
Abstract
Background
Aortic stiffness is an independent predictor of coronary events.
Aims
We assessed the predictive value of aortic stiffness for ⩾50% asymptomatic coronary artery disease in a stroke/transient ischemic attack population.
Methods
We enrolled 300 consecutive patients aged 45–75 years with nondisabling, noncardioembolic ischemic stroke or transient ischemic attack, and no prior history of coronary artery disease. Coronary artery disease was assessed with 64-section computed tomography coronary angiography and all patients had a detailed cervicocephalic arterial work-up. Aortic stiffness was determined from carotid-femoral pulse wave velocity with 9·6 m/s as cutoff value. The predictive value of aortic stiffness was assessed by logistic regression and reclassification tables method after adjustment for the Framingham Risk Score and the presence of cervicocephalic stenosis, which were previously shown to be independent predictor of ⩾50% asymptomatic coronary artery disease.
Results
Among the 274 included patients who had computed tomography coronary angiography, 26% (95% CI, 21%–32%) had an increased stiffness (pulse wave velocity > 9·6 m/s) and 18% (14%–23%) had ⩾50% asymptomatic coronary artery disease. Increased aortic stiffness was associated with the presence of ⩾50% asymptomatic coronary artery disease, both in univariate (odds ratio = 3·4 [1·8–6·4]) and multivariate analyses (odds ratio = 2·3 [1·2–4·7]) after adjustment for Framingham Risk Score and presence of cervicocephalic stenosis. After carotid-femoral pulse wave velocity was added to the standard model including Framingham Risk Score and the presence of cervicocephalic stenosis, net reclassification improvement was 12·6% (P < 0·005), integrated discrimination index was 2·51% (P = 0·025), and model fit was improved (likelihood ratio = 4·99, P = 0·025).
Conclusions
In stroke/transient ischemic attack patients, aortic pulse wave velocity improves the prediction of ⩾50% asymptomatic coronary artery disease beyond classical risk factors.
Introduction
Coronary artery disease (CAD) is a significant cause of morbidity and mortality in patients who had a stroke or a transient ischemic attack (TIA) (1). Although recurrent strokes occur more commonly than cardiac events over the long term after stroke, cardiac events still account for a greater proportionate mortality (2–4). In order to improve the prevention of CAD in stroke patients, it could be relevant to identify those patients with asymptomatic coronary artery stenosis who might benefit from specific additional therapeutic measures to prevent a first-ever coronary event. We previously showed in a stroke/TIA population that in addition to traditional vascular risk factors, the severity of cervicocephalic artery stenosis was strongly associated with ⩾50% asymptomatic CAD [as detected by computed tomography (CT) coronary angiography] (5). However, other potential predictive factors should be assessed to refine the identification of stroke patients with high risk of asymptomatic CAD. Several studies have demonstrated that carotid-femoral pulse wave velocity (PWV), a direct measure of stiffness of the thoracic and abdominal aorta, is associated with higher cardiovascular disease event rates in high-risk (6–9) and community-based samples (10–13). By contrast, there are no data on predictive value of carotid-femoral PWV for CAD in patients with stroke or TIA.
Aim
We therefore assessed the predictive value of aortic stiffness for ⩾50% asymptomatic CAD in a stroke/TIA population.
Methods
The study was conducted prospectively in consecutive patients admitted to our stroke unit from January 2006 to February 2009. The methods of the study have been previously reported (5). Patients were eligible if they were 45 to 75 years of age; had had an ischemic stroke (confirmed by brain imaging) regardless of the duration of symptoms (14) or a probable TIA according to the National Institute of Neurological Disorders and Stroke criteria (15) resulting from large-artery atherosclerosis, small-vessel disease, or an undetermined cause according to the Trial of Org 10172 in Acute Stroke Treatment classification (16); and had no prior history of CAD. Patients with disabling stroke (modified Rankin scale score ⩾3), cardioembolic stroke, contraindications to multislice CT (MSCT) coronary angiography, or life expectancy of <3 years were not eligible. The study was approved by the local ethics committee, and all patients provided informed consent. During the study period, among 368 eligible patients, 300 were included and 274 had MSCT and arterial stiffness measurement (5).
Demographic data, previously known vascular risk factors, and cardiovascular medical history were collected prospectively by an investigator during a face-to-face interview using a specific case report form (5). All patients had brain magnetic resonance imaging with spin-echo diffusion-weighted imaging (n = 271, 99%) or CT scan, a standardized causal workup that included standard blood tests, 12-lead ECG, prolonged 3-lead cardiac monitoring, arterial investigations, and echocardiography (transthoracic in all and transesophageal in 264 patients, 96%). Imaging of cervical and intracranial arteries consisted of cervical and transcranial Doppler ultrasound in all patients and 3-dimensional time-of-flight magnetic resonance angiography of the circle of Willis in 271 patients (99%), cervical gadolinium-enhanced magnetic resonance angiography in 263 patients (96%), 64-section CT angiography in 12 patients (4%), and conventional angiography in 8 patients (3%). CT angiography and conventional angiography were done in case of contraindication to magnetic resonance angiography or discrepancies between Doppler ultrasound and magnetic resonance angiography. Cervicocephalic atherosclerosis was assessed with a standardized method (5). An investigator blinded to clinical data and results of the MSCT coronary angiography reviewed all available arterial investigations and assessed each arterial segment for the presence of cervicocephalic atherosclerosis. Each arterial segment was classified as normal, <50% stenosis, or ⩾50% stenosis. The presence of atherosclerosis was defined by at least one stenosis in at least one of the following arterial segments: common carotid artery, carotid bifurcation, cervical internal carotid artery, intracranial internal carotid artery, segments of the vertebral artery (ostium, prevertebral, transversarial, atlas loop, intracranial), segments of the basilar artery (proximal, middle, distal), proximal segment of the posterior cerebral artery, or proximal segment of the middle cerebral artery.
Carotid-femoral PWV measurement
At inclusion, systolic and diastolic brachial blood pressures (BPs) were measured after a 10-min rest period in a supine position by using a semiautomatic BP device. Pressure was measured three times, and the mean of the last two measurements was calculated.
After BP was measured, carotid-femoral PWV was determined with an automatic device, the Complior SP (Colson, France). Briefly, waveforms were obtained transcutaneously over the right common carotid and femoral arteries, and the time delay (t) was measured between the feet of the two waveforms. The distance (D) covered by the waves was assimilated to the distance measured between over the body surface between the recording sites (17). Carotid-femoral PWV was calculated as PWV = 0·80 × D (meters)/t (seconds) as recently proposed (18). A cutoff value of 9·6 m/s (i.e. 12 m/s for direct measure) was used for PWV according to European guidelines (18,19). The median time from stroke or TIA onset to inclusion with BP and carotid-femoral PWV measurement was eight-days.
MSCT coronary angiography
We performed 64-section CT examinations of coronary arteries using a technique that we reported elsewhere (5,20). In that study conducted in patients at high risk for CAD (20), MSCT coronary angiography had a sensitivity of 100% and a specificity of 89% (compared with conventional coronary angiography) for detecting patients with ⩾50% CAD. All MSCT coronary angiographies were reviewed by a single experienced radiologist blinded to clinical data. Arterial segments that were ⩾1·5 mm were analyzed. The degree of stenosis was quantified on orthogonal views with automatic vessel analysis tool (21). The degree of stenosis was measured only if the visually observed degree of stenosis was ⩾30%. The percentage of stenosis was evaluated as a diameter percentage. Patients were categorized as no CAD (no plaque), <50% CAD (at least one lesion <50% and no stenosis ⩾50%), and ⩾50% CAD (at least one stenosis ⩾50%).
Statistical analysis
The Framingham Risk Score (FRS) (22) was calculated for each patient, and standard cutoffs [<10%, 10% to 19%, and ⩾20% 10-year risk of coronary heart disease (CHD)] were used (23). Values of carotid-femoral PWV in patients with or without ⩾50% asymptomatic CAD were compared by analysis of covariance, adjusted for major covariates [age, sex, pulse pressure, and low-density lipoprotein (LDL) cholesterol]. The relationships between ⩾50% CAD and patient characteristics were assessed by calculation of crude and adjusted odds ratios (ORs) through logistic regression models.
We previously showed that the prevalence of ⩾50% asymptomatic CAD was 18% (95% CI, 14 to 23; n = 50) in this stroke/TIA population and independently associated with traditional risk factors assessed individually or through the FRS and the presence of at least 1 ⩾ 50% cervicocephalic artery stenosis. The prevalence of ⩾50% asymptomatic CAD increased gradually with FRS level and with the presence of stenosis of cervicocephalic stenosis (5).
To assess the additional predictive value of carotid-femoral PWV for CAD, we built two separate multivariate logistic models. The first model included traditional risk factors assessed through the FRS and the presence of cervicocephalic stenosis. The second model took into account carotid-femoral PWV using 9·6 m/s as cutoff value in addition to variables included in the first model. Interactions of carotid-femoral PWV with FRS and carotid-femoral PWV with the presence of cervicocephalic atherosclerosis were tested. The Hosmer–Lemeshow test was used to assess calibration of multivariate models. The comparison of predictive values of the models was assessed by using the likelihood ratio test and by comparing the C statistics [which is analogous to the area under the receiver operating characteristic (ROC) curve]. Finally, we computed the net reclassification improvement and the integrated discrimination improvement (24). The cutoff values used for the reclassification analysis were: 0 to 9%, 10 to 19%, 20 to 29%, 30 to 39%, and 40% and more.
Results
Mean age was 62·5 years (SD, 8·0 years), and 192 patients (70%) were male. Two hundred thirty-five patients (86%) had ischemic stroke, and 39 (14%) had TIA. Carotid territory was involved in 180 patients (66%); vertebrobasilar territory in 94 (34%). Mean carotid-femoral PWV (SD) was 8·7 (2·0) m/s and median (interquartile range) carotid-femoral PWV was 8·5 (7·4–9·8). Among the 274 patients, 72 (26%) had a carotid-femoral PWV > 9·6 m/s.
Compared with patients who did not have ⩾50% asymptomatic CAD, those who had ⩾50% CAD had a higher carotid-femoral PWV (9·6 versus 8·6 m/s, respectively; P < 0·0001). This difference remained significant after adjustment for sex, age, pulse pressure, and LDL cholesterol (P < 0·0001). Patients with ⩾50% asymptomatic CAD were more likely to have carotid-femoral PWV > 9·6 m/s than those without ⩾50% asymptomatic CAD (crude OR = 3·4, 95% CI: 1·8–6·4). Adjustment for delay from stroke onset to carotid-femoral PWV measurement and pulse pressure did not change the relation (data not shown).
Table 1 shows that FRS and the presence of cervicocephalic stenosis were strongly associated with the presence of ⩾50% asymptomatic CAD (Model 1). The OR was 4·9 (1·8–13·3) for patients with at least one ⩾50% stenosis of cervicocephalic arteries and increased from 2·9 (1·1–7·3) in patients with a 10–19% FRS-predicted 10-year risk of CHD to 7·6 (3·0–19·3) in those with a ⩾20% FRS-predicted 10-year risk of CHD. Table 2 shows that carotid-femoral PWV was also an independent predictive factor of ⩾50% asymptomatic CAD, OR = 2·3 (95% CI: 1·2–4·7) (Model 2). There was no interaction between carotid-femoral PWV and FRS (P = 0·925) and between carotid-femoral PWV and the presence of cervicocephalic stenosis (P = 0·948). The Hosmer–Lemeshow test demonstrated excellent calibration of the two models (χ2 = 1·26, P = 0·98 for Model 1 and χ2 = 1·54, P = 0·99 for Model 2). The model fit was improved when carotid-femoral PWV was added to Model 1, as by reduction in log likelihood (likelihood ratio = 4·99, P = 0·025). The increase in C statistics was not statically significant [Model 1, c stat = 0·77 (0·70–0·74); Model 2, C stat = 0·79 (0·72–0·84)]. The addition of carotid-femoral PWV to model 1 resulted in an upward reclassification of 34% of patients who had ⩾50% asymptomatic CAD (Table 3a), as well as an upward reclassification of 17% of patients who did not have ⩾50% asymptomatic CAD (Table 3b), yielding an overall net reclassification improvement of 12·6% (P < 0·05). The net reclassification improvement was 14·4% (P < 0·05) when three categories of predicted risk were used in the reclassification tables (<20%, 20 to 39%, ⩾40%). The addition of carotid-femoral PWV to Model 1 also led to a significant integrated discrimination improvement of 2·51% (P = 0·025).
First multivariate model – relationship between FRS, severity of cervicocephalic atherosclerosis, and ⩾50% asymptomatic CAD
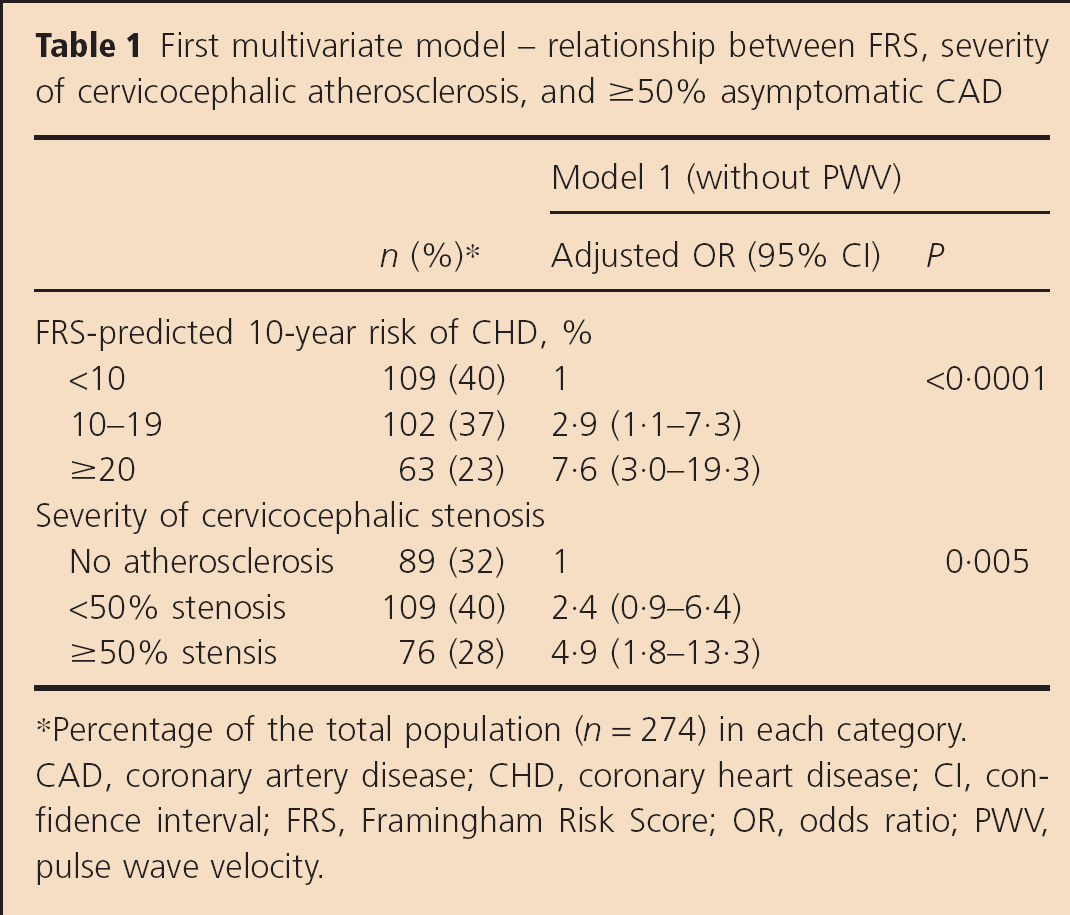
Percentage of the total population (n = 274) in each category. CAD, coronary artery disease; CHD, coronary heart disease; CI, confidence interval; FRS, Framingham Risk Score; OR, odds ratio; PWV, pulse wave velocity.
Second multivariate model – relationship between FRS, severity of cervicocephalic atherosclerosis, carotid-femoral pulse wave velocity, and ⩾50% asymptomatic CAD
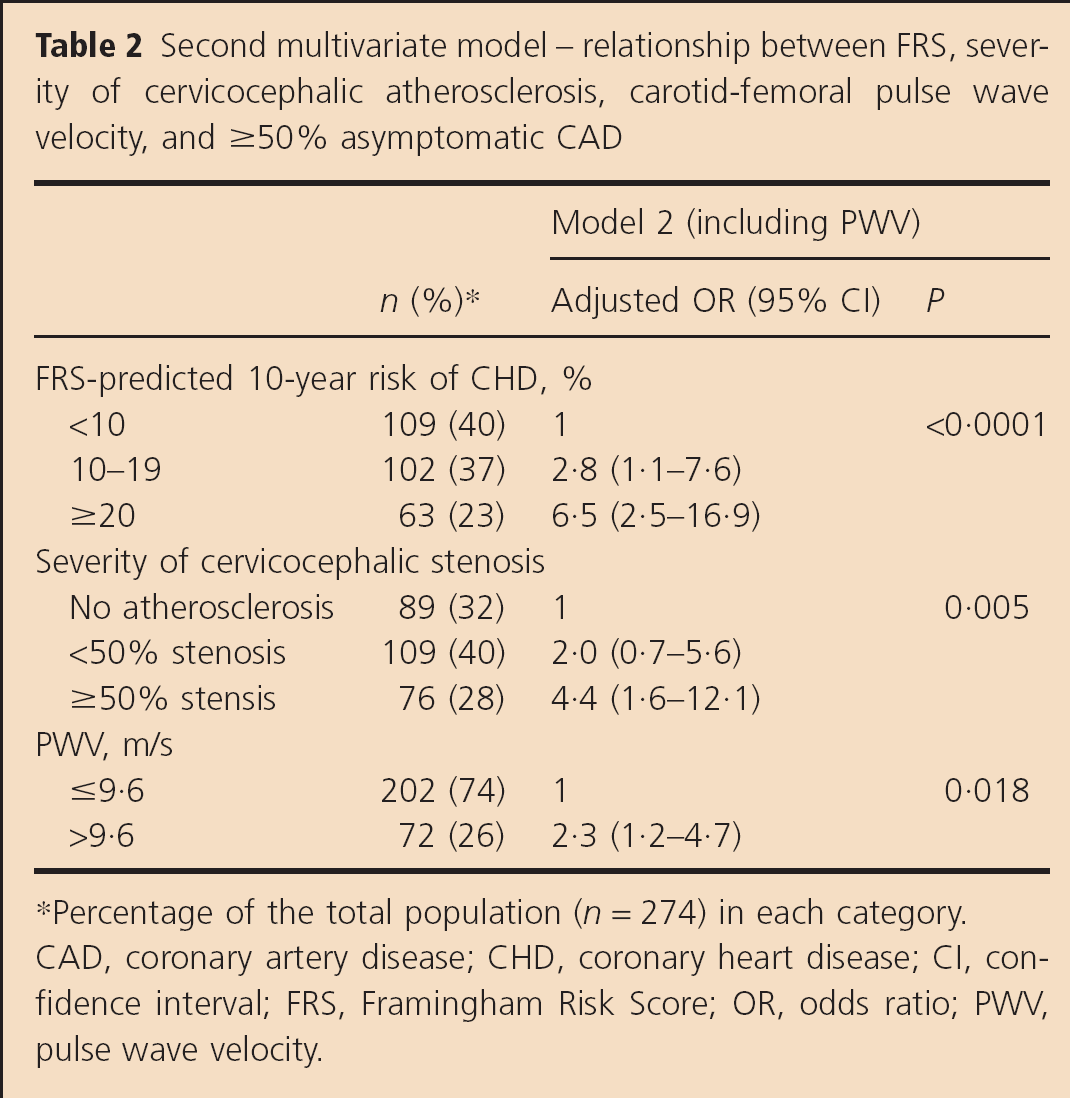
Percentage of the total population (n = 274) in each category. CAD, coronary artery disease; CHD, coronary heart disease; CI, confidence interval; FRS, Framingham Risk Score; OR, odds ratio; PWV, pulse wave velocity.
Reclassification tables – predicted risk for the presence of ⩾50% asymptomatic CAD before and after reclassification with PWV in patients with and without asymptomatic CAD
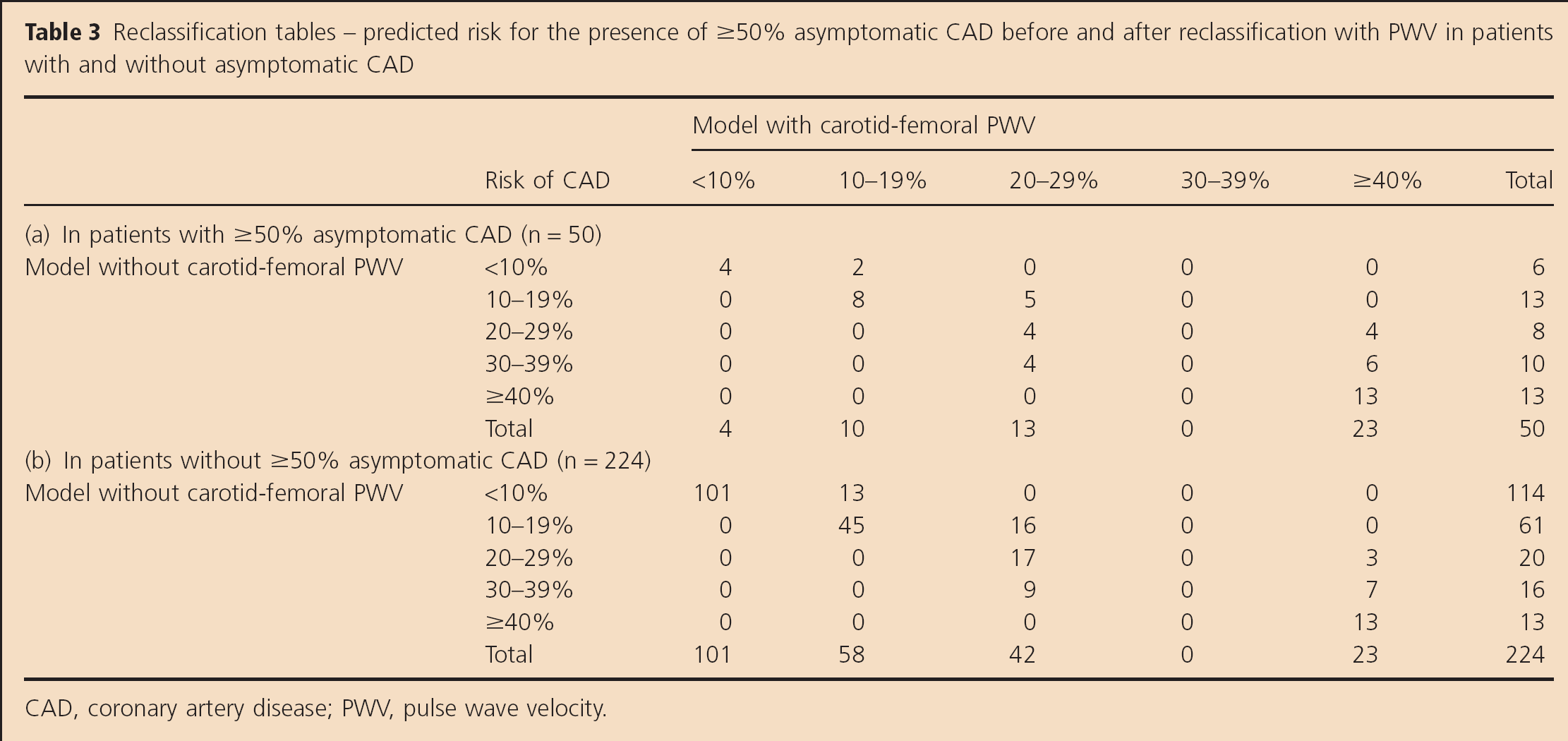
CAD, coronary artery disease; PWV, pulse wave velocity.
Discussion
This study shows that measurement of carotid-femoral PWV improves the prediction of ⩾50% asymptomatic CAD provided by the FRS and the presence of cervicocephalic stenosis in patients aged 45–75 years with nondisabling, noncardioembolic ischemic stroke or TIA.
Aortic stiffness and cardiovascular risk
In recent years, there has been growing interest in the assessment of arterial stiffness and its role in the evaluation of an individual's total cardiovascular risk (18,25). Carotid-femoral PWV is a direct measure of aortic stiffness, which can be measured in a sufficiently simple and accurate way to be used as a diagnostic test for assessment of target organ damage (26). Several studies have shown that carotid-femoral PWV is associated with higher cardiovascular disease event rates in high-risk (6–9) and community-based samples (10–13). By contrast, there is a paucity of data regarding the association of carotid-femoral PWV with the severity and extent of atherosclerosis, particularly for asymptomatic atherosclerotic lesions. A cross-sectional study in a population of hypertensive patients showed that carotid-femoral PWV was strongly related to the presence and extent of a composite criterion combining the presence of a history of cardiovascular heart disease, peripheral vascular disease or cerebrovascular disease, and/or the presence of abdominal aorta aneurysm (27). In a population-based cohort study (28), aortic stiffness was strongly associated with common carotid intima-media thickness, the presence of plaques in the carotid artery and the aorta, and the presence of peripheral arterial disease. Interestingly, the association remained significant after adjustment for cardiovascular risk factors and after exclusion of subjects with prevalent cardiovascular disease. A few studies have reported an association between arterial stiffness and CAD [assessed by coronary angiography (29), CT coronary angiography (30), intravascular ultrasound catheter (31), and the presence and quantity of coronary artery calcium (32)]. Our study is the first large study that assessed the predictive value of aortic stiffness for asymptomatic CAD in a population of stroke patients.
Predictive value assessment of arterial stiffness
Appropriate model assessment is critical to the determination of clinical impact and to guideline development (33). The C statistic, a measure of discrimination also known as the area under the ROC curve (34), is the most popular measure of model fit. However, it has been shown that improvement of model performance can be missed if C statistic alone is performed (24). Pencina et al. (24) recently introduced the concept of net reclassification improvement. This method measures the extent to which persons with and without events or lesions are appropriately reclassified into clinically accepted higher or lower-risk categories with the addition of a new marker. The net reclassification improvement therefore provides a method of quantifying the enhancement in risk estimation when a novel marker is added to a standard risk prediction model. We showed that the addition of carotid-femoral PWV to the standard model including FRS and the presence of cervicocephalic stenosis led to a significant improvement of the prediction of ⩾50% asymptomatic CAD in stroke patients and may represent a valuable biomarker in clinical practice.
Limitations
Our study has potential limitations. From a methodological point of view, carotid-femoral PWV is a continuous variable and the choice of a cutoff value is questionable. The use of the 9·6 m/s cutoff was based on recent guidelines (26) and recommendations (18). Second, the net reclassification improvement is dependent on the choice of risk categories. Ideally, the risk categories should be done according to accepted higher or lower-risk categories leading to medical decisions. As the benefit of screening for asymptomatic CAD in stroke patients has not been assessed, it was not possible to propose such categories. Therefore, we stratified the risk of ⩾50% asymptomatic CAD in five categories (<10%, 10–20%, 20–30%, 30–40%, and >40%) and showed that results were similar when three categories were used. Moreover, we also showed a better integrated discrimination improvement, which is independent of risk categories and may be used as an objective indicator of reclassification improvement (13). Finally, the median time from the stroke/TIA onset to carotid-femoral PWV measurement could have affected the precision of carotid-femoral PWV measurement. The median time from stroke/TIA onset to carotid-femoral PWV measurement was eight-days and the predictive value of carotid-femoral PWV was not modified when this delay was accounted for (data not shown). From a clinical practice point of view, in these post-stroke patients, we used a threshold of at least one coronary lesion ⩾50% to define asymptomatic CAD, and identified the predictive factors for this condition. The natural history of asymptomatic CAD remains unknown and there is still uncertainty about potential benefits of treating specifically asymptomatic CAD (35). Therefore, the potential benefit of screening stroke/TIA patients for asymptomatic CAD remains to be specifically assessed through a randomized clinical trial comparing standard secondary prevention with a more aggressive approach that would include screening for asymptomatic CAD and specific treatments such as coronary revascularization, in particular for patients with left main trunk or 3-vessel disease. Our study provides useful data for conception of such a trial. Pending the results from randomized trial, the decision to screen for asymptomatic CAD in stroke patients should be individualized, and can be based on predictive factors and the feasibility of specific CAD preventive strategies.
Perspectives
Stroke/TIA patients with asymptomatic CAD are highly predictable from traditional vascular risk factors and the presence of cervicocephalic artery stenosis. Aortic stiffness appears to be also of interest and could be more assessed in order to predict vascular prognosis in patients with stroke or TIA.
Footnotes
Acknowledgement
We thank Ludovic Trinquart (French Cochrane Center, Paris, France) for statistical assistance.