
Abstract
Background
Stroke is a leading cause of death and disability worldwide. Stroke burden is immense as it leads to premature deaths, leaves survivors with ongoing disabilities, and has a major financial impact on the individual, their families, and the community. Reliable, high-quality evidence is needed on stroke risk factors, incidence, and outcomes to provide information on how best to reduce this burden. Population-based studies are regarded as the ‘gold-standard’ of measuring disease burden but are not common due to the logistical and financial challenges they present. The Auckland Regional Community Stroke Studies are among a few in the world that have been carried out at a population level and at regular intervals.
Aim
The aim of the fourth Auckland Regional Community Stroke Studies IV is to examine the current measures of stroke incidence, prevalence, and outcomes as well the trends over four decades. This article describes the methodology of the Auckland Regional Community Stroke Studies IV with stroke and transient ischemic attacks cases registered over a 12-month period from March 1, 2011 to February 29, 2012.
Conclusions
The methodology described may be used as a guide in order to design similar population-based stroke incidence and outcome studies in other countries and populations, thus facilitating the collection of most consistent and accurate stroke epidemiological data.
Introduction
Stroke is the second most common cause of death and a frequent cause of adult disability worldwide (1,2). Stroke burden on families and society is projected to rise from ≈38 million disability-adjusted life year (DALYs) lost globally in 1990 to 61 million DALYs in 2020 (3) due to population aging. Lifetime costs per stroke patient range from US$60 000 to US$230 000 (4). Stroke has a large physical, psychological, and financial impact on patients and their families, the healthcare system, and society (4,5). Reliable methods of surveillance are crucial to accurately measure the incidence, outcomes, and burden of stroke.
The criteria for ‘ideal’ population-based studies are described by Sudlow and Warlow and others (6–8). There have been three previous population-based stroke incidence and outcomes studies in Auckland, New Zealand, covering a period of 30 years (1981–2003) (9–11) and several population-based studies worldwide (12–20) contributing to current knowledge on secular trends in stroke incidence and the burden of stroke. However, few such population-based stroke incidence and outcome studies have been carried out in an ethnically diverse population and even fewer examining trends over a 30-year period.
Population-based studies of transient ischemic attack (TIA) incidence (21) and outcomes are also uncommon. TIA is an important risk factor for stroke, with approximately 25% of people with ischemic stroke (IS) having a preceding or warning TIA (22,23). It is also important to determine the impact on stroke incidence and outcome of the increasing use of antithrombotic, antihypertensive and lipid-lowering medications, and surgical intervention in patients with internal carotid artery stenosis in the last 10 years.
Population-based studies are essential for accurately identifying the incidence and burden of stroke and TIA for evidence-based healthcare planning, resource allocation, and evaluating effectiveness of preventative strategies in the population. Hospital-based studies are not able to capture cases in the community that are not referred to hospitals, and therefore do not capture ‘true’ incidence of stroke and TIA. Data on population trends in stroke case fatality and functional outcomes are also needed to plan stroke services given high healthcare costs. In addition, health and health service access inequalities among socioeconomic and ethnic groups that are a key public health concern (10,24–29) can be evaluated by such studies. There are also notable gender and ethnic disparities in stroke incidence and outcomes in NZ (10,30–34) and elsewhere (35–38) that can best be studied in a population-based context. Given the growing numbers in the most stroke-prone groups (the elderly), as well as the existing ethnic disparities in stroke burden, accurate and representative population-based data are also crucial.
This article aims to describe the methodology involved in the day-to-day running of a large population-based epidemiological study of stroke incidence and outcomes. We include information about the actual procedures and other information generally not included in reports of population-based studies as practical advice for future researchers who wish to conduct studies of a similar nature.
Aims
The six main objectives of the ARCOS IV study are to:
determine the ‘true’ incidence, causes, and outcome of stroke and TIA in an ethnically diverse population;
provide an evidence base for healthcare planning across the care spectrum
evaluate the need for, and impact of, preventative/management strategies;
address persistent uncertainty about what key factors impact stroke recovery in NZ;
examine the natural course of recovery poststroke and TIA, particularly for cognitive and behavioral outcomes; and
identify service gaps/unmet needs to ensuring evidence-based policy, resource allocation, as well as prevention planning.
Methods
Definition of stroke and TIA
Stroke, according to the World Health Organization (WHO) definition, was defined as ‘rapidly developing clinical signs of focal (or global) disturbance of cerebral function, with symptoms lasting 24 h or longer or leading to death, with no apparent cause other than of vascular origin’ (39). This definition includes IS, primary intracerebral hemorrhage (PICH), and sub-arachnoid hemorrhage (SAH), but excludes cases of ‘silent stroke’ detected by neuroimaging, without appropriate clinical signs and symptoms. TIA was defined by the WHO as an acute loss of focal cerebral or ocular function with symptoms lasting less than 24 h and which after adequate investigation, was presumed to be due to embolic or thrombotic vascular disease.
Target population
The target population covered the well-defined geographical area of the Auckland region, situated in the North Island and the largest city New Zealand (Fig. 1) with a population of just over one million people aged 16 years and older (40). The regional boundaries of Auckland were changed in 2010, however, for consistency of comparison; ARCOS IV used the same boundaries as those used in previous ARCOS studies.

Map of the world showing geographical location of New Zealand.
Case ascertainment
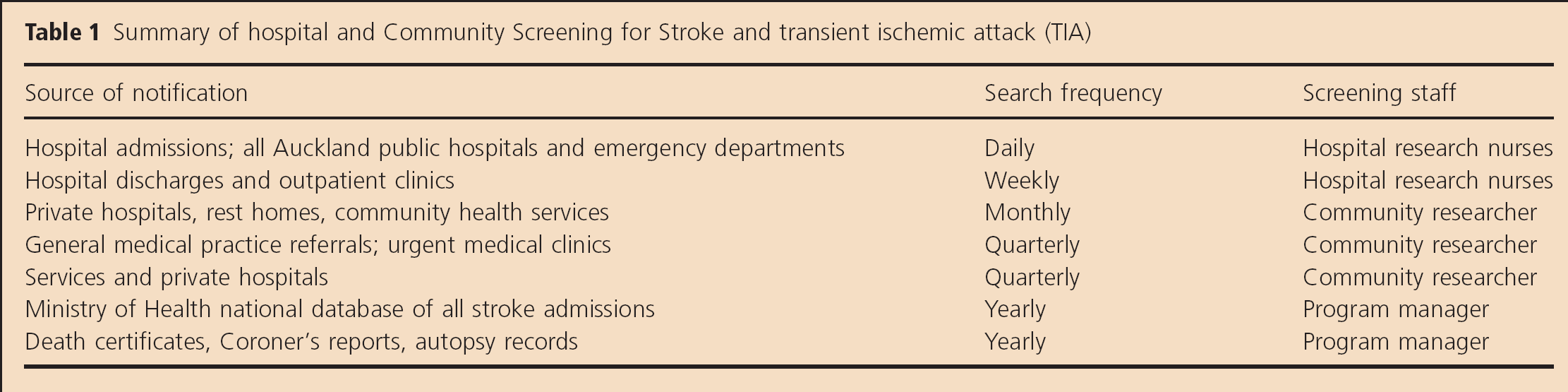
There are three main inclusion criteria: (1) incident stroke between March 1, 2011 and February 29, 2012; (2) resident of Auckland Region; and (3) ≥16 years. Complete case ascertainment is assured by multiple overlapping sources of information (Table 1) on all new hospitalized or nonhospitalized cases [‘hot-pursuit’ method (41)]. Admissions data of all four Auckland region public hospitals are searched on a daily basis for records of patients with symptoms indicative of a diagnosis of stroke or TIA. Additional weekly checks of hospital discharge and outpatient clinics are undertaken for stroke and TIA cases meeting the inclusion criteria. Regular checks of private hospitals, rest homes, and community health services (general medical practices, rehabilitation centers, and outpatient clinics) are made to capture nonhospitalized cases. Autopsy reports, death certificates (from registrar of births, deaths, and marriages), and coroner's reports for Auckland residents are cross-checked to identify people who had died with any mention of stroke in the record. New Zealand Health Information Systems data from the New Zealand Ministry of Health of all fatal and nonfatal stroke/TIA cases in the study population (‘cold-pursuit’ methods) will also be examined. All residents meeting the inclusion criteria but with stroke or TIA that occurred outside the Auckland Region are also included. Those people with stroke or TIA that occurred in the Auckland region but with usual residence outside the Auckland Region are excluded.
Summary of hospital and Community Screening for Stroke and transient ischemic attack (TIA)
Publicizing the study
In order to increase general awareness of the study and to enhance recruitment, medical personnel in stroke wards were informed about the study in the form of formal meetings as well as in writing. This enabled the ward staff to communicate with individuals regarding the study and refer potential cases to ARCOS IV researchers. Potential participants and their family members are provided with color brochures outlining the study, with contact details of researchers. In addition, all general practitioners (GPs) in the Auckland region are contacted by letter or e-mail and informed of the study. They are also asked to refer any stroke or TIA cases to ARCOS IV staff. A remuneration incentive is offered to doctors for any cases that were not otherwise identified by the ARCOS IV researchers.
Confirmation of stroke/TIA diagnosis
A diagnostic review committee comprising three stroke neurologists and a stroke physician meet fortnightly to confirm the diagnosis of TIA, stroke, and classification of all ischemic cases. The committee use medical history, hospital discharge summaries, clinical and laboratory findings (including vascular and cardiac imaging), or necropsy results when available. Stroke is divided into pathological types (IS, PICH, and SAH). Cases without imaging or pathological necropsy confirmation of sub-type are classified as stroke of undetermined type. All first-ever and recurrent new strokes (any new stroke event 28 days after the index stroke) during the study period are registered. The strokes are grouped by clinical criteria according to the Oxfordshire Community Stroke Project classification as total anterior circulation infarct, partial anterior infarct, lacunar infarct, or posterior circulation infarct (42,43). ISs are also grouped into five causal sub-types (large artery, cardioembolic, small artery, and other determined and undetermined) based on the Trial of ORG 10172 in Acute Stroke Treatment criteria (44,45). SAHs are classified into those with and without cerebral aneurysm. We also differentiated TIA with and without head computed tomography or magnetic-resonance imaging evidence of clinically relevant brain infarction.
Stroke/TIA incidence and outcomes
The study was given ethical approval by the Northern X Regional Ethics Committee (Approval number NTX/090/10) and the Auckland University of Technology Ethics Committee. The incidence of all first-ever recurrent strokes, TIAs, and all deaths is recorded for all individuals that met the inclusion criteria. The study has ethical approval to include de-identified information from all stroke/TIA patients, and this de-identified medical information available from hospital records is obtained for all stroke and TIA cases. Baseline demographic information is captured for all eligible participants. Serious adverse events, and case fatality information, is obtained from medical records for subsequent hospitalization, reports from family members when contacted for follow-up, the National Death Registry, or coroner's reports.
Informed consent
As soon as possible after stroke, the person with a stroke/TIA or a proxy is approached for informed consent to participate in the study. A proxy is used when the person is unable to provide informed consent. Families of people receiving comfort or palliative care are not approached. A detailed patient information sheet is included with consent form. Study researchers are available on-site at the hospital wards to explain the study and answer any questions patients or the families had about the study. Interpreters were available for non-English speakers to both explain the study and assist in follow-up assessments. Patient information sheets were also translated into Samoan, Tongan, and Mandarin languages to increase accessibility of study information for patients and family members with limited English. Cultural differences are acknowledged when approaching patients and families, and feedback from cultural advisors from the Maori and Pacific Island communities is acted upon by the research staff. Participants are also informed that they may withdraw their participation from the study at any time.
Follow-up assessments for outcomes
Outcome assessments are conducted at baseline, 28 days, six-months, and 12 months from the incident stroke (Fig. 2). Outcome assessments for ARCOS IV are due for completion by March 2013. Three modes of data collection for study questionnaires are being utilized: telephone, self-completion, and face-to-face with a study researcher (Table 2). This allows assessments to be broken up into smaller and more manageable portions in order to reduce participant burden and fatigue. The clinical researchers conducted the face-to-face interviews at the participant's preferred time and location for participant convenience.
Types and description of case record forms
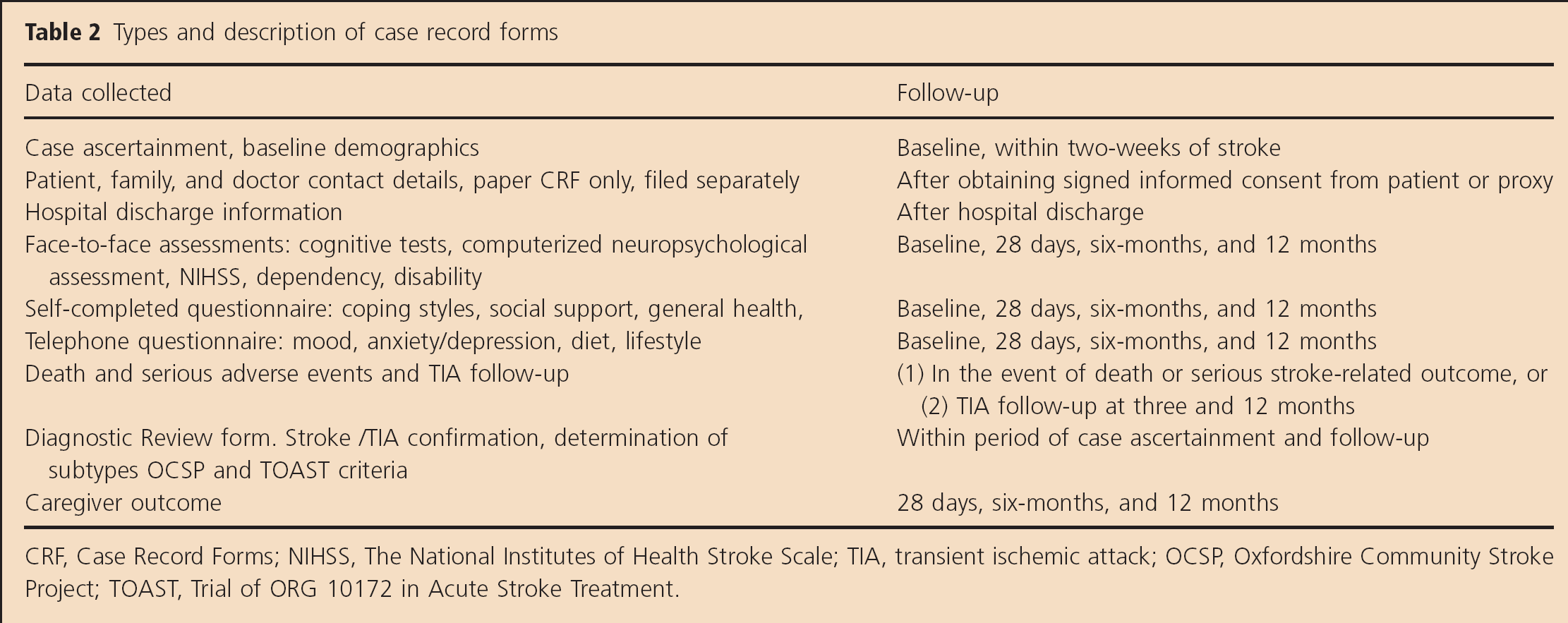
CRF, Case Record Forms; NIHSS, The National Institutes of Health Stroke Scale; TIA, transient ischemic attack; OCSP, Oxfordshire Community Stroke Project; TOAST, Trial of ORG 10172 in Acute Stroke Treatment.
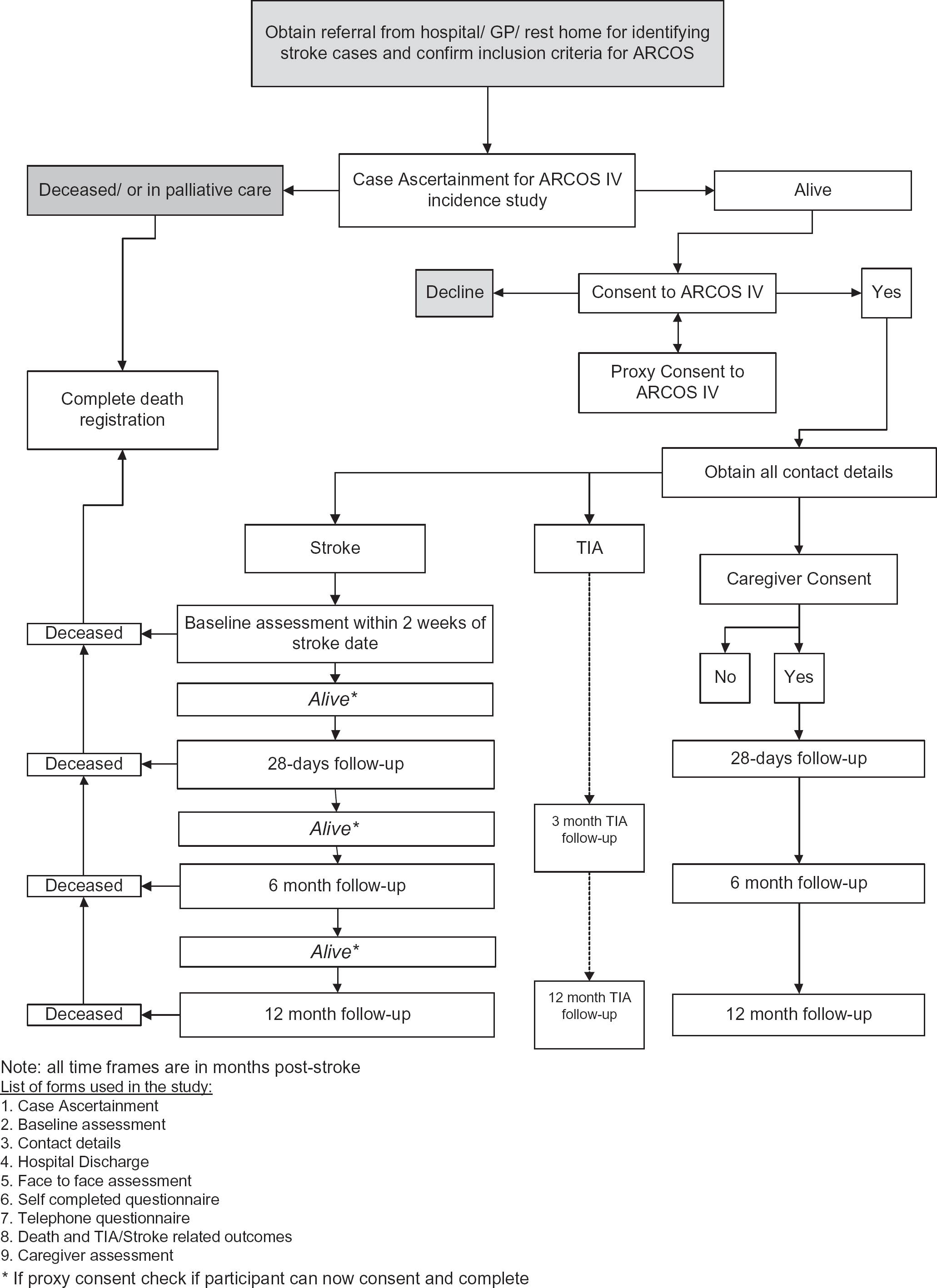
Flowchart of study procedures.
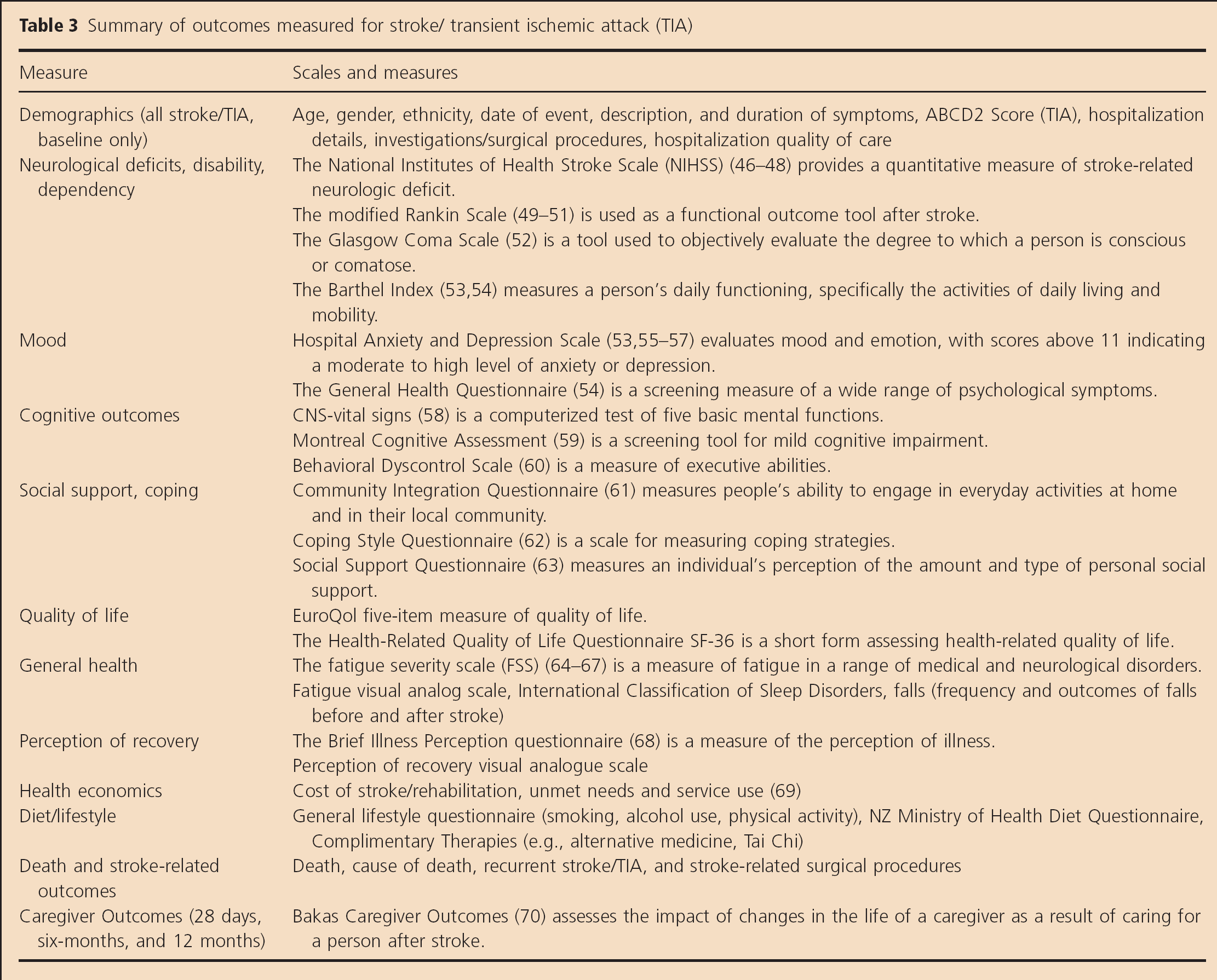
Baseline variables include sociodemographics, history of the stroke, medical and neurological history, family history, risk factor profiles, and results of routine cardiovascular and neurological examinations are also collected. Assessment of the patient's premorbid disability and a functional and self-care assessment are also conducted. To allow comparison of stroke outcomes over time, all major outcome measures used in the previous ARCOS studies (11) will be included (see Table 3). Assessments are completed with the aid of a proxy for participants who are unable to complete the assessments.
Summary of outcomes measured for stroke/ transient ischemic attack (TIA)
Caregiver outcomes
After obtaining consent, participants are asked if they wished to nominate a caregiver (a person they considered to be their main caregiver following the stroke) who could be approached to participate in the study to evaluate the impact of stroke on caregivers. Caregivers that consent to participate in the study complete questionnaires at 28 days, six-months, and 12 months.
Data capture and database management
All participants in the study are being allocated a unique registration number electronically generated by the data management team, which will be used to identify participants throughout the study. Data from case ascertainment and all assessments are being captured on paper case record forms initially, and then entered into electronic case record forms via a secure, password-protected, web-based database. Information about patient contact details is captured on paper only and securely filed separately. Paper copies of hospital discharge summaries, imaging, and other relevant medical information is de-identified and secured to paper case record forms for filing.
Mental health screening
During follow-up, all participants are screened for anxiety and depression using the Hospital Anxiety and Depression Scale and suicide risk using the General Health Questionnaire 28. In situations where the participant is deemed to be at serious risk of harm, a referral is made to the participant's doctor or the emergency mental health team was contacted. If there is no immediate risk of harm identified but high levels of anxiety or depression are recorded or thoughts of suicide are present, permission is sought for the researcher to contact the participant's GP or health care provider and the study operations group is notified.
Recruitment staff and training
Throughout the course of the study, a number of clinical researchers were employed on the ARCOS study. The clinical researchers were required to have some healthcare experience, and to attend an initial formal training session. They were closely supervised for several weeks to ensure consistent administration of the assessments. All clinical researchers completed the National Institute of Health Stroke Scale training certification (available online at http://www.nihstrokescale.org/) before proceeding with assessments. Feedback is provided on completed paperwork by study managers, and regular team meetings were held throughout the study to ensure the study protocol was adhered to or to share any difficult experiences or useful strategies. The team meeting also helped to ensure consistency of interview delivery among the team. Ongoing training in specific areas is provided to the team when there is a need for it, such as how to engage and work with people experiencing suicidal thoughts, how to deal with bereavement, and how to work with participants experiencing high levels of anxiety and depression. In addition to this, refresher training on the administration of the assessment measures is undertaken periodically throughout the study.
All clinical researchers are provided with a mobile phone to maintain contact with participants while working outside of the study offices and for personal safety reasons. To ensure that the study manager was aware of where researchers were for their appointments (in case of emergency), an electronic calendar booking system was established. The clinical researchers are also provided with a laptop computer and Internet access for the administration and scoring of assessments. This also facilitates communication and assists the study managers with the substantial organizational skills required to manage a considerably large research team.
Discussion
The ARCOS IV study utilizes an accepted (standard) population-based approach for complete case ascertainment for stroke and TIA incidence and outcomes. The city of Auckland has favorable characteristics to conduct a population-based epidemiological stroke study (6,7), four large public hospitals with access to emergency services and imaging, a well-defined geographical area, and an ethnically diverse population. The ARCOS IV study is conducted with the same methodology as the previous ARCOS studies with additional elements added to widen the breadth of information on stroke incidence and burden. One of the most significant additional elements incorporated was the capture of the incidence and outcomes of TIA. For the first time within the series of ARCOS studies, the complete case ascertainment of TIA will be carried out at a population level. The paucity of population-based studies of TIA may be due to the low rate of hospital admissions and the lack of follow-up for significant periods of time. While most TIA cases are likely to be identified via hospital admission information, regular and thorough searches of outpatient clinics are being carried out to capture TIA cases not presenting to an emergency department. Importantly, TIA patients who consent to participate in the study will be followed up after the index event, allowing the recording of the incidence of recurrent TIAs and other stroke-related events.
ARCOS IV also includes outcome assessments at 12 months post the index stroke or TIA. This will allow the measurement of longer term comparison for all outcomes assessed at baseline, 28 days, and six-months (stroke only) after stroke/TIA as well as calculation of one-year case-fatality rates.
The addition of extensive neuropsychological assessments is a distinctive feature of ARCOS IV. There is a lack of population-based data on neuropsychological outcomes after stroke (71). A long-term follow-up study of participants from the previous ARCOS III study has shown that a significant proportion of stroke survivors experiences neuropsychological deficits (72). ARCOS IV will measure cognitive impairment across all neuropsychological domains using a battery of cognitive tests including computerized assessments. The computerized assessments are initiated at 28 days poststroke when participants have undergone a period of recovery, then repeated at six- and 12 months to capture temporal changes.
It has been recognized that the health and well-being of the caregiver of the person with the stroke are often adversely affected (73). ARCOS IV not only includes assessments of caregiver outcome both in the short term as done in previous ARCOS studies but also repeats the outcome assessment at six- and 12-month time-points.
Finally, the population-based approach provided a robust sampling frame for two linked studies: (1) a randomized clinical trial to test the effectiveness of motivational interviewing and (2) a qualitative study on life experiences after stroke. The methodology of these is described elsewhere (74,75).
There are still areas of the world where crucial information on stroke incidence is lacking; similar population-based studies will form the basis for policies to reduce stroke burden worldwide. The detailed methods used in ARCOS IV could serve as a ‘guide’ for researchers wishing to design future comparable population-based studies of stroke incidence and outcomes.
Footnotes
Acknowledgement
The authors wish to acknowledge the contribution of the study participants, the ARCOS IV research assistants, and the medical staff at all the Auckland public hospitals.