
Abstract
Background
Cognitive impairment after stroke is a considerable burden to patients and their caregivers and occurs in one-third of stroke survivors. No strategy to prevent cognitive decline after stroke exists thus far. Established vascular risk factors have been associated with cognitive decline and may be a target for therapeutic interventions in stroke survivors.
Aim
To test whether intensive multifactorial non-pharmacologic interventions based on lifestyle modification can reduce the risk of cognitive decline in patients who recently suffered ischemic stroke.
Methods
A randomized, controlled, multicenter, observer-blind trial was designed. The reference group obtains stroke care according to standard guidelines. The intervention group additionally receives intensive control and motivation for better compliance with prescribed evidence-based medication, regular blood pressure measurements, healthy diet, regular physical activity and cognitive training. Primary outcomes are the rate of cognitive decline at 24 months, assessed by a neuropsychological test battery and the cognitive subscale of the Alzheimer's Disease Assessment Scale.
Results
202 patients (29% women), aged 62 ± 9 years, were recruited during 2010 to 2012. Stroke related impairment at inclusion was low (mean National Institutes of Health Stroke Scale: 1.9±1.8, median modified Rankin Scale: 1 (0-1)). At baseline, groups did not differ significantly in demographic, clinical or lifestyle characteristics.
Conclusion
The recruitment was successful and the groups are balanced regarding potential confounding variables. The study will provide essential data about the feasibility and efficacy of lifestyle intervention after stroke in order to develop a new approach to prevent cognitive decline in patients with mild ischemic stroke.
Introduction
Cognitive impairment following stroke is a considerable burden to stroke survivors and their relatives. The prevalence of post-stroke dementia was found to be up to 32% and is four to six times higher than in individuals free of stroke (1). The risk of developing dementia doubles after stroke and increases the progress from mild cognitive impairment to dementia compared with persons free of stroke (1–3). Depending on the criteria used, 17–66% of stroke patients have mild cognitive impairment at three-months after acute stroke (4,5) and within the first month after stroke its presence may be even higher (6,7) also depending on the stroke sub-type (8). Using the Mini-Mental State Examination (MMSE), a cognitive decline of 0·8-2 points was reported during the first year after acute stroke (9,10).
Well-known modifiable risk factors for stroke are hypertension, diabetes, dyslipidemia, obesity, low physical activity, unhealthy diet, smoking, or excessive alcohol consumption. These factors have also been found to be associated with increased risk for cognitive decline including dementia (11–20). Randomized controlled trials targeting single vascular risk factors have found some effect in the prevention of dementia and cognitive decline for antihypertensive drugs but not for cholesterol lowering drugs (21–27).
Current research emphasizes that the risk of cardiovascular diseases including stroke increases cumulatively with the number of risk factors and that preventive management should therefore be multifactorial and individualized (28). Guidelines on ischemic stroke treatment recommend such a multifactorial approach for secondary prevention of stroke and recommend different medications and lifestyle modifications adjusted to individual risk factors (29).
A recently published randomized controlled trial investigated the effect of lifestyle modification on cognitive functions after acute stroke and transient ischemic attack but could not prove the effectiveness of such intervention (30). Besides this study, no randomized controlled trial with the aim to prevent cognitive decline after acute stroke by lifestyle or multiple risk factor modification has been published.
Recently published reviews emphasize the need for properly designed trials that include people at high risk for developing dementia and use adequate neuropsychological test batteries that are sensitive to typical changes of these patients. A follow-up period of at least one-year is recommended (31,32). Therefore, we designed this study in order to provide data on the feasibility and efficacy of multifactorial intervention in the prevention of cognitive decline after stroke.
Methods
Design of the trial
This randomized controlled trial is designed as a multicenter, observer-blind, two parallel groups clinical study. The reference group obtains stroke care according to standard guidelines. The intervention group additionally receives intensive management and motivation for better compliance with medication, regular blood pressure measurements, healthy diet, regular physical activity, and cognitive training.
The study extends over an observation period of 24 months after randomization. At baseline, after 12 months and after 24 months a full assessment is performed (Fig. 1).
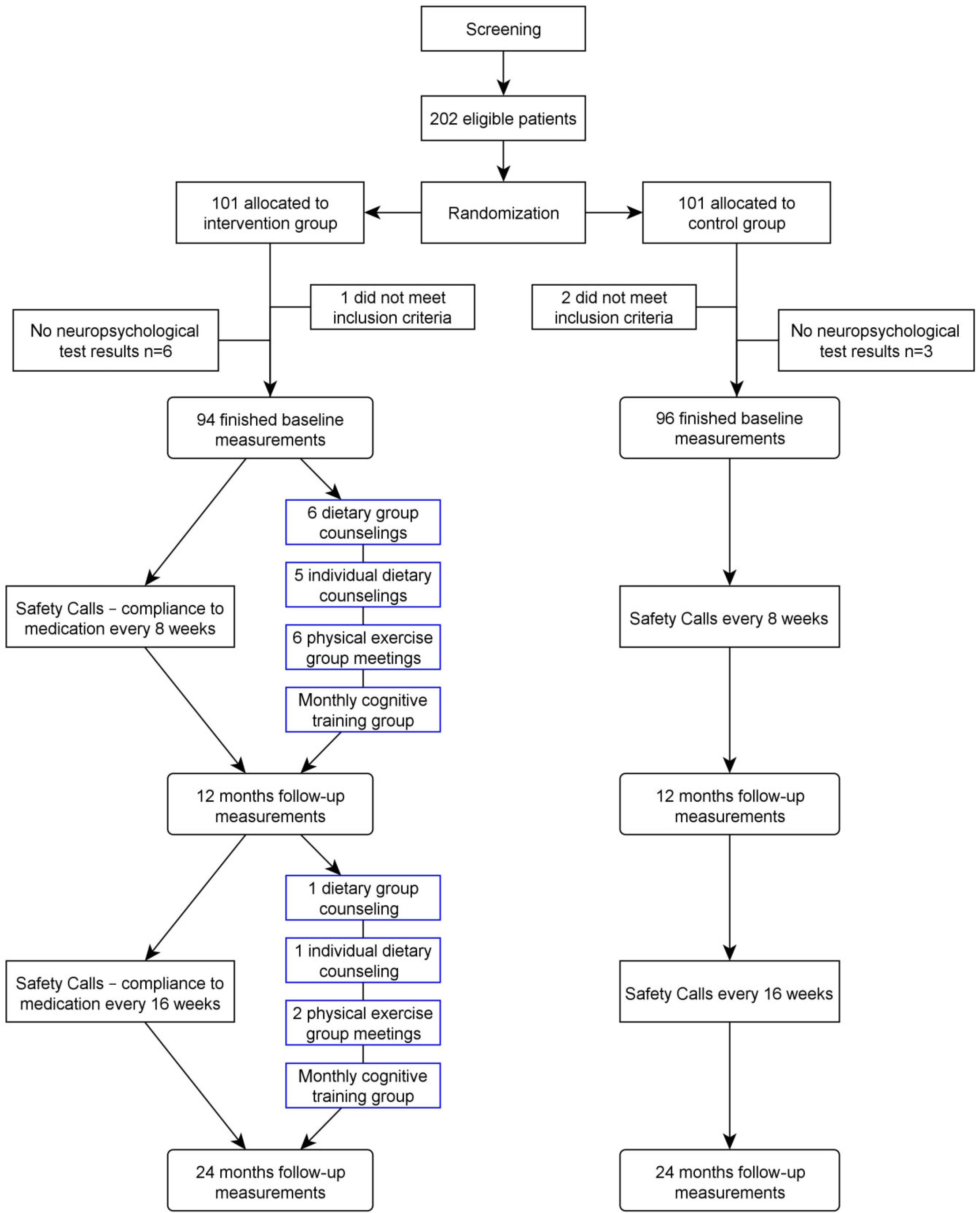
Study flowchart.
The primary objective of this study is to test whether intensive multifactorial intervention including lifestyle modification can reduce the risk of cognitive decline in stroke patients compared with a group of stroke patients receiving standard care.
Study population
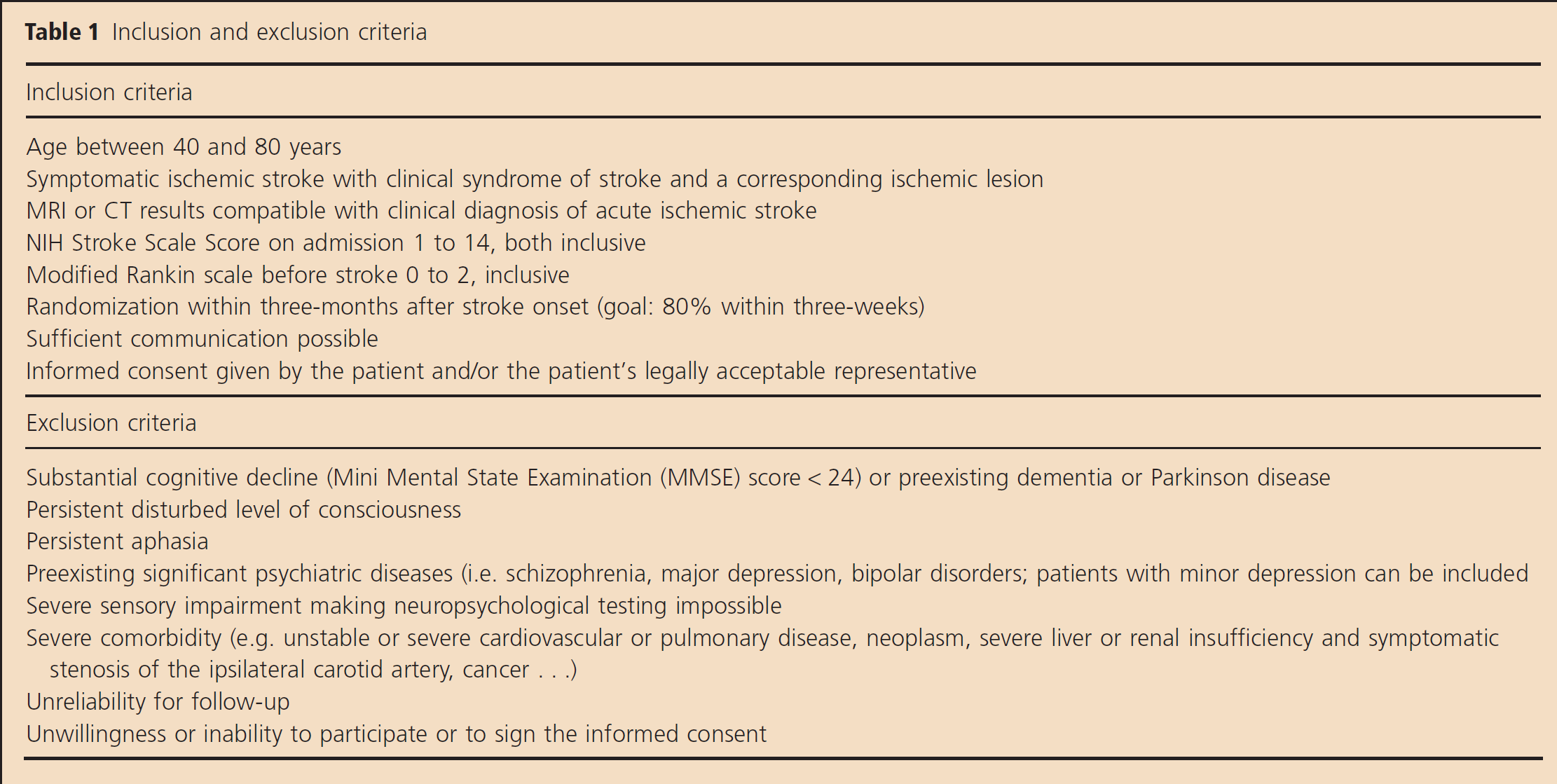
This study enrolls male and female patients, aged 40–80 years, with acute ischemic stroke based on tomography-based imaging (magnetic resonance imaging (MRI) or computer tomography (CT)). The inclusion and exclusion criteria are shown in Table 1.
Inclusion and exclusion criteria Inclusion criteria
Randomization
Block randomization using a computer-generated list with block sizes of 10 subjects is applied. A study collaborator who is independent of the conduct of the study in the local centers stores the random codes as a hard copy. Randomization is stratified by the level education, using two separate piles of opaque envelopes in each center.
Blinding
In this observer blinded study, the neuropsychologists who perform the neuropsychological test series to examine cognitive functions, and the statistician analyzing the data are blinded for the group allocation of the patients. Due to the different treatment applied for the intervention and control groups, the intervention personnel, project coordinator, neurologists, and patients could not be blinded.
Measurements
Every study participant in both groups gets a full assessment at baseline, after 12 and 24 months. The full assessment includes the collection of following data:
neuropsychological test series, Alzheimer's Disease Assessment Scale – cognitive subscale (ADAS-cog);
demographic data (gender, age, and education);
anthropometry (height, weight, and waist circumference);
medical history and risk factors (diabetes mellitus, hyperlipidemia, hypertension, cardiovascular diseases, and previous stroke);
stroke severity and activities of daily living [National Institutes of Health Stroke Scale (NIHSS), modified Rankin scale (mRS), and Barthel Index];
imaging results (CT or MRI);
lifestyle questionnaires (physical activity and diet);
quality of life (EQ-5D, 3 level) and depression scale [Center for Epidemiologic Studies Depression Scale (CESD)]; and
blood analysis.
From blood samples, the following parameters are carried out: C-reactive protein fibrinogen, glycated hemoglobin (HbA1c), glucose, triglycerides, total cholesterol, low-density lipoprotein-cholesterol (calculated), high-density lipoprotein-cholesterol, creatinine, blood urea nitrogen, aspartate aminotransferase, glu-tamatic pyruvic transaminase, gamma glutamyl transferase, and creatine kinase. Additionally, a two-hour oral glucose tolerance test is performed in nondiabetic patients. Apolipoprotein E geno-typing is performed.
Lipid values, HbA1c, and fasting blood glucose values are used to monitor the efficacy of the intervention program.
Safety
To ensure the safety of the participants and obtain information about adverse events (AEs), study neurologists are in regular phone contact with the participants. During the first year of follow-up, the investigator solicits and evaluates AEs every eight-weeks. During the second year of follow-up, possible AEs are detected every 16 weeks.
Description of the intervention
Over a period of 24 months, patients in the intervention group undergo an intensive intervention program to reach treatment goals according to current guidelines for treatment of ischemic stroke (31). Intervention starts as soon as possible after randomization. The priority lies upon interventions for which clinical trials or observational studies have shown beneficial effects on cognitive outcome measures. To check compliance with the treatment goals, the subjects of the intervention group keep a diary, where blood pressure, physical activity, food habits, and cognitive training are documented. The patients are called by the study center every month to inform about dates of the intervention sessions, to improve compliance, and to check adherence to the lifestyle recommendations.
Blood pressure control
Treatment of high blood pressure with antihypertensive drugs and regular self-monitoring of blood pressure are encouraged. Treatment goal is a blood pressure lower than 140/90 mmHg on at least 75% of self-recorded measurements. For patients with diabetes values lower than 130/85 mmHg were aimed. Participants have to record blood pressure in the diary at least twice a week; daily recording is recommended.
Physical activity
In the intervention group the goal is to perform moderate or vigorous physical activity at least three to five times per week. Participants of the intervention group participate in regular group meetings (six meetings during the first year and two meetings during the second year), which include general counseling, detailed instructions for exercises, and group activity planning. The patients are encouraged to participate in local activity groups in the participant's communities. Existing possibilities in the local communities are presented and individually recommended to the participants.
Diet
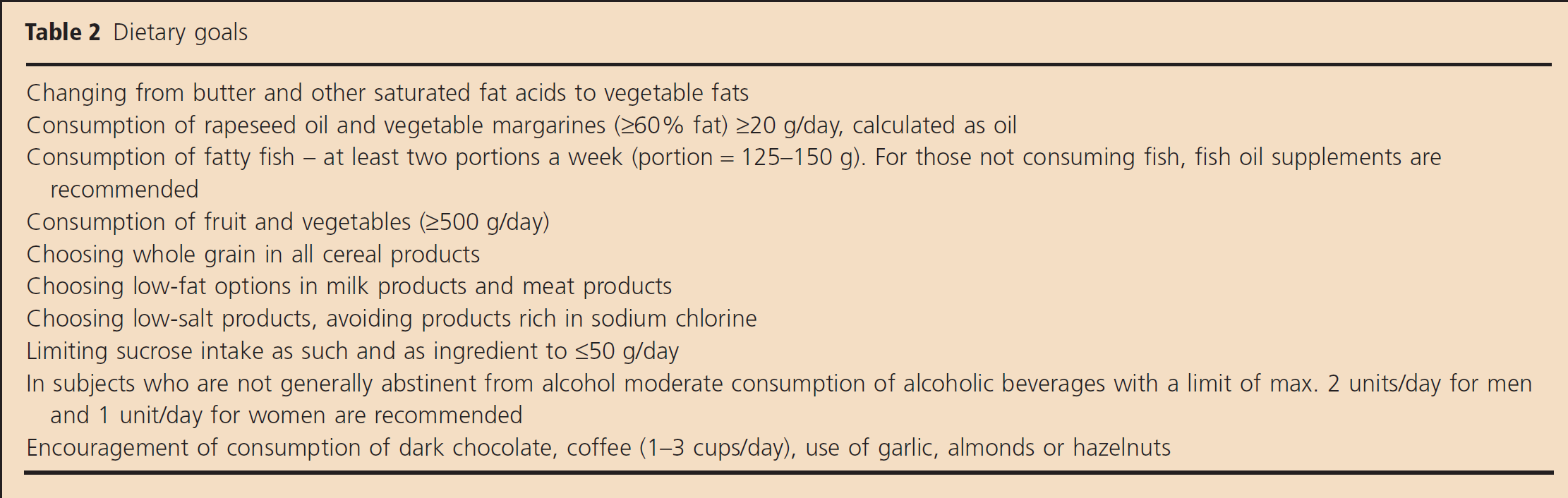
Dietary habits are evaluated at baseline during the first contact with the nutritionist. In obese individuals, weight reduction and the maintenance of at least 5% weight loss during the first year is targeted. Advices to modify the diet according to the nutritional goals (Table 2) are given during regular group and individual meetings (seven group meetings of 60 mins each and seven individual meetings of 30–60 mins each during the study period are recommended). Group meetings provide general information about nutritional basics similarly in all centers (fats, sugar, salt and cooking) and should motivate and support a healthy diet. Individual sessions aim at individual needs of the participant and should help to implement changes in diet as daily routine.
Dietary goals
Cognitive training
Participants have the opportunity to participate in cognitive training groups monthly. Training includes memory, reasoning, speed of mental processing, and attention. Participants are supplied with training material for training at home and are requested to bring the completed forms to the next session.
Other goals for lifestyle change
The patients who smoked are encouraged to stop smoking, and counseling is offered.
Compliance to medication
The pharmacological treatment is targeted to treatment goals of stroke prevention according to the European Stroke Organisation (ESO) guidelines (29). This includes the control of cholesterol with lipid-lowering drugs (preferably statins), blood pressure lowering drugs, and antithrombotic therapy in patients that are not eligible for oral anticoagulation. Patients with diabetes mellitus were treated according to current guidelines of the Austrian Association for Diabetes (33).
Patients of the intervention group receive regular phone calls from a study neurologist to improve adherence to medication and to secure compliance with the recommendations using a standardized questionnaire including questions about the current medication, blood pressure monitoring, and visits to a general practitioner. During the first year of follow-up, those phone calls are performed every eight-weeks, during the second year of follow-up every 16 weeks.
Control group
The patients in the control group obtain stroke care according to standard guidelines and advice for secondary prevention during hospitalization.
The patients get a full assessment at baseline, 12 months, and 24 months and receive regular phone calls to obtain AEs (every eight-weeks during the first year and every 16 weeks during the second year).
Primary outcome variables
The primary outcome is the change in cognitive decline at 24 months after randomization. Cognitive decline is defined as a significant decline in the composite scores of at least two of five neuropsychologically tested domains (executive functions, working memory, general memory, speed of cognitive processing, and visual spatial ability). Details of the neuropsychological test series are shown in the web table.
The second primary outcome variable is the change in ADAS-cog at 24 months after randomization compared with baseline.
Secondary outcome variables
The analysis of the secondary end-points includes cognitive decline and ADAS-cog at 12 months after randomization, mean composite scores of each cognitive domain at 12 and 24 months after randomization, composite outcome for vascular events, NIHSS, mRS, and Barthel Index at 12 and 24 months after randomization, quality of life (EQ-5D) index and depression (CESD) index at 12 and 24 months after randomization and all-cause mortality.
Data monitoring and safety body
Due to the small size of the study and the fact that no pharmacological treatments besides the recommended evidence-based drugs are used, no data monitoring committee was assembled. A clinical trial manager collects data on AEs, whether or not considered to be associated with medication used or lifestyle intervention, documents and reports them to an independent safety committee.
Sample size calculation
One-third of patients with lacunar stroke were previously found to show cognitive decline three-months after acute stroke (34). Up to 66% (depending on the instruments and criteria used) of stroke patients have mild cognitive impairment three months after stroke (4,5). It is however unclear in how many of these cognition had declined as a result of the stroke event. Therefore, we assumed that 50% of stroke patients show a cognitive decline at two-years after stroke. Randomized controlled trials testing the effect of antihypertensive drug treatment on cognition found a relative risk reduction for cognitive decline in four-years of 19% (21), of 25–55% for dementia (22,27), and 59% for ‘change in cognition’ (23). The cardiovascular risk reduction after eight-years in an intensive multifactorial trial found an absolute risk reduction of 20% and a hazard ratio of 045–0·5 (35). Therefore, we assumed a relative risk reduction of 40% in the present trial.
Assuming an incidence of cognitive decline at 24 months of 50% and a relative risk reduction of 40%, i.e. 30% cognitive decline in the intensive multifactorial intervention group, sample size calculations for detecting a significant effect at the two-side level of P = 0·05 with a power of 0·8 showed that 93 patients for each of the two groups would be needed; i.e. a total of 186 patients. As we have a clear direction for our hypothesis (we may exclude the possibility that active lifestyle intervention increases the risk of cognitive impairment), we may also use a one-sided level of P = 0·05, which reduces the number to 74 patients for each of the two groups; i.e. a total of 158 patients would be sufficient. After considering the fact that some patients will drop-out, we concluded that 200 randomized patients should be sufficient to detect an above-mentioned effect of the intervention.
Statistical analysis
Statistical analyses were performed using SPSS (Version 19.0 for Windows, SPSS Inc., Chicago, IL, USA) and the statistical software R. Baseline data are presented as median and interquartile range (IQR), as mean and standard deviation (SD) or as percentages depending on the level of measurement.
To check for differences between the two groups, the χ2 or Fisher's exact test, the t-test and the Mann-Whitney U-tests were used, also depending on the level of measurement.
To test the primary hypotheses, an intention-to-treat analysis will be carried out.
A second-line analysis for supportive purposes will be performed for a per-protocol data set as an explanatory approach.
The primary outcome variable is cognitive decline at 24 months after randomization. For each of the five cognitive domains, standardized composite scores are calculated from the differences between baseline and 24 months in individual neuropsychological test results. Cognitive decline at 24 months after randomization is defined as a significant decrease of function in at least two out of five domains of the cognitive test battery. The alpha level for the decision is 0·05. Accordingly, the critical level for a single domain is the 0·076 quantile of the standard normal distribution, i.e. —1·43. This relatively rigorous and statistically relevant criterion was chosen to ensure that cognitive decline was not an artifact of the measurements.
The second primary outcome variable is the ADAS-cog. Both primary efficacy criteria will be tested by a regression analysis with cognitive decline/ADAS-cog at 24 months as dependent variable and study group, age, gender, education, and NIHSS as explaining variables. Each secondary efficacy criterion will be tested by a regression analysis with the respective criterion as dependent variable and study group, age, gender, education, and NIHSS as explaining variables.
Study organization and funding
The ASPIS trial is supported by a Grant from the NÖ Forschungs- und Bildungsgesellschaft m.b.H. (former Life Science Krems GmbH) with the Grant Agreement Number LS09–002.
The study is coordinated by the Danube University Krems and overseen by a Steering Committee, which consists of experts in the fields of stroke, neurology, and clinical trials. A clinical trial manager, who is in close collaboration with the Steering Committee, ensures that the trial is conducted in accordance to the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) Note for guidance on good clinical practice.
This study is registered at clinicaltrials.gov with the identification number NCT01109836.
Results
Recruitment
Five recruiting centers in Lower Austria participate in this study. Patient recruitment started in June 2010 and was completed in October 2012. Two hundred two patients met the inclusion criteria and signed the informed consent. Baseline assessment was completed for 190 patients. Three patients were excluded because baseline assessments have shown that these patients did not meet the inclusion criteria (one dementia diagnosis found in medical records, 2 MMSE < 24). Five patients withdrew from the study before the neuropsychological test series could be conducted. For another four patients, the neuropsychological test series was cancelled prematurely because their health and cognitive status did not allow the completion of the test series (one mentally unstable, one analphabet, and two aborted the testing by own will) (Fig. 1).
Baseline data
At baseline, the mean age of the study participants was 61·8 years (SD ± 94) and 29% were female. Patients were recruited 16 days after stroke onset on average, 73·5% of the patients were recruited within 21 days after stroke.
Of the participants, 92% were functionally unimpaired before stroke (mRS = 0). At recruitment, stroke-related impairment was low. The patients had a mean NIHSS score of 1·9 ± 1·8 and a median mRS of 1 (IQR 0–1). Cognitive impairment at inclusion was mild. The study population had a mean MMSE score of 28·8 ± 14. A history of ischemic stroke was found in 6·8% of the patients.
Regarding the risk factors for stroke, 79% had hyperlipidemia, 9·5% had atrial fibrillation, and 32% had diabetes. Hypertension was documented in the medical history of 784% of the patients, out of which 67% had blood pressure values of ≤140/90 at baseline while on current drug treatment.
According to World Health Organization classification (36), 31% of the women had a normal body mass index, 31% were overweight and 38% were obese, and in men 21%, 47%, and 32%, respectively.
At baseline, there were no significant differences in demographic, clinical, or lifestyle characteristics between the control and the intervention groups (Table 3).
Baseline characteristics
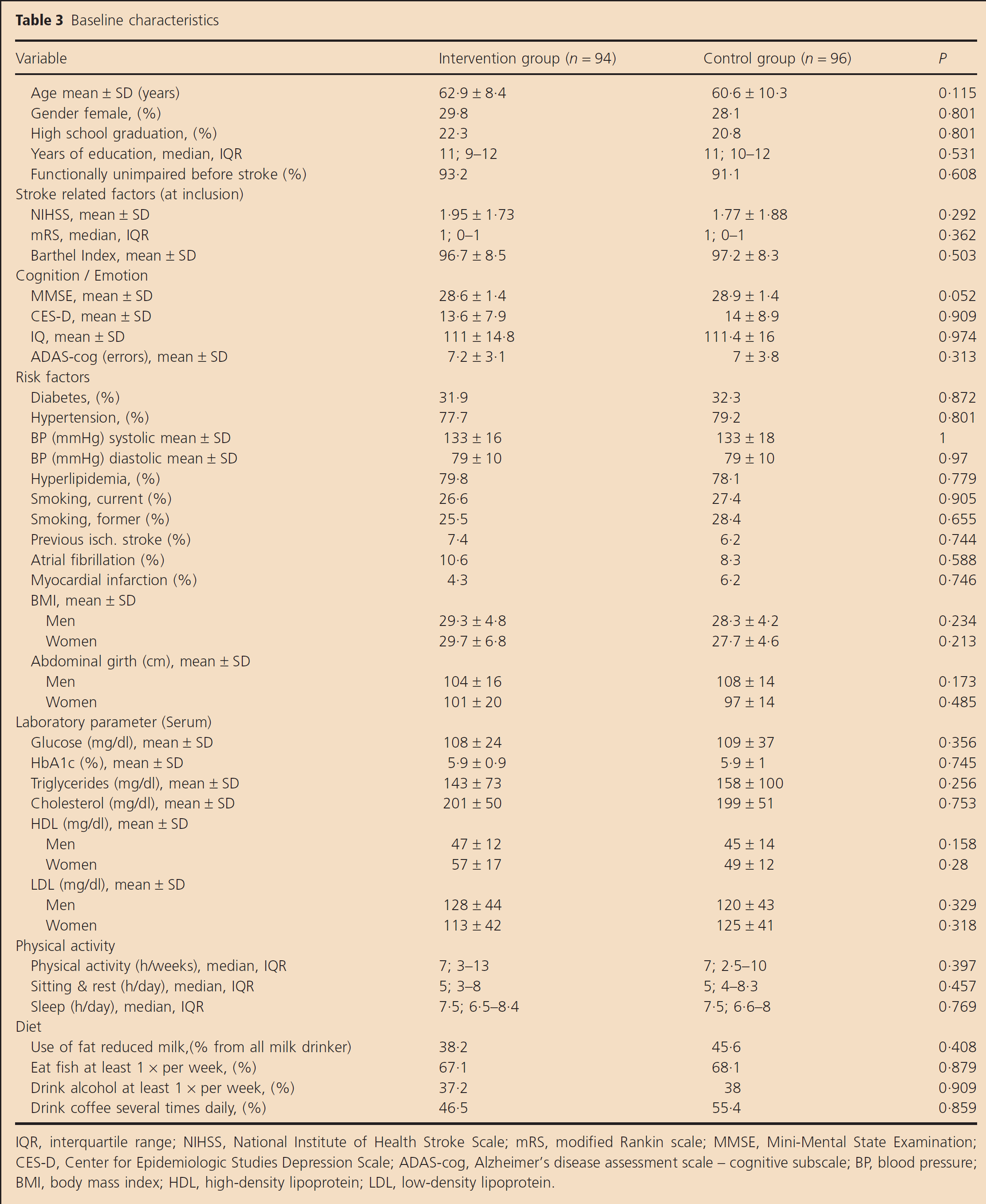
IQR, interquartile range; NIHSS, National Institute of Health Stroke Scale; mRS, modified Rankin scale; MMSE, Mini-Mental State Examination;
CES-D, Center for Epidemiologic Studies Depression Scale; ADAS-cog, Alzheimer's disease assessment scale – cognitive subscale; BP, blood pressure;
BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
We also compared the nine patients who dropped out before baseline cognitive tests could be finished with the overall study population. These nine patients had a higher systolic blood pressure, less hyperlipidemia, and shorter sleep; these findings are not secured. There were no differences in severity of stroke.
Discussion
Observational studies have shown that several modifiable vascular risk factors that increase the risk of stroke, and coronary heart disease are also associated with cognitive impairment and dementia (11–20). Although healthy diet, physical activity, weight control, effective control of high blood pressure, and dyslipidemia can be recommended in general for everybody, it is important to know whether these could help high risk individuals such as stroke survivors.
In this study, a multifactorial lifestyle intervention was applied. Pharmacological treatment was only prescribed according to the current guidelines as necessary, not as a part of the study. This design was chosen because all patients were screened for risk factors at baseline and received the appropriate medication according to the ESO guidelines (29). As adherence to medication in secondary prevention is often poor (37), regular phone calls are part of the intervention to ensure the adherence to the prescribed medication.
In this study, a follow-up of two-years with an interim follow-up of one-year was chosen to evaluate a trend over time and the long-term potential of a lifestyle intervention. We suggest that the intervention needs time to take effect and that group differences will increase over time. This could be one reason why the only published study that evaluated the prevention of cognitive impairment after stroke by lifestyle modifications could not prove its efficacy (30). The intervention group showed better results at the Trail Making Test and the 10-word test than the control group, but the group differences were not statistically significant. In the present study, we expect larger group differences because of a more intensive intervention treatment and a longer follow-up period.
Of the study population, 29% is female, which is less than the overall stroke population in the recruiting centers (47%, unpublished data of the Austrian Stroke Unit Registry). When the main inclusion criteria (age from 40 to 80 years, NIHSS 1–14, mRS 0–2 before stroke) are applied, the percentage of women in the registry is reduced to 36%. This shows that the distribution between the genders is representative and that the small difference in gender distribution may be caused by the fact that stroke in women occurs at a higher age.
Our goal was to recruit 80% of the patients within three-weeks after stroke onset. In spite of the fact that 22% of the patients were recruited in rehabilitation centers, where patients are admitted a few weeks after stroke onset, we almost reached our target with 73·4% recruited within three-weeks.
The main strength of this study is the use of an extensive neuropsychological test series. This test series consists of eight different sub-tests in the domains executive functions, working memory, general memory, speed of cognitive processing, and visual spatial ability. This test series was especially assembled by experienced neuropsychologists to be sensitive to cognitive changes over time in those cognitive domains, which are most frequently affected after stroke. Our experience has shown that the conduction of this test series with acute stroke patients is possible but requires a lot of effort from the patients to complete the test series. The less sensitive but commonly used ADAS-cog is used as second primary outcome to enable comparisons with other similar stroke trials.
There are also some limitations. Only patients with mild to moderately severe impairment were included (NIHSS 1-14) to ensure the applicability of a lifestyle intervention including physical activity. Therefore, the results may not be transferable to patients with severe stroke. Because no other comparable studies aiming at preventing cognitive decline after stroke by lifestyle interventions were found, we could not reliably compare our own sample size calculation. According to our pragmatic approach, a total sample size of 200 patients may be sufficient to prove the efficacy of our lifestyle intervention with a 40% relative risk reduction. If this study shows a positive trend but no significant difference between the two groups, it will help to specify the calculations and provide information for an extension phase of this study.
This study is one of four similar ongoing trials testing different interventions with cognition as primary end-point targeting multiple risk factors for vascular dementia simultaneously (31). The FINGER trial (NCT01041989) includes subjects at increased risk for developing dementia and the PreDIVA trial (38) includes healthy elderly subjects. Only the PODCAST trial (ISRCTN85562386) also includes subjects after ischemic stroke. Even if the participants receive lifestyle advice in the PODCAST trial, it focuses on the effect of intensive blood pressure lowering and/or intensive lipid lowering therapy on cognitive decline and dementia after stroke.
The present study will provide essential data about the feasibility and efficacy of lifestyle intervention after stroke and the extent to which such intervention may prevent the risk of cognitive decline in these high-risk patients. Larger international studies can follow to prove effects of a polyinterventional therapy including lifestyle modification on cognitive functions after stroke, using our experiences obtained in the ASPIS trial. This would extend evidence-based management of poststroke patients to more intensive lifestyle intervention aiming at preventing cognitive decline after stroke.