
Abstract
Background
Specific information about the nature of recurrent events that occur after each subtype of index stroke may be useful for refining preventive therapies. We aimed to determine whether stroke recurrence rates, the pattern of subtype recurrence, and prescription of secondary prevention agents differed according to initial stroke subtype.
Methods
Multiple overlapping sources were used to recruit all first-ever stroke patients from a geographically defined region of Melbourne, Australia over a 3-year period from 1996 to 1999. Potential stroke recurrences (fatal and nonfatal) occurring within 2 years of the initial event were identified following patient interview and follow up of death records. Subjects were classified into the different Oxfordshire groups and the type of first-ever stroke was compared with recurrent stroke events.
Results
One thousand, three hundred and sixteen first-ever strokes were registered during the 3-year period (mean age 74·4 years). A total of 103 first recurrent stroke events (fatal and nonfatal) occurred among those with a first-ever ischemic stroke or intracerebral hemorrhage (ICH) during the 2-year follow-up period. The recurrent stroke subtype was different to the index stroke subtype in most (78%) patients. People with partial anterior circulation infarct had the greatest proportion of recurrences (13%), with a third of these being the more severe total anterior circulation infarct subgroup. The relative risk of ICH after an index lacunar infarct (LACI) compared with an index non-LACI was 4·06 (95% CI 1·10–14·97, P=0·038). Prescription of secondary prevention agents was greater at 2 years after stroke than at hospital discharge, and was similar between ischemic stroke subtypes.
Conclusion
Approximately 9% of people with first-ever stroke suffered a recurrent event, despite many being prescribed secondary prevention agents. This has implications for the uptake of current preventive strategies and the development of new strategies. The possibility that ICH is greater among index LACI cases needs to be confirmed.
Introduction
Population-based studies on long-term prognosis (survival and recurrence) after stroke are crucial for identifying explanations for the decline in mortality from stroke and for generating strategies for public health policy (1). Mortality (2–16) and stroke recurrence (3, 17–19) are high after a first-ever stroke, although the figures vary. The 3-year cumulative risk of recurrent stroke has been reported to be in the range of 6–25% (3, 17–19). This risk could be reduced if appropriate secondary prevention measures were adequately implemented. Such preventive measures might include the use of antiplatelet, blood pressure and cholesterol lowering agents, anticoagulants and carotid artery surgery. Given the heterogeneous nature of stroke, it is likely that more specific information about the types of recurrences that occur after each subtype of index stroke may provide evidence to help refine the form of therapy administered.
The Oxfordshire Community Stroke Project (OCSP) (20) classification offers a simple and practical clinical approach, with satisfactory inter-observer reliability, which can be used at the bedside (21, 22). Although, this classification is useful in predicting the prognosis of stroke, few investigators have compared mortality or recurrences after stroke between OCSP subtypes (20, 23–25). These studies are limited either by the relatively small number of recurrences, or by the fact that OCSP subtypes have not been classified prospectively.
We have previously reported 1-year mortality and recurrence data for the OCSP subtypes among the cohort of first-ever ischemic stroke patients (n = 200) registered during the first year of recruitment for the North East Melbourne Stroke Incidence Study (NEMESIS) (23). Overall, 10% of first-ever ischemic stroke patients experienced a recurrent event and recurrences were greatest among cases of partial anterior circulation infarct (PACI) (17%). We have now expanded our investigation to assess mortality and recurrences according to initial OCSP subtype established prospectively among the entire NEMESIS cohort. Our aims were to determine whether
stroke recurrence rates differed according to the initial stroke subtype
the pattern of subtype recurrence differed according to the initial stroke subtype, and
the use of secondary prevention agents varied between stroke subtypes.
Methods
Study Population
The study methods have been described in detail previously (15, 15, 16). Briefly, NEMESIS was conducted in a defined region of inner north-east Melbourne. We ascertained all cases of fatal and nonfatal first-ever stroke occurring in a population of 133 816 between 1 May 1996 and 30 April 1997 and a population of 306 631 between 1 May 1997 and 30 April 1999. Multiple overlapping sources were used to recruit stroke patients, and much of the effort was expended in locating those stroke patients managed solely in the community without admission to a hospital. Potential cases were reviewed by a panel of stroke experts before inclusion.
Baseline Characteristics
We obtained information about age, gender and independent living status. Presence or absence of risk factors was obtained from the medical or nursing home records. Risk factors that were recorded were:
hypertension
diabetes mellitus
smoking
alcohol consumption
transient ischemic attack (TIA)
and cardiac conditions including myocardial infarction and atrial fibrillation.
Definitions
Stroke was defined according to the World Health Organization criteria as rapidly developing signs of focal or global disturbance of cerebral function, lasting > 24 h or leading to death, with no apparent cause other than vascular (27).
A recurrent stroke occurring during the recruitment phase of the study and during the 2-year follow-up period was defined as a fatal or nonfatal stroke occurring more than 28 days after the index stroke (18, 18, 28). Additional events occurring within 28 days of the first registered event were also counted when they occurred in a different vascular territory.
An ever smoker was a patient who had either a prior history of smoking (ex smoker) or who smoked daily (current smoker) at the time of the stroke.
Previous TIA was defined as a history of acute, focal neurological deficit of vascular origin within the previous 6 months, lasting < 24 h and diagnosed by a medical practitioner.
Stroke classification
Pathological stroke subtype [IS, intracerebral hemorrhage (ICH)] was determined using neuroimaging or autopsy findings (16). Patients with neither neuroimaging nor autopsy were classified as ‘undetermined stroke’. Ischemic stroke cases were further categorized using the OCSP classification (20), based on the symptoms and signs present at the time of maximal deficit after stroke and was made without reference to brain imaging findings. The classification of IS comprised total or partial anterior circulation infarct (TACI or PACI, respectively), posterior circulation infarct (POCI) and lacunar infarct (LACI), the latter including pure motor stroke, pure sensory stroke, sensorimotor stroke and ataxic hemiparesis (20).
Follow-up
Face-to-face follow-up interviews were conducted every 12 months following stroke and any potential recurrent events identified. Further information about all such possible events was sought from the treating medical practitioner and relevant hospital medical records. A panel of neurologists reviewed these potential events before inclusion.
Information about death was collected on all subjects via linkage of all study participants with the National Death Index. In the second and third year of the study information about medications prescribed at the time of discharge from hospital was obtained for those patients attending hospital for initial stroke care. In addition, in a subset of patients (i.e. those recruited in the third year of the study), information about medication use at 2 years after stroke was also obtained.
Main outcome measure
The main outcome measure was the first recurrent stroke event (fatal and nonfatal) during the 2-year follow-up period.
Statistical Analysis
The differences in recurrence rate between each Oxfordshire subtype of index stroke vs. each other ischemic subtype was tested using a two-sided Fisher's exact test. The effect of index Oxfordshire stroke subtype on time to stroke recurrence was investigated using Kaplan–Meier survival curves. Log-rank tests for equality of survivor functions were used to test for differences between these subtypes. The magnitude of the effect of having a LACI as the index stroke subtype, compared with other subtypes, on having an ICH for the second event was explored using the Fisher's exact test and estimation of the odds ratio. All of the analyses were performed using Stata 9·2.
Results
In total, 1316 first-ever strokes occurred within the study region from 1 May 1996 and 30 April 1999 and were followed up for 2 years. Of these 921 (70%) were ischemic strokes, 191 (15%) were ICH, 68 (5%) SAH and 136 (10%) were undetermined strokes. Of those with IS there were 329 (36%) PACI, 217 (24%) LACI, 187 (20%) TACI and 188 (20%) POCI. Patients with TACI tended to be older than those with other types of ischemic stroke, and were more often female (58%; Table 1). The characteristics and prevalence of the risk factors in different subtypes of ischemic stroke are listed in Table 1.
Baseline characteristics and 2-year outcome according to Oxfordshire subtype
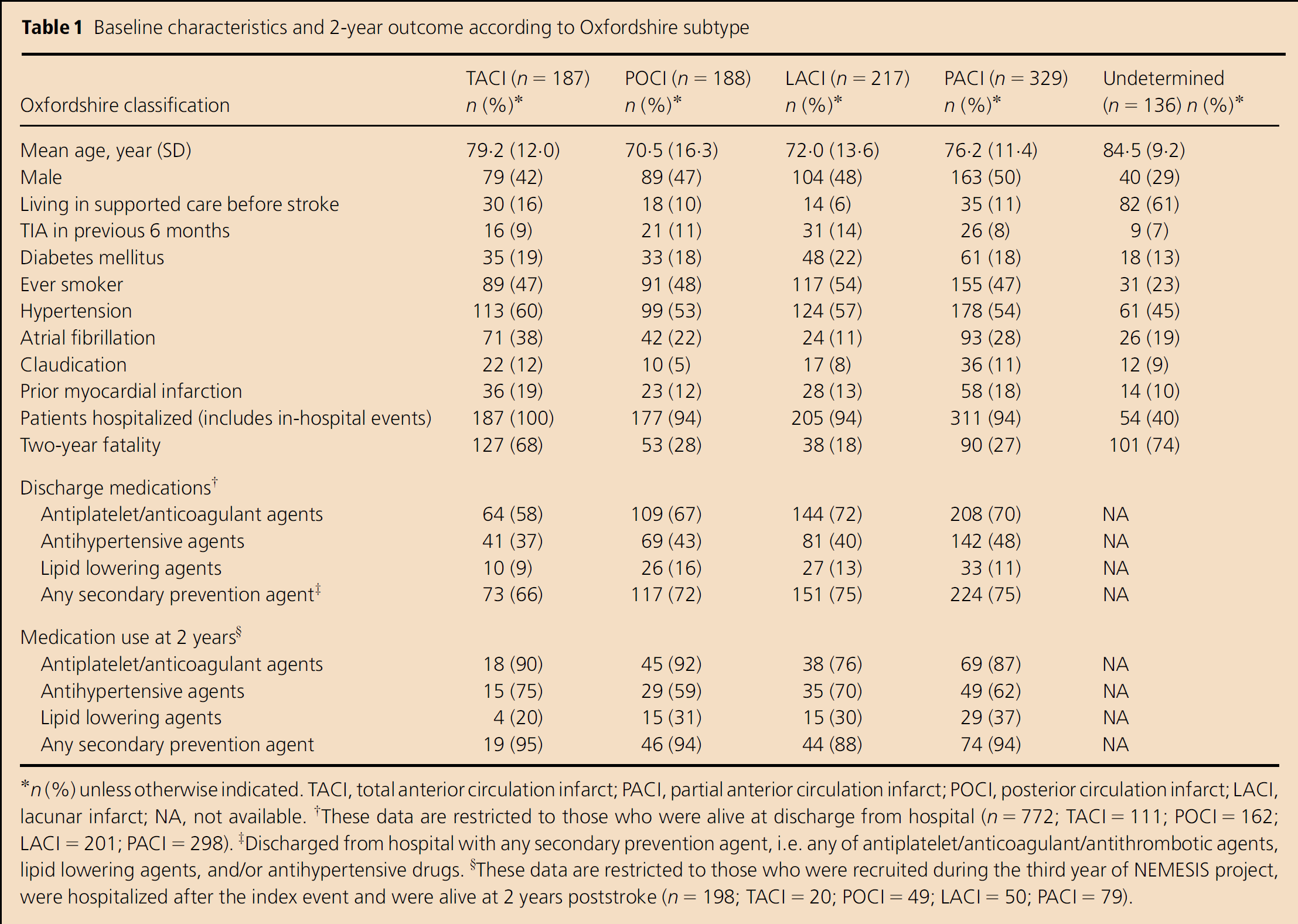
n (%) unless otherwise indicated. TACI, total anterior circulation infarct; PACI, partial anterior circulation infarct; POCI, posterior circulation infarct; LACI, lacunar infarct; NA, not available.
These data are restricted to those who were alive at discharge from hospital (n = 772; TACI = 111; POCI = 162; LACI = 201; PACI = 298).
Discharged from hospital with any secondary prevention agent, i.e. any of antiplatelet/anticoagulant/antithrombotic agents, lipid lowering agents, and/or antihypertensive drugs.
These data are restricted to those who were recruited during the third year of NEMESIS project, were hospitalized after the index event and were alive at 2 years poststroke (n = 198; TACI = 20; POCI = 49; LACI = 50; PACI = 79).
During the 2-year follow-up period, 121 first recurrent stroke events (fatal and nonfatal) were observed. Overall, the proportion of cases with recurrent stroke over the 2-year period was 9·2% (6·3% in the first year and 2·9% in the second year after stroke). Among those with a first-ever IS or ICH 103 recurrences occurred, and in 92 of these brain imaging was performed. TACI patients had a significantly lesser rate of recurrence than other ischemic Oxfordshire subtypes combined (P < 0·001).
Figure 1 shows the probability of having a recurrent stroke up to 2 years after stroke according to each initial ischemic stroke subtype. The difference in time to recurrence between Oxfordshire subtypes was of borderline statistical significance overall (χ2 = 6·93, P = 0·074). Analysis of the pairwise differences between individual Oxfordshire subtypes revealed that PACI had increased probability of having a recurrent stroke, which may occur sooner after the index stroke than for cases with TACI as the index stroke (χ2 = 6·49; P = 0·011).
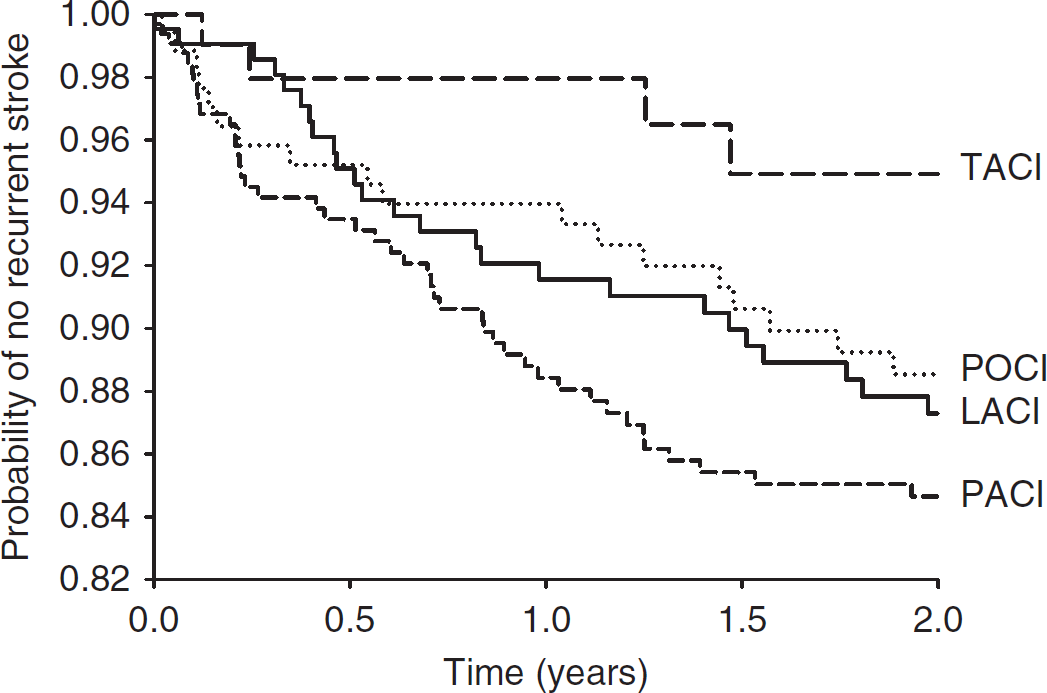
Kaplan–Meier curve of stroke recurrence (fatal and nonfatal) according to Oxfordshire subtype
Excluding those with undetermined stroke and subarachnoid hemorrhage, the pattern of recurrent stroke subtype was different to the index stroke subtype in 72 (78%) patients (Table 2). Half of the recurrent events in TACI were TACI (n = 2), the remainder being undetermined strokes. The relative risk of having an ICH as the second stroke among those with a LACI index stroke when compared with those having a non-LACI index ischemic stroke was 4·06 (95% CI 1·10–14·97, P = 0·038). Among PACIs the subsequent stroke was PACI in 11 cases (24%) and TACI in 15 patients (33%).
Classification of recurrent strokes according to initial stroke subtype
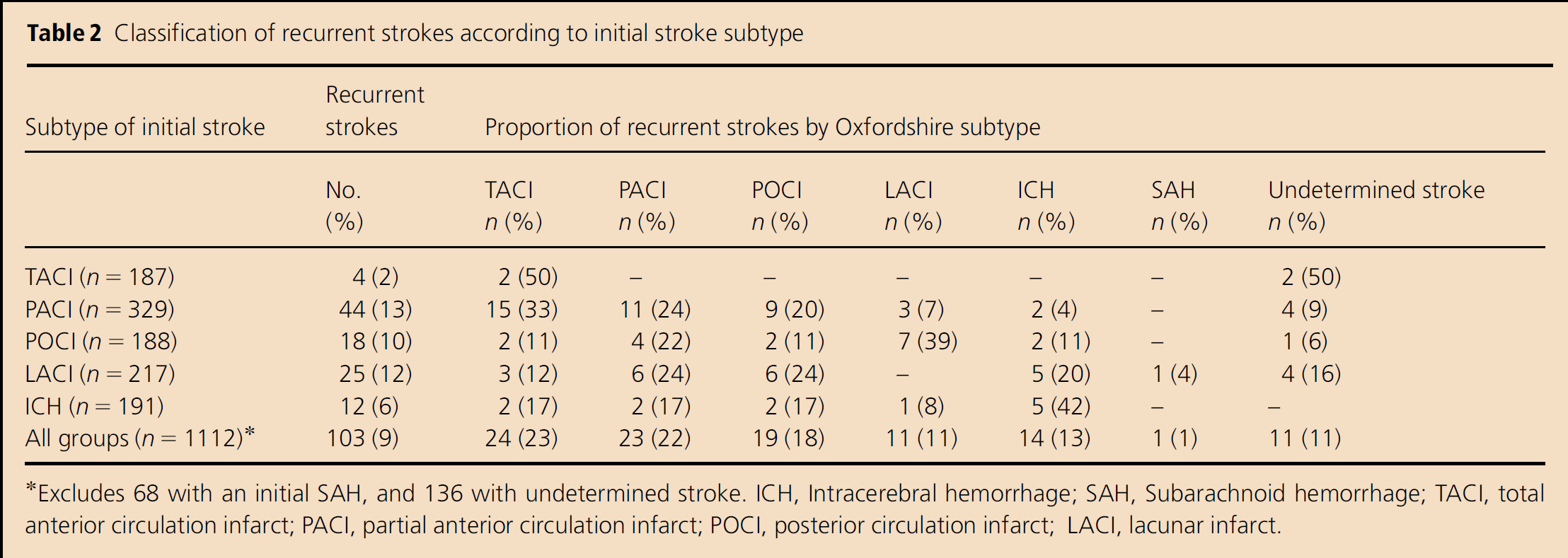
Excludes 68 with an initial SAH, and 136 with undetermined stroke. ICH, Intracerebral hemorrhage; SAH, Subarachnoid hemorrhage; TACI, total anterior circulation infarct; PACI, partial anterior circulation infarct; POCI, posterior circulation infarct; LACI, lacunar infarct.
The proportion of survivors discharged from hospitals that were taking secondary prevention therapies are provided in Table 1 . Overall, people with a TACI were less likely to be taking any secondary prevention therapies at hospital discharge than any of the other stroke subtypes (P < 0·0001).
Treatment with any secondary prevention agents at 2 years (these data being available for those who were recruited during the third year of the study, n = 198) was similar between ischemic stroke subtypes, and appeared to be greater than at discharge from hospital.
Discussion
Recurrent stroke is frequent and results in increased mortality, morbidity and duration of hospital stay (3, 3, 7). Attention to the index stroke, particularly to clinical presentation, classification and also mechanism might be useful to identify patients at a high risk of recurrence. It may also allow identification of patients who will benefit from early therapeutic and interventional procedures. The proportion of recurrent strokes, which are potentially avoidable with the use of secondary prevention strategies, is currently estimated to be approximately 20% (30). If secondary prevention strategies could be more efficiently targeted for the type of recurrence expected it is possible that this proportion could be improved. We found a significant difference between the rates of recurrence for the first nonfatal or fatal stroke between stroke subtypes based on the Oxfordshire classification. Specifically, those classified as TACI had the least recurrences. People with an index PACI had an average recurrence rate of 7% per year over the 2-year period (10% in the first year and 3% in the second year). This is somewhat less than previously published data from the NEMESIS population, where 17% of those with a first-ever PACI had a recurrent event during the 12-month study (23). The reduced recurrence rate in the present study was evident among all ischemic stroke subtypes, and may relate to the greater socioeconomic disadvantage in the population of the previous report (31).
The importance of the identification of a high risk subset of ischemic stroke patients in whom current secondary prevention strategies appear to be less effective than for other subtypes must be emphasized. First, in epidemiological cohort terms, this represents an ideal group in which to test new interventions, which may reduce the unacceptably high rate of stroke recurrence. In other words, when recruiting patients for large clinical trials where initial sample sizes are driven by event rates and the duration of the trial may be also determined by this parameter, the setting of inclusion criteria to capture this group may be useful. Second, an exploration of the underlying mechanisms may help identify secondary prevention strategies, which are more likely to be effective because of their specific biological effects. A further exploration of this issue with modern neuroimaging techniques may be fruitful.
The observation that secondary prevention therapies were not well utilised requires some comment. Firstly, at the time this study was completed, HMG-CoA reductase inhibitors (‘statins’) could not be routinely prescribed for secondary stroke prevention under the publicly funded pharmaceutical benefits scheme. This explains the small proportion of patients being treated with these medications. Secondly, the fact that only about two-thirds of patients were being prescribed antithrombotic agents at discharge suggests that these agents were being underutilised. It is possible that more recurrences may have been prevented if standard evidence-based care had have been practised at all institutions.
Patients with TACI had a significantly lower recurrence rate than those with PACI, LACI and POCI, in keeping with the reported low rates of stroke recurrence in the former during the first few months after index stroke (19, 20). This finding may be an artefact resulting from the difficulty in diagnosing new neurological deficits in severely affected patients (19), as well as to the high mortality in the first month of stroke in the TACI group. The proportion of recurrences was not significantly different between patients with PACI, POCI and LACI.
In our study, we found no strong relationship between the Oxfordshire subtype of the index stroke and subtype of recurrent events. This is in contrast to the findings from a recent meta-analysis where recurrent lacunar infarction was greater among those with an index lacunar infarction than among those with an index nonlacunar infarction (32). Indeed, we found no lacunar re-infarctions following an original lacunar infarction. The reason for this disparity is unclear, but may be related to differences in diagnosis of subtypes or to the fact that, because hot pursuit was not used throughout the 2-year follow-up period, milder recurrent strokes were sometimes missed. Given that lacunar strokes comprised only 11% of all recurrences it is possible that some lacunar strokes were missed.
The observation that people with a LACI index stroke showed a greater proportion of ICHs as the second stroke than did other stroke subtypes might relate to similar pathophysiological processes (particularly small vessel lipohyalinosis) between ICH and lacunar infarcts (33, 34). This finding is unlikely to be attributable to inaccuracy of neuroimaging diagnosis as 73% of imaged patients (67/92) had imaging within 1 day and 90% (83/92) had imaging within 4 days. Hence the diagnosis of hemorrhage could be made accurately in the majority of cases. Others have also shown that ICHs occur more frequently after a lacunar than a nonlacunar infarction, although there were few ICHs and the difference did not reach statistical significance (32). Larger populations and/or analyses of pooled individualized data from existing studies are required to pursue this matter further.
Interestingly, those patients with index PACIs had a high proportion of recurrent TACIs; this subtype having a well-documented greater mortality. This may indicate further progression of underlying atherosclerosis, despite the use of currently available secondary prevention strategies. This further emphasizes the need to improve the uptake of current secondary prevention strategies in this group or to identify new methods of secondary stroke prevention in this group.
There are a number of limitations to our study. Firstly, 11 (11%) of our patients with recurrent events did not undergo neuroimaging, and so we could not confirm the clinical diagnosis. It is possible that some of these patients may instead have had a condition that mimics stroke (35), although careful scrutiny was made of patients presenting with migraine and seizures. In addition, although a major focus of the NEMESIS project has been the accurate subtyping of both incident and recurrent strokes, the classification of recurrent events is likely to be less accurate than first-ever events, particularly in dependent individuals residing in nursing homes. However, when nursing home patients were cognitively impaired or otherwise too ill to be interviewed, either a next-of-kin or carer was interviewed instead. This may have helped to minimize any underestimation of recurrence in any particular group. As in most cohort studies the ‘hot pursuit’ technique was not used to ascertain recurrent events beyond the recruitment period but, rather, events were detected via yearly follow-up interviews and the clinical details of potential stroke events then further evaluated (medical records assessed and treating doctor contacted, if necessary).
Furthermore, use of the OCSP subtype for classification of strokes does not allow adequate assessment of the likely pathophysiological process, as would classification using the TOAST (Trial of Org 10172 in Acute Stroke Treatment) criteria (36). If the TOAST criteria had been used instead we would have excluded 362 patients with an index ischemic stroke (39%) from the subtype analysis as the etiology of stroke was uncertain, usually because of limited investigations. A total of 38 of these 362 patients had a recurrent event. Thus, 42% (38/91) of all recurrences would have been excluded from the analysis. The advantage of using the OCSP subtype instead, is that it can be used in a community-based setting, where all cases of stroke, including those not hospitalized or those not undergoing extensive diagnostic tests are included. However, the fact that brain imaging, particularly MR imaging, was not used to modify the clinical classification of stroke subtypes is likely to have resulted in some misclassification; thereby masking any differences in stroke subtypes. Our choice of a 28-day period to define a stroke event (except in the circumstance where a different vascular territory was involved) was in line with other stroke incidence studies (18, 18, 28). This approach provides clear delineation between given stroke events and is likely to increase the accuracy of recurrent event definition in a community-based study. However, very early recurrences were not included and it is of interest that the investigators of the Oxford Vascular Study (37) have recently reported a high risk of early recurrent stroke (15% at 1 month) within a community-based cohort by focusing on this issue. In view of these findings, it is likely that we have substantially underestimated recurrent events in our cohort. This may also have affected the results of the recurrent stroke patterns, and so the proportion of recurrent strokes that are of the same type as the index stroke may have been underestimated. Finally, our follow-up period of 2 years limits the total number of recurrent events. This is counterbalanced by the unusually large size of the study population base and, hence, cohort.
In conclusion, among 1112 patients with first-ever ischemic stroke or ICH we observed 103 fatal or nonfatal stroke recurrences over a 2-year follow-up period. The subtypes of recurrent strokes were different in comparison with the index stroke in 78% (based on patients with imaging) of our patients. This may suggest a multifactorial origin of stroke recurrence among Oxfordshire subtypes. In addition, among those where PACI has progressed to TACI, this may suggest a progression of the underlying disease, despite preventative strategies. Moreover, the tendency for ICH recurrence to occur more often among those with an initial LACI index stroke may also highlight that secondary prevention strategies in this group may need to be modified. Clearly, current secondary prevention strategies appear to be either insufficiently used or be insufficient to prevent stroke, particularly for those with much to lose (the PACIs and LACIs).
Footnotes
Acknowledgements and funding
This work was supported by grants from the National Health and Medical Research Council (NHMRC), the Victorian Health Promotion Foundation, the Foundation for High Blood Pressure Research and the National Stroke Foundation. The Australian Institute of Health and Welfare matched the study patients with the National Death Index.