
Abstract
Background and rationale
The increasing use of oral anticoagulants, mostly to prevent ischemic stroke due to atrial fibrillation in an ageing population, has been associated with a fivefold increased incidence of oral anticoagulant-associated intracerebral hemorrhage: a rare, serious, and unpredictable complication. We hypothesize that cerebral microbleeds and other markers of cerebral small vessel disease on magnetic resonance imaging, and genetic polymorphisms (e.g. influencing cerebral small vessel integrity or anticoagulation stability), are associated with an increased risk of oral anticoagulant-associated intracerebral hemorrhage, with potential to improve risk prediction.
Aims
(1) To determine the incidence, clinical, radiological, and genetic associations of oral anticoagulant-associated intracerebral hemorrhage in a prospective, multicentre cohort study of patients with atrial fibrillation-related ischemic stroke or transient ischemic attack started on oral anticoagulants; (2) To investigate characteristics of oral anticoagulant-associated intracerebral hemorrhage compared with non-oral anticoagulants related intracerebral hemorrhage in a prospective study.
Design and methods
Study 1: Prospective, multicentre, inception cohort study of 1425 adults started on oral anticoagulants (including vitamin K antagonists and the nonvitamin K oral anticoagulants) after recent ischemic stroke and concurrent atrial fibrillation. Participants will have standardized brain magnetic resonance imaging (including a T2*-weighted gradient-recalled echo sequence) and DNA sample collection at baseline, with two-year follow-up by postal questionnaire and medical records surveillance for symptomatic intracranial hemorrhage, other serious vascular events, and death. We will compare the rates of symptomatic intracranial hemorrhage (primary outcome; subclassified as intracerebral, subdural, extradural, intraventricular), other vascular events, and death (secondary outcomes) in participants with one or more cerebral microbleeds to the rates in those without cerebral microbleeds. Study 2: Prospective case-control study of oral anticoagulant-associated intracerebral hemorrhage compared with non-oral anticoagulant-associated intracerebral hemorrhage to investigate genetic, clinical, and radiological associations with oral anticoagulant-associated intracerebral hemorrhage. In participants with intracerebral hemorrhage (including at least 300 with oral anticoagulant-associated intracerebral hemorrhage), we will collect a DNA sample, standardized clinical data and routine brain imaging (magnetic resonance imaging or computed tomography), and information on functional outcome.
Expected outcomes
We will identify the factors associated with increased intracranial hemorrhage risk after oral anticoagulants for secondary prevention after ischemic stroke due to atrial fibrillation. We will determine clinical, radiological and genetic factors, and clinical outcomes associated with oral anticoagulant-associated intracerebral hemorrhage.
Keywords
Introduction and rationale
Oral anticoagulants [OACs, including warfarin and nonvitamin K OACs (NOACS)] are effective in reducing the relative risk of future ischemic stroke in people with atrial fibrillation (AF) by over 60% (1). The most feared of all bleeding complications of OAC is intracranial hemorrhage [bleeding within the skull, of which ∼70% are intracerebral hemorrhage (ICH), i.e. bleeding within the brain substance] (2). OACs are used increasingly in an ageing population; there has been a fivefold increase in the incidence of OAC-associated ICH (OAC-ICH) in population-based studies (3–5), so that it now accounts for about 15% of all ICH (3).
People with ischemic stroke due to AF are at high risk of future ischemic stroke, but paradoxically, they may also have the highest risk of ICH (1). Concern over bleeding risks may account for low rates of anticoagulation for AF in recent studies (6,7). A key research goal in stroke medicine is to improve judgment of the risks and benefits of anticoagulation to increase the use of OAC and allow personalized, safe, and effective stroke prevention treatment.
Magnetic resonance imaging (MRI) can provide detailed information about cerebral small vessel disease, a strong candidate risk factor for OAC-ICH. Potential markers of small vessel disease include subcortical infarcts (including lacunes), white matter hyperintensities of presumed vascular origin (sometimes termed leukoaraiosis), and cerebral microbleeds (CMBs) (8). CMBs - small rounded hypointense lesions seen on blood-sensitive MRI sequences - are hypothesized to be a marker of bleeding-prone small vessel diseases, with high future risk of ICH (9). Genetic variants related to cerebral small vessel integrity or anticoagulant metabolism could also influence the likelihood of ICH during anticoagulation. The Clinical Relevance of Microbleeds in Stroke (CROMIS-2) study is a multicentre prospective UK study designed to determine whether MRI markers of small vessel diseases, and genetic factors, are related to the risk of intracranial hemorrhage (including ICH), other vascular events, or death during oral anticoagulation (OAC) after ischemic stroke associated with AF.
AF and OAC
AF causes up to about 20% of all ischemic strokes, with a lifetime risk of one in four men and women over the age of 40 (10,11). It affects about 12% of people over the age of 75 and is more common in ageing populations (11). Untreated, AF increases the overall risk of stroke fivefold, with the highest risk in elderly patients with previous stroke or transient ischemic attack (TIA) (11). OAC reduces ischemic stroke risk by about 65% in patients with AF, but this benefit has to be balanced against an increased risk of intracranial hemorrhage, including ICH. ICH is the most feared complication of OAC, causing death or severe disability in up to 75% of patients (12). Although RCTs suggest that the rate of symptomatic ICH in anticoagulated patients is low (particularly with the use of NOACs), RCTs may not be generalizable to populations given these drugs in routine clinical practice, and are not designed or powered to investigate predictors of rare adverse events (13,14). A recent observational inception cohort study of patients treated with OAC (of whom a quarter had a previous history of stroke) reported a 2.5% (95% CI 1.1-4.7%) risk of ICH at one-year (15).
Because OAC-related ICH is so often fatal or disabling, even a small increase in the absolute risk of ICH of only 1-2% per year could modify the net benefit of OAC treatment (16). Clinical risk factors for OAC-related bleeding (including ICH) include increasing age, previous ischemic stroke, and intensity of OAC. However, these are not sufficiently reliable for clinical decision making (1), and overlap strongly with the risk factors for ischemic stroke, so it remains extremely difficult to balance the risks and benefits of OAC in practice.
Cerebral small vessel disease, CMBs, and ICH risk
Neuroimaging can identify biomarkers of the presence and severity of age-related cerebral small vessel diseases, including cerebral amyloid angiopathy (CAA) and disease of the deep perforating arteries (often termed hypertensive arteriopathy), which may predispose to ICH in elderly patients treated with OACs (17). CMBs are a key MRI marker of small vessel disease and potential predictor of future stroke including ICH (14,18). CMBs are small, rounded, hypointense lesions on blood-sensitive MRI sequences, including gradient-recalled echo T2*-weighted MRI (T2*-GRE) and susceptibility-weighted imaging (SWI) (9,19). Radiologically defined CMBs correlate pathologically with small collections of blood-breakdown products (in particular, hemosiderin-laded macrophages) adjacent to small vessels mainly affected by hypertensive arteriopathy (including lipohyalinosis and arteriolosclerosis) or CAA (20–22). Hence, CMBs are a promising new marker for bleeding-prone arterial pathology affecting cerebral small vessels (19). CMB distribution in the brain parallels the underlying small vessel disease: strictly lobar (cortical-subcortical) CMBs are characteristic of CAA, with high specificity for CAA when used according to the Boston criteria (23), while deep CMBs likely reflect hypertensive arteriopathy (9,17,19). A mixed pattern of CMBs may reflect either severe widespread hypertensive arteriopathy or a combination of CAA and hypertensive arteriopathy.
CMBs are common in the populations likely to be exposed to OAC (24): They are found in about 30% of patients with ischemic stroke, up to 40% of the healthy population over the age of 80 (25,26), and 60% of patients with ICH (27). CMBs are associated with an increased risk of ICH in patients with previous ischemic stroke or ICH (28). A recent systematic review of case-case comparisons of 1460 patients with ICH and 3817 patients with ischemic stroke or TIA showed that CMBs are more common in warfarin-related ICH than nonwarfarin-related ICH (OR: 2.7; 95% CI: 1.6-4.4; P < 0.001) (18).
There are only limited prospective studies of CMBs, including patients with ischemic stroke (29–31), ICH (32,33), or healthy elderly individuals (34). The largest prospective cohort of CMBs and antithrombotic use included 908 patients with ischemic stroke, treated with a single antithrombotic agent (93% with aspirin) (30). During a mean follow-up of 26 months, the risk of ICH was 0.6% in patients with no CMB, 1.9% in patients with one CMB, 4.6% in patients with two to four CMBs, and 7.6% in patients with five or more CMBs (P < 0.001) (30). Overall, 15/908 (1.7%) patients suffered ICH at an average follow-up time of 27 months; of patients with CMBs, 4.4% developed ICH, while 0.6% of patients without CMBs developed ICH (30), giving a relative risk of CMBs on ICH of 7.3 (4.4/0.6). However, the findings from this Asian cohort may not be generalizable to other populations: CMBs were detected in 27.8% of the patients, most commonly in deep brain regions (e.g. basal ganglia and thalamus), suggesting that hypertensive arteriopathy was the main small vessel pathology. A recent systematic review and meta-analysis pooled data from 10 cohorts including 3067 patients with ischemic stroke or TIA, and found that (35) CMBs were associated with an increased risk of recurrent stroke (OR: 2.25; 95% CI: 1.70-2.98; P < 0.0001), but especially symptomatic ICH (OR: 8.52; 95% CI: 4.23-17.18; P = 0.007). However, in Caucasians, the OR for CMB presence on ICH risk was 3.9 (95% CI 0.91-16.4), while in Asian cohorts, it was 10.4 (95% CI 4.6-23.7) (35). The systematic review found no large prospective studies of CMBs in ischemic stroke Caucasian cohorts treated with anticoagulants for AF.
CMBs are being found more often with the increasing use of MRI in stroke patients (22). The clinical relevance of CMBs for ICH risk needs to be clarified to avoid patients being denied effective treatment due to concerns regarding CMBs; conversely, if patients at very high bleeding risk could be identified, they could have individualized antithrombotic treatment or alternative ischemic stroke prevention methods (e.g. left atrial appendage occlusion devices) and be spared the devastating yet potentially avoidable hazard of ICH related to long-term anticoagulation.
Rationale for the research questions
Because OAC-ICH is associated with increased age, and often occurs with anticoagulation intensity within the therapeutic range (36), the mechanism may be related to individual patient factors, for example, age-related cerebral small vessel disease, such as CAA or disease of the deep perforating arteries (sometimes termed hypertensive arteriopathy) (37–41). Moreover, some studies suggest that white matter abnormalities of presumed vascular origin - confluent deep white matter abnormality seen as low attenuation on computed tomography (CT) or hyperintensities on T2-weighted MRI – increase the risk of OAC-ICH (42,43). Because CMBs provide evidence of leakage of blood from pathologically fragile small vessels (44), we hypothesize that CMBs may be an independent predictor of OAC-ICH. There is also increasing interest in genetic factors that might predispose to OAC-ICH, with two plausible mechanisms: First, some genes may influence the sensitivity to OAC and stability of anticoagulation (45), and second, other genes may make cerebral small vessels more likely to bleed by affecting the integrity of the arterial wall (46).
Research questions
Study 1: CROMIS-2 AF
What is the incidence of OAC-associated intracranial bleeding (subclassified as intracerebral, subdural, extradural, intraventricular, and subarachnoid) in a multicentre, prospective, inception cohort study of patients with recent ischemic stroke anticoagulated for nonvalvular AF? Are CMBs (or other markers of small vessel disease) associated with the future risk of symptomatic OAC-related intracranial hemorrhage (subclassified as intracerebral, subdural, extradural, intraventricular, and subarachnoid)? Are CMBs (or other markers of small vessel disease) associated with an increased risk of other vascular events (including recurrent TIA and ischemic stroke) or death? Can our findings be used to develop a risk model for OAC-related intracranial hemorrhage?
Study 2: CROMIS-2 ICH
Are genetic, clinical, or radiological risk factors associated with OAC-ICH or functional outcome after ICH? What are the clinical and radiological characteristics of OAC-ICH (including those associated with warfarin or NOACS)?
Methods
Patient population, sample size, and study design
Study I (AF): observational inception cohort study (n ≥ 1425) of patients started on OAC (without prior anticoagulant use and timing dependant on treating physician) for presumed cardioembolic stroke due to nonvalvular AF with follow-up for the occurrence of ICH, other vascular event including ischemic stroke, for an average of two-years. Our main baseline exposures (risk factors of interest) are the presence of CMBs and other markers of small vessel disease on MRI, and genetic polymorphisms in candidate genes with potential functional relevance to ICH risk.
Study 2 (ICH): prospective study of patients admitted to participating centers with spontaneous (primary) ICH (with a minimum target of at least 300 OAC-ICH). We will collect detailed clinical and imaging data and DNA.
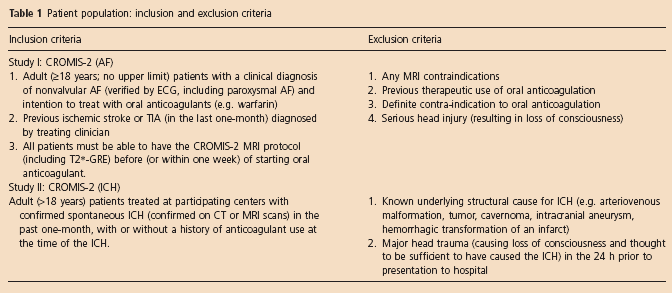
Table 1 summarizes the eligibility criteria for both studies.
Patient population: inclusion and exclusion criteria
Sample size and recruitment of subjects
Study I (AF): We will recruit a total of 1425 patients from UK centers over 47 months. Sample size estimates are based on the incidence of ICH as this is the only intracranial hemorrhage subtype for which data on the influence of CMBs on risk is available. We expect that 20% of our cohort will have CMBs and that overall 2% will have an ICH over two-years. If we assume a conservative relative risk of 4 for CMBS on ICH risk (30), then we estimate the rate of ICH at two-year follow-up to be 5.0% in patients with CMBs, compared with 1.25% in patients without CMBs. This difference would be clinically important and could tip the risk-benefit judgment in favor of avoiding or reducing the intensity of OAC, or considering alternative treatments (e.g. left atrial appendage occlusion device, an antiplatelet agent, or no antithrombotic treatment) in patients with CMBs. To detect such a difference as statistically significant at the 5% level with 90% power would require 1425 patients. Although the best current evidence for the relative risk associated with CMBs in Caucasian populations is 3.9 (35), we have calculated the power for a range of risk ratios, with all other assumptions kept the same (Fig. 1). We would still have 80% power to detect a statistically significant effect of CMBs on ICH risk if the true relative risk was as low as 3.3. Attrition could further reduce power, but we will still have 80% power even with attrition of 28% (based on a relative of risk of 4).
Power of the study (without attrition) across a range of risk ratios, based on an overall event rate of 2% over two-year follow-up and 20% of patients having CMBs.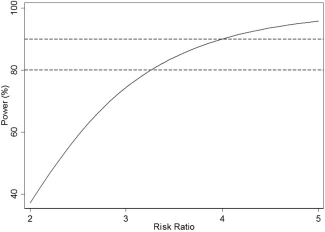
The anticipated ICH event rate of 2% over two-years taking into account attrition suggests that we will observe up to 30 intracranial hemorrhage events in total. The ‘rule of 10’ for developing risk models will allow us to include just three predictor variables (47), though more will be possible through use of modern regression techniques (48). A risk model based solely on CMBs would have a sensitivity of 50% and a specificity of 81% for predicting an ICH within two-years. A risk model based on more predictors should improve on these values. We expect to use existing summary AF prediction risk scores (incorporating multiple variables, e.g. CHADS2VASC, HAS-BLED) as single predictor variables to allow us to assess the additional value of including CMBs as a predictor.
Study 2 (ICH): We will recruit at least 300 patients with OAC-ICH, with an overall target of at least 1000 patients with ICH.
Brain imaging protocol
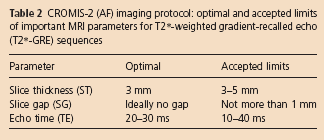
In Study I (AF), all patients will have a standardized MRI at baseline, as soon as possible after stroke or TIA attributed to AF, and within one- to two-weeks after starting OAC. The protocol includes axial T2, T2*-GRE (essential for detecting CMBS), diffusion-weighted imaging, coronal T1-weighted, and FLAIR MR sequences (Fig. 2). The T2* GRE sequence parameters are specified in Table 2. We will acquire additional 3D GRE SWI at as many sites as possible. Where no CMB-sensitive sequences have been obtained, patients will be withdrawn. Where a 3D GRE SWI but not a T2* GRE has been obtained, patients will be included in the primary analysis if no CMBs are detected. A planned sub-analysis will be undertaken including those patients with CMBs on 3D GRE SWI but no corresponding T2*-GRE given the higher sensitivity for CMBs of 3D GRE SWI compared with T2*-GRE (49).
CROMIS-2 (AF) MRI protocol. (A) axial T2-weighted image; (B) axial T2*-weighted gradient echo image; (C) axial diffusion-weighted image; (D) coronal T1-weighted image; (E) coronal FLAIR image; (F) axial susceptibility-weighted image. The arrows in panel B are cerebral microbleeds in the right thalamus.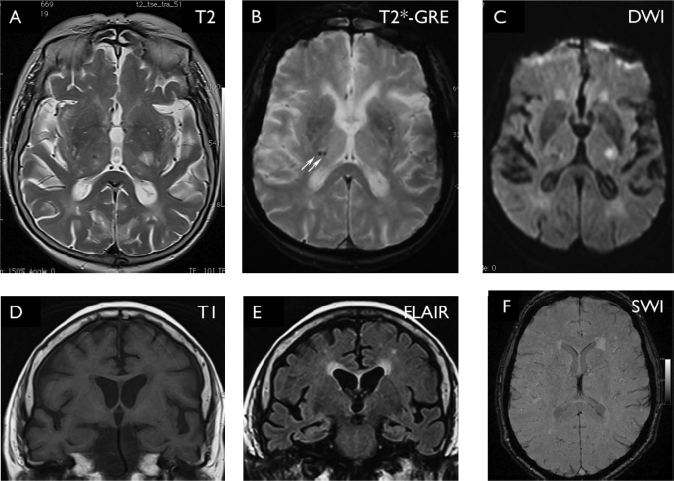
CROMIS-2 (AF) imaging protocol: optimal and accepted limits of important MRI parameters for T2*-weighted gradient-recalled echo (T2*-GRE) sequences
All imaging analysis for CMBs and other imaging markers of cerebrovascular disease will take place at the coordinating center by raters trained in using appropriate validated rating scales, blind to clinical details. CMB number and anatomical distribution will be rated using The Microbleed Anatomic Rating Scale (50). White matter hyperintensity of presumed vascular origin will be graded using standard validated rating scales or semi-quantitative methods. Other potential markers of small vessel disease (e.g. MRI-visible perivascular spaces, lacunes of presumed vascular origin, cortical superficial siderosis) will be rated. Regional atrophy (including medial temporal lobe atrophy) will be rated using validated rating scales or semi-quantitative methods using either coronal/volumetric T1-weighted or coronal FLAIR imaging.
In Study 2 (ICH), all brain imaging undertaken as part of standard clinical care will be collected and analyzed. Hematoma volume will be estimated on plain CT imaging using ABCD/2 or planimetric methods. Perihematomal edema will be measured using a validated planimetric method. We will analyze all available MRI on patients with ICH for markers of cerebral small vessel disease.
Genetic data
Two vials of blood in EDTA will be collected. DNA will be extracted and stored at the UCL Institute of Neurology, Queen Square. Genotyping will be undertaken in collaboration with the International Stroke Genetics Consortium (http://www.strokegenetics.org), subject to regulatory approvals and funding. We will request the use of publically available control genetic data, including the Wellcome 1956 cohort.
Prospective follow-up schedule
The follow-up schedule is shown in Table 3. Multiple ascertainment methods will be used to ensure high rates of complete follow up data. In CROMIS-2 (AF), patients will be followed up at 6, 12, and 24 months by postal questionnaires to patients and their general practitioners. Data collected will include INR monitoring, antithrombotic drug use, and stroke events (ischemic stroke and intracranial hemorrhages). In CROMIS-2 (ICH), patients will be followed up using similar postal questionnaires at six-months. All outcome events will be notified to the central study team by each participating hospital research team. The central study team will also be notified of all deaths and hospital attendances in study participants from the Health and Social Care Information Centre; this includes data on all admitted patient care episodes, outpatient appointments, and emergency attendances in England. We will request data access reports every six-months for the duration of the study.
Summary of data to be collected at baseline and during scheduled follow-up assessments
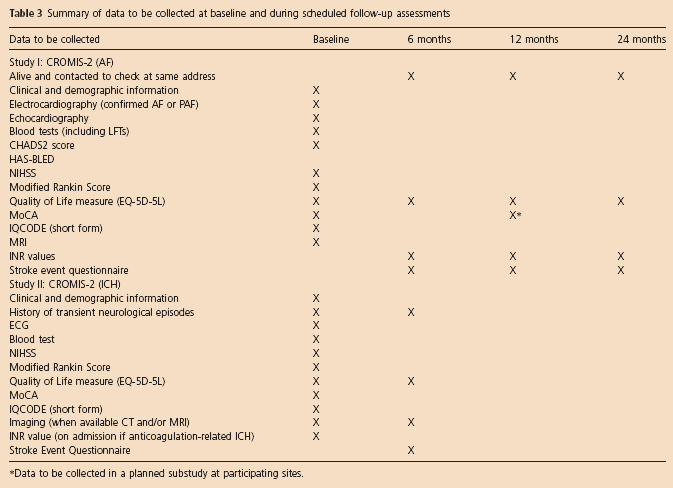
Data to be collected in a planned substudy at participating sites.
Using all available clinical and imaging information, all clinical stroke events will be adjudicated using standardized definitions (51) by a member of the central study team blinded to all baseline clinical and imaging data.
Outcomes
The primary outcome for Study 1 is symptomatic intracranial hemorrhage (including ICH), confirmed on brain imaging. Intracranial hemorrhage includes any bleeding within the skull, regardless of the site. We will record the incidence of different hemorrhage subtypes (subclassified as intracerebral, subdural, extradural, intraventricular, and subarachnoid). Secondary outcomes in study 1 include ischemic stroke, TIA, cardiac events (including myocardial infarction), death of any cause, major hemorrhagic events other than ICH, quality of life, and long-term physical disability. Similar outcomes will be collected for Study 2.
Statistical analyses
We will compare the rate of ICH between the CMB and CMB-free groups using the log-rank test and will investigate whether the number of CMBs is associated with the risk of ICH using Cox regression. Cox regression will be used to develop a risk prediction model for ICH using TRIPOD guidelines (52). Potential risk factors for the model will be prespecified in the statistical analysis plan based on published literature, and variable selection methods may be used to reduce the number of predictors in the risk model. We expect to include existing validated risk scores (including CHADS2VASC for ischemic stroke and HASBLED for serious bleeding) as single variables in the risk model. Penalized estimation, such as ridge or lasso (48), may be used to guard against overfitting. Cross-validation, used in conjunction with calibration slopes and the c-index, will be used to internally validate the model and assess calibration, discrimination, and predictive accuracy. Missing data, and the reasons for it, will be investigated. Imputation may be used if deemed necessary.
Study organization and funding
CROMIS-2 has been adopted by the National Institute of Health Clinical Research Network (NIHR). Recruitment commenced August 2011 and will continue until summer 2015. The sample size will be kept under review by the Steering Committee and may be revised in line with the best available data on CMB-associated relative risks. There are currently 80 sites open to recruitment across the UK and one other European centre (Maastricht). CROMIS-2 is funded by the British Heart Foundation and the Stroke Association. A study website accessible to the public has been set up providing up-to-date information for participants and researchers on study progress (www.ucl.ac.uk/cromis-2).
Summary
Cerebral small vessel disease is a plausible risk factor for intracranial hemorrhage (including ICH) related to OAC use. CMBs have emerged as a potential marker of bleeding-prone small vessel disease and future ICH risk, but high-quality prospective studies of CMBs and ICH risk on anticoagulation are not available. CROMIS-2 will provide prospective data on how CMBs (and other neuroimaging small vessel disease markers) may contribute to assessing the future risk of intracranial hemorrhage on OAC. This risk assessment may become even more important as new drugs will increase the use of OAC (14,53). CROMIS-2 will assess the feasibility of developing a risk model to identify those patients at higher risk of symptomatic intracranial hemorrhage.
Footnotes
Conflict of interest: None declared.