
Abstract
Until recently, resilience among adults exposed to potentially traumatic events was thought to occur rarely and in either pathological or exceptionally healthy individuals. Recent research indicates, however, that the most common reaction among adults exposed to such events is a relatively stable pattern of healthy functioning coupled with the enduring capacity for positive emotion and generative experiences. A surprising finding is that there is no single resilient type. Rather, there appear to be multiple and sometimes unexpected ways to be resilient, and sometimes resilience is achieved by means that are not fully adaptive under normal circumstances. For example, people who characteristically use self-enhancing biases often incur social liabilities but show resilient outcomes when confronted with extreme adversity. Directions for further research are considered.
Keywords
Life is filled with peril. During the normal course of their lives, most adults face one or more potentially traumatic events (e.g., violent or life-threatening occurrences or the death of close friends or relatives). Following such events, many people find it difficult to concentrate; they may feel anxious, confused, and depressed; and they may not eat or sleep properly. Some people have such strong and enduring reactions that they are unable to function normally for years afterward. It should come as no surprise that these dramatic reactions have dominated the literatures on loss and trauma. Until recently, the opposite reaction—the maintenance of a relative stable trajectory of healthy functioning following exposure to a potential trauma—has received scant attention. When theorists have considered such a pattern, they have typically viewed it either as an aberration resulting from extreme denial or as a sign of exceptional emotional strength (e.g., McFarlane & Yehuda, 1996).
RESILIENCE (NOT RECOVERY) IS THE MOST COMMON RESPONSE TO POTENTIAL TRAUMA
Over a decade ago, my colleagues and I began an ongoing investigation of this supposedly rare response, and the means by which people might achieve such presumably superficial (or exemplary) functioning in the aftermath of a potentially traumatic event. The results of our research have consistently challenged the prevailing view on the subject. We took as our starting point the burgeoning developmental literature on resilience. Developmental researchers and theorists had for several decades highlighted various protective factors (e.g., ego-resiliency, the presence of supportive relationships) that promote healthy trajectories among children exposed to unfavorable life circumstances such as poverty (e.g., Garmezy, 1991; Rutter, 1987). We sought to adapt this body of research to the study of resilient outcomes among adults in otherwise normal circumstances who are exposed to isolated and potentially highly disruptive events.
Our research led to three primary conclusions, each mirroring but also extending the insights gained from developmental research. First, resilience following potentially traumatic events represents a distinct outcome trajectory from that typically associated with recovery from trauma. Historically, there have been few attempts to distinguish subgroups within the broad category of individuals exposed to potential trauma who do not develop post-traumatic stress disorder (PTSD). When resilience had been considered, it was often in terms of factors that “favor a path to recovery” (McFarlane & Yehuda, 1996, p. 158). However, studies have now demonstrated that resilience and recovery are discrete and empirically separable outcome trajectories following a dramatic event such as the death of a spouse (e.g., Bonanno, Wortman, et al., 2002) or direct exposure to terrorist attack (e.g., Bonanno, Rennicke, & Dekel, in press). Figure 1 depicts the prototypical resilience and recovery trajectories, as well as trajectories representing chronic and delayed symptom elevations (discussed later).
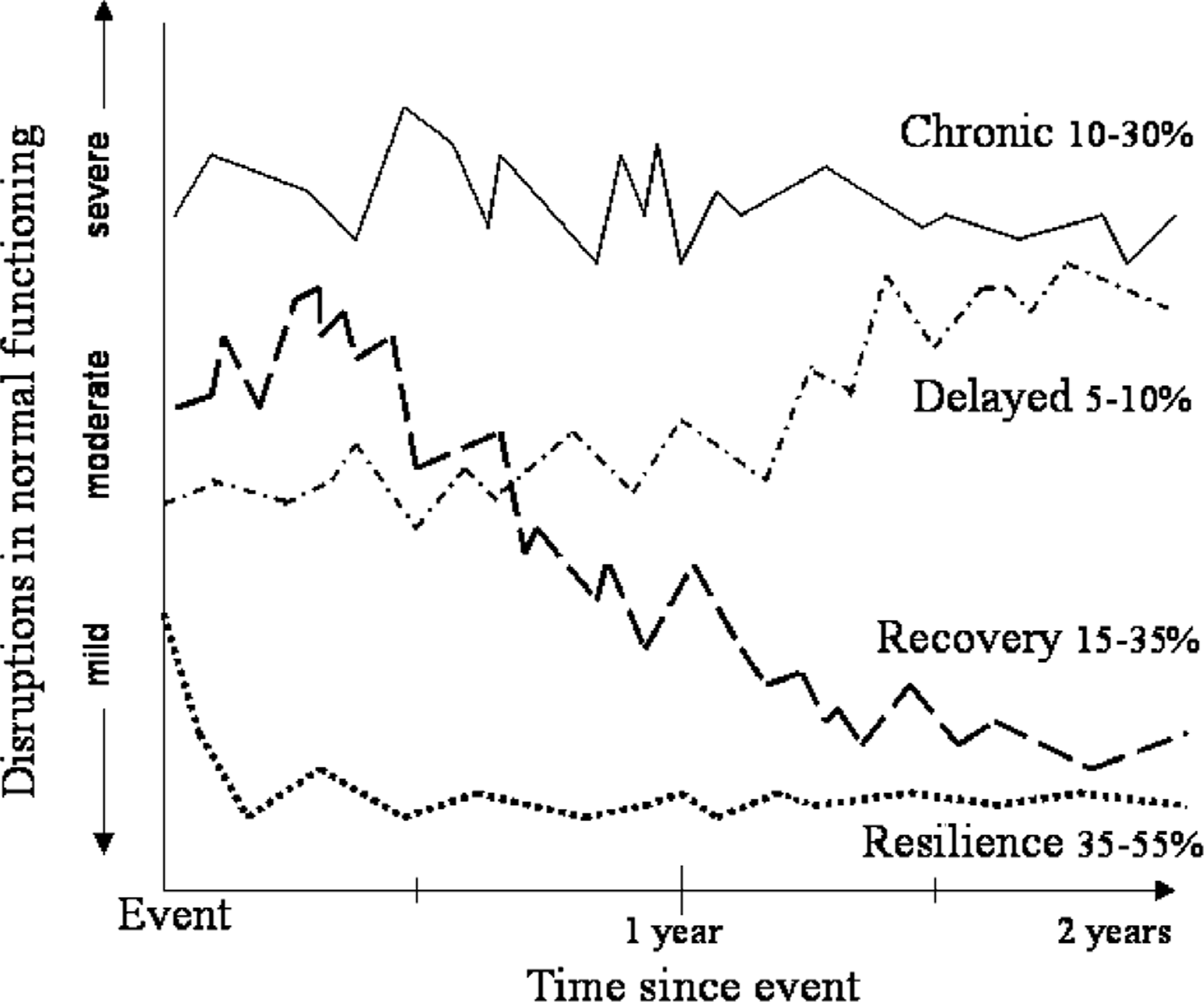
Prototypical trajectories of disruption in normal functioning during the 2-year period following a loss or potential trauma.
In this framework, recovery is defined by moderate to severe initial elevations in psychological symptoms that significantly disrupt normal functioning and that decline only gradually over the course of many months before returning to pre-trauma levels. In contrast, resilience is characterized by relatively mild and short-lived disruptions and a stable trajectory of healthy functioning across time. A key point is that even though resilient individuals may experience an initial, brief spike in distress (Bonanno, Moskowitz, Papa, & Folkman, 2005) or may struggle for a short period to maintain psychological equilibrium (e.g., several weeks of sporadic difficulty concentrating, intermittent sleeplessness, or daily variability in levels of well-being; Bisconti et al., in press), they nonetheless manage to keep functioning effectively at or near their normal levels. For example, resilience has been linked to the continued fulfillment of personal and social responsibilities and the capacity for positive emotions and generative experiences (e.g., engaging in new creative activities or new relationships), both immediately and in the months following exposure to a potentially traumatic event (Bonanno & Keltner, 1997; Bonanno, Wortman, et al., 2002; Bonanno, Rennicke, & Dekel, in press; Fredrickson et al., 2003).
A second conclusion that emerges from our research is that resilience is typically the most common outcome following exposure to a potentially traumatic event. It has been widely assumed in the literature that the most common response to such an occurrence is an initial but sizeable elevation in trauma symptoms followed by gradual resolution and recovery (McFarlane & Yehuda, 1996). However, although symptom levels tend to vary for different potentially traumatic events, resilience has consistently emerged as the most common outcome trajectory. In one study, for example, over half of the people in a sample of middle-aged individuals who had lost their spouses showed a stable, low level of symptoms; and stable low symptoms were observed in more than a third of a group of gay men who were bereaved after providing care for a partner dying of AIDS, a considerably more stressful context (Bonanno, Moskowitz, et al., 2005). Resilience was also readily observed in a random phone-dialing survey of Manhattan residents following the September 11 terrorist attack (Bonanno, Galea, Bucciarelli, & Vlahov, 2005). Following conventions established in the study of subthreshold depression, we defined a mild to moderate trauma reaction as two or more PTSD symptoms and resilience as one or no PTSD symptoms in the first 6 months following the attack. Over 65% in the New York metropolitan area were resilient. Among people with more concentrated exposure (e.g., those who had either witnessed the attack in person or who were in the World Trade Center during the attack), the proportion showing resilience was still over 50%. Finally, even among people who were physically injured in the attack, a group for whom the estimated proportion of PTSD was extremely high (26.1%), one third (32.8%) of the individuals were resilient.
In establishing the validity of the resilient trajectory it is imperative to distinguish stable, healthy functioning from denial or other forms of superficial adjustment. To this end, several studies have now documented links between resilience and generally high functioning prior to a potentially traumatic event (Bonanno, Wortman, et al., 2002; Bonanno, Moskowitz, et al., 2005). Several studies have also documented resilient outcomes using relatively objective measures that go beyond participant self-report, including structured clinical interviews and anonymous ratings of functioning from participants' friends or relatives (e.g., Bonanno, Rennicke, & Dekel, in press; Bonanno, Moskowitz, et al., 2005). For example, we (Bonanno, Rennicke, & Dekel, in press) recruited the friends and relatives of high-exposure survivors of the World Trade Center terrorist attack and asked them to assign the survivors to either the resilience trajectory or one of the other outcome trajectories depicted in Figure 1. The assignments of friends and relatives closely matched the survivors' actual symptom levels over time, and thus provided important validation for the resilience trajectory.
THE HETEROGENEITY OF RESILIENCE: FLEXIBLE AND PRAGMATIC COPING
A third conclusion to emerge from our research, again extending the conclusions of developmental researchers, is that there are multiple and sometimes unexpected factors that might promote a resilient outcome. At the most general level, many of the same characteristics that promote healthy development should also foster adult resilience. These would include both situational factors, such as supportive relationships, and individual factors, such as the capacity to adapt flexibly to challenges (Block & Block, 1980). The capacity for adaptive flexibility was mirrored in a recent study associating resilience among New York City college students in the aftermath of September 11 with flexibility in emotion regulation, defined as the ability to effectively enhance or suppress emotional expression when instructed to do so (Bonanno, Papa, LaLande, Westphal, & Coifman, 2004).
In addition to these general health-promoting factors, however, our research also underscores a crucial point of departure from the developmental literature. Childhood resilience is typically understood in response to corrosive environments, such as poverty or enduring abuse. By contrast, adult resilience is more often a matter of coping with an isolated and usually (but not always) brief potentially traumatic event. The key point is that whereas corrosive environments require longer-term adaptive solutions, isolated events often oblige a more pragmatic form of coping, a “whatever it takes” approach, which may involve behaviors and strategies that are less effective or even maladaptive in other contexts. For instance, considerable research attests to the health benefits of expressing negative emotions. Although most resilient bereaved individuals express at least some negative emotion while talking about their loss, they nonetheless express relatively less negative emotion and greater positive emotion than other bereaved individuals (e.g., Bonanno & Keltner, 1997), thereby minimizing the impact of the loss while “increasing continued contact with and support from important people in the social environment” (p. 134).
Another example of pragmatic coping is illustrated by trait self-enhancement, the tendency toward self-serving biases in perception and attribution (e.g., overestimating one's own positive qualities). People given to self-serving biases tend to be narcissistic and to evoke negative reactions in other people. However, they also have high self-esteem and cope well with isolated potential traumas. Our research team examined self-enhancement among people dealing with two powerful stressor events, the premature death of a spouse and exposure to urban combat during the recent civil war in Bosnia (Bonanno, Field, Kovacevic, & Kaltman, 2002). In both samples, trait self-enhancement was positively associated with ratings of functioning made by mental health experts. In the bereavement study, however, untrained observers rated self-enhancers relatively unfavorably (lower on positive traits, e.g., honest; and higher on negative traits, e.g., self-centered). Yet, these negative impressions did not appear to interfere with self-enhancers' ability to maintain a high level of functioning after the loss.
This same pattern of findings was observed among high-exposure survivors of the September 11 attack (Bonanno et al., in press). Trait self-enhancement was more prevalent among individuals exhibiting the resilient trajectory, whether established by self-reported symptoms or ratings from friends or relatives. Self-enhancers also had greater positive affect and were rated by their friends and relatives as having consistently higher levels of mental and physical health, goal accomplishment, and coping ability. However, self-enhancers' friends and relatives also rated them as decreasing in social adjustment over the 18 months after September 11 and, among those with the highest levels of exposure, as less honest. This mixed pattern of findings suggests again that self-enhancers are able to maintain generally high levels of functioning in most areas except their social relations. Interestingly, however, self-enhancers themselves perceived their social relationships in relatively more positive terms than other participants, and this factor fully mediated their low levels of PTSD symptoms. In other words, self-enhancers appear to be blissfully unaware of the critical reactions they can evoke in others, and this type of self-serving bias evidently plays a crucial role in their ability to maintain stable levels of healthy functioning in other areas following a potentially traumatic event.
DIRECTIONS FOR FUTURE RESEARCH
The study of adult resilience is nascent and there are myriad questions for future research. An obvious imperative is to learn how the various costs and benefits of resilience vary across different types and durations of potentially traumatic events. Is there a point, for example, when the long-term costs of a particular type of coping might outweigh whatever crucial short-term advantages it provides? Might such trade-offs vary by gender or culture? Western, independence-oriented societies, for example, tend to focus more heavily than collectivist societies on the personal experience of trauma. However, little is known about the extent that loss and trauma reactions vary across cultures. A recent comparative study showed that bereaved people in China recovered more quickly from loss than did bereaved Americans (Bonanno, Papa, et al., 2005). However, as is typical of Chinese culture, Chinese bereaved also reported more physical symptoms than Americans. These data raise the intriguing questions of whether resilience has different meanings in different cultural contexts and, perhaps even more important, whether different cultures may learn from each other about effective and not-so-effective ways of coping with extreme adversity.
These questions in turn raise multiple practical and philosophical uncertainties about whether resilience can or should be learned. On the one hand, the observed link between resilient outcomes and personality variables suggests that resilient traits may be relatively fixed and not easily inculcated in others. And, given the social costs associated with some of the traits found in resilient people (e.g., self-enhancement), the advantage of simply imitating resilient individuals is questionable. On the other hand, a more promising avenue for training people to cope resiliently with trauma is suggested by the evidence linking resilience to flexible adaptation (Block & Block, 1980; Bonanno et al., 2004). Because adaptive flexibility can be manipulated experimentally (e.g., people's ability to engage in various cognitive or emotional processes can be measured under different stressor conditions; Bonanno et al., 2004), it should be possible to systematically examine the stability of such a trait over time and the conditions under which it might be learned or enhanced.
A related question pertains to how resilient individuals might view their own effectiveness at coping with potential trauma. Although at least some resilient individuals are surprised at how well they cope (Bonanno, Wortman, et al., 2002), it seems likely that others (e.g., self-enhancers) might overestimate their own resilience. This issue is particularly intriguing in relation to the distinction between stable resilience and delayed reactions. Although delayed reactions are not typically observed during bereavement (e.g., Bonanno, Wortman, et al., 2002), a small subset of individuals exposed to potentially traumatic events (5–10%) typically exhibit delayed PTSD. Preliminary evidence indicates that delayed-PTSD responders have higher initial symptom levels than do resilient individuals (e.g., Bonanno et al., in press). Further evidence of this distinction would hold potentially important diagnostic implications for early intervention.
Finally, another question pertains to how resilient individuals experience the crucial early weeks after an extreme stressor event. A recent study by Bisconti, Bergeman, and Boker (in press) shed some welcome light on this issue by examining daily well-being ratings in the early months after the death of a spouse. Although resilient bereaved typically show only mild and relatively short-lived overall decreases in well-being, examination of their daily ratings indicated marked variability across the first 3 weeks and then a more stable but still variable period that endured through the second month of bereavement. Perhaps similar research using larger samples and Internet methods might illuminate how resilient individuals manage to continue functioning and meeting the ongoing demands of their lives while nonetheless struggling, at least for a short period, to maintain self-regulatory equilibrium.
Footnotes
Acknowledgements
This research was supported by grants from the National Institutes of Health (R29-MH57274) and the National Science Foundation (BCS-0202772 and BCS-0337643).