
Abstract
Caregiver burden following stroke is increasingly recognised as a significant health care concern. A growing number of studies have evaluated the patient, caregiver, and social support factors that contribute to increased caregiver burden. We conducted a systematic review of this literature to guide future research. A search of the MEDLINE, PsyclNFO, CINAHL, and EMBASE databases (up to July 2008) and reference sections of published studies using a structured search strategy yielded 24 relevant articles. Studies were included if they evaluated predictors and/or correlates of caregiver burden in the setting of stroke. The prevalence of caregiver burden was 25–54% and remained elevated for an indefinite period following stroke. In studies that evaluated independent baseline predictors of subsequent caregiver burden, none of the factors reported were consistent across studies. In studies that assessed concurrent factors independently contributing to caregiver burden in the poststroke period, patient characteristics and social support factors were inconsistently reported. Several studies identified caregiver mental health and the amount of time and effort required of the caregiver as significant determinants of caregiver burden. Our findings highlight the need for more research to identify caregivers in need of support and guide the development and implementation of appropriate interventions to offset caregiver burden.
Introduction
Stroke is a leading cause of persistent disability and handicap (1). Stroke survivors experience significant functional limitations resulting from decreased mobility, cognitive impairment, depression, and personality changes (2). The considerable psychosocial impact of stroke extends to family members and other unpaid caregivers. Informal caregivers play a pivotal role in maintaining stroke survivors in the community (3, 4) but this often comes at a substantial personal cost.
Many caregivers experience adverse health effects as a result of caring for stroke survivors, caregiving has been linked to higher rates of depression (5, 6), anxiety (4, 7), cardiovascular disease (8), general ill-health (5), and mortality (9). Caregivers, in general, have a poorer quality of life (10) and greater restraints in their social activities (4, 7).
The health consequences of providing care to stroke survivors have important implications for patient well-being. Stroke recovery is optimised if the family is healthy and supportive (11). Individuals at home experience less handicapped than those living in institutional care (12) and supportive family is an important factor in enabling stroke patients to remain in the community (3).
Caregiver burden is a term used to describe the weight or load carried by caregivers as a result of adopting the caregiving role. It can be further distinguished by considering subjective and objective burden. Objective burden refers to the physical assistance provided by caregivers in the form of caregiving tasks that are performed. Subjective burden refers to the psychological, social, and emotional impact on caregivers as a consequence of objective burden (13).
A number of studies have considered how patient, caregiver, and support characteristics contribute to both subjective caregiver burden in the context of stroke, but these critical contributions to our understanding have not been systematically evaluated and summarised. The objective of this article is to identify determinants of caregiver burden following stroke through a systematic review and analysis of the existing literature.
A computer search of the MEDLINE database was conducted using the MeSH terms, ‘cerebrovascular disorders’ and ‘caregivers’ and the words ‘burden’, and/or ‘strain.’ Our search yielded 119 articles. The terms ‘stroke’ and ‘caregiver burden’ were entered into the CINAHL database (207 articles); ‘cerebrovascular accidents’ and ‘caregiver burden’ were used in PsycINFO (95 articles); and ‘stroke’ and ‘caregiver’ and ‘burden’ were used in EMBASE (92 articles). Studies were included if they were published before July 2008, evaluated caregiver burden or strain as a dependent variable, and specifically assessed caregivers of stroke survivors. Reviews, clinical practice guidelines, and empirical studies that focused on topics other than caregiver burden or strain in caregivers of stroke patients were excluded from the review. The abstracts and, if necessary, the full texts were reviewed by a single reviewer who found that 23 studies met the inclusion criteria. A careful review of the reference sections yielded one additional study (3).
Twenty-four studies were reviewed. The sample size, design, time period studied, relationship of caregivers to patients, outcomes examined, and key findings are outlined in Table 1.
Summary of studies examining caregiver burden or strain in caregivers of stroke survivors
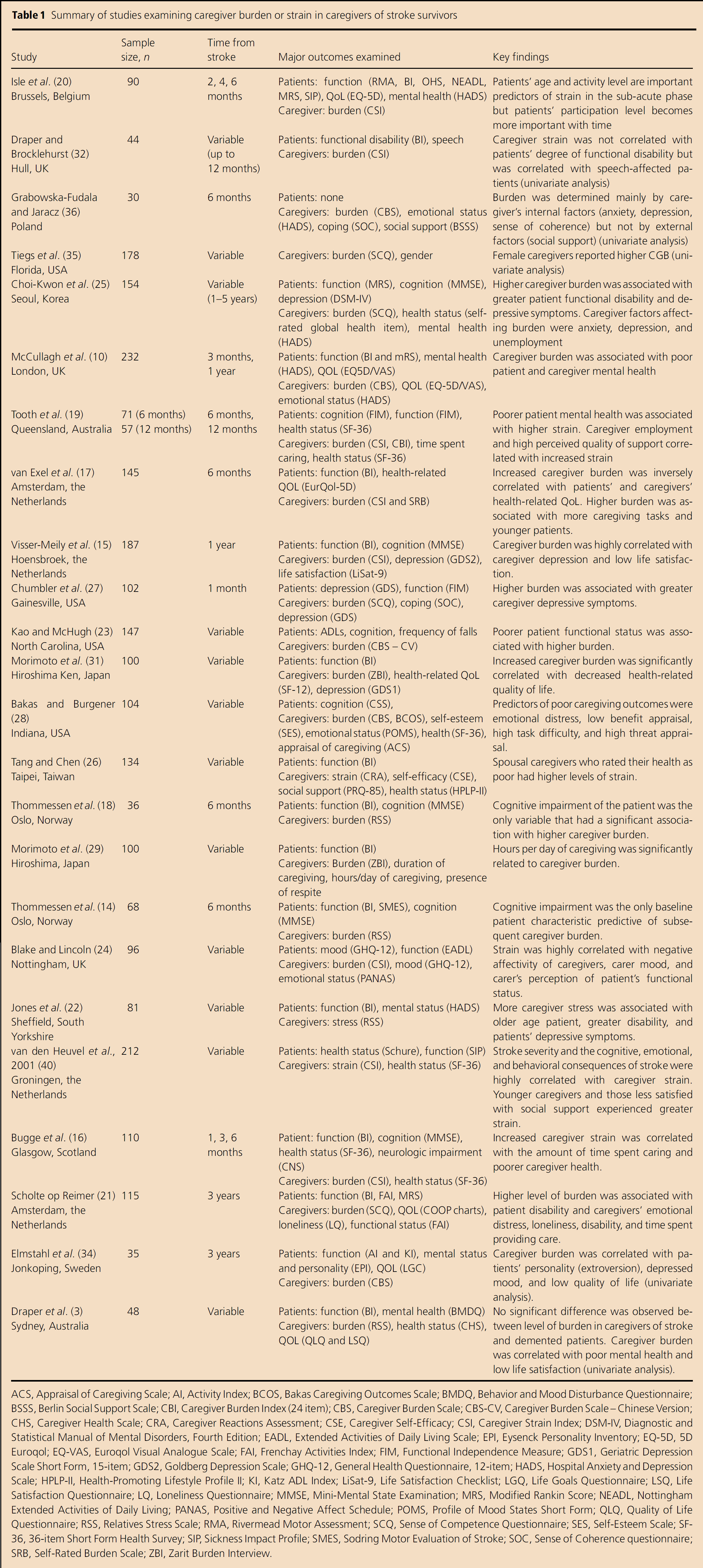
ACS, Appraisal of Caregiving Scale; AI, Activity Index; BCOS, Bakas Caregiving Outcomes Scale; BMDQ, Behavior and Mood Disturbance Questionnaire; BSSS, Berlin Social Support Scale; CBI, Caregiver Burden Index (24 item); CBS, Caregiver Burden Scale; CBS-CV, Caregiver Burden Scale – Chinese Version; CHS, Caregiver Health Scale; CRA, Caregiver Reactions Assessment; CSE, Caregiver Self-Efficacy; CSI, Caregiver Strain Index; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; EADL, Extended Activities of Daily Living Scale; EPI, Eysenck Personality Inventory; EQ-5D, 5D Euroqol; EQ-VAS, Euroqol Visual Analogue Scale; FAI, Frenchay Activities Index; FIM, Functional Independence Measure; GDS1, Geriatric Depression Scale Short Form, 15-item; GDS2, Goldberg Depression Scale; GHQ-12, General Health Questionnaire, 12-item; HADS, Hospital Anxiety and Depression Scale; HPLP-II, Health-Promoting Lifestyle Profile II; KI, Katz ADL Index; LiSat-9, Life Satisfaction Checklist; LGQ, Life Goals Questionnaire; LSQ, Life Satisfaction Questionnaire; LQ, Loneliness Questionnaire; MMSE, Mini-Mental State Examination; MRS, Modified Rankin Score; NEADL, Nottingham Extended Activities of Daily Living; PANAS, Positive and Negative Affect Schedule; POMS, Profile of Mood States Short Form; QLQ, Quality of Life Questionnaire; RSS, Relatives Stress Scale; RMA, Rivermead Motor Assessment; SCQ, Sense of Competence Questionnaire; SES, Self-Esteem Scale; SF-36, 36-item Short Form Health Survey; SIP, Sickness Impact Profile; SMES, Sodring Motor Evaluation of Stroke; SOC, Sense of Coherence questionnaire; SRB, Self-Rated Burden Scale; ZBI, Zarit Burden Interview.
Instruments to assess caregiver burden/strain
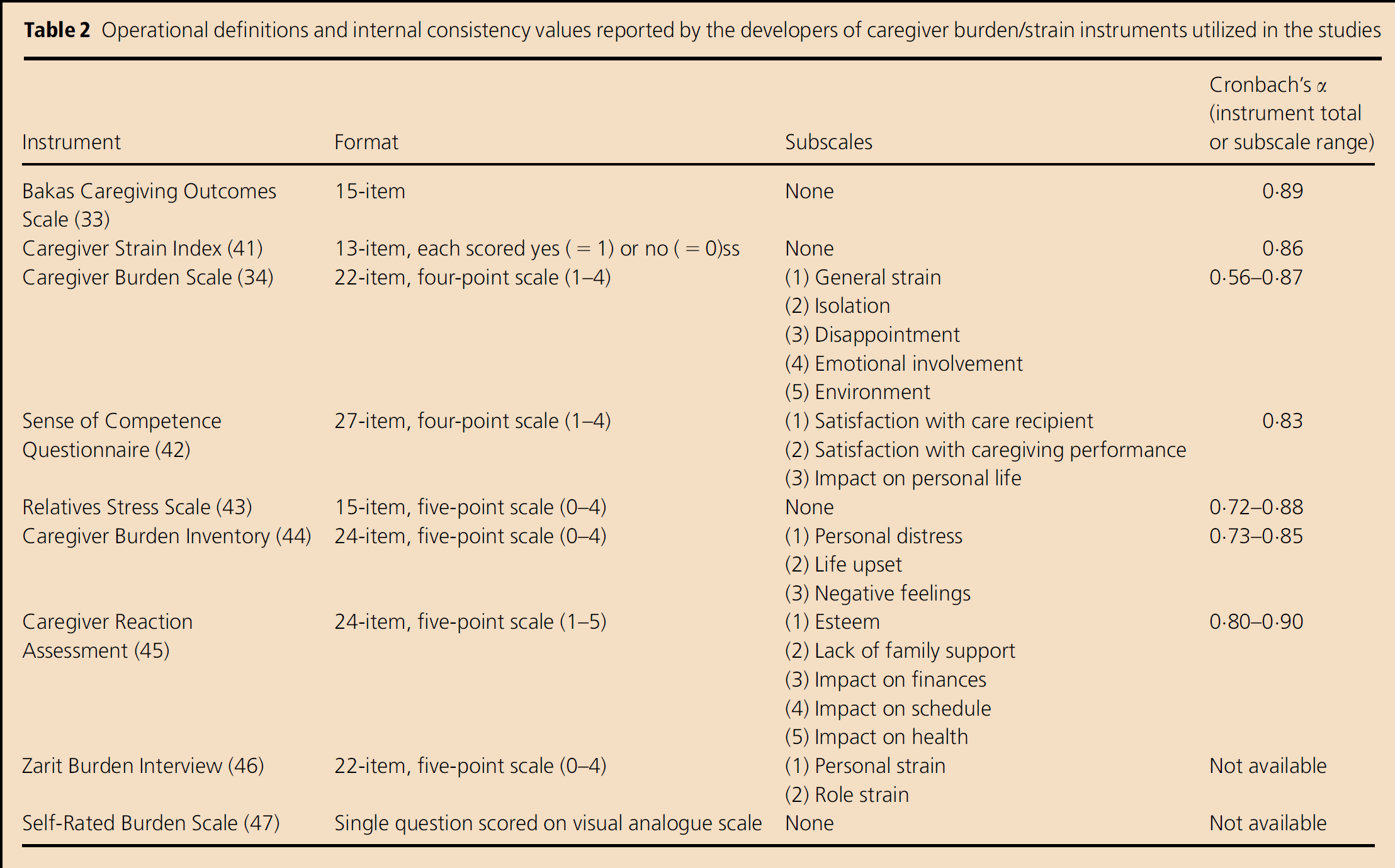
Nine different instruments were used to measure caregiver burden in the 24 studies (Table 2).
Operational definitions and internal consistency values reported by the developers of caregiver burden/strain instruments utilized in the studies
The instruments most frequently used:
Caregiver Strain Index (CSI, n = 8),
Relatives Stress Scale (RSS, n = 4),
Caregiver Burden Scale (n = 3), and
Sense of Competence Questionnaire (n = 4).
Other instruments included:
Caregiver Burden Inventory (n = 1),
Caregivers Reaction Assessment (n = 1),
Zarit Burden Interview (n = 2),
Self-Rated Burden Scale (SRB, n = 1), and
Bakas Caregiving Outcomes Scale (n = 1).
Several studies used more than one instrument. Most of the instruments have been evaluated for internal consistency through calculation of the coefficient of reliability (Cronbach's α) (Table 2).
Prevalence of caregiver burden
Seven of the 24 studies reviewed, evaluated the prevalence of caregiver burden (14–20). The proportion of caregivers experiencing significant burden ranged from 25% (moderate or considerable burden on nine or more items on the RSS) (14, 18) to 54% (total score on the CSI>6) (15). Three studies reported the changes in prevalence of significant caregiver burden over time. Bugge et al. (16) demonstrated that 25% of caregivers were under significant burden at 1 month, 28% at 3 months, and 37% at 6 months. The other two studies did not show an increase in prevalence of burden with time. Isle et al. (20) reported rates of 28%, 31%, and 29% at 2, 4, and 6 months, respectively, while Tooth et al. (19) reported 44% of caregivers under considerable burden at 6 months and 42% at 12 months.
Baseline predictors of caregiver burden
A number of studies have evaluated the potential factors that correlate with caregiver burden poststroke. Some of the studies consider antecedent variables such as patient and caregiver demographics. However, few studies have specifically assessed factors at the time of the stroke that may contribute to subsequent caregiver burden. Three studies addressed baseline predictors of burden. In a study of 187 caregivers of stroke survivors, Visser-Meily et al. (15) found that the patients’ functional dependency (measured by Barthel Index) and caregiver depressive symptoms (measured by the Goldberg Depression Scale) were the only significant predictors at admission of caregiver burden at 1 year. In this study, patients’ cognitive status (measured by the MMSE) was not predictive of subsequent burden. In contrast, Thommessen et al. (14) found that impaired cognitive function (also defined by MMSE score) was the only baseline patient characteristic predictive of caregiver burden at 6 months. In that study, score on the Barthel Index was not associated with subsequent burden. Bugge et al. (16) found that better motor function at stroke onset (measured by the Glasgow Coma Scale) and continence within 7 days of stroke onset were associated with less caregiver strain at 6 months.
Poststroke determinants of caregiver burden
Evidence is mixed with respect to concurrent factors associated with caregiver burden. A number of studies have analysed patient and caregiver variables to determine those that contribute to burden (summarised in Table 3). Only those factors identified by multivariate regression analyses are included in this summary. Four longitudinal studies evaluated the contribution of factors at different time points poststroke (10, 16, 19, 20). In those studies, a variable may have been correlated at one time point but not at another. In such instances, both results are recorded in the table.
Factors examined in relationship to caregiver burden/strain: Number of studies that report a positive, negative, or no correlation
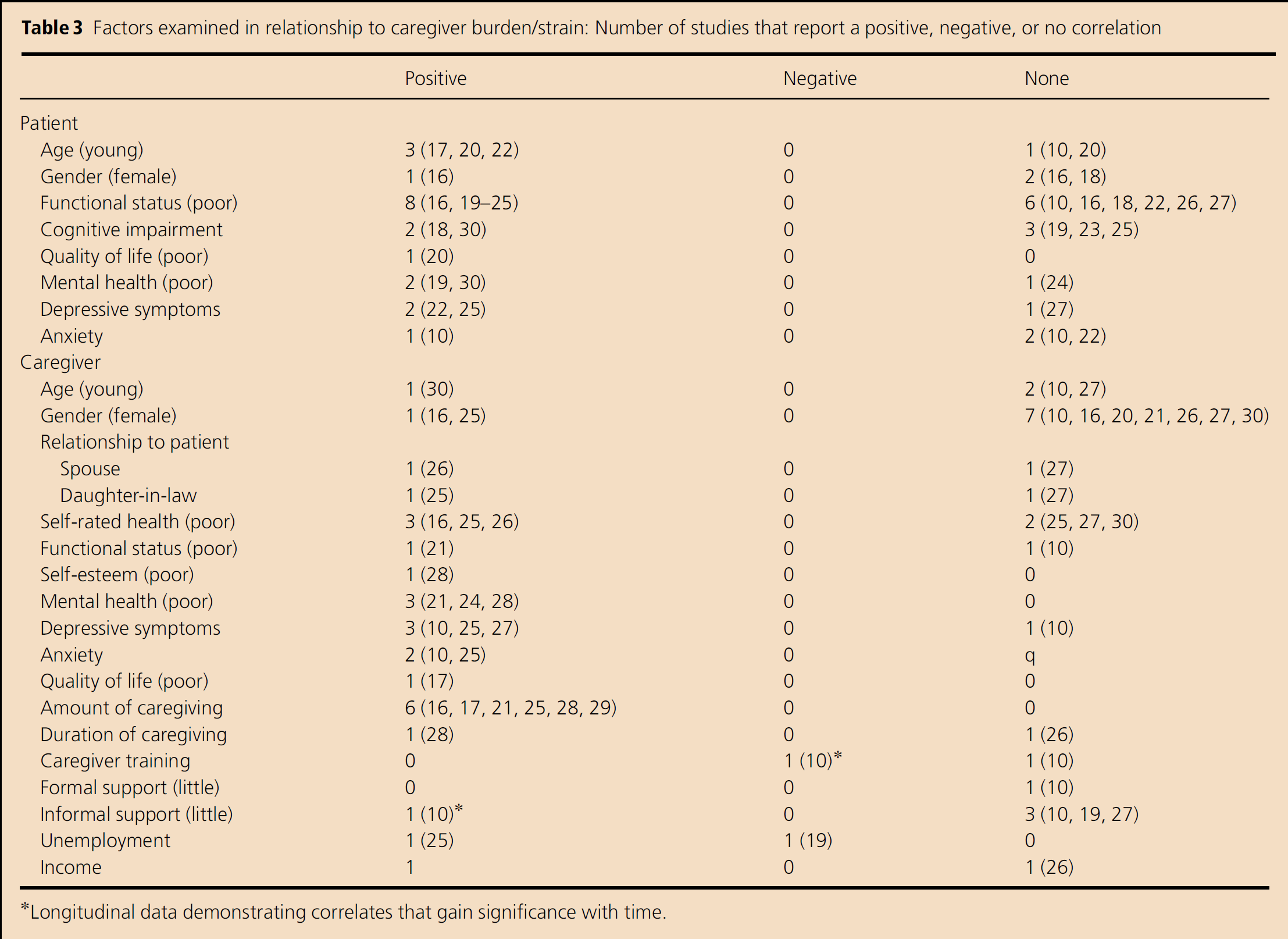
Longitudinal data demonstrating correlates that gain significance with time.
Patient characteristics
A conflicting picture emerges with respect to the impact of functional outcomes on caregiver burden. Eight studies found a positive relationship between poor functional status and caregiver burden (16, 19–25), whereas, six found no significant association (10, 16, 18, 21, 26, 27). Similarly, there is disagreement in the literature over whether patient age, gender, cognitive impairment, and mental health are correlated with increased caregiver burden (Table 3).
Caregiver characteristics
Among caregivers, age and gender are generally shown to be unrelated to increased caregiver burden. Evidence is mixed with respect to the importance of caregiver relationship to patients. Poor mental health [general measures (21, 24, 28) depressive symptoms (10, 25, 27), anxiety (10, 25)] and the amount of caregiving provided (16, 17, 21, 25, 28, 29) are consistently linked with increased burden. However, duration of caregiving is not shown to be a significant correlate (26). Caregiver training has been shown to alleviate caregiver burden in one study (10); other studies suggest that increased family and social support does not (10, 19, 27). The relative contributions of poor self-rated health, functional disability, income, and employment to caregiver burden are unclear (Table 3).
Caregiving and chronic disease
Two studies compared caregivers of stroke patients with other caregivers in order to understand the disease-specific impact of stroke on the caregiving experience. In one study, caregiver burden was significantly correlated with psychological morbidity in caregivers of both dementia and stroke patients (3). In the other study, a lower cognitive function in the patient was associated with high burden in spouses of patients with stroke and Parkinson's disease. In the dementia group, significantly higher burden was identified in caregivers who were female spouses (18).
Discussion
Methodological critique
These studies make valuable contributions to our understanding of a serious and widespread health care concern. However, a number of methodological concerns limit the general application of these findings at this point in time. The inconsistent results reported by the studies reviewed highlight the need for more definitive data on a critical topic in stroke management.
Selection bias
Selection bias is a major limitation in the majority of studies examined. Caregivers who were more highly motivated and in better health themselves may have been more likely to participate. Only three studies performed a statistical comparison of the participants and nonparticipants (17, 19, 21). In each case, characteristics of the consenting and nonconsenting patients were compared and no significant differences were found. However, differences in the characteristics of the caregivers, if present, may have influenced the results. In studies that performed serial outcome measurements, caregivers were excluded if the care recipients died or were placed in long-term care facilities during the interval. These caregivers may have been more physically and emotionally burdened resulting in an underestimation of caregiver burden.
Sampling bias
Many of the studies in this review examined a selected population of stroke patients and caregivers. As a result, data may not be representative of an elderly stroke population with respect to socio-demographic variables and functional status. Thirteen studies restricted the study population to caregivers of stroke survivors living at home (3, 14, 18, 19, 21, 22, 24, 26, 27, 30–33), five also included informal caregivers of patients living in institutions (16, 17, 23, 25, 34), and three studies looked exclusively at caregivers of patients admitted to rehabilitation centre (10, 15, 20). Three studies did not specify the patients’ living situation (29, 35, 36). Stroke survivors living at home are less likely to be severely disabled and, therefore, caregiver burden may be underestimated (12). Furthermore, patient functional status may be a more significant determinant of burden in studies that examine caregivers of severely disabled patients.
Some study populations are defined by specific cultural or demographic characteristics. One study examined caregivers of veterans who are disproportionately male (27). Four studies were conducted in the Netherlands where the majority of stroke patients have a low socio-economic status (30) and 70% of all stroke patients are admitted to hospital (37). Two studies were conducted in Taiwan where most stroke survivors are cared for at home by family members (23, 26).
Publication bias
It is difficult to quantify the impact of publication bias on the results of our systematic review. Language bias was minimised by searching for articles published in languages other than English. We found several studies reporting positive and negative correlations between the same predictive variables and caregiver burden. This suggests that there was not a major bias in favour of publications reporting positive results.
Restricted amount of information gathered
There was wide variability in the datasets considered by the studies reviewed. Some factors that may have important influences on caregiver burden were not consistently assessed. These include the presence and adequacy of community and social service support, patient and caregiver spirituality, and concomitant illnesses of patients and caregivers. Despite a wide range of patient, caregiver, and support variables considered in many of the studies, regression models were unable to account for a significant proportion of the variance in burden as indicated by the R2 (range 17–62·7%) (14, 19).
Lack of longitudinal data
Longitudinal data are necessary to understand the temporal pattern of caregiver burden poststroke. Only four studies examined caregiver burden at serial time points (16, 19, 20, 25). Sequential follow-up studies are required in order to comprehend the changing nature of caregiver burden and the ways in which factors function differently at different times.
Small sample size
Many studies lacked the statistical power to make confident conclusions about the prevalence of caregiver burden and factors that independently correlate with higher levels of burden. Sample sizes for the 18 studies ranged from 35 to 232 (Table 1).
Statistical methods
All but six studies (3, 31, 32, 34–36) used multiple regression analytical methods to assess the complex interrelationships of various caregiver outcomes and determinants. Univariate analysis alone fails to account for the interdependency between variables.
Measures
Caregiver burden is a complex and multidimensional construct that encompasses psychological, emotional, physical, sociological, and economical domains. Many instruments have been developed to measure caregiver burden but they are not all clinically validated in stroke patients nor are the psychometric properties always established for this population. In one study comparing four burden scales, the SRB was recommended as a quick screening tool and the CSI for more complex evaluations of burden. However, further work is needed to develop instruments that reliably measure all aspects of the caregiver experience (38).
Attempts to make meaningful comparisons of the prevalence and determinants of caregiver burden are made difficult by the diversity of instruments used in the assessment. To our knowledge, none of the instruments utilised in these studies have validated cut points for delineating levels of burden. Moreover, in measures of other outcomes, the conventional delineation is not always used. For example, Chumbler et al. (27) uses an MMSE cut-off value of 18 rather than the customary score of 20 to indicate cognitive impairment.
Conclusions
Our findings suggest that proportion of caregivers under considerable burden is significant and remains high for an indefinite period poststroke.
Disagreement exists over which factors independently contribute to increased caregiver burden. The discrepant findings may be explained, in part, by differences in assessment instruments, study populations, sample sizes, and by the restricted amount of information gathered. Despite these limitations, certain variables appear to be persistently correlated with higher levels of caregiver burden. The most consistent patient and caregiver characteristics associated with burden are those relating to mental health (anxiety, depression, and emotional distress). The amount of time caregiving and the number of caregiving tasks performed, sometimes referred to as objective burden (13), are also highly correlated with increased levels of subjective burden. Studies suggest that there is overlap between determinants of burden across chronic disease. In particular, patients’ psychological and cognitive morbidity may be common predictors of burden in caregivers of chronically disabled elderly populations.
Long-term care of stroke patients should include the identification and assessment of vulnerable caregivers in need of support so that appropriate interventions can be implemented. Mental health and objective burden, identified in this review as consistent predictors of caregiver burden, are easily measured and potentially modifiable risk factors. A study by Kalra et al. (39) showed that a training programme for caregivers of stroke patients decreased caregiver burden and reduced anxiety and depression of both patients and caregivers at 1 year. These findings point toward a pressing need for the stroke community to move toward a patient- and caregiver-centred approach so that long-term outcomes for can be optimised (10).