renewal and gentrification go hand in hand with policing strategies; block–by–block, low–income inner–city neighborhoods are shrinking. Under the constant threat of cleansing or restructuring, these neighborhoods are also composed of a “constellation of social services” (McLean 2012:295). Syringe programs, safe injection sites, and other harm reduction tools have become part of the “institutional landscape” of certain neighborhoods, including Vancouver's DTES and the Tenderloin area in San Francisco (Mitchell and Heynen 2009:613). As McLean (2012) outlines, areas characterized by “booming drug sales and an entrenched homeless population” have been seen by some researchers as dumping grounds for services yet there is arguably nowhere else for these spaces to operate (p. 296).
Researchers point out that the experiences of clients of harm reduction and drug–related services are diverse and contextual (Faulkner–Gurstein 2017; Gowan et al. 2012; Jozaghi 2014). Gowan et al. (2012) acknowledge that certain harm reduction strategies are guided by neoliberal policies; however, they also note that spaces like syringe programs allow service users to develop a collective political goal (p. 1253). The drop–in space where they completed their fieldwork not only strengthened clients’ senses of entitlement to resources, such as clean syringes or local services, but also fostered solidarity among community members (Gowan et al. 2012). Faulkner–Gurstein's (2017) study similarly describes a sense of connection amidst clients of harm reduction agencies; her specific case speaks to the “social logic of naloxone” and a growing network in the Bronx of training programs for the overdose reversal tool (p. 20). According to Faulkner–Gurstein (2017), the decentralization of authority in local services has led to a rise in peer–administered solutions to overdoses. Jozaghi's (2014) study with the Vancouver Area Network of Drug Users highlights how one peer–led organization has brought substantial changes to the rhetoric surrounding the DTES in Vancouver and its residents, specifically injection drug users. One of Jozaghi's (2014) most substantial arguments is that out of their advocacy works arises possibilities for a “new DTES,” wherein the “practice of public drug use” is destigmatized and drug users have a recognized civic voice (p. 217).
Each of these studies make conclusions regarding harm reduction interventions, client and member experiences, and the city blocks that house services (Faulkner–Gurstein 2017; Gowan et al. 2012; Jozaghi 2014). In the context of recent spikes in overdoses and fatalities in North American cities, these neighborhoods are again at the forefront of conversations. Thinking back to the moral panics over the city, there is a similar language being employed to speak to the urban crisis of opioid overdoses (Hall 1978; Macek 2006; Smith 1996; Wacquant 2007). However, these neighborhoods are not static “skid rows”—nor have they ever been. These neighborhoods are also increasingly interconnected. The prevalence of opioid–related addiction in cities has made way for a greater overlap of ideas, policies, and approaches to the governance of urban health. McCann (2011b) argues that Canadian cities have long served as examples of “hot policy ideas,” suggesting that Vancouver is seen as a prime example of public health initiatives, influential to planners and city officials in cities such as Portland, Seattle, and San Francisco (p. 109). I would argue that certain cities in the United States, such as San Francisco, as also viewed as more progressive municipalities. The “mobilities” of urban policy has drastically changed the fields of power globally—drug policy decisions made at the municipal, state, or provincial levels are more likely than ever to be employed by “experts” in other contexts (McCann 2011b:124).
Research Sites and Methodology
McCann's (2011b) analysis provides an entry point to discuss the interurban exchange of harm reduction strategies and municipal approaches to drug use. As the participants will speak to, organizations and public health departments in Vancouver and San Francisco seem to borrow from each other in terms of mitigating risk. A comparative approach allows one to identify both the distinctions and overlaps of urban drug policy. Comparative research on cities has long been an approach favored by urban studies (Robinson 2014; Ward 2010). In this article, I have introduced some comparative research literature, namely, the works of Bourgois (2003) and Bourgois and Bruneau (2000), which employ ethnographic methods to better conceptualize discourses of addiction in the United States and Canada. Bollens (2007) describes comparative research as an approach that takes the “richness of the single case study” and extends it to urban policy and governance in multiple contexts (p. 3). Lees (2012) argues that comparative approaches—particularly from a postcolonial perspective—can actually identify the “relational” nature of urban knowledge (p. 166). Lees (2012) suggests that new comparisons among cities can reorient how researchers theorize about the urban. For the purposes of this article, I also draw on Hart (2004), who posits that the “sociospatial change[s]” happening in our world are diverse yet increasingly interwoven (p. 91). Hart's discussions of critical ethnography state that comparison is an investigation of the “processes of constitution and interconnection” (Hart 2004:98). In part, this article will answer Robinson's (2014) call for a “comparative imagination” with specific attention to drug–related epidemics, marginality, and urban theory (p. 10).
Though comparison can accommodate the similarities and differences of interurban dynamics, it has its limitations. For Ward (2010), the weaknesses of a comparative approach fall into the following categories: scale, territory, and causation. Comparison can often rely on an ontological understanding of the city as fixed—meaning that the city is viewed as having distinct “levels” that are interdependent (Ward 2010). There is a danger in treating comparative forms as separate, suggesting that the neighborhood is distinct from the metropolis or from the state and therefore ignoring relations across these dimensions (Ward 2010). Similarly, a second possible weakness is “methodological territorialism” that views all social relations as tied to place or bounded up in space (Ward 2010:479). I would add to this weakness by suggesting that comparative methods can also be very limited in their attunement to time, disconnected from the political and economic restructuring that is constantly at work in the urban context. By choosing two sites, I have minimized the time spent in each neighborhood, which may obstruct a more nuanced and intensive approach to the field. This limitation also extends to the rigor and depth of analysis that is possible when analyzing through a bifocal lens. Last, Ward (2010) argues that comparative work might be fixated on identifying “causal mechanisms” or rather, the shared patterns that might explain a phenomenon (p. 480). Ward (2010) provides a reframing of the relational approach that seeks to minimize these weaknesses. He argues that interurban studies should view the city as “open and constituted in and through relations that stretch across space” and understand that scale is “constructed and politicized” (Ward 2010:481).
What is most methodologically valuable about comparative research is its sensitivity to interurban forms of governance and the production of marginality. Building on the possibilities of relational comparison, San Francisco and Vancouver are positioned to “pose questions of one another” and look beyond what is mutually exclusive (Ward 2010:480). For decades, communities in both Vancouver and San Francisco have treated heroin and crack addiction, and mobilized to address the health implications of a predominantly unhoused and high–poverty user population (Davidson et al. 2003; Jozaghi 2014; Kerr et al. 2013; Visconti et al. 2015). These two sites were selected because of their legacies of urban health activism and commitment to low barrier interventions, which city officials have responded to by institutionalizing (to some degree) harm reduction policies. The DTES and the Tenderloin are also complex networks—major streets might distinguish the edges of the neighborhoods, but for residents and service users, the relationship between communities and urban space is not determined by what roads you cross. Conversations with local organizations and service providers elucidate local micro dynamics and the ways in which overdoses are governed from policing to federal legislation. Participants were asked how they (as community advocates, service providers, or peer workers) respond to overdose epidemics in their neighborhoods. Participants were invited to share their experiences during public health emergencies, discussing how they evaluate municipal responses to high–risk opioid use.
The qualitative dataset consists of 11 semi–structured interviews, all completed during a 4–month period. For Vancouver–based groups, five interviews were conducted with one individual speaking to their previous work experience in San Francisco. In San Francisco, six interviews were conducted. Interviews ranged from 45 minutes to 2 hours and initial participants were recruited via email, based on my working knowledge of harm reduction organizations in each of the cities. Subsequent participants and their organizations were recruited by word of mouth and all participants were randomly assigned pseudonyms. Interviews were transcribed and coded using a thematic framework that highlighted some of the key theoretical and pragmatic concerns regarding drug use, public health epidemics, and urban crises. These concerns included the operationalization of overdose strategies, the impact of state and/or municipal regulation on neighborhood resources and services, and the relational dimensions of marginalized communities and harm reduction policy formation. Initial coding identified symbolic and practical aspects of overdose tools (i.e., naloxone, safe injection sites, and overdose prevention sites). Interviews were analyzed to better understand how readily these tools have been made available to drug users and how spatial regulation in “progressive cities” has impeded rates of reversal. Analysis also involved the interpretation of the different meanings of epidemic and crisis as articulated by the participants.
I spoke with three types of organizations/service providers in each city, as categorized: (1) harm reduction–focused services, (2) anti–homelessness advocates, and (3) health departments and policy groups. First, groups focused on harm reduction include overdose prevention programs and syringe access programs, which have traditionally specialized in the distribution of syringes. These organizations are more involved in front–line or community–based work, operating drop–in spaces or mobile services. Second, the anti–homelessness advocacy groups are more directly involved in increasing access to shelters and social housing. For many of these groups, their work now includes educating on the use of and distribution of overdose reversal tools (i.e., naloxone). The third category includes health departments and drug policy groups that address the management of overdoses in urbanized neighborhoods, but also consider broader regional issues. The major commonality among these types of organizations is their involvement in overdose prevention and ongoing engagement with populations most at risk. These organizations either employed peer workers or liaised closely with drug user unions/alliances. In addition to interview data, site–specific participant observation was conducted in the aforementioned neighborhoods and community spaces. I attended one meeting in the Tenderloin in San Francisco, which was hosted by a local union to discuss safe consumption sites, and visited two drop–in spaces that provide safe injection facilities in Vancouver's DTES.
The participants’ efforts are concentrated in two main neighborhoods: Vancouver's DTES and San Francisco's Tenderloin. Table 1 identifies population demographics and neighborhood characteristics of each area, which have been selected to describe the average income, household composition, and housing types of the neighborhoods. I note that the qualitative interviews discussed in this article will include reference to other municipal areas, such as San Francisco's Mission and Bayview districts or Vancouver's neighboring municipality of Surrey; however, all of the qualitative interviews begin by focusing on the DTES and the Tenderloin. As evidenced in Table 1, these neighborhoods share similarities in terms of housing typology (single room or one bedroom rented apartments or hotels) and income characteristics. A large number of residents in both neighborhoods are living in poverty and these neighborhoods have the highest poverty rate in their respective cities. Demographically there is more diversity in terms of the ethnic make–up of the Tenderloin with the DTES having a greater proportion of Aboriginal residents. Some of these demographic differences, such as who is most impacted by poverty and addiction in these communities, will be addressed in the empirical analysis.
Population Demographics and Neighborhood Characteristics
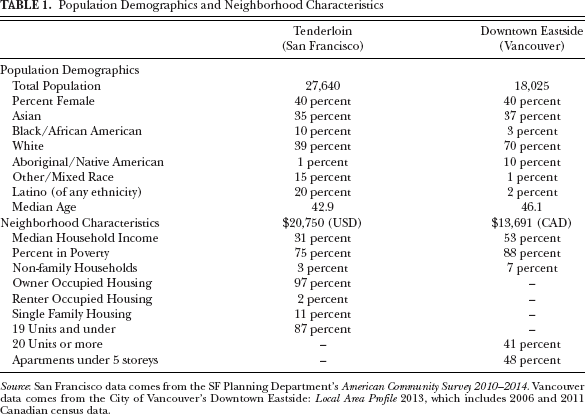
Source: San Francisco data comes from the SF Planning Department's American Community Survey 2010–2014. Vancouver data comes from the City of Vancouver's Downtown Eastside: Local Area Profile 2013, which includes 2006 and 2011 Canadian census data.
Naloxone in the Neighborhood: Practices of Overdose Prevention in San Francisco, Ca
The risk of overdose has always been a factor in opioid–related drug use (Faulkner–Gurstein 2017). Naloxone (the generic name) has become a staple in efforts to reverse opioid overdoses; the drug effectively blocks the effects of opioids, restoring breathing in those who have overdosed. Naloxone can be injected or administered intranasally and is effective against opioids, including highly toxic opioids such as fentanyl or long acting ones such as methadone. Naloxone (or Narcan in its branded form) has become one of the major tools to fight the recent overdose epidemics, though some organizations and municipalities have been using the drug for the last several years. Although naloxone has proven to be highly effective in most cases of overdose, temporarily alleviating the effects so that further medical attention can be sought, the road to distribution has been difficult for communities. Organizations in San Francisco and Vancouver have had to mobilize in creative ways, operating within or sometimes beyond the confines of the law. Since 2001, there has been one primary naloxone distribution program in San Francisco. Coordinated by one and half staff members, as Anna describes, the program services organizations across San Francisco:
What we do is coordinate with any program in San Francisco that is directly working with drug users that is not a medical establishment, right? We train their staff and their volunteers to be able to use naloxone. So we have about 150 trainers and 14 programs in the city that distribute naloxone. And so essentially if you are a drug user in San Francisco you can get naloxone about 400–500 hours of availability a month.
Anna states that there are five syringe programs in San Francisco with multiple sites—“a lot of coverage.” They serve as their primary distributors within several neighborhoods, the majority of that being within the Tenderloin and Mission areas. Anna compares their model of distribution to that of vaccines. Getting naloxone into the hands of every drug user is their paramount goal to “inoculate against death,” as she suggests. The ability to work in sheer volume (she estimates that they distribute about 10,000 kits per year) and to use the networks established by other organizations has streamlined their model, but this was not always the case. Though their program was the first naloxone program in the country to be funded by a health department, there was not a lot of legal precedent for the prescription and distribution of overdose reversal drugs; she clarifies that it was not the first naloxone program, just the first to be “backed” by a public health authority. In the early days, Anna describes deferring to medical and legal knowledge: because naloxone was not a controlled substance in theory, it could be prescribed to anyone at risk of overdose on opioids. However, under this “general prescribing law,” there were limitations regarding the intent to use naloxone on another individual. The “first wave” of regulations then they had to contend with was liability. The first model they relied on was utilizing the license of one doctor who ran a housing and urban health clinic in the Tenderloin; they were able to secure prescriptions of naloxone that would be distributed by nurse practitioners at select spaces (mainly syringe exchanges). The nurses would need to be present while the overdose prevention team trained local drug users; Anna estimates this was limited to 14 hours a month.
This model greatly hindered the accessibility of naloxone; in order to expand, they found another legal loophole that allowed them more mobility within the neighborhoods, greater time to spend with community members, and most importantly, eliminating the necessity for a medical professional's physical presence. Borrowing from her time spent working in Massachusetts where a “standing order model” had been used, Anna sought to replicate the issuance in California. Previously in Massachusetts, the distribution of naloxone required individual prescriptions. A standing order, a declaration signed and issued by a physician, acted as a kind of statewide prescription and under the order, pharmacists were legally allowed to provide rescue kits to any individual personally at risk of an overdose. In fact, the order also stipulated that all pharmacists in the state were required to stock naloxone. The Massachusetts order also extended to peer–to–peer administration and gave naloxone access to nonclinicians with no limitation on the quantity of kits that pharmacists could distribute. Anna approached a physician in California's public health department. “Is it legal?” she recalls him asking. “Eh, sorta.” Arguing that San Francisco was “lagging behind” and that the city's innovative reputation was at stake, they were able to convince the physician to issue the order. A trained employee of a naloxone program would collect and distribute the drug directly to service users and even those not directly at risk of overdose. It was not until 2010 that Anna says they could really start “decentralizing” under this model, training staff, and peers at other organizations.
Anna's description of the restrictions on naloxone distribution is reminiscent of some of the challenges that syringe programs faced when first introduced. As discussed, needles exchanges in San Francisco and Vancouver opened in the late 1980s; however, these programs initially operated under one–for–one regulations: a new syringe could only be given when the used one was returned. Municipal and public fears over excessive public drug use and the “dangers” of dirty needles informed these restrictive policies. San Francisco's major needle exchange lifted this policy in 1990, whereas Vancouver's NEP kept the policy until 2002 (Hyshka et al. 2012; San Francisco Aids Foundation 2017). Thinking back to the “policy world[s]” that Bourgois (2003) describes, it is interesting to consider how communities have learned to innovate under constant spatial and social control (p. 35). For advocates in San Francisco, mass distribution of naloxone has been the key to preventing overdoses and their unique model has entirely relied on what Anna calls the “helpful fiction” of the standing order. Their organization found a way around the “carceral model” that so viciously punishes poor drug users and instead, used the medical community to open up a channel (Bourgois 2003, p. 35). And once opened, it never closed. The standing order became official legislation in California in 2014, 13 years after the overdose prevention program was funded by the city of San Francisco. The freeing–up of ownership has had direct impacts for reducing fatalities; another participant (Karen) involved in a syringe access program in San Francisco corroborates that there were 877 reversals in 2016.
Anna describes some of the key changes that decentralization brought about, notably the opportunity to reach both public and private at–risk drug users. As Faulkner–Gurstein (2017) notes, naloxone as a harm reduction strategy relies on logics of decentralization, meaning that it is quick and easy to circulate. Decentralization also suggests a lack of hierarchy in terms of medical practitioners, giving anyone the opportunity to reverse an overdose. This vision has shaped the territories of overdose outreach in San Francisco, establishing a response that is collective, rapid, and routine for community members. Anna describes how some of the most impacted city blocks are now sites of reversals:
When we get outbreaks of overdoses from a strong batch of heroin or some fentanyl or something you will just literally see Narcan wrappers on the ground. It's crazy. The story has become in San Francisco…cause Civic Center and UN Plaza is really epicenter, right downtown. Overdoses happen there all the time. People will be like does anyone have Narcan? And like five people will run and have it.
The accessibility of naloxone also means that overdose responses are often contained to a small radius and informal chain of actors, circumventing traditional medical channels such as ambulances. As the overdose prevention manager at a syringe access program and harm reduction center, Karen's role involves initiating a response when there is a reported overdose. Karen describes the close–knit “corridor” that she calls 6th Street:
6th and Mission is our cross street and it is kinda literally right smack in the middle of one of the most impacted areas in the city…regarding homelessness, mental health and drug use. It always has been and most likely always will be because the SROs – the hotels – on that corridor are protected legally so in some respects as the city kind of changes drastically and very rapidly, 6th Street will always be 6th Street.
Increasingly, new residents are surrounding the intersection that Karen describes as demographics change due to gentrification in the area. These newcomers express NIMBY (“Not In My Backyard”) sensibilities, jeopardizing the future of their service. Karen states that their “brick and mortar location” is “smack in the middle” of the action on 6th Street and in close proximity to single room occupancy (SRO) hotels, which many of her clients live in. The small storefront is utilized in a variety of ways, serving as a local syringe program but also at times a community space, offering lounge hours. Drug users rely on the neighborhood “corridors” surrounding their storefront to share information regarding the strength of opioids and heightened risks. In a recent case, where crack turned out to be laced with fentanyl, one individual came running into their space from a nearby hotel to report the overdose. To Karen's knowledge, there have been about nine crack–related overdoses. Now that their drug of choice has the potential to be laced with synthetic opioids, this user population has been absorbed into the overdose prevention circle. Although the Department of Public Health needs to wait for the medical examiner to confirm cause of death, peer groups and harm reduction organizations generally trust the firsthand experiences of drug users. At the first word of an overdose, peers and syringe team members immediately “hit the pavement” to find anyone who might be smoking crack and let them know that their current supply might be laced with an unexpected substance.
Although the syringe team members and peer workers do much of their work beyond the physical location of the center, Karen notes that police still heavily control their space. A “memorandum” they have with the San Francisco Police Department means that members, clients, and visitors cannot hang outside their doors. Despite the agreement about the inside/outside use of space, Karen comments that police have nonetheless charged into the space during arrests or altercations with local residents and service users. The organization seems to exist within another layer of “advanced marginality” (Wacquant 2007:67). Wacquant's (2007) analysis of urban space focuses on public city blocks; Karen's comments highlight that for organizations supporting poor communities of drug users, their “private” spaces are vulnerable to the same punitive measures. Karen responds to this invasion of space by developing more connections with community members. She usually takes a walk around the block when she comes into work, collecting syringes but mainly saying hello to those that frequent 6th Street. Her own act of surveilling the neighborhood is not about policing drug users’ behaviors and instead, is more of a means to map of the rapid displacement of service spaces, SROs, and other forms of marginal housing. Karen's routine suggests that this dispossession, which Wacquant (2007) describes as being distinct to urbanized and impoverished neighborhoods, must be catalogued every day.
Another participant Rachel, who is involved in a coalition fighting homelessness, details some of the effects of Prop Q or the tent ban, which passed in November 2016 and banned the use of tents on sidewalks. The passing of this proposition now means that the city, namely, the Department of Public Works, can authorize the displacement of any individuals camping in San Francisco if they can offer them a shelter bed, disproportionately targeting the unhoused and marginally housed individuals. In most cases, participants state that the shelter beds being offered are only available for one night. Herring et al. (2019) suggest that legislation such as Prop Q and the issuance of citations actually contributes to more homelessness, failing to combat the perceived urban disorder. Anna suggests that another outcome of displacement amidst shrinking numbers of shelter beds is that “outdoor public drug use has exploded in the last couple years.” The increased visibility of drug use and national frenzies regarding opioid–related fatalities play into political and public concerns, replicating a moral panic over the city discussed by Macek (2006). Rachel argues that this fear can be used to justify more policing and has contributed to a “vitriolic response” by municipal and state law–makers toward both drug use and homelessness, often times conflating the issues.
One example Rachel provides is the passing of laws that sought to target “aggressive” panhandlers. There has been a steady increase in anti–homelessness laws in California over the last 10 years, in addition to a rise in “vagrancy” arrests (Policy Advocacy Clinic 2016). Rachel notes that community members have complained of being pressured into drug treatment by police regardless of whether or not addiction was a factor in their panhandling. In October 2017, the Law Enforcement Assisted Diversion program (LEAD SF) multi–agency initiative was launched (San Francisco Department of Public Health 2017). Funded by the Board of State and Community Corrections, this model seeks to “refer repeat, low–level drug offenders […] to community–based health and social services as an alternative to jail and prosecution” (San Francisco Department of Public Health 2017). As stated by the San Francisco Department of Public Health (2017), efforts will be concentrated in the Tenderloin and Mission districts. Similar to Gowan et al.'s (2012) discussion of rehabilitation centers in inner–city neighborhoods, these police–led tactics push “offenders” into drug treatment service or other programs as a means to clear the streets. However, anti–homelessness legislation and policing in San Francisco is actually “accelerating the circulation of bodies and camps around the city” (Herring et al. 2019:15).
As the city attempts to revamp San Francisco's downtown neighborhoods, organizations and peer workers are making moves toward introducing more permanent harm reduction resources. Participants felt that in spite of some of the more aggressive anti–homelessness and public drug use policies, timing could be right to establish safe consumption/injection sites. The concept of a safe consumption site (SCS) is not new in areas such as the Tenderloin. Karen notes that at their own space they have an “overdose response protocol for the bathroom.” They cannot legally condone the use of drugs in their space but it happens, she says, and in other hidden spots on the stretch of 6th Street. Part of their work is responding to overdoses that might occur in local establishments; Karen mentions they have a good relationship with a club a few doors down, as well as a sex shop that sometimes has to call in overdoses in the their peep show booths.
The unsanctioned operation of SCSs in San Francisco neighborhoods echoes the history of NEPs (McLean 2012). As McLean (2012) highlights, these grassroots and often “illegal” operations eventually become legitimized as “public health technologies” (p. 297). This push for legitimacy is underway in California. Mia works for a national drug policy organization and serves as the state director for policy. Her efforts in San Francisco are currently being largely directed at passing legislation that would allow SCSs to exist in the city. In June, the bill (AB 186) was passed by the California State Assembly and has gone on to the state Senate for review. I join Mia to attend a meeting at a local union, where she addresses several organizations based in the Tenderloin, including housing providers, an elementary school, and mental health services. We sit in a circle, in the back room of the union offices. Mia mentions to me, gesturing to the middle of the circle, that a few months ago in this same space they had built a mock–up of a safe consumption site for local residents and organizations to come check out—a room within a room to break down some of the panic over SCSs. Responses from attendees of the meeting are mainly concerned with the elimination of public drug use, equivocating street safety to the housing of illicit drug consumption. One on one, Mia shares some concerns with the city's perception that SCSs will solve the publicness of drug use. In her mind, it is about reducing harm and saving lives, though she is cautious about bringing another medicalized service into the Tenderloin “where everything gets dumped.” The actualities of what these spaces will look like, how they will operate, and where they will exist are yet to be determined. Mia drops keywords for an ideal SCS: accessible, welcoming, and culturally competent. Hoping to achieve a “geographic equity,” Mia mentions that mobile options are also a possibility.
Participants acknowledge that their rates of overdose are not nearly as high as other North American cities yet there is a heightened political interest in SCSs at the state level. Several participants argue that this is because more people are being affected by overdoses. As Anna states, “their constituents are dying.” She elaborates that white constituents are now dying. “Your constituents have always been dying,” she scoffs. Karen acknowledges that Bayview, “one of the last Black neighborhoods in San Francisco,” has been dealing with a crack epidemic for years; even though fentanyl is being found in this drug supply as well, she worries that this population will remain underserved and programs underfunded in the area. These conversations bring up important points regarding the concentration of services that other researchers have highlighted (McLean 2012; Mitchell and Heynen 2009). Overdose epidemics present an opportunity to think beyond the most obvious areas and toward other communities that might be at risk. Participants suggest that municipalities continue to associate these “crises” with a specific area and that there is a hesitance to provide outreach elsewhere in an effort to seemingly contain the problem. Rather than learning from the Tenderloin, the city seems pre–occupied in trying not to replicate its social characteristics by extending services too far beyond the “borders” of the neighborhood.
Harm reduction organizations and peer networks in San Francisco express hope that SCSs will normalize drug use, de–stigmatize injection, and noninjection drug users and minimize the criminalization of poverty. As Anna states, naloxone is a “solution to death,” but not the urban and social marginality that has existed in San Francisco for decades. The momentum behind SCSs can then be conceptualized as a kind of territory grab—a deepening of roots in areas that are being edged out by gentrification. In the world of overdose prevention and harm reduction strategies, organizations have to rely on what has come before and other urban contexts. Vancouver and particularly the legacy of InSite have inevitably come up during our interviews; it is an evidence–based success story that overdose programs and SCS advocates regularly call upon.
“The Pendulum Swung Too Far”: Spatial and Moral Regulation of Drug Use in Vancouver, Bc
Although San Francisco advocates seem optimistic about safe injection/consumption sites coming to their city in the near future, Vancouver has hosted one such site since 2003. Throughout the 1990s and into 2000, the DTES experienced what could be called an injection drug epidemic, with high rates of overdoses and fatalities (Jozaghi 2014). Local drug users and advocates had been talking about the possibility of operating a safe injection site (SIS) as early as 1997, borrowing from models in Germany and Europe. Opened initially as a pilot project called “Health Quest” in February 2003, Portland Hotel Society (PHS) initially operated the site without support from the municipal, provincial, or federal government. One participant (Greg) was deeply involved in its infancy having formerly worked at PHS. Because there were no other safe injection sites in the United States or Canada, there was no “roadmap” for introducing the space in Vancouver. The dream of the supervised injection site was built on both scientific expertise and activist knowledge. The PHS worked with the peer network Vancouver Area Network of Drug Users (VANDU), which Greg saw as the “radical aggressive arm” of the “mechanisms” at play to make the SIS a viable option.
By September 2003, the site was granted an exemption under the federal drug laws (Controlled Drugs and Substances Act) and gained support from the local health authority Vancouver Coastal Health, who would become a co–operator of the space (Boyd 2013). InSite was met with political attacks in 2006, with particular pressure coming from the federal government. The Portland Hotel Society and the VANDU would enter into a B.C. Supreme Court battle to keep InSite's doors open. The case would be heard in the Canadian Supreme Court in 2011, ruling in favor of InSite's plea to remain open, concluding that safe injection sites improved access to healthcare (Boyd 2013). Greg talks me through the legal and bureaucratic history of the space to highlight how the community was trying to create something “out of its time and space,” especially when public opinion was against such interventions. Now very much part of the “time and space” of the DTES, InSite has been in operation for 14 years.
If urbanized neighborhoods like the DTES are indeed “constellation[s] of social services,” then InSite is one of the most important nodes in Vancouver (McLean 2012:295). The space operates in part as a drop–in medical facility with nurses on staff and a team supervising clients when they access the injection booths, but it also offers counseling and mental health services. Located along the Hastings Street corridor, InSite's branded storefront gestures to its own global notoriety. In terms of overdose prevention, there has been approximately a 35 percent reduction in fatalities in the neighborhood since InSite opened (Marshall et al. 2011). Major reductions in syringe sharing and an increased likelihood of entering detox are some of the other contributions made by the SIS (Marshall et al. 2011). Although these results are substantial and encourage cities such as San Francisco to follow the “roadmap,” as McCann (2011b) argues, Greg challenges the idealization of Vancouver and Canada in the drug policy world:
Canada did what? A couple of things. They had a supervised injection site that was like a speck of sand. And they also had a heroin maintenance study, which is also like a speck of sand. The federal government and the city and state authorities, up until this crisis, hammered those things…tried to stop them. Harassed them politically. They've done everything that they could to stop those things. Now, at this moment in time, they have to embrace those things because what else have they got to offer? So too many people are dying. Canada in the harm reduction world is seen as like a leader, but we just made such a stink!
Greg states that the “fentanyl crisis didn't happen in one day.” Years of neglect in the DTES by city officials and other authorities have contributed to another wave of opioid–related overdoses and fatalities. “To some extent what has been created is a moral panic,” he argues; Greg suggests that the current overdose epidemic is convincing some of their harshest critics to now turn to the “old technologies,” such as SISs, which they had formerly challenged. Greg agrees that the spike in fatalities is changing the tide but is concerned that authorities are relying on strategies that fall within their limited understanding. Although tools like InSite are important, it is substantially more complicated than replicating one strategy or “speck of sand.”
Greg struggles with the idea of “harm reduction” when addressing the work of InSite and the future of overdose prevention; though it is a term he has had to rely on when advocating for InSite, he also feels it covers up some of the “real issues” facing the neighborhood, such as poverty, trauma, and hunger. Each of the participants in Vancouver says that overdose epidemics are shaped by institutionalized racism and classism surrounding drug use, which has had devastating effects on specific populations. Participants note that Aboriginal drug users have been some of the most neglected by service providers; although harm reduction strategies like SISs lessen health risks for drug users, they cannot address in full the systemic disparity. Greg reflects on claims by health authorities that the “pendulum has swung too far” in terms of the liberal prescription of opiates; however, he suggests that this is naive to the reality of illicit drug use. “There's always shit in drugs,” he says, stating bluntly that fentanyl is a “good” drug: strong. Participants suggest that the City of Vancouver and media have a fixation on fentanyl, and its supposedly miraculous appearance in heroin, crack, and other illicit drugs. Participants acknowledge that it is not a conversation about a single substance because the “epidemic” is much more complex than consumption habits.
Greg's comments mirror a similar disconnect that Bourgois and Bruneau (2000) identify between city officials and drug users. Though Vancouver presents a “progressive” approach to public health, municipal–led strategies continue to treat addiction in the DTES as a curable phenomenon or the choice of the individual. This is most evident in the privileging of spatial and medical regulation of drug use in Vancouver. Participants note how city and provincial authorities have insisted on the presence of medical professionals in SISs, funded shelters that do not allow drug use, and positioned an increase in treatment beds as a solution to the crisis. One participant prefers to use the term “respite” for the treatment they offer at InSite, suggesting that treatment on demand programs do not necessarily lead to clients exiting the street, but letting people have a bed and a break is just as important. These forms of regulation and surveillance can often make basic necessities, such as healthcare or shelter, higher barrier. In some ways, the DTES that participants describe comes off as a bureaucratic tangle that is intensively regulated. The image of service–heavy neighborhoods has also been suggested in the literature (Mitchell and Heynen 2009; McLean 2012). Participants contested whether or not Vancouver is representative of this to various degrees; however, many spoke on one example: the availability of naloxone or rather, the restrictions on its distribution and route of administration.
Naloxone became an official strategy in Vancouver and throughout the province of British Columbia beginning in August 2012. The take–home naloxone program, which now does the majority of distributions, is overseen by the BC Centre for Disease Control (BCCDC). Sarah works with the major health authority for Vancouver, though she previously lived in San Francisco. Trained as a nurse, she was closely involved in the roll out of naloxone distribution in San Francisco. Coming to back to Vancouver in 2013, she notes that it was right at the beginning of the community naloxone distribution program in BC—10 years after San Francisco's own program began. At the time, “lay staff” in San Francisco could also train on the use of naloxone, while Vancouver was “nurse driven.” Working at InSite after her return, Sarah got involved in naloxone education and revising policy for housing providers on overdose prevention strategies. Sarah notes that several other shelter or housing organizations were involved in the take–home naloxone program. Their strategies include adapting the spatial and operational “manual” of InSite for other organizations. Sarah notes that housing providers are adopting spaces like safe injection rooms—or at least they can now talk openly about the existence of such spaces.
In April 2016, the provincial health officer declared a public health emergency in response to the rise of drug–related overdoses and deaths. Factors influencing the declaration included the prevalence of fentanyl (60 percent of all overdoses were fentanyl–related in 2016) and high rates of death, which surpassed numbers from 1997 to 1998 during which a public health emergency was also declared in BC (BC Centre for Disease Control 2017). Sarah says this declaration broke down some walls and made room for more “innovation” in a city that assumed it had all the tools in place. In terms of what the emergency declaration means for the DTES, there is shift away from the centralized SIS model and toward overdose prevention sites. Popping up throughout the neighborhood—a portable building on a vacant lot or a modified room in a hotel/SRO—these spaces allow users to inject but without the supervision of medical professionals. Overdose prevention sites rely mainly on peers to respond if an overdose occurs. In March 2016, naloxone was removed from the Drug Schedules Regulation by Health Canada, making the injectable form of naloxone available without prescription (Government of Canada 2016). This change has dramatic effects on the take–home naloxone program. The BC Centre for Disease Control reports that in 2017, they distributed 61,787 kits: a significant increase from the 618 kits that were distributed in 2013 (BC Centre for Disease Control 2018). Several participants highlight that Health Canada's regulatory barriers continued to limit the supply of intranasal naloxone—the more costly but easier to administer option—until October 2016 (House of Commons of Canada 2016).
Generally participants felt the roll out of overdose solutions was stagnated due to tools having to be first approved by BCCDC or Health Canada, as well as budget limitations that made only certain kinds of interventions and neighborhoods a priority. A few participants noted that they did have an off–brand supply of intranasal naloxone at InSite and other spaces in the DTES prior to it being de–listed. Alex, who now works in the DTES with a large anti–homelessness organization, said he was very surprised when he moved to Vancouver in 2014. At his former organization based in the municipality of Surrey, a neighboring municipality of Vancouver, they had been distributing injectable naloxone via their own “ad hoc” take–home program as early as 2012. Surrey had been experiencing a growth in drug use, both injection and inhalation, particularly on and around 135A Street. Operating under a different health authority, Fraser Health, they initiated the program with very little support from the authority directly; nonetheless the organization saw over 200 reversals in that first year. Coming to the DTES, Alex entered a new network of services, where he saw people navigating the “system” pretty well. In a city with a high rate of fatalities, several participants spoke of the neighborhood as a safety net or a system that has to constantly evolve in order to save lives. But even amidst one of the most serviced urban areas in North America, there is stigma against drug users, Alex says:
Particularly around the opioid epidemic, is how do we make it safe for them to share that I am going to go to my room and use, right? Folks are dying alone in their rooms in this province. In the Downtown Eastside.
Although the declaration of a public health emergency has allowed for the reigns of medical regulation to be loosened in terms of distributing naloxone or opening overdose prevention sites, alleviating the negative and often patronizing responses to injection (and non–injection) drug use is a different problem:
Interviewer: What do you feel has been one of the biggest asks – especially in terms of the increase of overdoses and fatalities – from community members?
Sarah: It is regulation and legalization. We have to do both. If it just within a regulation framework then it is just people going to their doctor.
Legalization would demand a reorientation of the relationship between health authorities and service users. As McLean (2011) states, municipalities tend to focus on the “biomedical needs” of drug users or rather solutions that can be overseen by clinical services (p. 301). This political interest in maintaining control over vulnerable populations is contrasted by the vision shared by local drug users and veteran community workers. Sarah does not reject regulation all together and suggests that it has its place in the DTES neighborhood. Prescription opioids (or heroin–assisted treatments) are another potential intervention; particularly crushable opioids such as oxycodone, which might steer users away from heroin or fentanyl that carry a higher risk of overdose due to their potency. Sarah is wary nonetheless of “policy windows closing,” suggesting that the recent spike in overdoses does not guarantee that all the pieces will be in place for legalization. An “epidemic” or “crisis” seems to suggest a temporary state, but the current emergency did not begin when provincial authorities announced it; for example, Alex's organization in Surrey was dealing with overdoses and fatalities several years before the emergency declaration in 2016. Each of the Vancouver participants acknowledged that epidemic is an appropriate term to use, but also argue that it must be understood successively. Participants reiterate the history of the DTES, not to play into skid row abstractions, but to accentuate how deep the trauma has been for the community. Alex states that “we haven't begun to scratch the surface” of what epidemic means in terms of the “sheer volume of friends that we have lost,” in recent months and in years previous.
Discussion: Space, Survival, and the Future of Urban Drug Policy
The increase in opioid–related overdoses across North America is difficult to detach from the localized knowledge of urban neighborhoods. It has been my effort in this article to work across urban communities, tracing historical and institutional conceptualizations of illicit drug use to the practices and strategies of individuals in Vancouver and San Francisco. As Roe (2005) outlines, harm reduction organizations, which are now mainly responsible for overdose prevention in these urban contexts, were founded on early histories of “unlikely coalition[s] of public health authorities and activists” (p. 244). What has grown out of grassroots, bottom–up interventions are complex networks of service providers (Roe 2005). This article surveys harm reduction studies that speak to both the social and spatial characteristics of these neighborhoods (Faulkner–Gurstein 2017; Gowan et al. 2012; Jozaghi 2014; McCann 2011a; McLean 2012). Participants provide insights into how harm reduction models are strained due to the rise of overdoses. I employ semi–structured qualitative interviewing and participant observation to ground these discussions in the experiences of those working directly in overdose prevention, contextualizing two cities generally perceived as the progressive branches of urban governance. Although participants were able to speak to broad issues, I situated our conversations in specific neighborhoods: Vancouver's DTES and San Francisco's Tenderloin.
In the empirical analysis, two interconnected themes emerge: (1) the legacy of distrust between municipal officials and drug users and how this informs urban control and (2) the disconnection between “epidemics” as narrowly constructed public health emergencies and the long–term, complex needs of communities. As discussed, the first theme is well evidenced in the literature; however, it is important to re–emphasize stigma when exploring contemporary public health crises. The case of Vancouver is a distinctive example of distrust, echoed in Bourgois and Bruneau's (2000) analysis of municipal rejection of the “cultural logics of street addicts” (p. 341). The lag in approving naloxone emphasizes the reliance of the Canadian state on official approval rather than front–line expertise. Similarly, the increase in police presence in the Tenderloin re–inscribes the street as deviant spaces and residents as criminals. For example, one participant's account of the politics of a doorway—a syringe exchange near 6th and Mission—shows how organizations must constantly renegotiate their right to exist with police and other municipal authorities. Although “special measures” like policing or drug regulation are historically part of San Francisco and Vancouver's wars on drugs, this article highlights how these tactics are prioritized during epidemics, often in opposition to evidence–based approaches (Wacquant 2007:69).
These observations also lend themselves to the second theme: the systemic belief that an epidemic can be singularly eradicated by a medical response. I argue that this is the one of the most significant contributions of this study—peer workers and advocates do not view epidemics as data points that are reduced to a singular moment or location. The increased risk of drug–related overdose or death is the culmination of social disregard and spatial disenfranchisement that has long affected these communities. Therefore, emergency measures are only the first step; long–term support must be holistic and multifaceted, led by those that still exist in the margins. Municipal responses are eager to fund emergency efforts and interventions, but in certain cases these put greater pressure on harm reduction organizations and drug user unions/alliances. In some instances, city officials develop interventions that undermine the successes of low barrier services, such as increasing police presence. The physical displacement under the Tenderloin's tent ban causes disruption as the City of Vancouver's stronghold on naloxone, which attempts to funnel at–risk drug users to closed–door spaces like InSite.
The findings suggest that effective overdose prevention is ultimately a struggle against conflicting imaginaries of a progressive city. Neighborhoods, such as the DTES and the Tenderloin, associated with skid row narratives generally share the same social and spatial characteristics: these areas are close to the downtown centers of large cities, the population is unhoused or marginally housed, and there is a significant amount of public inhalation and intravenous drug use (Cloke et al. 2010). With the advent of harm reduction strategies, these neighborhoods have undergone a kind of transformation, developing networks that provide various services to drug users (Faulkner–Gurstein 2017; Gowan et al. 2012; Jozaghi 2014; McLean 2012). Many of these services have reduced some of the risks associated with poverty and addiction, thanks largely to the involvement of peer workers and drug users themselves (Faulkner–Gurstein 2017; Jozaghi 2014; McLean 2012). As participants highlight, San Francisco and Vancouver exist in more forward–thinking municipal bubbles, giving the impression that there is a stronger safety net for vulnerable groups during overdose epidemics. However, the rise of overdoses in San Francisco, Vancouver, and many other North American cities has shifted the rules of the street, demanding more accessible and novel strategies to fight the risk of death. Despite the institutionalization of certain harm reduction policies, organizations have resorted to unsanctioned means, such as stocking off–brand naloxone and operating safe consumption rooms (in cities where SISs are still illegal).
This article argues that overdose epidemics can challenge how researchers perceive seemingly well–serviced areas and the formation of harm reduction policy. Although the DTES and the Tenderloin are comparable in many ways, one of most acute differences that this article identifies is their success rate in reducing overdoses. Participants in San Francisco state that they have drastically reduced overdoses. Comparatively, Vancouver participants see the numbers of fatalities growing each day. This finding disrupts assumptions about the efficacy of certain harm reduction tools. Despite Vancouver's reputation as a leader in harm reduction, marked by its early introduction of safe injection sites, it did not have a provincially mandated naloxone program until 2012 (Bourgois 2003). Participants claim that the roll–out of a naloxone distribution program in the neighborhood was complicated by the medical and legal bureaucracy of the province, resulting in unsanctioned pathways to distribute the life–saving drug. Navigating the legal grey zones of doctor licenses and standing orders, advocates in the Tenderloin were able to introduce a comprehensive naloxone distribution program. This decentralized approach flooded the Tenderloin and the adjacent Mission with the life–saving drug—reversals are now incredibly commonplace.
The tensions between community solutions and municipal responses have created unique landscapes of overdose prevention in the DTES and the Tenderloin. With the passing of time, the cities are traversing the same paths, introducing tools that another community might have had years before them such as SIS/SCSs or overdose prevention sites. Participants are hopeful that the recent opioid–related epidemics could finally be enough to revolutionize the relationship between municipal authorities and harm reduction organizations suggesting that their years of operating on the edges of the law or experimenting with rogue distribution programs might be behind them. As Ward (2010) writes, cities like Vancouver and San Francisco are continually “implicated in each other's past, present, and future” (p. 480). In order to address the future of drug policy and public health, this article welcomes research that interrogates local and global forms of governance. This research should also address “progressive cities,” which appear to already have the resources to mitigate drug–related epidemics. I would argue that these municipalities have the greatest reach to qualify (or disqualify) the rights of drug users. By conceptualizing overdose epidemics as sociospatial fields of power, research can prioritize the experiences of the urban poor and imagine life beyond survival.
Footnotes
Acknowledgements
The author would like to acknowledge the tireless efforts of peer workers and front–line organizers in Vancouver and San Francisco. The author would also like to thank David Madden and Suzi Hall, who each in their own way taught her to trust in the work. Last, the author would like to thank the anonymous reviewers whose feedback was integral to improving the manuscript.