
Abstract
Background
Caregiver burden following stroke can have significant adverse health consequences for caregivers and threatens the recovery and successful rehabilitation of patients. Our objective was to identify patient factors that contribute to higher levels of caregiver burden.
Methods
We prospectively studied patients admitted to our stroke unit over a 2-year period (2001-2002). Data were collected at baseline and at 1 year. Caregiver burden was measured at 1 year using the Relatives Stress Scale (completed by 155 caregivers) and the Bakas Caregiver Outcomes Scale (143 caregivers). Explanatory patient factors at baseline included sociodemographic status, stroke severity, stroke sub-type, functional disability (Barthel Index), functional handicap (Oxford Handicap Scale and Modified Rankin Scale), and cognitive status (orientation, clock drawing). At 1 year, mental health and health-related quality of life were assessed using the Fatigue Impact Scale, Geriatric Depression Scale, Global Deterioration Scale, and 36-item Short Form Health Survey.
Results
The baseline patient factors predictive of caregiver burden by multiple regression analysis were older patient age (P<0·01), male gender (P<0·05), ischemic stroke (P<0·05), urinary incontinence (P<0·0001), and impaired clock drawing (P<0·05). At 1 year, significant correlates of caregiver burden were older patient age (P<0·05), male gender (P<0·01), poor mental health (P<0·05), functional handicap (P<0·05), and functional disability (P<0·001).
Conclusions
The functional status of patients can be used to identify caregivers at risk of caregiver burden. Patient demographic variables, cognitive function, and mental health status may further expose vulnerable caregivers. These factors should be considered in the development of strategies to offset caregiver burden.
Background
Caregiver burden is increasingly recognized as a serious health threat for stroke survivors and their caregivers. A number of studies have identified significant adverse consequences on the health of the caregiver including psychiatric and physical morbidity (1–5). There is some evidence to suggest that caregiver stress may also hinder the recovery and successful rehabilitation of stroke patients (3, 6).
Caregiver burden is a multi-dimensional concept that encompasses the psychological, health, social, and economic impacts of caregiving (7). It can be measured by quantifying the degree of burden [as in the Relatives Stress Scale (RSS)] or by evaluating the life changes that result from providing care (as in the Bakas Caregiver Outcomes Scale). Both approaches are considered in this study.
A number of studies have evaluated factors that contribute to subjective caregiver burden but there is remarkably little consensus in the literature. Researchers theorize that caregiver burden is mediated by patient and caregiver physical, psychological, demographic, and social support factors. In studies that have performed advanced statistical analyses to understand the complexity of caregiver burden, objective burden (8–11), and mental health problems in the patient and caregiver (10, 12–14) are the variables most consistently associated with increased subjective burden. The evidence is inconsistent with respect to the importance of patient demographic variables, functional status, cognitive impairment, and social support (8, 10, 12, 15–17).
Few studies have attempted to identify factors present in the early-stage poststroke that predict subsequent caregiver burden, those that do disclose different independent predictors creating a conflicted picture (8, 8, 18).
A number of caregiver interventions have been examined for their utility in alleviating caregiver burden, with mixed results. Training for caregivers in basic nursing and personal care techniques was shown to reduce caregiver burden and improve other psychosocial outcomes in patients and caregivers at 1 year (20). The assignment of family care workers and specialist nurses for caregiver support has shown limited benefits (21, 22). The design and appropriate application of caregiver interventions may be facilitated if the determinants of burden and needs of caregivers are better understood (12). The purpose of this study was to identify patient factors that contribute to higher levels of caregiver burden.
Methods
Participants
Participants in this study were consecutive patients with a stroke or transient ischemic attack admitted to the Queen Elizabeth II Health Sciences Centre (QEII) Stroke Unit from January 2001 to December 2002.
Procedure
This study was approved by the QEII Research Ethics Committee. Written consent was obtained from study participants. Assessments were conducted in-person within 7 days of admission for stroke and at 12 months. An informal caregiver was defined as any unpaid person directly involved in the personal care of the patient.
Patient demographics and place of residence were recorded at the time of admission and confirmed at the follow-up assessment. Stroke sub-type and severity (23) were documented at the time of admission. Cognitive function was assessed within 7 days of admission and at 12 months with orientation (24) and clock drawing tests (25) and at 12 months using the Global Deterioration Scale (26) to screen for dementia. Global handicap was measured at the time of discharge using Oxford Handicap Scale (27) and at 12 months using the modified Rankin Scale (MRS) (28). Functional disability was measured by the Barthel Index (BI) (29) and by self-reported dependency (30). Assessment of mental health and health-related quality of life (HRQOL) was conducted at 12 months using the Geriatric Depression Scale (31), the Modified Fatigue Impact Scale (32), the Reintegration to Normal Living questionnaire (33), and the 36-item Short Form Health Survey (SF-36) (34). Informal caregivers present at the 12-month follow-up visit were invited to complete two questionnaires measuring caregiver burden, the RSS (35), and the Bakas Caregiving Outcomes Scale (BCOS) (36). The BCOS was introduced later in the study.
The RSS is an instrument originally applied to a population of elderly patients with dementia. It measures the degree of stress and upset experienced by friends or relatives involved in the care of elderly patients (35). It is composed of 15 items and each is scored on a five-point scale (never = 0 to always = 4). The questionnaire is composed of three independently validated subscales: personal distress, life upset, and negative feelings. The reliability coefficients for the subscales as reported by the original authors are 0·72, 0·80, and 0·88, respectively (35). The RSS has been shown to be clinically valid and reliable in assessing burden in caregivers of stroke patients (15, 18, 37, 38).
The BCOS was developed to address the need for an instrument that measures life changes that result from providing care (36). This 15-item questionnaire evaluates the adaptations made by caregivers to the caregiver situation. Each item is scored from −3 (changed for the worst) to +3 (changed for the best). Responses are recoded from 1 to 7 so that positive numbers are obtained for analysis. Lower scores are indicative of greater burden. The reliability coefficient for the modified instrument used here was 0·89 in a study of caregivers of stroke survivors (39).
Statistical analysis
All statistical analyses were performed using SPSS 14·0 and SAS Version 9·1. Descriptive data for continuous variables are presented as median and interquartile range and for categorical variables as numbers and percentages. Nonparametric tests were used for all further analyses because of the non-Gaussian distribution of the data. Differences between variables from baseline to 12 months were analyzed using the Wilcoxon signed ranks test and McNemar–Bowker test. Explanatory factors for caregiver burden were assessed through univariate analyses using the Spearman correlation, Wilcoxon two-sample test, and the Kruskal–Wallis test. Variables with P≤0·10 were entered into robust multiple linear regression models using backward stepwise method for variable selection. If two determinants were found to be strongly correlated (intercorrelations >0·70), only one was selected for inclusion in the regression analysis. Potentially influential variables such as age and gender were also included. Patients with caregiver respondents (n = 155) and those for whom a caregiver did not complete the BCOS or RSS (n = 290) were compared using the Pearson χ2 and Mann–Whitney tests.
Results
Participation
Between January 2001 and December 2002, 671 patients were admitted to the QEII stroke unit (40). Complete datasets, excluding the BCOS, were available for 155 patients and their caregivers (Fig. 1). Data for the BCOS, introduced after data collection had begun, were available for 143 of the 155 patients and their caregivers.
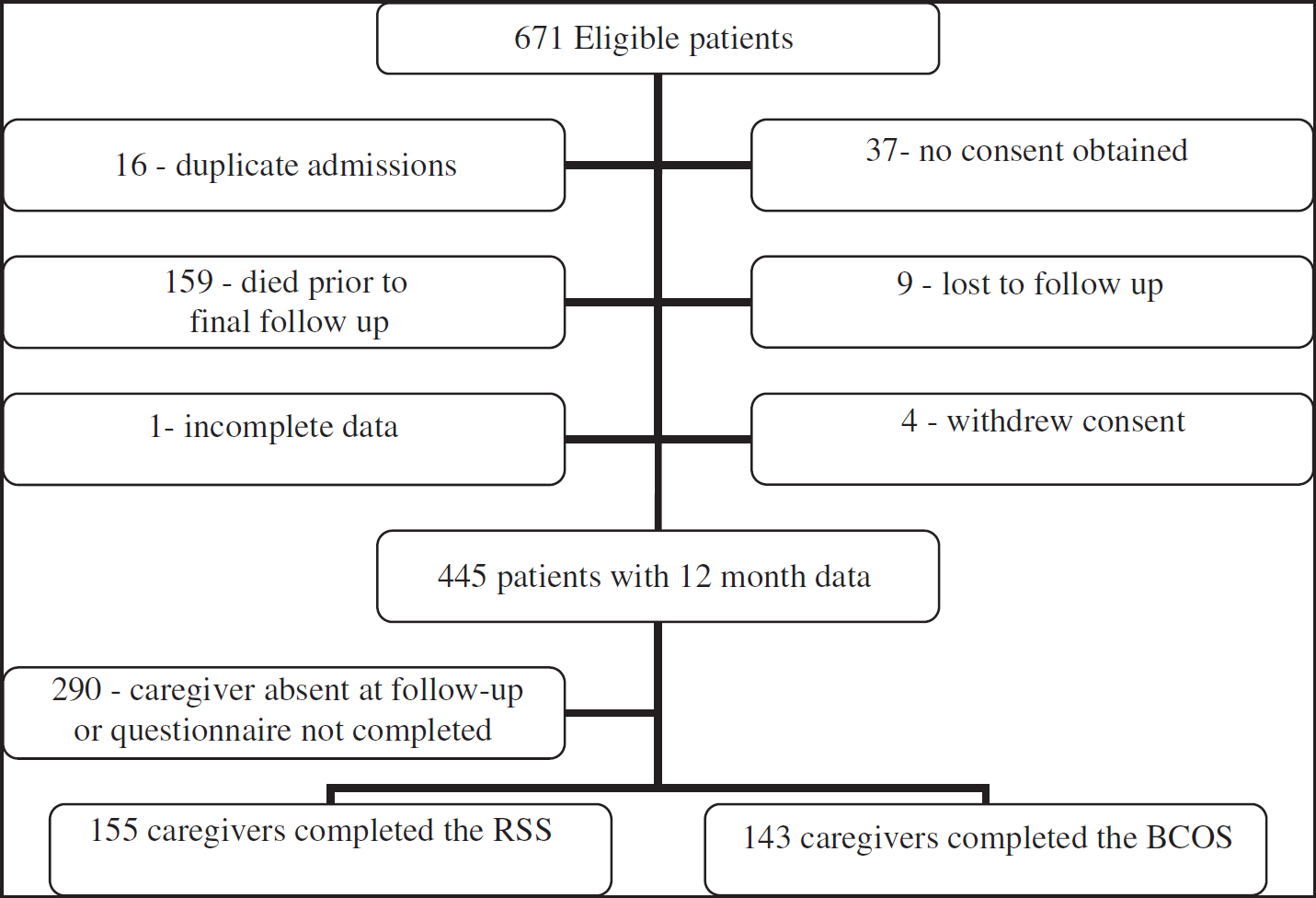
Study participation of patients and caregivers.
The 290 patients for whom a caregiver did not complete the BCOS or RSS were compared with participants to evaluate selection bias. The nonparticipants were significantly younger (mean age 66·3 ± 0·8 vs. 70·4 ± 1·0; P = 0·002) and had significantly lower MRS scores (68·3% vs. 54·5% with a score of 0–2; P = 0·004) (i.e. less handicap). There was no significant difference in sex, marital status, BI at baseline, BI at 12 months, stroke type, stroke severity, or presence of other health problems between the two groups.
Clinical characteristics of participating patients
The demographic characteristics of patients with caregiver data at baseline are summarized in Table 1 . The median patient age was 73 years (range 19–92), 58·7% were male, and 88·4% of patients were married. More than half (61%) of the caregivers were spouses of the care recipients. The clinical outcomes are listed in Table 2 . There was a significant increase in the proportion of patients with BI scores ≥95 between baseline and 12 months (32·9% vs. 61·3%, P<0·0001) indicating greater overall independence in activities of daily living. Median patient scores on clock drawing (12·0 vs. 14·0) and orientation tests (11·0 vs. 12·0) increased significantly from baseline to 12 months (P<0·0001) indicating an overall improvement in those measures of cognitive function.
Patient characteristics at baseline
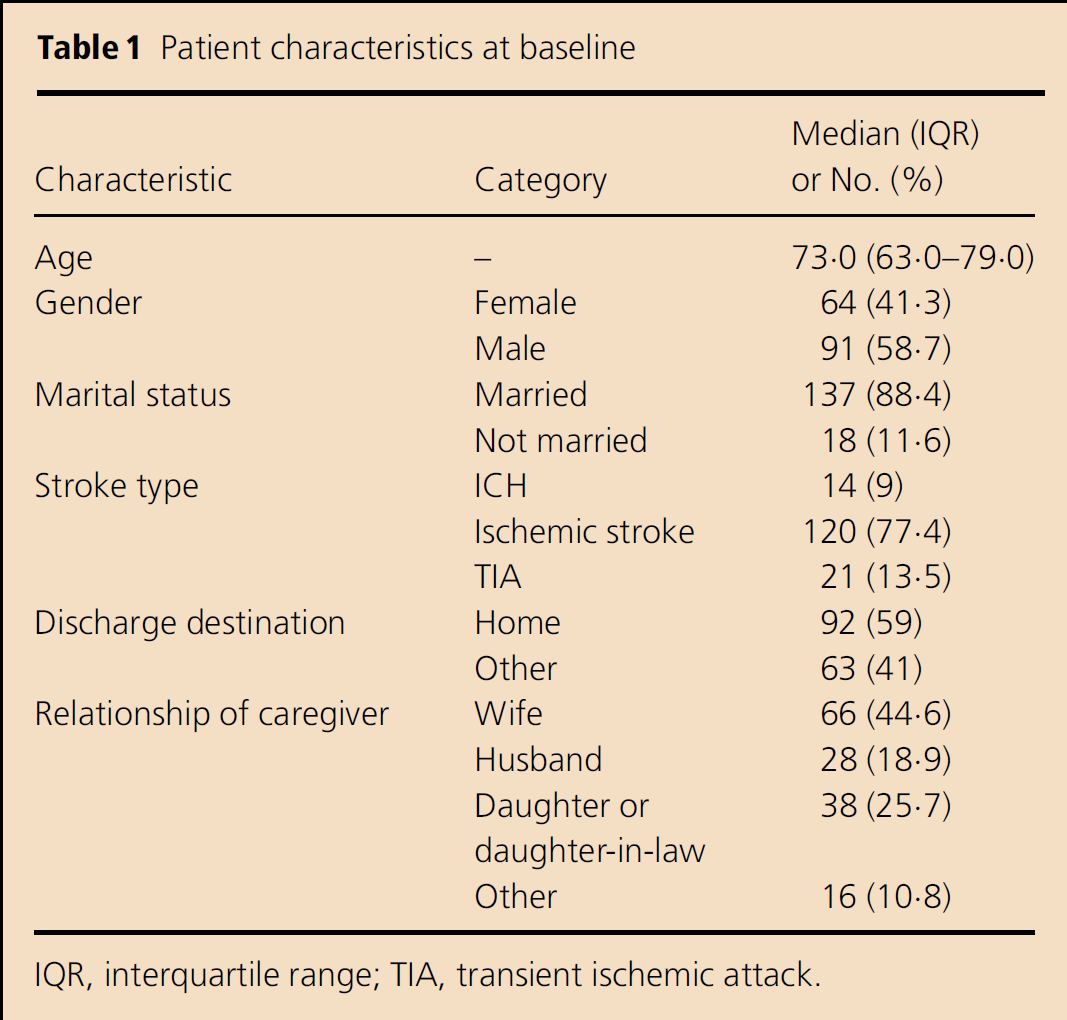
IQR, interquartile range; TIA, transient ischemic attack.
Patient outcomes at baseline and 12 months (n = 155)
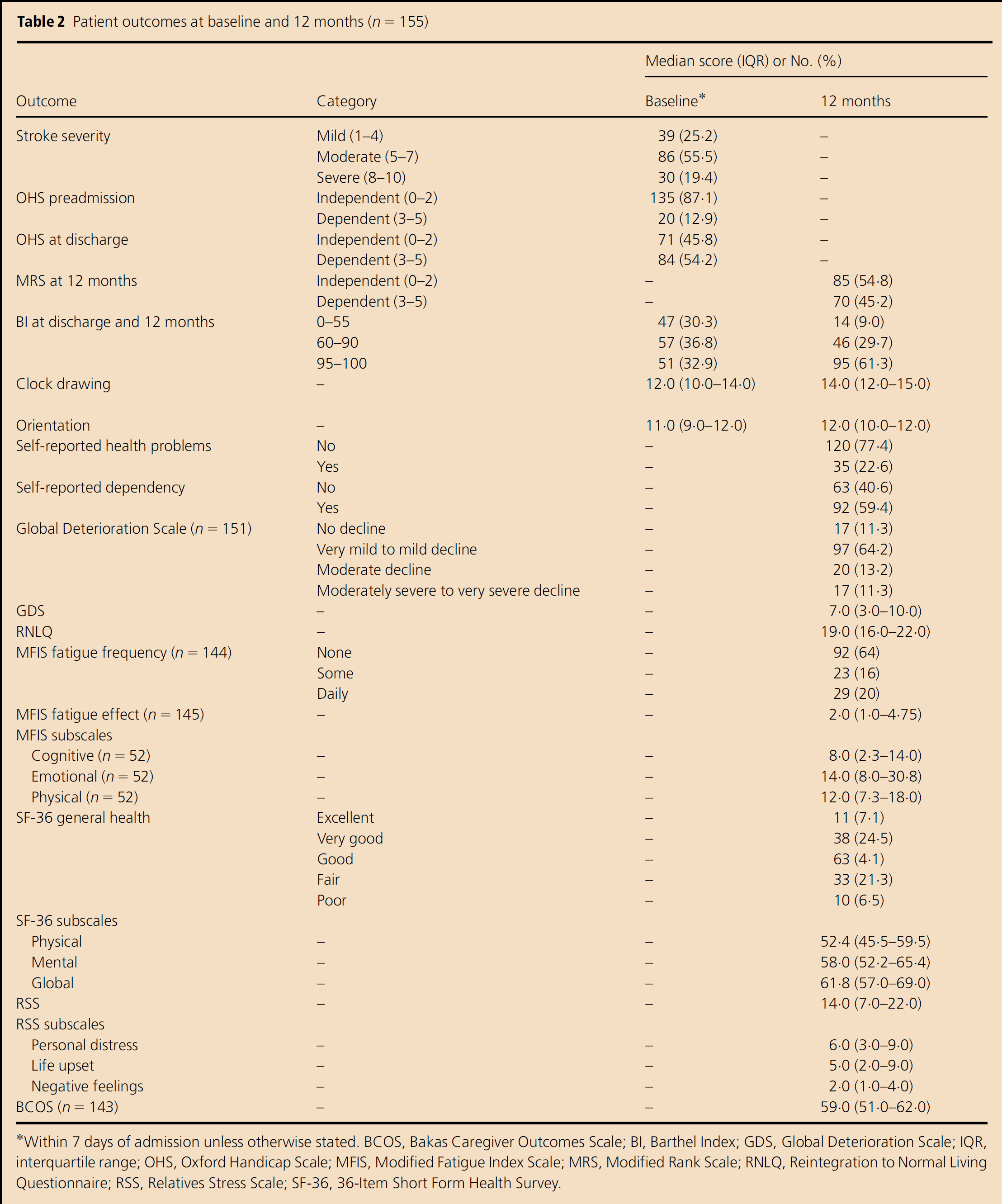
Within 7 days of admission unless otherwise stated. BCOS, Bakas Caregiver Outcomes Scale; BI, Barthel Index; GDS, Global Deterioration Scale; IQR, interquartile range; OHS, Oxford Handicap Scale; MFIS, Modified Fatigue Index Scale; MRS, Modified Rank Scale; RNLQ, Reintegration to Normal Living Questionnaire; RSS, Relatives Stress Scale; SF-36, 36-Item Short Form Health Survey.
Baseline and 12-month correlates of caregiver burden
All patient characteristics and outcomes were entered into univariate analyses to determine their relationship to caregiver burden. Significant (P<0·10) correlates of caregiver burden on one or both burden scales (Table 3) were further examined using multiple linear regression analyses. The baseline variables that predicted greater caregiver burden (Table 4) measured by the RSS were urinary incontinence (P≤0·0001) and ischemic stroke (P = 0·031); using the BCOS, significant explanatory factors at baseline were older age (P = 0·008), male gender (P = 0·013), and impaired clock drawing (P = 0·032).
Univariate analysis of baseline and 12-month predictors of caregiver burden
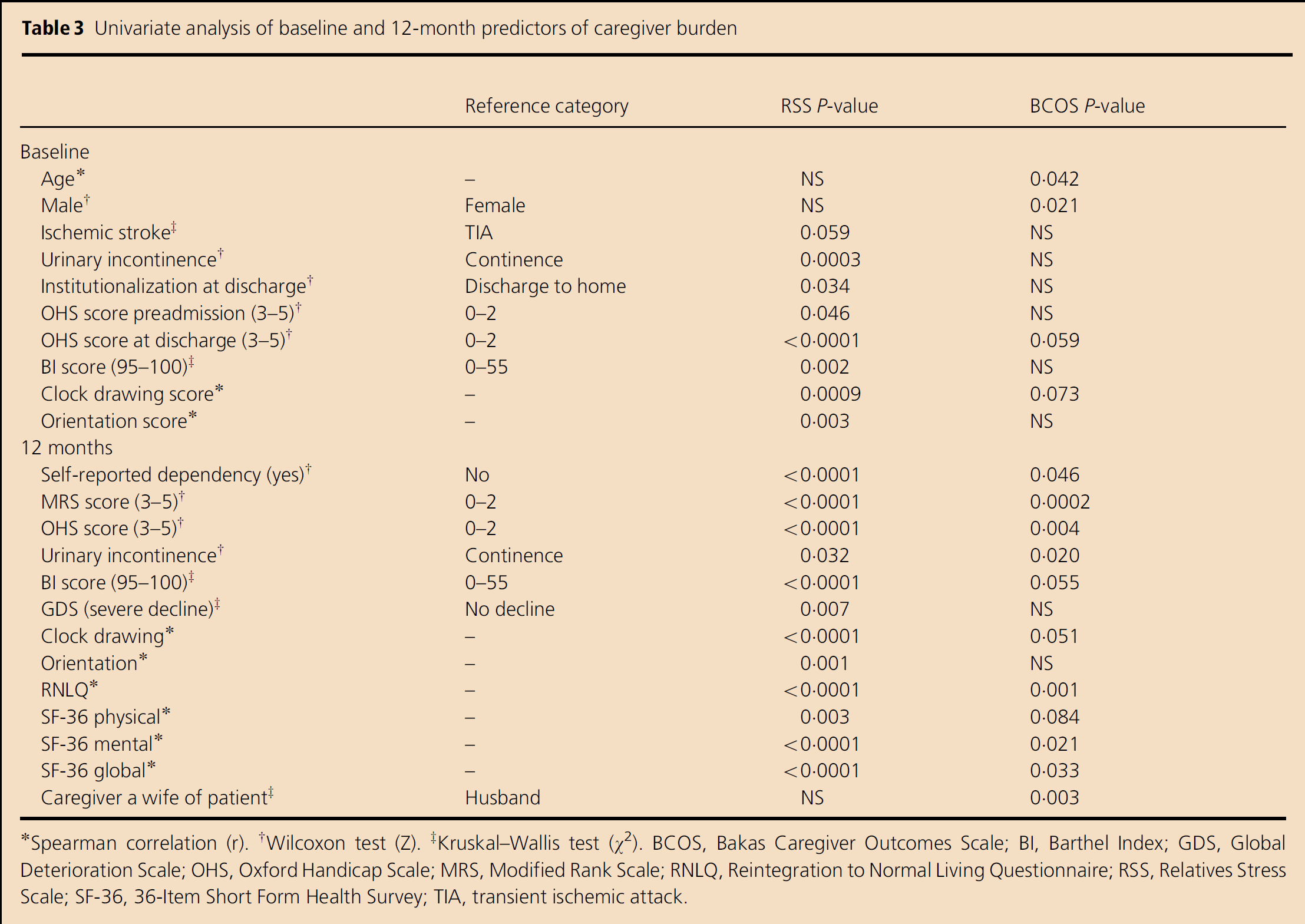
Spearman correlation (r).
Wilcoxon test (Z).
Kruskal–Wallis test (χ2). BCOS, Bakas Caregiver Outcomes Scale; BI, Barthel Index; GDS, Global Deterioration Scale; OHS, Oxford Handicap Scale; MRS, Modified Rank Scale; RNLQ, Reintegration to Normal Living Questionnaire; RSS, Relatives Stress Scale; SF-36, 36-Item Short Form Health Survey; TIA, transient ischemic attack.
Multiple regression analysis of factors affecting caregiver burden
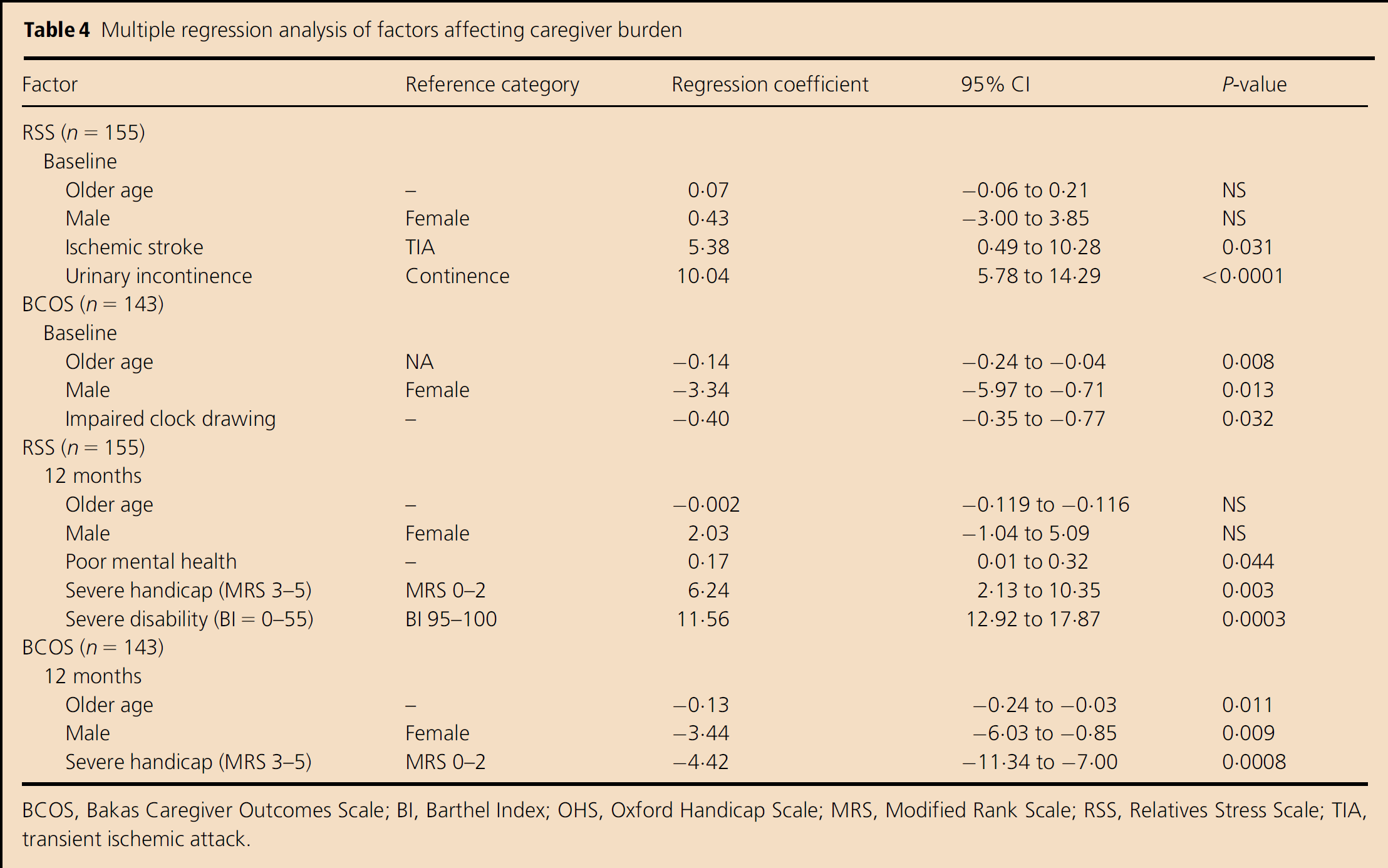
BCOS, Bakas Caregiver Outcomes Scale; BI, Barthel Index; OHS, Oxford Handicap Scale; MRS, Modified Rank Scale; RSS, Relatives Stress Scale; TIA, transient ischemic attack.
At 12 months (Table 4), functional handicap (MRS) (P = 0·0029), functional disability (BI) (P = 0·0003), and poor mental health HRQOL (sub-category of SF-36) (P = 0·044) were correlated with increased caregiver burden on the RSS, whereas male gender (P = 0·009), older age (P = 0·011), and functional handicap (MRS) (P = 0·0008) were correlated with greater burden on the BCOS.
Discussion
Markers of impaired functional status (urinary incontinence at baseline and functional disability and handicap at 12 months) were highly correlated with caregiver burden. We also observed an association between increased caregiver burden and patients' cognitive function and mental health status at baseline and at 12 months, respectively. Patient demographic variables (older age and male gender) were significantly correlated with higher levels of caregiver burden at both time points.
The difference between the predictors observed at baseline and the correlates identified at 12 months underscores the complex and evolving nature of caregiver burden. Our findings suggest that factors may contribute differently over time. In this study, patients' functional impairment and poor mental health (SF-36) become increasingly important variables with time. Preexisting factors such as age and gender may have a less dynamic role.
The explanatory factors of burden identified differed somewhat between the two burden scales. This may be explained by the distinctive approaches taken by developers of the instruments. The RSS quantifies the degree of caregiver upset but does not emphasize the practical impact of caregiving. In contrast, the BCOS measures life changes that result from providing care. Our data suggest that caregiver upset/distress (RSS) is more strongly correlated with the functional impairment of care recipients and may reflect the shared emotional impact of functional loss. Life changes (BCOS) have a greater association with demographic variables (older patient age and male gender). Gender roles that help define caregiver function in different generations may have contributed to the observed differences.
The regression models used in this study were able to explain only a small proportion of the variance of caregiver burden (indicated by values of 0·07, 0·09, 0·13, and 0·27). The R2 values derived from our analyses are comparable to those reported in other studies that have examined patient characteristics alone in predicting caregiver burden (11, 12). Caregiver characteristics and social support factors have been shown to have a significant influence on caregiver burden (10, 11). Our models present a paradigm for caregiver burden with an emphasis on patient characteristics. Models with greater predictive value likely require analysis of more diverse variables such as caregiver factors, social supports, personal beliefs, coping skills, etc.
A review of the literature revealed three studies that have evaluated patient factors present in the immediate aftermath of stroke. Visser-Meily et al. (19) demonstrated that patients' functional disability (BI) was predictive but that impaired cognitive function (Mini Mental State Examination score) was not. Using the same outcome scales for functional disability and cognition, a study by Thommessen et al. (18) found the opposite – impaired cognitive function predicted future caregiver burden but functional disability did not. A third study found that better motor function at the time of stroke (measured by the Glasgow Coma Scale) and urinary continence were inversely correlated with the development of caregiver strain (8).
A number of studies have considered concurrent factors associated with caregiver burden following stroke. As in our study, two report an association between general measures of poor patient mental health and elevated caregiver burden (14, 17); one shows no significant relation (41). Two studies report a correlation between younger patients and increased caregiver burden (9, 38), while one study reports no significant correlation (12). We demonstrate a positive correlation between patients' functional handicap and caregiver burden but evidence in the literature is mixed with respect to the significance of this factor. A number of studies have used the MRS as a measure of handicap with mixed results; two show a positive relationship (10, 11) and an equal number show no significant correlation (12, 18).
A methodological critique of the studies reviewed reveals a number of study limitations that may explain the inconsistencies reported. First, many different instruments were used in these studies to measure caregiver burden but they are not all clinically validated in stroke patients nor are the psychometric properties always established for this population. Second, many of the studies examined selected populations of stroke patients and caregivers defined by specific cultural and demographic characteristics. Sampling bias restricts the generalizability of the results. Finally, most studies evaluate small sample sizes and therefore lack the statistical power to make meaningful conclusions.
The strengths of our study are the large number of participants, longitudinal design, wide range of patient predictor variables examined, and long follow-up period. There are also some limitations. Our data are restricted to patient factors and do not account for the complex interplay of caregiver and patient characteristics. Further, our patient population excludes nonconsenting patients, those who died in the 12-month period poststroke, and those for whom a caregiver was not available or willing to complete the questionnaire. The consenting participants in our study were older and in worse functional health than the consenting nonparticipants which may have resulted in an overestimation of burden. A common reason for nonparticipation in this study was absence of a caregiver to complete the questionnaire. It is likely that patients unaccompanied by a caregiver had greater functional independence. Consequently, the care recipients in this study likely required greater time and effort caring, both of which have been linked in other studies to greater subjective burden (8–11).
The ability to predict and identify caregivers in need of training and support has important implications for practice. Caregiver burden is a significant health care concern and the adverse effects may be diminished through primary and secondary prevention programs. Risk factors for caregiver burden must be identified so that effective policies and interventions can be devised. In this study, we have identified patients' functional status as a strong predictor of caregiver burden. Functional outcomes are easily assessed and should be evaluated in all stroke survivors to help guide their management while at the same time being mindful of the needs of caregivers. The development of caregiver supports is increasingly important as advances in stroke care continue to improve patient survival.