
Abstract
Rotator cuff tears in adolescents are extremely rare, with no reported cases of arthroscopic repair being available in the literature thus far. A 14-year-old boy sustained a traumatic tear of his supraspinatus and infraspinatus muscles of the rotator cuff during a fall off his motorcycle during a motocross race. He also sustained a contralateral mid-shaft clavicle fracture. The rotator cuff was repaired arthroscopically with two rows of double loaded suture anchors. The clavicle was fixed with an elastic intramedullary nail. This was followed by intensive physiotherapy, and the patient returned to full pre-injury function in his shoulder by 6 months postoperatively.
Introduction
Rotator cuff tears in adolescents are uncommon and may be overlooked on initial examination. In the acute setting, pain may limit the accuracy of clinical examination in determining pathology. Ultrasound scans and magnetic resonance imaging (MRI) are both reliable tests to diagnose full thickness tears of the rotator cuff. Posterior cuff tears can also be very difficult to adequately visualize at open surgery because the tear may retract under the scapula spine and acromion. These tears can be managed arthroscopically, reducing the peri-operative complications related to open surgery. Although this is well described in adults, it has not previously been reported in an adolescent.
Case Report
An active 14-year-old boy presented after having been thrown over the handlebars of his motorcycle. He complained of pain in both shoulders. On examination there was tenderness and deformity over the left clavicle. There was also tenderness and swelling of the right shoulder, with a reduced range of active and passive movement of his right shoulder. Active movements were much less than passive. There were no neurovascular deficits. Radiographs of the left clavicle confirmed a significantly displaced and shortened midshaft clavicle fracture, whereas radiographs on the right shoulder revealed a halo of calcification superior to the humeral head in the subacromial space, possibly related to the supraspinatus tendon. He was managed in slings for comfort and referred to the orthopaedic fracture clinic.
The patient was reviewed in the fracture clinic 2 days after the injury. Clinically he had significant weakness of infraspinatus, teres minor and supraspinatus, with positive lag signs for all three. A full passive range of motion was present. MRI confirmed an avulsion of the rotator cuff from the greater tuberosity, extending from the level of the mid-supraspinatus, through the infraspinatus with involvement of the teres minor (Fig. 1). The anterior supraspinatus and the subscapularis were intact, as was the long head of biceps tendon. There was fluid in the right shoulder joint, and some marrow oedema around the region of the greater tuberosity.
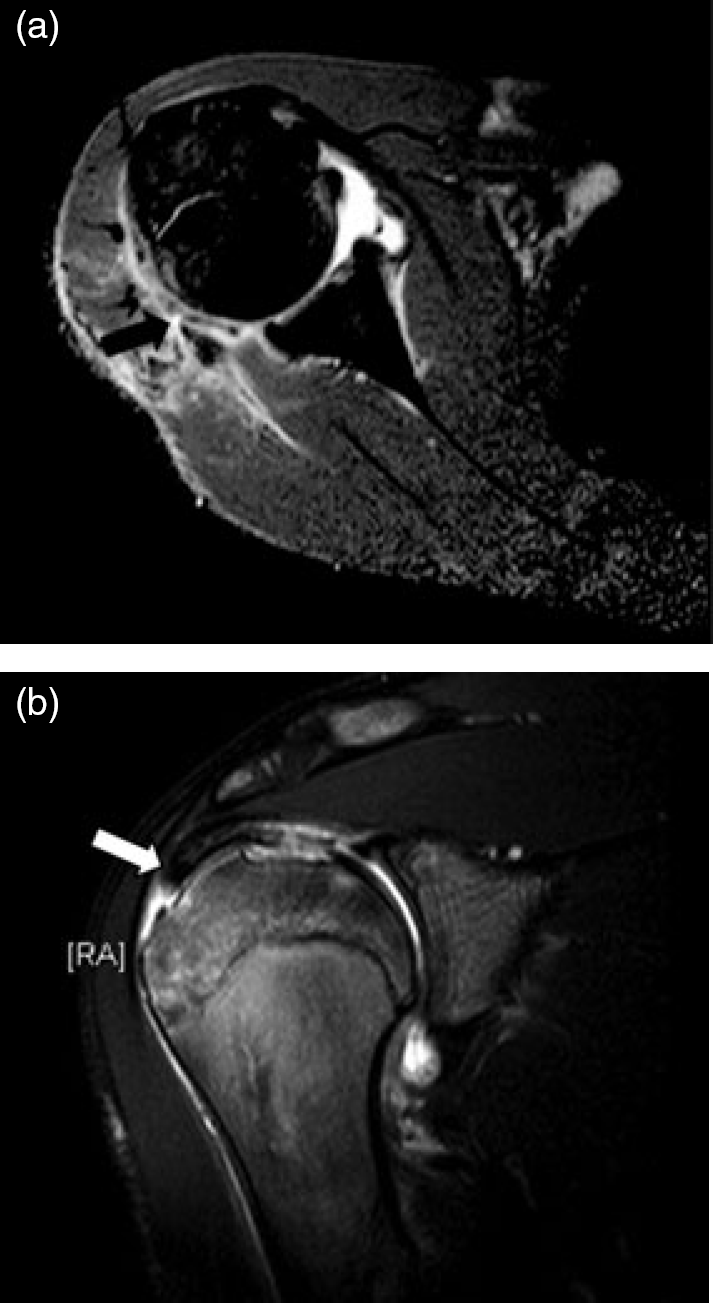
(a) Retracted torn infraspinatus and teres minor on MRI scan (black arrow). (b) Retracted torn supraspinatus tendon on MRI scan (white arrow).
Surgery was performed 11 days post injury. On the left side he underwent elastic intramedullary nailing of the clavicle. On the right side he had a diagnostic shoulder arthroscopy leading to an arthroscopic rotator cuff repair. The patient was positioned in the beach chair. The scope was inserted into the glenohumeral joint and the subacromial bursa. The standard posterolateral, anterolateral and lateral portals, and portal of Wilmington were used. There was a full thickness tear of the rotator cuff involving the supraspinatus and infraspinatus. The tendon was of good quality and thick. Its appearance was that of an acute traumatic lesion. It was large (3–5 cm by 3 cm wide) in an inverted ‘L’ shape and extended as far as the glenoid (Fig. 2a).
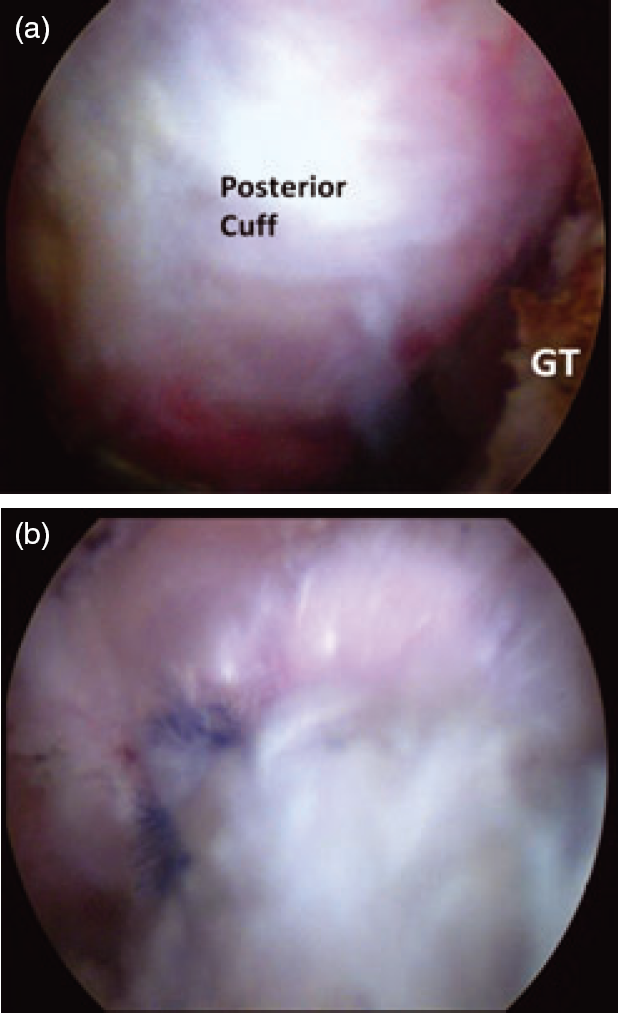
(a) Part of the torn infraspinatus tendon (rotator cuff) as viewed from the lateral portal. GT, greater tuberosity. (b) Repaired infraspinatus portion of tear.
Mobilization of the tendon was fairly extensive to allow nontensioned relocation to its insertion (Fig. 2b). The tendons were secured laterally using an end-to-bone repair with several anchors in a double row using a suture-bridge technique. The shoulder was held in neutral abduction and under minimal tension and a water-tight repair was achieved. In both the medial and lateral rows the anchors were 5 mm titanium anchors double-loaded with high-strength suture. A simple partial bursectomy only was performed without acromioplasty.
Rehabilitation postoperatively involved both passive and active assisted motion, as tolerated for 3 weeks, progressing to active motion and resistance, as per our standard protocol [1] (Fig. 3a). At 3 weeks he had almost full range of movement at the right shoulder, which was pain free, and evidence of some early muscle power. At 3 months, he was doing press-ups, light weights and had an excellent range of movement (Fig. 3b). He returned to motocross racing at 7 months.
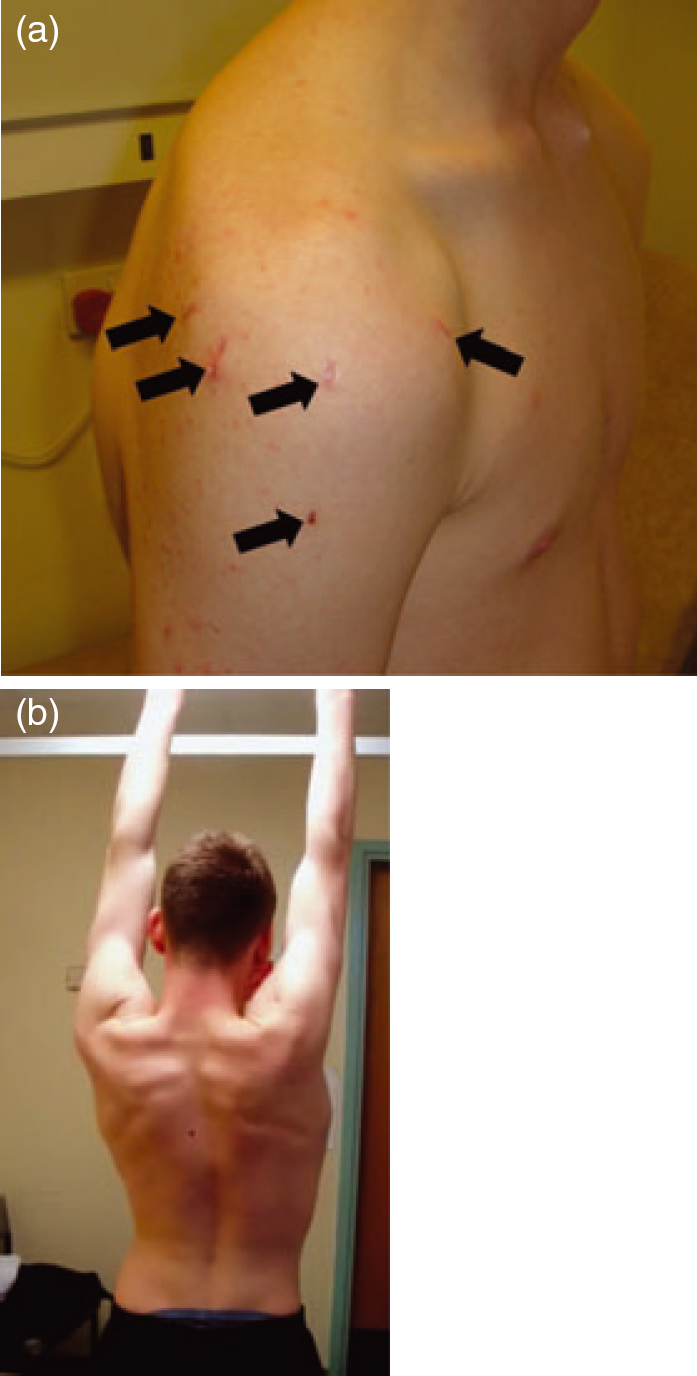
(a) Postoperative scars at 3 weeks (arrows). (b) Full active abduction at the 3-month review.
Discussion
Rotator cuff tears are rare in the young population because of higher strength, elasticity and resilience in youth [2], [3]. It has been shown that degenerative changes of the rotator cuff begin at age 40 years, and tears become more common as a result of less stress being needed to produce one [4].
In the young it is more common for the weaker cartilaginous parts or bony physis to give and produce an avulsion fracture, rather than have a tear of the cuff because the muscles are stronger than the physis [2], [3].
High-energy trauma is required to produce rotator cuff tears in young patients [2]–[4]. Tabata reported a 0.8–1% incidence of rotator cuff tears in young patients in a large study. Tabata and Itoi reported that, in three such cases, histological changes were present [5]. Tears secondary to competitive sports, particularly those involving throwing, are increasingly being recognized in adolescents, although still remain uncommon.
Patients present with reduced shoulder movement and painful passive movements [2], [3]. Pain can be a confounding factor acutely and hinder clinical diagnosis. Imaging, therefore, becomes important [2].
Radiographs can show narrowing of the acromiohumeral space [4]. Computed tomography (CT) is not as sensitive as MRI [3]. In our case, CT only implied the possibility of a cuff tear. The tear was confirmed by MRI. MRI can detect 84–100% of rotator cuff tears [4]. Ultrasound scans also have high detection rates [3], [4].
Due to the rarity of the injury and difficulty to interpret the examination in the acute clinical setting acute rotator cuff tears are overlooked in young patients, particularly in Accident and Emergency. A patient is often told they have only a soft tissue injury and discharged on the basis of apparently normal radiographs, leading to a delay in diagnosis and definitive management. It is important to have a high degree of suspicion for rotator cuff tears in adolescents following trauma with restricted active shoulder movements and radiographs which appear normal.
Full thickness rotator cuff tears are best managed by surgical intervention, particularly in the younger patient to restore full function [4]. Surgery should be performed early (before 3 months post injury) for best results, reducing complications of scar tissue formation and atrophy [4].
There are many reports of the use of open surgery or McLaughlin's technique for adolescents [3]. One report previously described an arthroscopic repair of the cuff in an adult but does not provide details of follow-up.
In our case, diagnostic arthroscopic surgery with an arthroscopic rotator cuff repair was performed. We recommend this approach, particularly for a posterior cuff tear as in this case. It is easier to visualize and access the retracted infraspinatus and teres minor muscles arthroscopically as they escape under the scapula spine. However, this does require a significant level of comfort and experience on the part of the surgeon in arthroscopic surgery to appreciate, access and repair a posterior cuff tear.
High clinical suspicion of a rotator cuff injury is required in adolescents following shoulder trauma with normal radiographs and loss of active range of motion. We recommend arthroscopic surgical repair of all full thickness posterior rotator cuff tears in adolescents, followed by intensive physiotherapy to regain full function of the shoulder and return to activity.