
Abstract
Background
Coronary artery disease is highly prevalent in patients with stroke, but because revascularization does not improve major clinical outcomes in patients with stable coronary artery disease relative to intensive medical therapy, routine evaluation for this disease is not warranted in stroke patients. However, it might be warranted in patients destined to undergo vigorous physical therapy. The Locomotor Experience Applied Post-Stroke study, a randomized controlled trial of 408 participants that tested the relative efficacy of two rehabilitation techniques on functional walking level, provided the opportunity to address this question.
Aim
The study aims to test the efficacy of screening for cardiovascular disease and an exercise tolerance test in assuring safety among patients undergoing vigorous rehabilitation for gait impairment.
Methods
All participants were screened for serious cardiovascular and pulmonary conditions. At six-weeks poststroke, they also completed a cardiovascular screening inventory and underwent an exercise tolerance test involving bicycle ergometry. Participants received 36, 90-min sessions of a prescribed physical therapy (three per week), initiated at either two-months or six-months poststroke.
Results
Twenty-nine participants were excluded on the basis of the cardiac screening questionnaire, and 15 failed the exercise tolerance test for cardiovascular reasons. No participant experienced a cardiac event during a treatment session. Two participants experienced myocardial infarctions, but continued in the trial. In three additional participants, myocardial infarctions caused or contributed to death.
Conclusions
The combination of a negative cardiac screen and the absence of exercise tolerance test failure appeared to have a high negative predictive value for cardiac events during treatment, despite the likelihood of a high prevalence of coronary artery disease in our population.
Keywords
Coronary artery disease (CAD) is highly prevalent in patients with stroke. Coronary plaques and coronary stenosis of ≥50% were observed in 72·4% and 37·5%, respectively, of patients who underwent autopsy after fatal stroke (1), and in 61·9% and 25·7%, respectively, of patients who underwent coronary angiography after stroke (2). In a meta-analysis of 39 population and randomized controlled trials (RCTs), the annual risk of myocardial infarction (MI) was 2·2% (95% CI 1·7–2·7) (3). It may be twice this high in patients with internal carotid artery disease and a history of symptomatic CAD (4). However, because neither routine revascularization (5,6) nor percutaneous coronary intervention (7,8) improves major clinical outcomes when compared with intensive medical therapy in patients with stable CAD, and this medical therapy is identical for patients with stroke, this high prevalence of CAD is not, in and of itself, cause for diagnostic inquiry. Further diagnostic evaluation is warranted only if patients are symptomatic or have evidence of ischemia on noninvasive tests. It might also be warranted if patients are to undergo vigorous physical therapy in the course of stroke rehabilitation. This is the focus of the present investigation, which involves a secondary analysis of results of the Locomotor Experience Applied Post-Stroke (LEAPS) trial, a large, multicenter RCT of rehabilitation interventions for gait impairment after stroke (9,10). LEAPS employed a cardiovascular screening questionnaire in conjunction with an exercise tolerance test (ETT) involving bicycle ergometry immediately prior to randomization to minimize the probability of entering subjects at risk for coronary events during study treatments. Our hypothesis was that such screening would eliminate the risk of therapy-induced MI. We report here the results of this strategy.
The LEAPS trial compared two types of rehabilitation interventions provided by physical therapists to improve walking after disabling first stroke. LEAPS targeted adults who had hemiparesis due to a stroke severe enough to require inpatient rehabilitation, followed by discharge home. At the time of randomization, two-months after stroke, participants were still limited to walking with assistance in the home or to walking short distances in the community. Interventions were: (1) a progressive, task-specific locomotor training program (LTP) that included walking on a treadmill with partial body weight support and over-ground practice; and (2) a progressive strength and balance exercise program delivered in the home [home exercise program (HEP)]. LTP and HEP were delivered at two-months (early) poststroke in addition to usual care. A delayed LTP group received the intervention at six-months poststroke. Because the LEAPS protocol involved three 90-min treatment sessions/week for 12 weeks, subjects were exposed to repeated vigorous exercise over an extended period of time, thereby testing the adequacy of our screening procedure.
Aim
Our aim was to test the efficacy of screening for cardiovascular disease, combined with an ETT, in assuring safety among patients undergoing vigorous rehabilitation for gait impairment.
Methods
Study design
The LEAPS trial was a multicenter, single-blind RCT, stratified by walking impairment level at two-months after onset of stroke (severe, <0·4 m/s, and moderate, 0·4 – <0·8 m/s), with randomization to three protocol intervention groups, early LTP, late LTP, and HEP (proportions 7:7:6).
The LEAPS protocol and 12-month primary outcomes have been reported (9,10). Ethics review boards at all participating centers approved the protocol. All participants provided written informed consent. An independent medical monitor and a data safety monitoring board (DSMB) appointed by the National Institutes of Health (NIH) oversaw the conduct, safety, and efficacy of the trial, and monitored adverse events.
Study population and screening
Participants were recruited from six inpatient rehabilitation sites in California and Florida. Inclusion criteria were age ≥18 years; stroke within 45 days and ability to be randomized at two-months poststroke; residual paresis in the lower extremity; ability to walk 10 ft with no more than one-person assistance; ability to follow a three-step command; physician approval for participation; self-selected 10-m walking speed less than 0·8 m/s; and living in the community by the time of randomization.
General exclusion criteria included: dependency in activities of daily living before the stroke; inability to ambulate at least 150 ft prior to stroke, or intermittent claudication while walking less than 200 m; preexisting nonvascular neurological disorders; prior stroke with residual motor impairment; uncontrolled diabetes not responsive to medication or diet; and inability to travel to the treatment site.
Exclusion criteria related specifically to serious cardiovascular and pulmonary conditions included: (1) hospitalization for MI or heart surgery within the previous three-months; (2) history of congestive heart failure; (3) documented serious and/or unstable cardiac arrhythmias; (4) hypertrophic cardiomyopathy; (5) severe aortic stenosis; (6) angina or dyspnea at rest or during activities of daily living; (7) meeting the New York Heart Association criteria for Class 3 or Class 4 heart failure; (8) coronary artery bypass grafts (CABG) or valve replacement within the previous three-months if participation was not approved by two physicians: a cardiothoracic surgeon and either a cardiologist or the participant's primary care physician; (9) history of serious chronic obstructive pulmonary disease or use of supplemental oxygen; (10) history of pulmonary embolism within six-months; (11) severe hypertension with systolic blood pressure (SBP) >200 mmHg and diastolic blood pressure (DBP) >110 mmHg at rest, that could not be reduced to ≤180/100 mmHg with appropriate medical therapy; and (12) contraindication to the performance of an ETT.
Interventions
The LTP and HEP programs were controlled for exercise frequency (90-min sessions, three times per week) and duration (12 to 16 weeks), for a total of 30–36 exercise sessions. LTP included stepping on a treadmill with partial body weight support for 20–30 min at 2·0 mph, with manual assistance as needed, followed by a progressive over-ground walking program, sustained for 15 min, provided by a physical therapist and rehabilitation technician(s) (0–2) in the clinic. HEP included progressive flexibility, joint range of motion, upper- and lower-extremity strength, coordination, and static and dynamic balance exercises provided by a physical therapist at home. In addition to the LTP and HEP interventions, all participants were allowed to receive any prescribed usual and customary care during the intervening periods.
ETT
The ETT was conducted at all participating centers six-weeks after stroke, prior to trial randomization at two-months poststroke. A participant could not be randomized without completing the ETT. The purpose of the ETT was to enhance patient safety during the trial and not to definitively elicit myocardial ischemia by maximizing physical stress. Participants first completed a cardiovascular screening inventory (Appendix S1) to assess cardiac medical history, cardiac disease risk factors, family cardiac history, and current medications. On the basis of this inventory and a physical examination, a cardiologist determined ETT eligibility. If the ETT was contraindicated, participants were referred to their primary care physician for appropriate follow-up and did not proceed with the trial screening process.
A previously established bicycle ergometry protocol (11,12) was used to assess exercise tolerance. As the only ambulatory requirement for the LEAPS trial was the ability to walk 10 ft, a treadmill protocol was not feasible. The ETT was conducted on a bicycle ergometer (Monark Ergonomic Testing Bicycle, Model 828E, HealthCare International, Langley, WA, USA) in cardiology assessment laboratories at the six clinical trial sites under the supervision of a cardiologist, with trial staff providing standardized instructions to participants. Electrocardiogram (ECG) electrodes (n = 10) were placed in the standard configuration. ECG, blood pressure (BP), and heart rate (HR) were recorded for one-minute supine followed by 1 one-minute in the sitting position. Participants either sat on the bicycle seat or in a chair (if necessary because of poor sitting balance), with their hemiparetic leg secured to the bicycle footplate with a boot and their hemiparetic arm to the handle bar with a glove support. Once subjects were positioned, vital signs were recorded for an additional two-minutes. Requisite parameters to commence the ETT were: BPD ≤ 100 mmHg, BPS ≤ 180 mmHg, and HR ≤ 100. Participants pedaled at 40–60 r.p.m. with a power increase of 10 watts (from an initial 0 watts) per minute. HR obtained from the ECG tracing was recorded every minute, and BP readings, obtained manually, every two-minutes. Participants reported their rate of perceived exertion (RPE), using the Borg Scale (13), every minute. Standardized verbal encouragement was provided throughout the test. ETT end-points were established a priori.
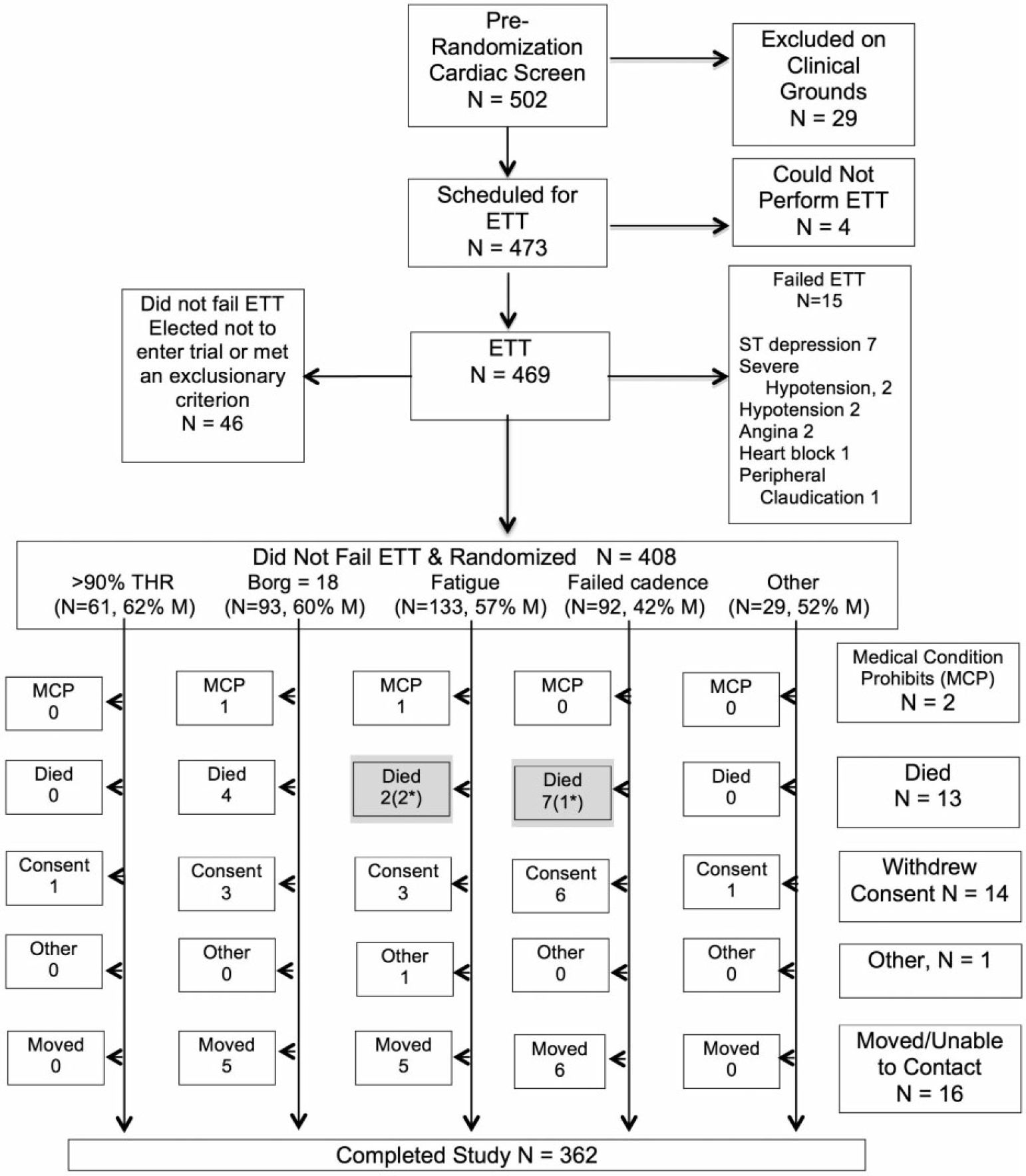
CONSORT diagram for subjects who were eligible to complete the prerandomization cardiovascular screening questionnaire. *In three participants who died (shaded boxes), MI was a primary or contributing cause of death. ETT = exercise tolerance test; medical condition prohibits (MCP) = development of a noncardiac medical condition that precluded further participation; MI, myocardial infarction; THR = targeted heart rate.
The ETT primary end-point – the targeted heart rate (THR) – was ≥ 90% predicted maximum HR (220-age). For those on β-blockers, the primary end-point was RPE >18. The ETT was terminated prior to attaining these end-points if 40 r.p.m. could not be maintained or if the participant experienced onset of preestablished limiting clinical manifestations (Fig. 1). At test termination, a final RPE score was recorded, resistance removed, and the participant continued to pedal at 40 r.p.m. for one-minute. BP and HR were recorded after the one-minute cool-down and at three and five-minutes, or until HR and BP returned to pretest values. The cardiologist provided written documentation for ETT termination and determined trial eligibility. If a preestablished ETT failure point occurred, the participant was managed medically, referred for follow-up care, and was no longer eligible for trial participation.
There were three possible ETT outcomes:
Failure defined by the clinical judgment of the onsite cardiologist performing this test (an exclusionary criterion).
Successful completion as defined by achievement of >90% THR or RPE >18 (eligible for randomization).
Neither ETT failure nor achievement of criteria for successful completion, e.g., because of extreme fatigue, inability to maintain cadence, or other causes (but eligible for randomization). We posited that because of their inability to meet criteria for successful completion, the ETT might have been less informative in these participants and they might have been at higher risk for coronary events during treatment.
Statistical analysis
Descriptive statistics were provided for the ETT results. In addition, 95% confidence intervals were calculated for rate of failing the ETT and for the rate of MI during treatment by reason of ETT termination. All statistical analyses were performed using SAS software, version 9.1 (SAS Institute, Cary, NC).
Results
The LEAPS trial screened a total of 4909 subjects in four successive screens: the first a chart review under the Health Insurance Portability and Accountability Act waiver; the second a direct contact with the potential participant or family member to determine interest in participating in the trial and continued eligibility; the third a clinical evaluation conducted between 5 and 45 days after stroke; and the fourth a prerandomization reevaluation conducted between 45 and 60 days after stroke (Table 1). The table does not provide an exhaustive list of exclusionary criteria met because once a potential participant was determined to meet one exclusionary criterion, he/she was eliminated from further consideration.
Reasons for exclusion in the four screens (reasons of particular interest in boldface)
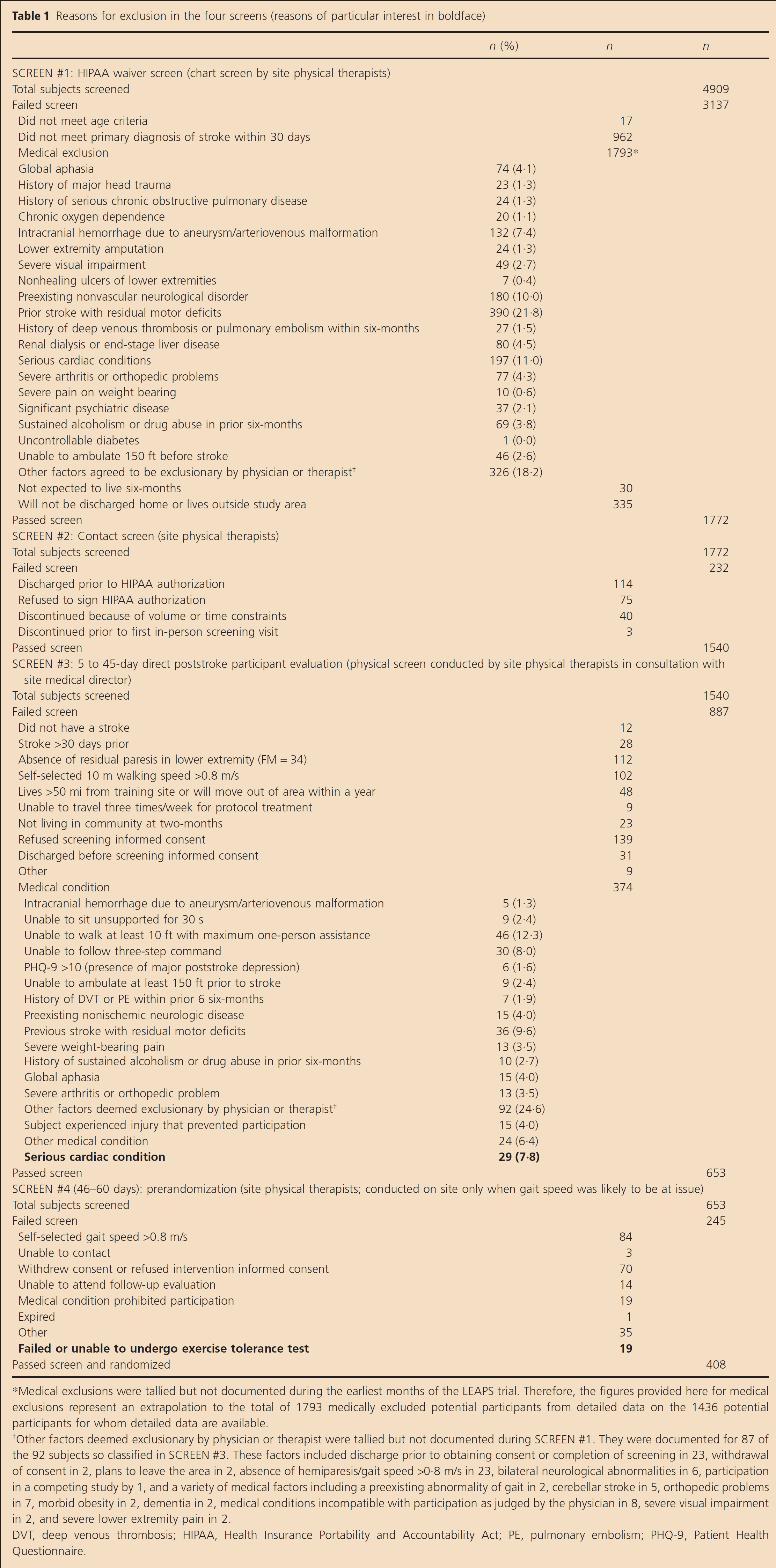
Medical exclusions were tallied but not documented during the earliest months of the LEAPS trial. Therefore, the figures provided here for medical exclusions represent an extrapolation to the total of 1793 medically excluded potential participants from detailed data on the 1436 potential participants for whom detailed data are available.
Other factors deemed exclusionary by physician or therapist were tallied but not documented during SCREEN #1. They were documented for 87 of the 92 subjects so classified in SCREEN #3. These factors included discharge prior to obtaining consent or completion of screening in 23, withdrawal of consent in 2, plans to leave the area in 2, absence of hemiparesis/gait speed >0·8 m/s in 23, bilateral neurological abnormalities in 6, participation in a competing study by 1, and a variety of medical factors including a preexisting abnormality of gait in 2, cerebellar stroke in 5, orthopedic problems in 7, morbid obesity in 2, dementia in 2, medical conditions incompatible with participation as judged by the physician in 8, severe visual impairment in 2, and severe lower extremity pain in 2.
DVT, deep venous thrombosis; HIPAA, Health Insurance Portability and Accountability Act; PE, pulmonary embolism; PHQ-9, Patient Health Questionnaire.
Of the 502 subjects who completed the prerandomization cardiac screening inventory, 29 met cardiopulmonary exclusion criteria and were excluded (Fig. 1). Four additional participants could not perform the ETT, leaving 469 participants who actually undertook the ETT. Fifteen (3·2%) of these failed the ETT for cardiovascular reasons (95% CI: 1·9–5·3%) (Fig. 1), and 46 did not fail but either met other trial exclusionary criteria or elected not to participate in the trial, leaving 408 who were actually randomized. Because some exclusionary events occurred after the cardiac screen or even after the ETT (e.g., improvement in self-selected gait to >0·8 m/s, withdrawal of consent, acquisition of medical illness, or death), 46 of the subjects excluded for noncardiac reasons in Screens 3 and 4 are included in Fig. 1.
Of those randomized, 154 (38%) met the criteria for passing the ETT [THR, 61 participants (15%); Borg RPE >18, 93 participants (23%)]. Two hundred fifty-four (62%) did not fail the ETT, but could not meet criteria for passing for various reasons: 133 (33%) complained of intolerable fatigue (e.g., ‘I need to stop’ or ‘I can't do this anymore.’); 92 (23%) could not maintain cadence to at least 40 r.p.m.; and 29 (7%) for a variety of reasons. These included dyspnea (2), angina (1), ≥1 mm horizontal or down-sloping ST-segment depression (1), unspecified abnormal ECG response (1), hypotension (drop in SBP of >20 mmHg) (1), severe hypertension (BPS ≥220, BPD ≥120) (21), and knee pain (2). ETT failure was defined by the clinical judgment of the onsite cardiologist performing this test, and the three subjects with angina or ST segment changes were judged not to have failed the test despite these manifestations.
The mean (±SD) age of the 408 randomized participants was 62·0 ± 12·7; 54·17% were men and 22·1% were black (10). At randomization, the average number of days since the stroke was 63·8 ± 8·5. Of the strokes, 71% were ischemic infarcts, 17% were hemorrhages, and 12% were undefined. Twenty-seven percent of participants had a history of cardiovascular disease; 81% hypertension, 35% diabetes; 9% peripheral vascular disease; 6% chronic obstructive pulmonary disease; and 36% arthritis or another musculoskeletal condition. The modified Rankin score was between 2 and 4 (slight to moderately severe disability) in 99·5% of participants. Self-selected walking speed was less than 0·.4 m/s in 53·4% and between 0·4 and 0·8 m/s in 46·6%. The mean lower extremity Fugl-Meyer score was 24·38 ± 6·46.
Of the 408 randomized participants, a total of 46 were unable to complete the trial (Fig. 1). Two participants were eliminated from the trial because of the development of medical conditions that precluded continued participation [‘medical condition prohibits (MCP’)]; 13 died; 14 withdrew consent; 16 moved or were lost to contact; and one was eliminated by mutual agreement.
The intensity of the exercise involved in body weight-supported treadmill training is reflected indirectly in the HR response of participants in the early-LTP group compared with that of participants in the HEP group (Table 2).
Heart rate response to exercise
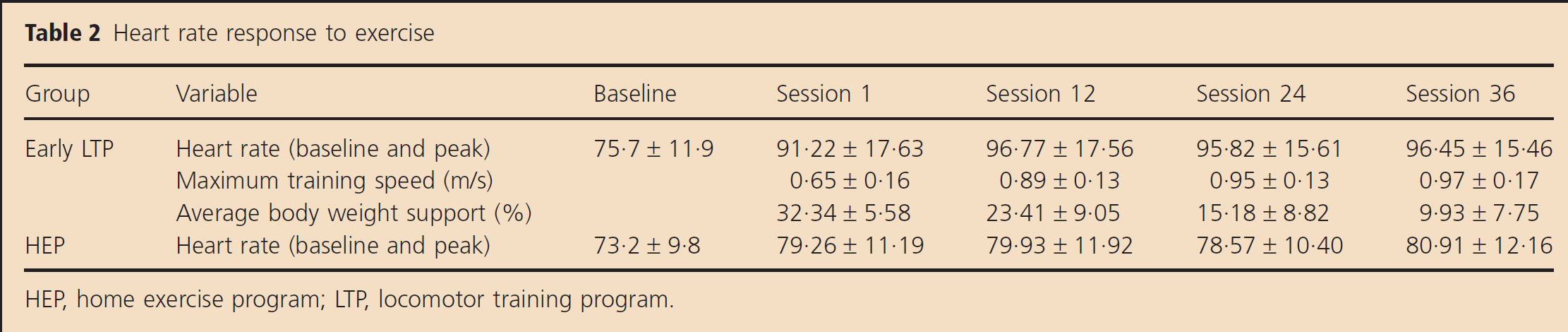
HEP, home exercise program; LTP, locomotor training program.
Of the randomized participants, none experienced a cardiac event in the course of a trial intervention. Two experienced an MI during the 10 months they were in the trial, but continued in the trial cohort. In three participants who died, MI was the primary cause of death in two, and in a third, MI complicated a recurrent stroke. Two of these participants were in the fatigue and three were in the failed cadence ETT group. The 95% confidence intervals for an MI during treatment were 0, 0·08% in the ETT THR group; 0, 0·38% in the Borg >18 group; 0, 0·27% in the fatigue group; 0, 0·06% in the failed cadence group; and 0, 0·18% in the ‘other’ group.
Although the number of deaths was not sufficient to enable statistical inference, the disproportionate occurrence of death in two ETT groups, Borg >18 and failed cadence, led us to a case-by-case review of the causes of death. The causes of death in the Borg >18 group were a mediastinal mass, basilar thrombosis with a locked-in syndrome complicated by pneumonia and sepsis, sepsis and adult respiratory distress syndrome (ARDS), and lung cancer. In the fatigue group, the causes of death were recurrent stroke followed by MI, and MI. In the failed cadence group, the causes were cancer (2), MI, complications of a hip fracture, a complication of plasmapheresis, aspiration pneumonia with ARDS, and uncertain (1).
Discussion
The first major finding of this secondary analysis of the LEAPS trial was that among those who did not fail the ETT and were randomized to LEAPS, not a single subject experienced a coronary event while receiving a treatment. The achievement of this level of safety was our goal in carefully screening subjects and in employing the combination of a cardiovascular screening inventory and the ETT. These results suggest that this process was highly effective in identifying subjects who might be at risk for a coronary event precipitated by treatment exertion. However, because we did not randomize subjects who did not pass the prerandomization cardiac screen or who failed the ETT, our study does not constitute proof that these two measures were responsible for the good outcome. We can say that the combination of a negative cardiac screen and the absence of ETT failure appeared to have a high negative predictive value for cardiac events during treatment, despite the likelihood of a high prevalence of CAD in our population.
Second, our screening procedures and our cardiopulmonary review of systems did not successfully exclude all subjects at risk for MI: 15/469 (3·2%) of the participants who underwent the ETT failed on cardiac grounds, as judged by a participating cardiologist; two subjects experienced an MI during the trial period, though not in the course of actual treatment; and in three subjects, MI was the cause or a contributing factor to death. The small but clinically significant number of subjects who passed the cardiovascular screening but failed the ETT may have been at risk for a coronary event while participating in a physically intensive rehabilitation program. A recent study of 98 patients with chronic stroke and roughly similar cardiovascular risk factors reported that 11·2% demonstrated clinically significant abnormalities on ETT (14), possibly because they were less disabled (six-minute walk distance of 272 ± 139 m compared with 125 ± 78 m in LEAPS) and therefore capable of exercising more vigorously (pedaling rate of 60 r.p.m. compared with 40 r.p.m. in LEAPS). These observations suggest that an ETT should be considered in patients who engage in walking training that places substantial physical demands on them, demands comparable with those made in the LEAPS treatments, or that extra caution should be taken in building up to high-intensity exercise. The intensity of the exercise involved in body weight-supported treadmill training, as judged by the HR response in our participants (Table 2), could best be characterized as moderate, but certainly substantially greater than that in the HEP group, which might be considered roughly comparable with that achieved in customary and usual physical therapy.
Third, although the ETT provided major accommodations for the neurological disability of the trial participants, only 154 (38%) of the participants were able to meet criteria for passing the ETT. The fraction of participants performing an ETT that does not fail by cardiologic criteria but cannot meet the THR or Borg threshold is likely to depend substantially on severity of neurologic impairment. We are unaware of other studies of an ETT after stroke that have fractionated ETT outcomes in the way we have, and therefore we cannot determine how representative our data are. The participants in our study who had to stop the ETT because of fatigue or could not maintain bicycling cadence appeared to be at greatest risk for future myocardial events, suggesting that in these groups, the ETT, combined with the cardiovascular screening inventory, was not an adequate screen for coronary risk in general. The reasons for this heightened risk in these subpopulations are unclear and the very small N's do not warrant statistical inferences. Our case-by-case analysis of causes of death revealed multiple causes, most of which bore no relationship to CAD. Our study does suggest that inability to meet THR or Borg criteria on the ETT, in the absence of signs of CAD during the test, is not associated with greater risk of MI during treatment.
Marzolini et al. (14). found that women were significantly less likely than men to reach cardiopulmonary exercise levels of adequate intensity to inform therapeutic exercise regimens. We, too, found that women were numerically less likely than men to achieve >90% THR or a Borg score of ≥18 (Fig. 1). However, in our study, the difference was not significant (P = 0·06, Fisher's exact test).
It might be asked to what extent the LEAPS population was representative of the general population of patients undergoing gait rehabilitation in rehabilitation clinics. A review of the reasons for study exclusion and major exclusionary medical comorbidities (Table 1) suggests that, by and large, the excluded subjects would not likely be candidates for intensive treatment of gait impairment in any rehabilitation clinic. Furthermore, LEAPS participants had medical comorbidities quite characteristic of the stroke population in general.
Our study does not speak to risk for coronary events in the first two-months poststroke, during which time the risk of these events is maximal (15). In a study of 1029 consecutive admissions to the Rehabilitation Institute of Chicago, in which mean stroke to admission interval was 17·4 days and mean length of rehabilitation stay was 28 days, 2·9% of patients experienced angina and none an MI (16).
Because exercise stress tests have a sensitivity of 45–50% and a specificity of 85–90% for CAD (17), failure on the ETT cannot be regarded as proof of CAD, even in at-risk populations. For example, assuming the pretest probability of coronary artery stenosis of 26% that has been reported in a stroke population (2), and assuming that our ETT had a sensitivity and specificity similar to that of conventional exercise electrocardiography, there would be a 35% probability that a patient failing the ETT would have no coronary artery stenosis.
Conclusion
The combination of a negative cardiac screen and the absence of ETT failure appeared to have a high negative predictive value for cardiac events during treatment, despite the likelihood of a high prevalence of CAD in our population.