
Abstract
Rationale
About 20% of stroke patients develop dementia within a few months after their event, but the determinants and mechanisms of poststroke dementia are insufficiently understood.
Aims
To identify and characterize the determinants of cognitive impairment poststroke.
Design
Observational prospective study in patients with acute stroke and no prior dementia. Six hundred subjects will be characterized by detailed interview, standardized clinical examinations, biometric measures (intima-media thickness, waist-hip ratio, and ankle-brachial index), multimodal imaging (magnetic resonance imaging, fluorodeoxyglucose-positron emission tomography (FDG-PET), amyloid-positron emission tomography (amyloid-PET), and retinal imaging), analysis of biomarkers derived from blood and cerebrospinal fluid, and detailed cognitive testing at repeat time points. Patients will be followed for five-years with a total of five personal visits and three telephone interviews.
Study Outcomes
Primary end-point is the occurrence of post-stroke dementia. Secondary end-points include poststroke cognitive impairment–no dementia, stroke recurrence, and death. Predictive factors for poststroke dementia will be identified by multiple Cox proportional-hazards model.
Results
Baseline characteristics of the first 71 patients (study inclusion between May 2011 and August 2012) are as follows: median age, 70 years (interquartile range, 65–75); female gender, 25 (35%); median National Institutes of Health Stroke Scale at admission, 2 (1–4); and etiological stroke subtypes according to TOAST classification, 15% large artery disease, 18% small vessel disease, 35% cardioembolic, and 32% undetermined or multiple competing etiologies.
Discussion
This study will provide insights into the mechanisms of poststroke dementia and hold the potential to identify novel diagnostic markers and targets for preventive therapies. The study is registered at http://www.clinicaltrials.gov (NCT01334749) and will be extended as a multicenter study starting 2013.
Introduction and rationale
About 20% of stroke patients develop dementia within a few months after their event (1). After the first year, the annual incidence rate of dementia amounts to about 3%/year (2). The determinants of cognitive decline and dementia after stroke are insufficiently understood. Previous studies have identified specific stroke characteristics and complications of stroke that are associated with poststroke dementia (PSD). However, most studies have been small and there are few studies that have assessed the role of coexisting neurodegenerative pathology in PSD. Vascular and neurodegenerative pathology interact in causing cognitive decline. About 40% of patients with a clinical diagnosis of probable Alzheimer's disease (AD) display ischemic pathology at autopsy (3). Vascular pathology modulates the clinical expression of neurodegenerative disease and there are multiple biological interactions between neurodegenerative and vascular pathology (4). Thus, for example, β-amyloid promotes vascular insufficiency, while ischemia may cause accumulation of β-amyloid. Cross talk between neurodegenerative and vascular pathology is now also recognized as an important factor in patients with stroke (5) and signs of neurodegenerative pathology on neuroimaging are a major predictor of PSD (1,6), which includes all types of dementia that occur after stroke, irrespective of their cause (5). Patients with acute stroke provide a target for both studying the interactions between vascular and neurodegenerative pathology and for future preventive strategies aimed at lowering the burden of dementia (7). The Determinants of Dementia After Stroke (DEDEMAS) (http://www.clinicaltrials.gov, NCT01334749) trial is designed to disentangle the interplay between factors contributing to the development of a dementia after stroke.
Methods
Design
DEDEMAS is an observational hospital-based cohort study in patients suffering from acute stroke conducted at the Interdisciplinary Stroke Center, Munich, Germany. Six hundred subjects will be deeply characterized and followed for five-years with a total of five personal visits and three telephone interviews (Table 1). Structural and functional magnetic resonance imaging (MRI) examinations on all patients will be done on a 3-Tesla system using an imaging protocol, which has specifically been designed to allow optimized assessment of both neurodegenerative and vascular changes.
Schedule of assessments
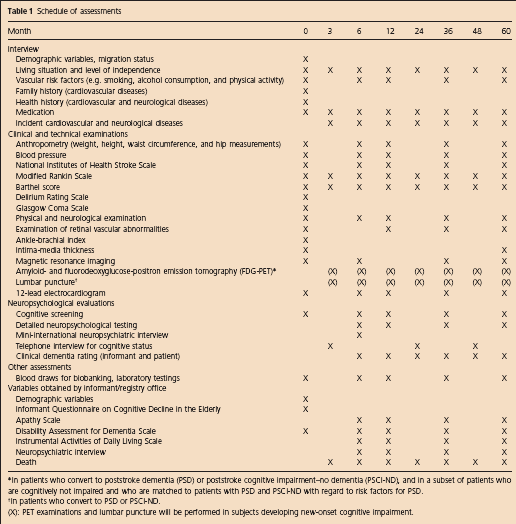
In patients who convert to poststroke dementia (PSD) or poststroke cognitive impairment–no dementia (PSCI-ND), and in a subset of patients who are cognitively not impaired and who are matched to patients with PSD and PSCI-ND with regard to risk factors for PSD.
In patients who convert to PSD or PSCI-ND.
(X): PET examinations and lumbar puncture will be performed in subjects developing new-onset cognitive impairment.
18FDG- and amyloid-PET examinations will be done in patients converting to dementia, in patients showing cognitive decline, and a limited number of controls. Subjects will provide biomaterial at baseline and at follow-up. Patients included in local stroke registries will serve as a reference to control for selection bias.
Patient population – inclusion and exclusion criteria
Patients are recruited through the local certified stroke unit. Stroke is defined by an acute focal neurological deficit in combination with a new lesion detected by magnetic resonance or computed tomography scan. Patients with prior dementia are excluded. Prior dementia is defined by a summed score of >64 (corresponding to an average score >4) in the short version of the ‘Informant Questionnaire on Cognitive Decline in the Elderly’ (IQCODE) (8). This cut-off point was chosen to achieve a high specificity while avoiding the exclusion of a large number of patients without prior dementia. The area under the curve for this cut-off value has previously been shown to be 0·82 (9). The IQCODE scores of all patients will be included in multiple regression analysis to account for possible confounding. For detailed inclusion and exclusion criteria, see Table 2.
Inclusion and exclusion criteria
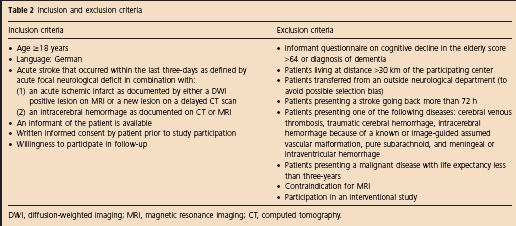
DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging; CT, computed tomography.
Treatment or intervention
No study-related interventions are planned. Patients are treated following current guidelines (10).
Primary outcome
Primary outcome is the occurrence of any PSD irrespective of its cause.
Secondary outcomes
Occurrence of any poststroke cognitive impairment–no dementia (PSCI-ND), irrespective of its cause
Secondary cognitive improvement of PSD or PSCI-ND
Dementia subtype [vascular dementia (VaD), AD, mixed dementia, and other categories]
Occurrence of recurrent stroke
Death.
End-point assessment
The cognitive end-points of any cognitive impairment are assessed by a committee consisting of a board-certified neurologist who specialized in stroke care, a board-certified psychiatrist, and a neuropsychologist. Diagnoses are reassessed on a monthly basis by a second, independent committee without personal contact to the patient and blinded to identifying information. Additionally, all patients will be classified into the following diagnostic categories: AD, VaD, mixed dementia, and other categories by Diagnostic and Statistical Manual of Mental Disorders, Version IV (DSM-IV) criteria and according to the diagnostic guidelines of the ‘National Institute on Aging-Alzheimer's Association Workgroup’ (11). The considerations underlying the use of the workgroup guidelines are the following: (i) that the guidelines incorporate the use of biomarkers based on imaging and cerebrospinal fluid measures and (ii) that memory deficits are not mandatory in the workgroup guidelines, which reflects that patients with VaD may have relatively preserved memory (12). A domain is considered impaired if a performance score is more than 1·5 standard deviations below the mean score of the normative samples according to age and gender.
The diagnosis of PSCI-ND is based on the ‘National Institute on Aging-Alzheimer's Association Workgroup’ (13), which requests the presence of cognitive deficits without impaired activities of daily living.
Visits
The schedule of assessments is depicted in Table 1. Patients in whom new-onset dementia is suspected on the basis of the telephone interviews are invited to come to the study center for a full examination. Patients who are not able or not willing to attend the outpatient clinic will be visited at home.
Neurological examination
Stroke severity is assessed using the National Institutes of Health Stroke Scale (NIHSS) by a certified study clinician. The ‘modified Rankin Scale’ (mRS) and the ‘Barthel Index’ (BI) are used as functional outcome measurements (at baseline and at all follow-up assessments).
Neuropsychological assessments
At baseline, cognitive function is evaluated using the ‘Mini Mental State Examination’ (MMSE) and the ‘Montreal Cognitive Assessment’ (MoCA). Detailed neuropsychological testing is considered to be both unreliable and difficult to perform in the acute setting following a stroke and thus is done at the six-month visit. However, attention is paid to conduct the MoCA and MMSE as a cognitive screening under standardized conditions at baseline. We deliberately choose an interval of six-months after stroke for detailed neuropsychological testing to increase the number of patients able and willing to undergo the testing. To maximize the sensitivity for the detection of cognitive decline, we choose a comprehensive neuropsychological test battery covering a broad range of cognitive domains. As widely used screening tools for dementia, we repeat MMSE and the MoCA and apply the extended ‘Consortium to Establish a Registry for Alzheimer's Disease Plus'–battery (CERAD-Plus) (14) with the following sub-tests: ‘Word List Learning/Recall and Recognition’, ‘Boston Naming Test’, ‘Figure Copy and Recall’, ‘Semantic and Phonemic Fluency’, and ‘Trail Making Test Part A and B’. In addition, we perform the following:
Executive functions are further assessed using the ‘Stroop Colour-Word-Interference Test’ (15) and the ‘Digit-Symbol-Substitution Test of the Wechsler Intelligence Scale’ (16)
Verbal learning, recall, and recognition are investigated by the ‘Free and Cued Selective Reminding Test’ (17)
Visuoconstruction is measured by the ‘Rey-Osterrieth Complex Figure (ROCF) copying condition’ (18)
Visual memory is assessed using the immediate and delayed recall of the ROCF (18)
Language is evaluated using the subtest ‘Written Language of the Aachen Aphasia Test Battery’ (19)
Ideomotoric apraxia is assessed by conducting meaningful and meaningless movements to verbal command and by copying (20).
Furthermore, the following questionnaires are administered at the six-month visit:
‘The Centre for Epidemiologic Studies Depression Scale’ (CES-D) (21,22)
The Short Form (36) Health Survey (SF-36) (23) asking for quality of life
‘Visual Analogue Scale’ to measure fatigue (24)
‘The Clinical Dementia Rating Score’ (25) to assess dementia severity.
During the telephone interviews, the cognitive status is briefly screened using the ‘Telephone Interview for Cognitive Status’ (TICS) in its modified German version (26).
Neuroimaging
Patients undergo detailed MRI at repeat time points. Image analysis will include known predictors of neurodegenerative pathology (such as whole brain, medial temporal lobe, and hippocampal volume) (27), volumetric and spatial analysis of vascular lesions (28), and more advanced imaging techniques, such as tractography and resting-state functional MRI to study brain networks and distant effects of infarcts (29). PET imaging is done at the six-month follow-up and if a cognitive decline occurs with a focus on glucose metabolism and amyloid imaging (30).
Biomaterials
The collection of biomaterials includes sampling of DNA, RNA, plasma, and serum, as well as cerebrospinal fluid (CSF) for ‘omics’ approaches and targeted studies of prespecified factors (such as Apolipoprotein E (ApoE)) and novel candidates that will emerge over the course of the study.
Data monitoring body
Data collection is managed using TeleForm (Electric Paper GmbH, Lüneburg, Germany). Biosamples are processed using standard operating procedures harmonized with the ‘Munich Biotech Cluster m4’ (31). Imaging data are instantly checked for quality and protocol conformity. Additional quality controls are done on a monthly basis.
Sample size
We expect to include 600 patients.
Statistical analyses
To identify predictive factors for PSD, a multiple Cox proportional-hazards model will be used. The possible effect of previously published predictors will be investigated first. Factors having received less attention will be investigated afterward, including relevant confounders in the models and analyzing effect-measure modifications. Competing risks (like death) will be accounted for by using competing-risks analysis. We calculated the power for survival analysis. Chance of exposure for the 18 significant factors identified by a previous meta-analysis was between 14% (for atrial fibrillation) and 50% (for atrophy), with an odds ratio between 1·3 (for women) and 6·4 (for incontinence as a complication of stroke). Assuming a chance of exposure of 10% and a hazard ratio of 2·0, the power was calculated to be 91% (assumptions: alpha 0·05, cumulative rate for PSD = 30% within five-years after stroke, 10% dropout per year, and variance inflation factor of 1·11 to adjust for additional covariates). Generalized linear models for longitudinal data (e.g. ‘generalized estimating equations’ or ‘generalized linear mixed effects models’) and multi-state models will be used to estimate possible effects of patient characteristics or treatments on outcomes repeatedly measured over time (e.g. MMSE). All statistical analyses will be carried out with a statistical software package (SAS Institute Inc., Cary, NC). The significance level will be alpha = 0·05 for two-sided null hypotheses.
Study organization and funding
The DEDEMAS study is funded by the Vascular Dementia Research Foundation and led by the principal investigator (MD). The study is conducted according to the Declaration of Helsinki and approved by the local ethics committee.
Preliminary results
Between May 2011 and August 2012, we enrolled 71 patients. Their baseline characteristics are displayed in Table 3. As of August 2012, 48 subjects had received the three-month telephone interviews, 34 subjects underwent the first personal visits at six-month follow-up, and 12 subjects had their one-year visit. Three patients (4%) terminated the study for personal reasons. All 71 patients received a dedicated research MRI at baseline and 33 (97%) of the patients returning for the six-month visit received a follow-up MRI scan (one patient refused the MRI because of anxiety). Seventeen patients received PET imaging at the six-month follow-up.
Baseline characteristics of the first 71 patients
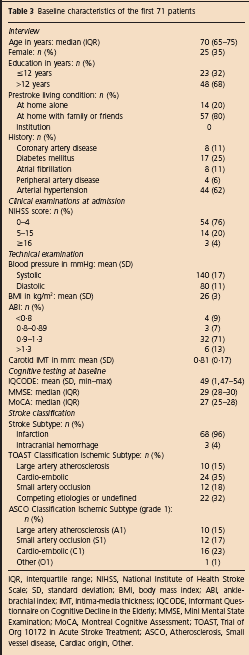
IQR, interquartile range; NIHSS, National Institute of Health Stroke Scale; SD, standard deviation; BMI, body mass index; ABI, ankle-brachial index; IMT, intima-media thickness; IQCODE, Informant Questionnaire on Cognitive Decline in the Elderly; MMSE, Mini Mental State Examination; MoCA, Montreal Cognitive Assessment; TOAST, Trial of Org 10172 in Acute Stroke Treatment; ASCO, Atherosclerosis, Small vessel disease, Cardiac origin, Other.
At six-month follow-up, 67% (23/34) of the subjects displayed cognitive impairment in single or multiple domains (PSCI-ND). One of the patients fulfilled the criteria of PSD. In two patients, an incidental diffusion-weighted imaging (DWI)-positive lesion was detected on the six-month follow-up MRI scan.
Discussion
Large studies investigating the interaction among vascular, neurodegenerative, and systemic processes in the development of PSD are needed (32). DEDEMAS is a prospective study combining systematic neuroimaging (structural and functional MRI, FDG-PET, and amyloid-PET) with advanced methods of image postprocessing (e.g. tractography and cortical thickness measurements to study white matter tract degeneration and secondary gray matter loss) (29), analyses of biomaterials (CSF and serum), and detailed cognitive testing at repeat time points. Motivating this study are the following considerations: (i) vascular and neurodegenerative pathology commonly co-occur in elderly patients; (ii) vascular brain injury induces secondary neurodegenerative changes, but the mechanisms are incompletely understood; (iii) neurodegenerative pathology modulates the response to vascular injury; (iv) vascular and neurodegenerative pathology interact in causing cognitive decline; and finally (v) better knowledge of the underlying mechanisms may help identifying individuals at risk for decline and who might benefit from targeted interventions.
Our preliminary data display a good feasibility of the study. The subjects included thus far are less severely affected than the average of stroke patients admitted to our center. This, in part, relates to the inclusion and exclusion criteria, which require that the patients are willing to return for personal follow-up visits. Nevertheless, 67% of the study participants displayed cognitive impairment six-months after stroke. We thus expect to reach a sufficient number of end-points during the planned follow-up period of five-years. Our preliminary results underline the importance of cognitive deficits following acute stroke, which – often overseen in clinical routine – are of major importance for both quality of life and long-term prognosis (33,34). Data from this study will also be used to derive and validate a risk score for PSD and PSCI-ND, which should be as simple as possible to be applicable in daily clinical routine.
Summary and conclusions
Poststroke cognitive impairment represents a major health problem and a central paradigm for how vascular and neurodegenerative pathology interacts in causing cognitive decline (1).
DEDEMAS will help defining the determinants of PSD and PSCI-ND and will likely provide important mechanistic insights. The study is quite unique in terms of size, quality, and elaborateness of phenotyping, as well as the type of investigations (e.g. resting-state functional MRI, FDG-PET, biomarkers from CSF, and retinal imaging). A good feasibility of the protocol could be demonstrated by enrolling the first 71 patients. Thus, DEDEMAS will likely improve our ability to predict dementia or cognitive impairment with no dementia following stroke. It further holds the potential to identify novel biomarkers and targets for therapeutic interventions to prevent PSD. Starting in 2013, the study will be continued as a multicenter study (DEMDAS – the DznE Mechanisms of Dementia After Stroke study) with five additional study centers in Germany. Another study using similar methodology is currently ongoing in France (Study of Factors Influencing Post-stroke Dementia (STROKDEM), http://www.clinicaltrials.gov, NCT01330160). Protocols have been harmonized to enable pooled analyses.