
Abstract
Background
Stroke survivors have less muscle mass in their paretic limbs compared with nonparetic limbs, which may or may not be accompanied by changes in regional and/or whole body fat mass.
Aim
To examine the current evidence regarding differences in regional fat mass between paretic and nonparetic limbs and changes in whole body fat mass over time in stroke survivors.
Methods
A systematic search of relevant databases. Studies measuring whole body or regional fat mass using dual-energy X-ray absorpiometry, computed tomography, or magnetic resonance imaging were included.
Results
Eleven trials were identified. Fat mass differences between paretic and nonparetic limbs and change in fat mass over time were not consistent. Meta-analyses were conducted using dual-energy X-ray absorpiometry-derived data from 10 trials (n = 324). There were no differences in fat mass between paretic and nonparetic legs (pooled mean difference 31.4 g, 95% confidence interval −33.9 to 96.6, P = 0.35), and slightly greater fat mass in the paretic arms compared with nonparetic arms (pooled mean difference 84.0 g, 95% confidence interval 30.7 to 137.3, P = 0.002). Whole body fat mass did not increase significantly between one-month and six-months poststroke (pooled mean difference 282.3 g, 95% confidence interval −824.4 to 1389, P = 0.62), but there was an increase between six- and 12 months poststroke (pooled mean difference 1935 g, 95% confidence interval 1031 to 2839, P < 0.001).
Conclusions
There were inconsistent findings regarding changes in fat mass after stroke. Large, well-designed studies are required to further investigate the impact of body composition changes on the health of stroke survivors.
Introduction
A recent systematic review (1) found strong evidence that people later after stroke (at least six-months) have significantly less muscle mass in their paretic limbs: in the order of 4% in the legs and 8% in the arms. An increase in lipid deposition in and around muscle fibers is a feature of muscular atrophy (2). Furthermore, muscle biopsy studies have found infiltration of lipids into muscle fibers in paretic limbs of people after stroke (3). Other studies have demonstrated an increase in the amount of low-attenuation muscle tissue on computed tomography (CT) slices of the paretic thigh (4), which is indicative of increased fat content within muscles (5). Therefore, it was hypothesized that stroke survivors may have an increase in regional fat mass in the paretic limb later after stroke and/or an increase in whole body fat mass over time.
The composition of muscles, particularly muscle fiber type and fat content, directly impacts on the ability of the body to metabolize glucose. Loss of muscle mass as well as increased fat content within muscles has been linked to greater insulin resistance, poor physical fitness, and greater risk of cardiovascular disease (5–7). More than 80% of stroke survivors have impaired glucose metabolism (8) and this has been linked to a twofold to threefold increase in the risk of recurrent stroke (9). Among healthy, sedentary adults with a range of body mass index scores, insulin-stimulated glucose disposal is negatively correlated with body fat mass, visceral fat, subcutaneous abdominal fat, and thigh fat (5). However, increased fat content within the thigh musculature (as evidenced by low-attenuation tissue on CT slices of the mid-thigh) has been shown to be the single strongest correlate of insulin resistance (5). Others (6) also found a positive correlation between mid-thigh low-attenuation tissue and fasting concentration of glucose in healthy sedentary women, but this was no longer significant after controlling for total body adiposity and age.
Before effective interventions to address changes in body composition after stroke can be developed, the incidence, rate, and magnitude of the changes in both fat and muscle must be known. We recently published a systematic review examining the current evidence for changes in muscle mass in stroke survivors (1).
Aim
The aim of this review is to examine the available evidence for changes in whole body and regional fat mass in people after stroke.
Methods
We searched the following databases from inception until 2 May 2010: Ovid (Medline, Ageline, Embase classic, and Embase, AMED Allied and Complementary Medicine), Cumulative Index of Nursing and Allied Health, Cochrane Library, and Web of Knowledge. Search terms were based on the population of interest (e.g. stroke, cerebrovascular accident, brain injury, hemiplegia) and the construct of interest (e.g. muscle or lean mass, fat mass, intramuscular, body composition, body dimensions). Search terms were truncated according to each database and combined. Searches were limited to humans and English language. The full search strategy for Ovid databases is included in Appendix 1. We sent the final list of included studies to five content experts for validation. We examined the reference lists of all included studies and the reference lists of all related literature or systematic reviews retrieved in the search. Gray literature and other unpublished sources were not searched.
Studies that had measures of fat mass or fat volume, derived from adult human stroke survivors were included. Only measures of fat mass or volume using gold standard methods [dual-energy X-ray absorptiometry (DEXA), CT, or magnetic resonance imaging (MRI)] were included, whereas body composition determinations by bioelectric impedance analysis or anthropometry were excluded. In cases where DEXA scans were reported but fat mass data were not reported, authors were contacted and invited to share raw data. There were no restrictions on study design. For intervention studies, only baseline or control group data were considered.
The full search results were reviewed by title and abstract by one reviewer. The full texts of all potentially eligible articles were independently reviewed by two reviewers. Any disagreements were resolved by discussion. Included articles were critically appraised for risk of bias by two reviewers. Four key criteria considered to have potential to introduce bias were risk of bias in recruitment, whether measurement of body composition was the primary aim of the study, whether assessors or those interpreting imaging data were blinded to either the aim of the study or the side of hemiplegia, and whether adequate steps were taken to minimize sources of error in the measurement technique. These criteria are identical to those used in our previous systematic review of changes in muscle mass after stroke (1). Data from all studies were extracted and synthesized narratively.
Where there were sufficient data available, either published or provided by authors, meta-analyses were performed using the review software package Revman5. The generic inverse variance method of meta-analysis was used as data were paired (10). This involved imputing an assumed correlation between measures taken from the paretic and nonparetic limbs. Based on raw data provided (11,12), a correlation of 0.9 was imputed for the leg comparisons and a correlation of 0.8 imputed for the arm comparisons. The statistical heterogeneity of each meta-analysis was assessed using the I2 statistic. Where I2 > 50%, sensitivity analyses were performed to investigate sources of heterogeneity. Where medians and interquartile ranges were reported rather than means and standard deviations, standard methods for conversion were used.
Results
Figure 1 shows the flow of trial selection. A total of 2232 records were examined by title and abstract. Of these, 66 potential articles were reviewed by full text. A total of 54 trials were excluded, leaving 12 articles (11 trials) to be included in the review. Two of these articles reported from the same trial (13,14). Table 1 summarizes the included studies. There were a total of 352 participants in the 11 trials, with mean ages ranging from 62.5 to 75.0 years (4,7,11–20). Seven of the trials were cross-sectional, where measures were taken from the paretic and nonparetic limbs at one point (4,7,11–14,16,19). In the remaining four trials, measures of fat mass were taken at several time points relative to stroke onset (15,17,18,20). In two of these trials (15,18), fat mass was reported for the paretic and nonparetic limbs separately at each time point. Mean stroke latency of participants in the cross-sectional trials ranged from six-months (16,19) to five-years (11,13,14). In the majority of cross-sectional trials, only people who were able to walk were included (4,7,11,13,14); in all other trials, either the level of participant functional ability was not reported (16,19) or people with a range of abilities were included (12,17). One trial included only people still unable to walk at three-months poststroke (18). In the four longitudinal studies, measures of body composition were made at various time points including one-week (17), one-month (20), three-months (18), six- to seven-months (15,17,18,20), and one-year (17,18,20) poststroke. In all the trials, DEXA scans were used to measure body composition. In one trial (7), CT scans of the mid-thigh were also taken, and the area of low-density lean tissue was measured.
Characteristics of included studies
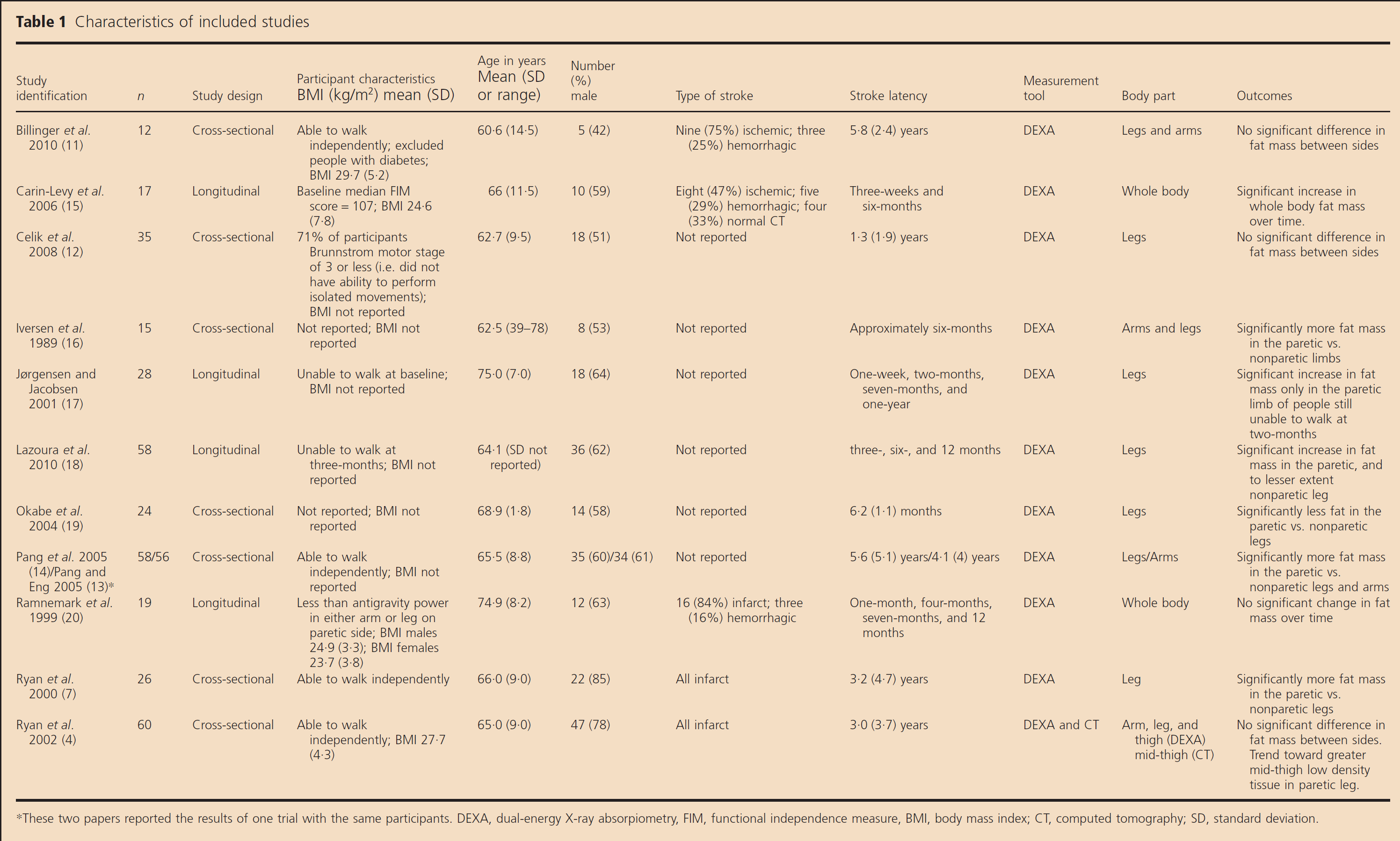
These two papers reported the results of one trial with the same participants. DEXA, dual-energy X-ray absorpiometry, FIM, functional independence measure, BMI, body mass index; CT, computed tomography; SD, standard deviation.
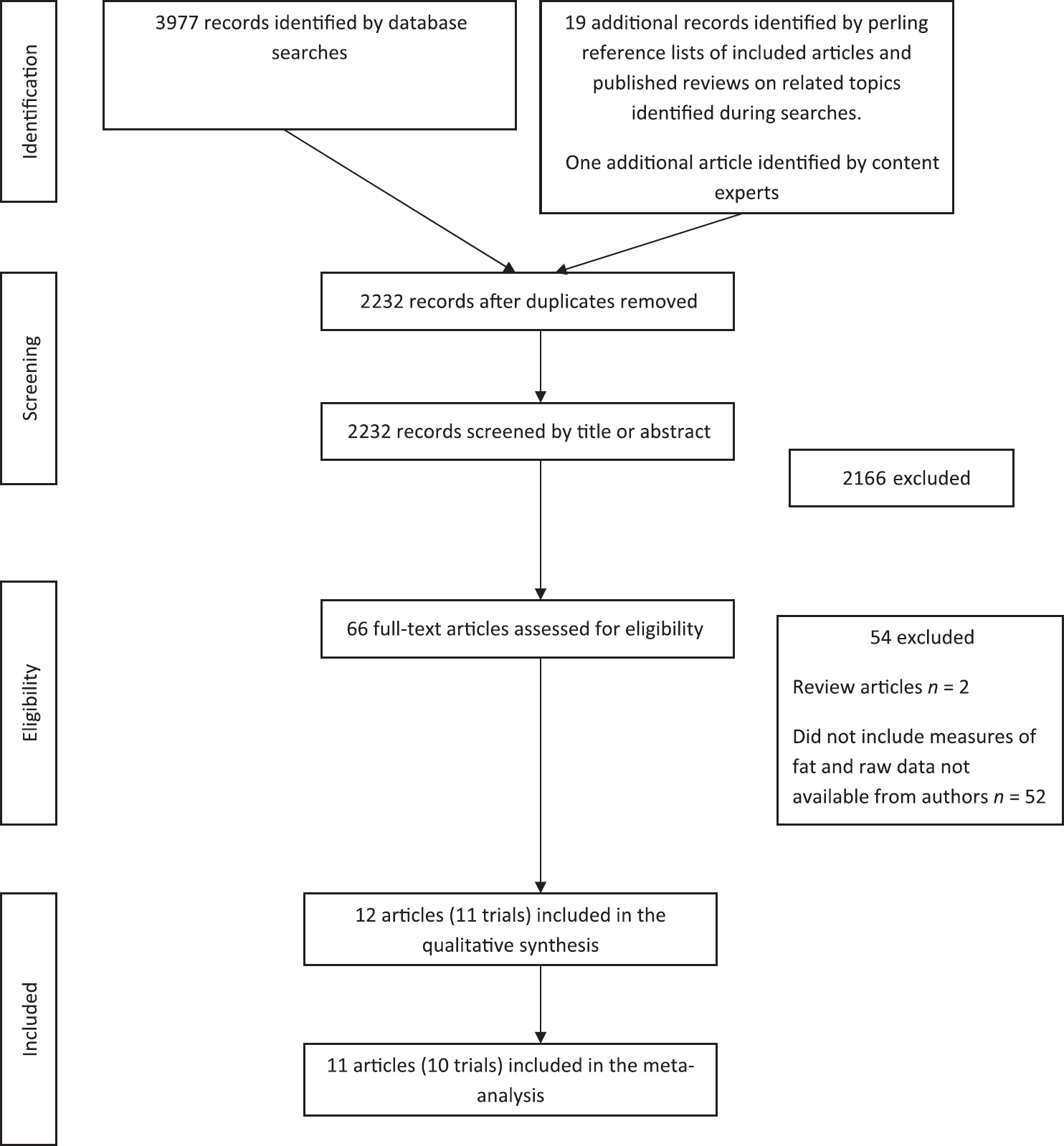
Flow chart of study inclusion.
The risk of bias in the included trials was rated as moderate to high. Blinding of the technicians taking the measures to the side of hemiparesis was reported in only one trial (17) and also occurred in two others (4,7). Only four of the 11 trials could be considered free of selection bias (i.e. used consecutive or random sampling methods). In the majority of trials (nine out of 11), investigation of either changes in body composition over time or differences between paretic and nonparetic limbs was a primary aim of the study. Finally, eight of the 11 trials either adequately reported or later confirmed the methods by which error was minimized in the measurement procedures (e.g. by reporting use of the standard positioning, the same technician, averages of two scans, or determination of the coefficient of variation of DEXA scans). Figure 2 shows the risk of bias assessment for each trial.

Risk of bias of included trials.
Differences between the fat mass in paretic and nonparetic limbs were not consistent across studies. In three trials, fat mass was greater in the paretic arm compared with the nonparetic arm (11,13,16), which contrasts with one trial where fat mass was greater in the nonparetic arm (15). In five trials, fat mass was greater in the paretic leg compared with the nonparetic leg (7,13–15,18), but in three trials, fat mass was greater in the nonparetic leg (11,12,19). In one trial, there were no differences found between sides (4).
For longitudinal studies, there were also inconsistent findings. In one trial, no significant changes in whole body fat mass were found between measures taken at one-month poststroke and measures taken at 12 months poststroke (20). However, in two other trials, an increase in whole body fat mass was found between three-weeks and six-months poststroke (15) and between three-months and six-months (18), and to a lesser extent, after a longer period of follow-up (six- and 12 months poststroke) (18). Lazoura et al. reported that both the paretic and nonparetic legs increased in fat mass over time, with no difference in the amount of fat mass gain between sides. In contrast, Jorgensen et al. reported an increase in fat mass in the paretic leg only, and only in those participants still unable to walk at two-months poststroke.
Meta-analyses
Data was pooled for the comparison between paretic and nonparetic limbs in participants later after stroke for DEXA measures of fat mass. The results of the meta-analysis of the nine trials (n = 305) in which fat mass in the paretic and nonparetic legs was reported showed an overall nonsignificant difference between sides [pooled mean difference 31.4 g, 95% confidence interval (CI) −33.9 to 96.6, P = 0.35, see Fig. 3]. The statistical heterogeneity of this analysis was high (I2 = 84%). Sensitivity analyses revealed that no single trial contributed significantly to this heterogeneity. The results of the meta-analysis of the five trials (n = 160) in which fat mass in the paretic and nonparetic arms was measured showed an overall statistically significant but very small difference in favor of greater fat mass in the paretic arm (pooled mean difference 84.0 g, 95% CI 30.7 to 137.3, P = 0.002, see Fig. 3). The statistical heterogeneity of this analysis was acceptable (I2 = 39%).
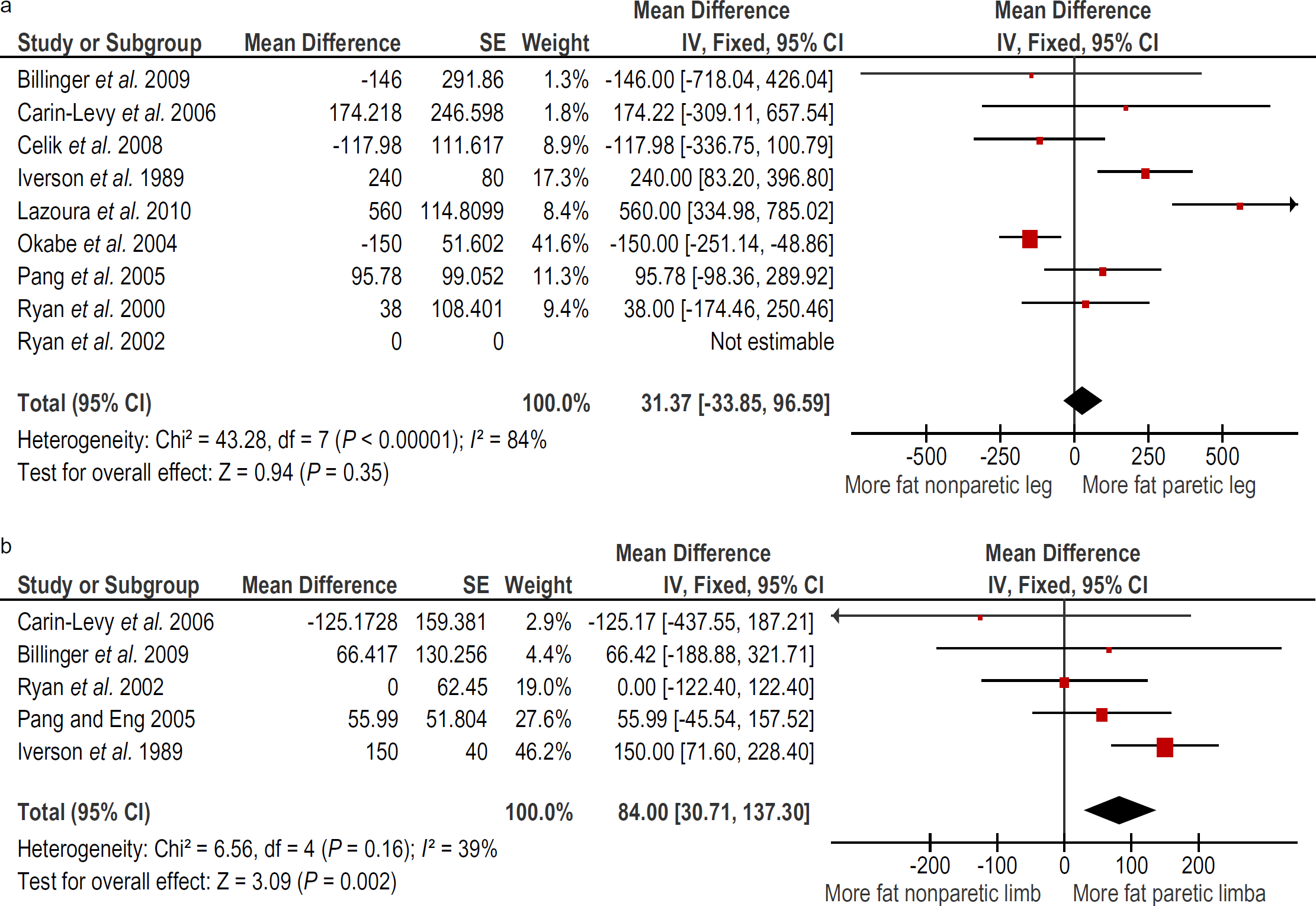
Paretic vs. nonparetic fat mass in the (a) leg and (b) arm.
Data were pooled from two trials (n = 37) (15,18,20) for the change in whole body fat mass between one-month and six-months poststroke. Combining data from these two trials resulted in a nonsignificant change (pooled mean difference 282.3 g, 95% CI −824.4 to 1389, P = 0.62), with a statistical heterogeneity of I2 = 54% (see Fig. 4). Finally, data were pooled from two trials (n = 77) (18,20for change in whole body fat mass between six- (18) or seven-months (20) and 12 months poststroke. The meta-analysis of these two trials found a significant increase in whole body fat mass (pooled mean difference 1935 g, 95% CI 1031 to 2839, P < 0.001) with a statistical heterogeneity of I 2 = 64%.
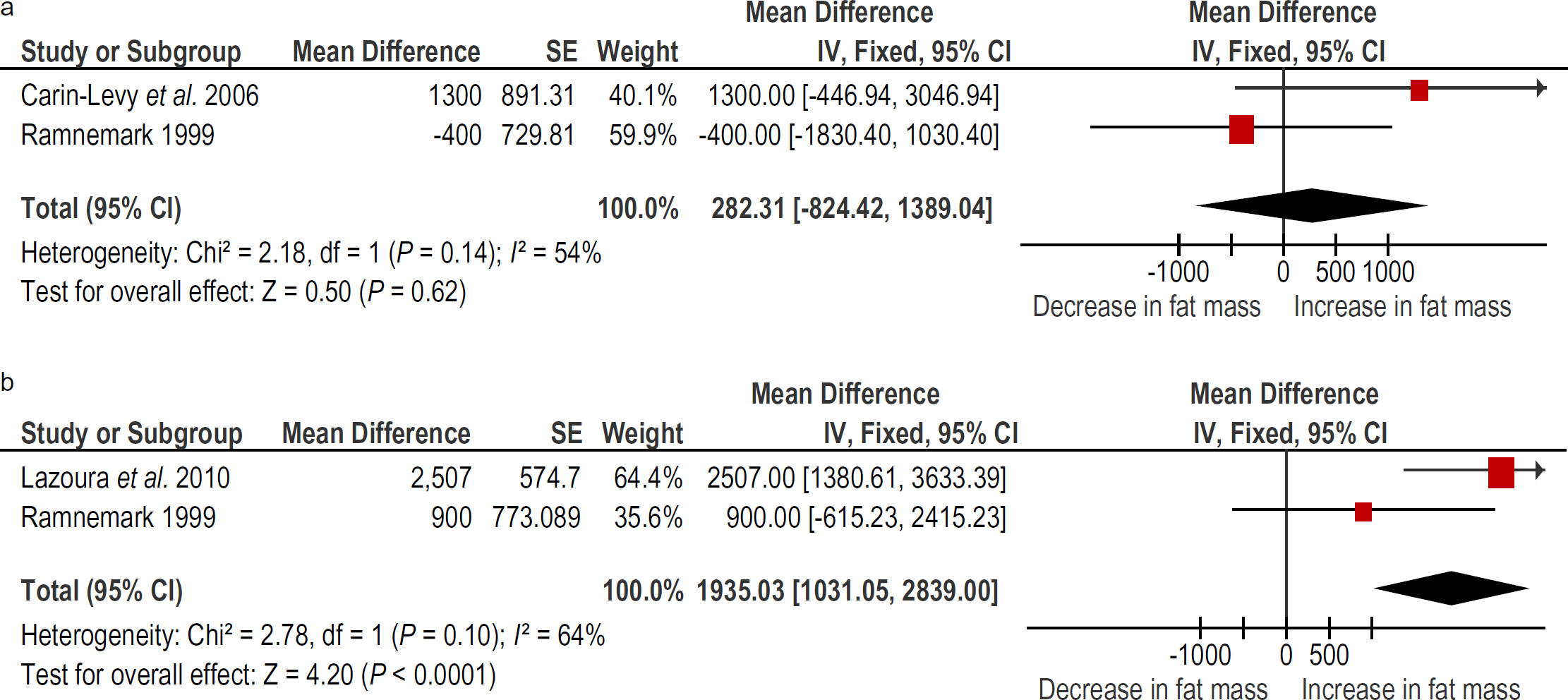
Change in whole body fat mass between (a) one-month and six-months poststroke and (b) six-months and 12 months poststroke.
Discussion
The results of this review demonstrated that there is little difference in regional fat mass between paretic and nonparetic limbs later after stroke. While there was a statistically significant finding in relation to more fat mass in the paretic arm, the magnitude of this difference is likely too small to be of clinical relevance. However, because the findings of individual trials regarding leg fat mass were conflicting, the statistical heterogeneity of this analysis was unacceptably high, and therefore, the results should be interpreted with some caution. The trials included in the review were of reasonably high quality. It is possible that risk of bias may have been overestimated due to lack of reporting of details such as blinding technicians to the side of paresis, use of standard positioning, and coefficients of variation.
There may be several reasons for the disparity in results between trials. It may be that changes in body composition after stroke are highly variable between individuals. However, this cannot fully explain the results; if this were the case, all trials would have reported high variability in their data and an overall nonstatistically significant difference either over time or between limbs. Changes in body composition are likely influenced by a variety of factors including nutritional status, level of physical activity (which, in turn, is strongly influenced by stroke severity), levels of circulating hormonal, and inflammatory factors (21,22). However, no trials reported associations between physical fitness, activity levels, or other potential confounders so their impact on results cannot be determined.
Similarly, the disparity in results of the longitudinal trials may possibly be explained by differences in the level of physical ability among participants. It is well-known that people after stroke participate in very low levels of physical activity both in the early weeks (23) and in the months and years following stroke (24). However, it is likely that those people who retained, or quickly regained the ability to walk after stroke, are less at risk of negative changes in body composition including increases in fat mass. This theory is supported by the results of the trial by Jorgensen et al., who found an increase in fat mass only in the paretic legs of people with persistent walking disability. Currently, it is not possible to speculate on the degree to which changes in body composition are independently related to stroke itself vs. being related to poststroke consequences, in particular inactivity and a reduction in contractile properties of the hemiparetic limbs. Further work is needed to tease out the relationships between degree of stroke-related disability, physical activity levels, and changes in body composition. Poor nutritional status and the presence and degree of control of diabetes mellitus may also play a role.
We identified only one study, which measured muscle tissue using CT – in this case, mid-thigh slices (4). Use of CT imaging allows quantification of low-density lean tissue, which reflects fat content in and around muscle fibers (5). In this study, a significantly greater amount of low-density lean tissue was found in the paretic vs. nonparetic leg. Low-density lean tissue has been related to insulin resistance in healthy men and older women (5,6), but no studies to date have investigated the impact of increased low-density lean tissue of the thigh in stroke survivors on health.
While DEXA is the most commonly used modality to measure whole body and regional fat mass, it has some limitations, including its reliance on estimations of fat mass based on a two-compartment body composition model of fat and fat-free tissue, being less accurate than CT or MRI measures, and not being able to differentiate between fat stored intramuscularly or subcutaneously.
There is some evidence that aerobic exercise can reverse some of the negative changes in body composition after stroke. A randomized controlled trial of a four-week program of robot-assisted treadmill walking demonstrated a significant increase in muscle mass and decrease in fat mass in the intervention group but not in the control group (25). Others have shown that programs of treadmill training improve leg strength (26), cardiovascular fitness (27), and walking ability (28). It is therefore logical to assume that encouraging physical activity very early after stroke may also help ameliorate changes in body composition, but there is as yet no evidence to support this hypothesis.
There is a need for more longitudinal trials involving frequent and accurate measures of body composition starting within the first few weeks after stroke. Such trials should also examine the interactions between stroke severity, physical activity levels, and fitness on changes in body composition. Links between changes in body composition and the metabolic regulation of glucose and how this may impact on risk of future stroke could also be examined. Information gleaned from such trials will inform the development of interventions to ameliorate negative body composition changes.
Footnotes
Acknowledgements
The authors would like to acknowledge the following people who contributed raw data for the meta-analysis: Dr Sandra A. Billinger, Dr Gillian Mead, and associate professor Berna Celik.
Appendix 1: full search strategy for Ovid databases
Characteristics of included studies
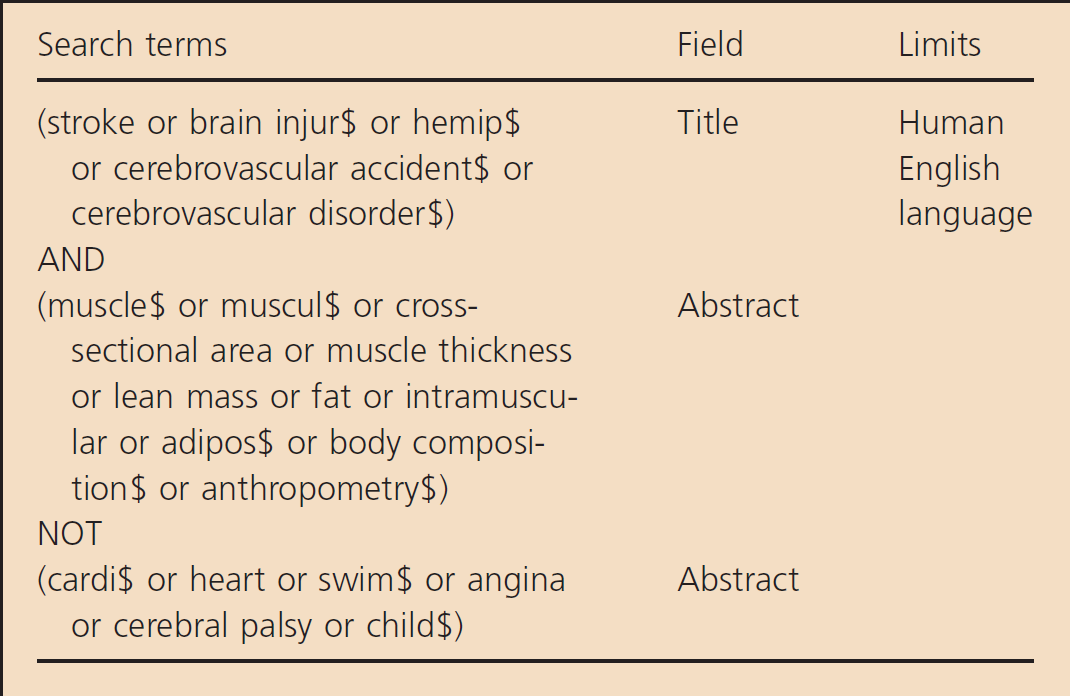
| Search terms | Field | Limits |
|---|---|---|
| (stroke or brain injur$ or hemip$ | Title | Human |
| or cerebrovascular accident$ or | English | |
| cerebrovascular disorder$) | language | |
| AND | ||
| (muscle$ or muscul$ or cross-sectional area or muscle thickness or lean mass or fat or intramuscular or adipos$ or body composition$ or anthropometry$) | Abstract | |
| NOT | ||
| (cardi$ or heart or swim$ or angina or cerebral palsy or child$) | Abstract |