
Abstract
Background
There are no current North American population-based incidence studies of elbow dislocations. This creates further challenges in assessing associated outcomes and complication rates. The present study aimed to determine the population-based incidence of elbow dislocations in a large Canadian city.
Methods
From April 2002 to March, 2005, consecutive cases of elbow dislocation were documented. Age-specific, gender-specific and age-adjusted rates for simple and complex dislocations were calculated according to patient demographic and 2001 Canadian census data. All rates were reported per 10,000 persons per year.
Results
One hundred thirty-seven dislocations (53 simple and 84 complex) were identified. Simple dislocations occurred at a rate of 0.262 (95% confidence interval [CI] = 0.191 to 0.332). Fracture-dislocations occurred at a rate of 0.415 (95% CI = 0.326 to 0.504). The overall age-adjusted incidence was 0.671 (95% CI = 0.638 to 0.704). With the exception of the 18 years to 29 years (rate = 0.916, 95% CI = 0.648 to 1.183) and ≥80 years groups (rate = 0.906, 95% CI = 0.112 to 1.700), all age groups had an approximate rate of 0.600.
Discussion
The results obtained in the present study are similar to those obtained in a previous European study. True population-based estimates of elbow dislocation incidence are provided, which may facilitate the assessment of outcomes and complication rates of such injuries.
Introduction
The elbow is a commonly dislocated joint, with studies suggesting it is second only to the shoulder as the most common major joint dislocation among skeletally mature individuals [1], [2]. Such events should be considered an emergency, with treatment directed toward the restoration of proper joint alignment. In adult populations, associated injuries are quite common. These may include fractures of the radial head and neck, coronoid process and olecranon, as well as avulsion fractures of the medial or lateral humeral epicondyle. Although rare, debilitating neurovascular injuries, including injuries to the brachial artery and median nerve, may also occur.
When elbow dislocations are managed using appropriate nonsurgical and/or surgical techniques, complications and poor outcomes are uncommon. However, sequelae such as recurrent instability and post-traumatic contractures may result, particularly among patients who have experienced an associated injury. Upon assessment of an elbow dislocation, clinicians should carefully examine the wrist and shoulder to rule out concomitant injuries, which have been estimated to occur in 10% to 15% of cases [3].
Previous research has shown that elbow dislocations mostly occur in the posterior direction, with one of three mechanisms responsible for the injury: (i) valgus and supination of the forearm, in combination with an applied axial load [4]–[6]; (ii) varus/posteromedial rotation, in combination with an applied axial load [7]–[8]; and (iii) hyperextension of the elbow. More debate is associated with the issue of soft tissue disruption associated with elbow dislocations. Several structures have been identified as at risk for injury, including the medial collateral ligament [6]–[12], lateral collateral ligament [4], [7], [8], [10]–[12], annular ligament [4] and anterior capsule [8]. There is, however, a lack of consensus as to the structure(s) at primary risk for injury. Currently, there are no population-based studies describing the incidence of elbow dislocations in North America. This creates further challenges in the assessment of outcomes and complication rates associated with such injuries. Therefore, the present study aimed to determine the population-based incidence of elbow dislocations among tertiary health care centres in a large Canadian city.
Materials and Methods
Before commencing the study, ethics approval was obtained from our institutional Research Ethics Boards.
The present study included cases of elbow dislocations during a 3-year period (1 April 2002 to 31 March 2005) within a large Canadian metropolitan health region. Inpatient discharges and ambulatory care visits among individuals aged ≥18 years were included, as identified with the aid of the regional administrative database used in the region. This database encompasses health records of patients treated in the three adult acute care hospitals, the two urgent care facilities and the three rehabilitation hospitals within the region. These sites provide the majority of orthopaedic care and almost all of the complex orthopaedic care within the region.
During the 3-year period of the study, the health region utilized the International Statistical Classification of Diseases and Related Health Problems, version 10 (ICD-10) coding system. The ICD-10 was used to record the diagnoses of patients at the aforementioned sites. Patients discharged from the hospital wards, emergency, day surgery, minor surgery, physiotherapy and occupational therapy departments, as well as cast clinics, were captured in the health records database. Each case was given at least one discharge diagnosis by the treating physician most responsible for the patient's care. The discharge diagnosis was then converted to the appropriate ICD-10 code by the health records department, for inclusion in the health records database.
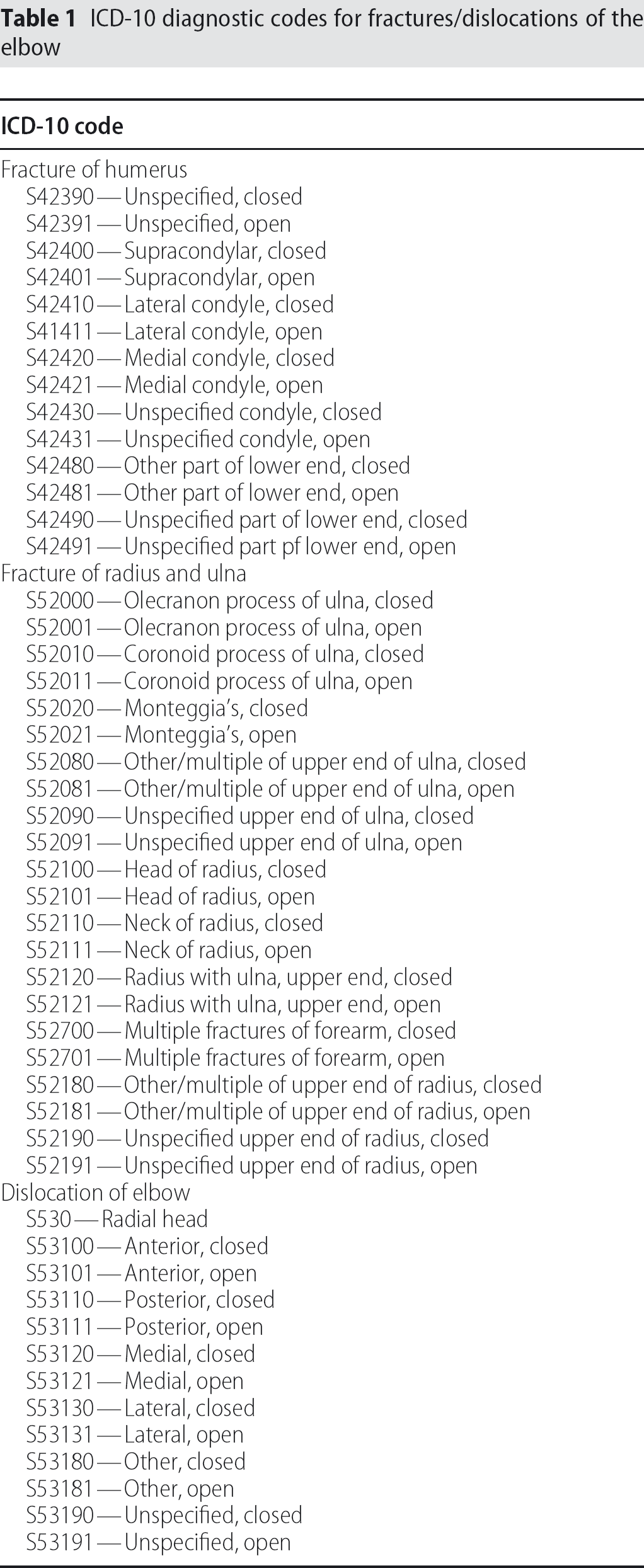
Before conducting the data base search, ICD-10 codes for fractures and dislocations of the elbow were identified (Table 1). This list of ICD-10 codes includes fractures of the distal humerus, proximal radius and proximal ulna, as well as dislocations of the ulnohumeral joint and radial head. Cases captured from the database included those that contained at least one eligible ICD-10 code. To ensure that duplicate cases were not included, cases from each site were cross-referenced with all other sites, utilizing personal health numbers, dates of service and type of injury.
ICD-10 diagnostic codes for fractures/dislocations of the elbow
Demographic data for each case, including the patient's date of birth, date of injury and gender, were collected. This information was used to calculate age- and gender-specific incidence rates and for the standardization of incidence rates to the Canadian population from the 2001 national census. Additionally, the patient's address was determined from the database to ensure the patient's residence within the city studied. If a patient's residential postal code was outside of the city, that patient was excluded from the study.
Radiographs for each identified case were collected for review. Pre-treatment radiographs were compiled for all cases where these were available. For cases where pre-treatment radiographs were not available, post-treatment radiographs were compiled along with relevant patient chart documents describing the pre-treatment injury. For the purpose of injury classification, two authors, who are also practicing orthopaedic surgeons, reviewed the radiographs and relevant patient chart documents.
The choice of classification system was based on the frequency of its use within the orthopaedic literature. The classification of simple dislocations (without fracture) has evolved from the original classification of Desault first described in 1811 [13]. It is based on the direction of the dislocation with the position of the radius and ulna described relative to the position of the humerus. Thus, the direction of the dislocation dictates how the injury is classified. Types included in the classification are posterior, anterior, lateral, medial and divergent [13]. Stimson further subdivided the original classification of Desault to include almost every possible anatomical position [14]. No reliability studies have been performed for the Desault classification system for elbow dislocations. For the purposes of the present study, the original classification of Desault was utilized.
Statistical analysis was performed using STATA, version 8.0 (STATA Corporation, College Park, TX, USA) and SPSS, version 13.0 (SPSS Incorporated, Chicago, IL, USA). Overall, age-specific, and gender-specific incidence rates were calculated utilizing the population of the city in question from the 2001 Canadian national census. Confidence intervals (CIs) were calculated for all incidence rates using a Poisson distribution. Standardization of the results was performed using the direct form of standardization. The age-standardized rates are weighted averages of the age-specific rates, with the weights equal to the proportion of the Canadian population in each age category from the 2001 national census. Both the crude rates and the standardized rates are included in the results of the study. During the 2001 national census, the adult (≥18 years) populations of Canada and the studied city were 23,040,965 and 674,695 persons, respectively.
Results
The study identified a total of 137 dislocations during the 3-year study period. Results relative to the types of injuries witnessed are presented according to sex in Fig. 1. Of the identified injuries, 53 were simple dislocations, and the remaining 84 occurred in combination with one or more fractures about the elbow. Utilizing the Desault classification system, posterior dislocations were the most common, representing just greater than 89% (n = 122) of the total number. Lateral dislocations and unspecified dislocations (for which a direction could not be determined from radiographs and charts), represented 4% (n = 6) and 5% (n = 7) respectively. A single anterior and a single medial dislocation were identified, with no divergent dislocations occurring in the health region during the period under study. Overall, age-based, and sex-based simple dislocation incidence rates are shown in Fig. 2.
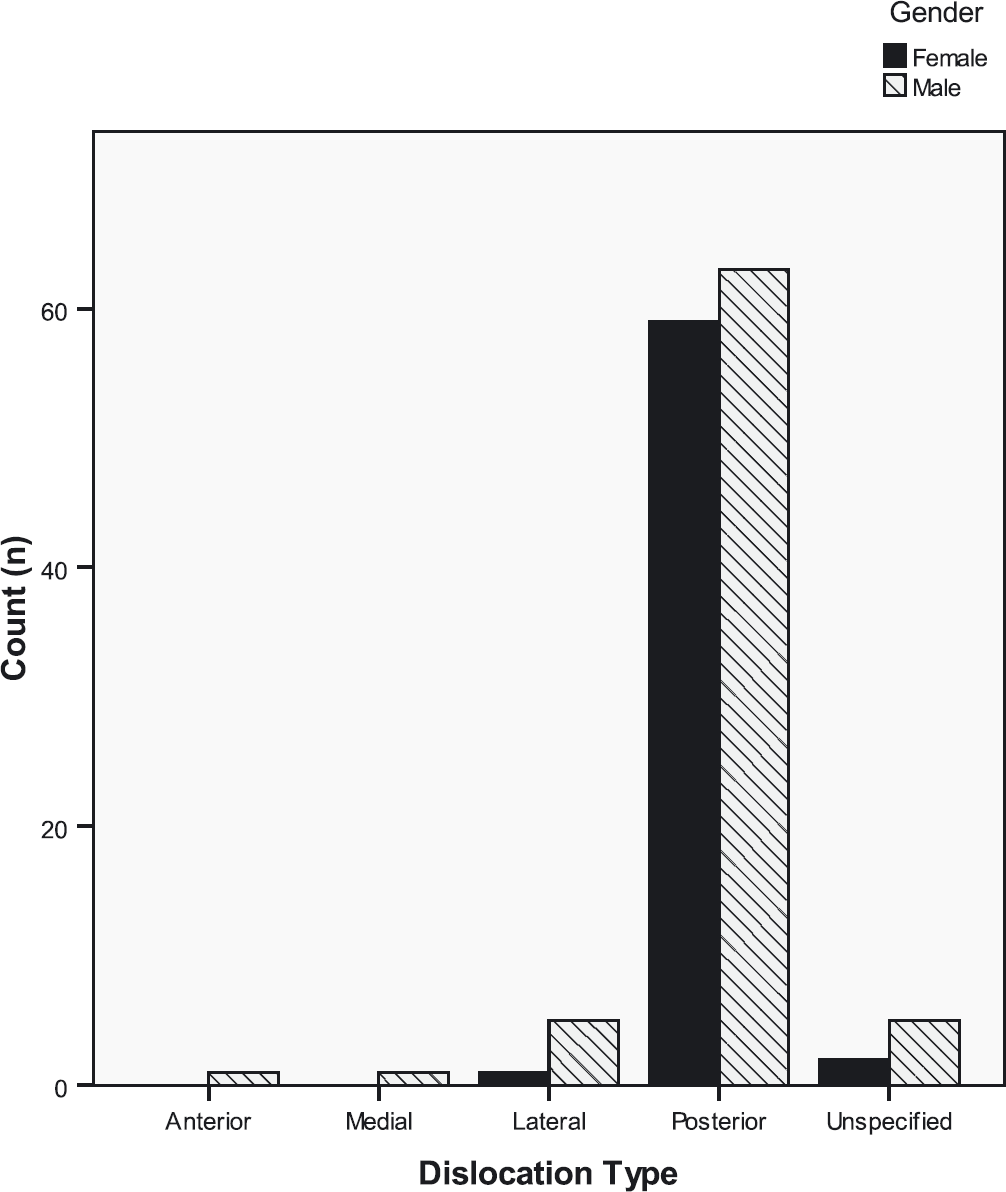
Types of dislocations (combined) by sex.
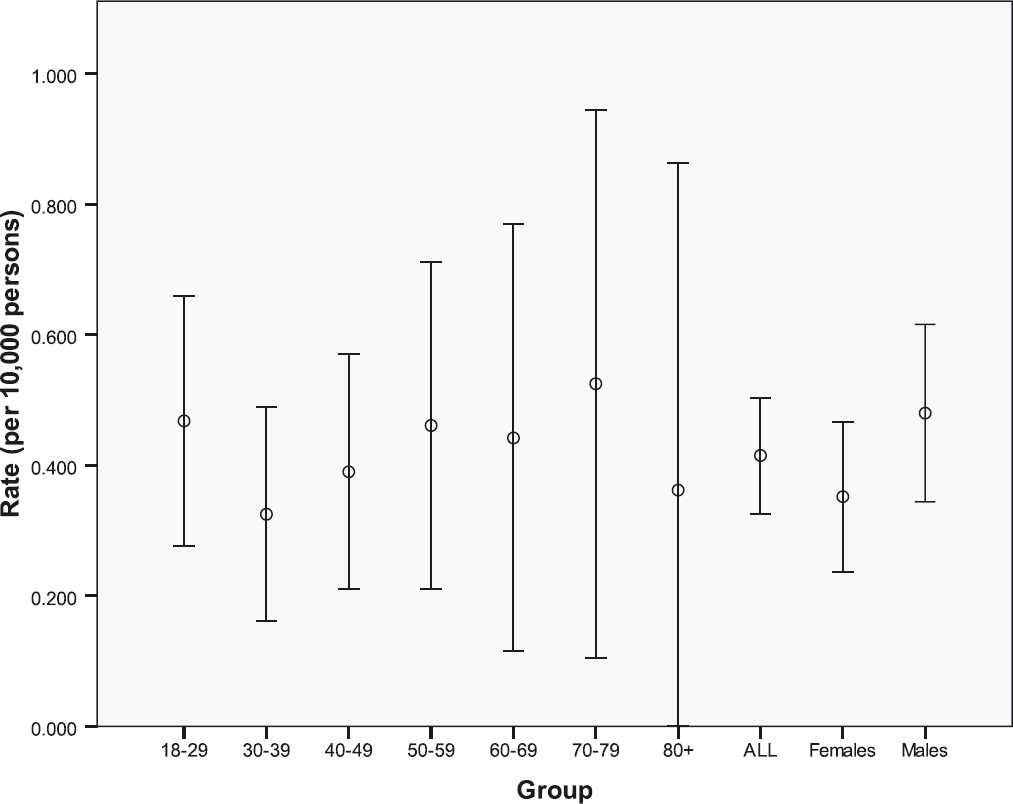
Annual rates of simple elbow dislocation.
Fracture-dislocations, which occurred just less than twice as often as simple dislocations, were most commonly associated with fractures of the radial head. Of the 105 fractures identified in the 84 fracture-dislocations, 48% (n = 50) were fractures of the radial head, whereas 37% (n = 39) were fractures of the coronoid. Other identified fractures included those of the olecranon (n = 4), lateral epicondyle (n = 4), lateral condyle (n = 3), capitellum (n = 3) and medial epicondyle (n = 2). Radial head fractures and coronoid fractures were also most likely to have occurred in combination, comprising 84% of the fracture-dislocations with two fractures and all of the fracture-dislocations with three fractures (together with a third type). Fracture-dislocation incidence rates are shown in Fig. 3.
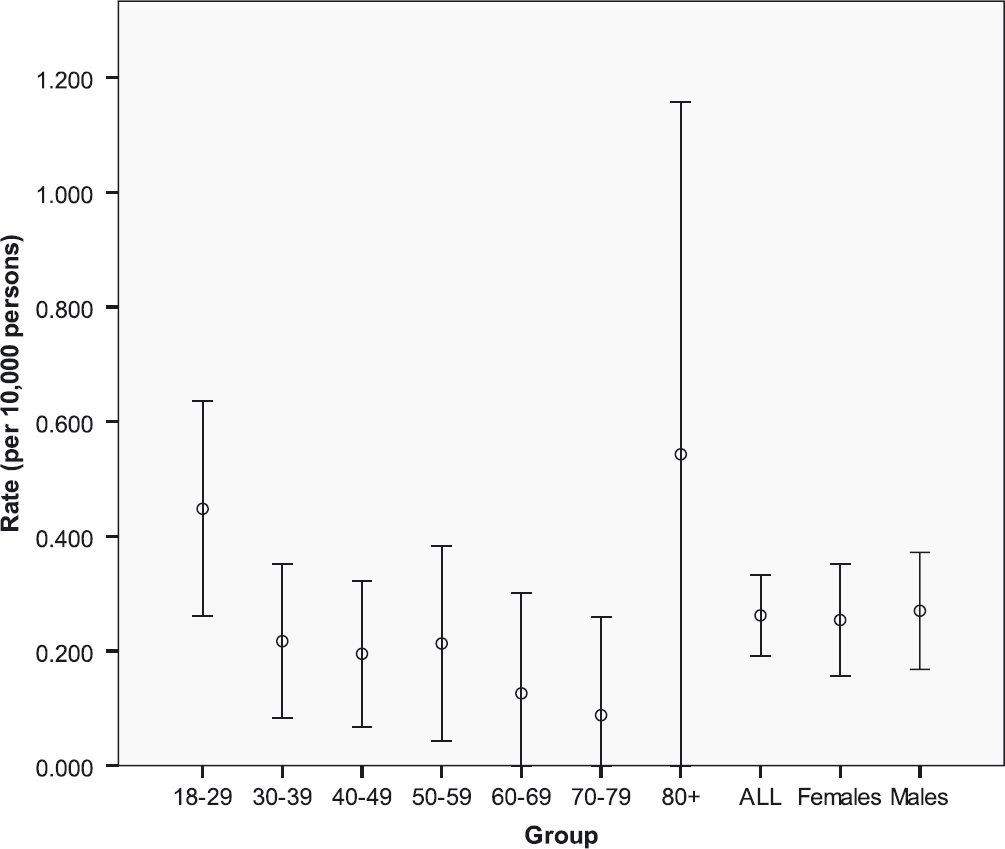
Annual rates of elbow fracture-dislocation.
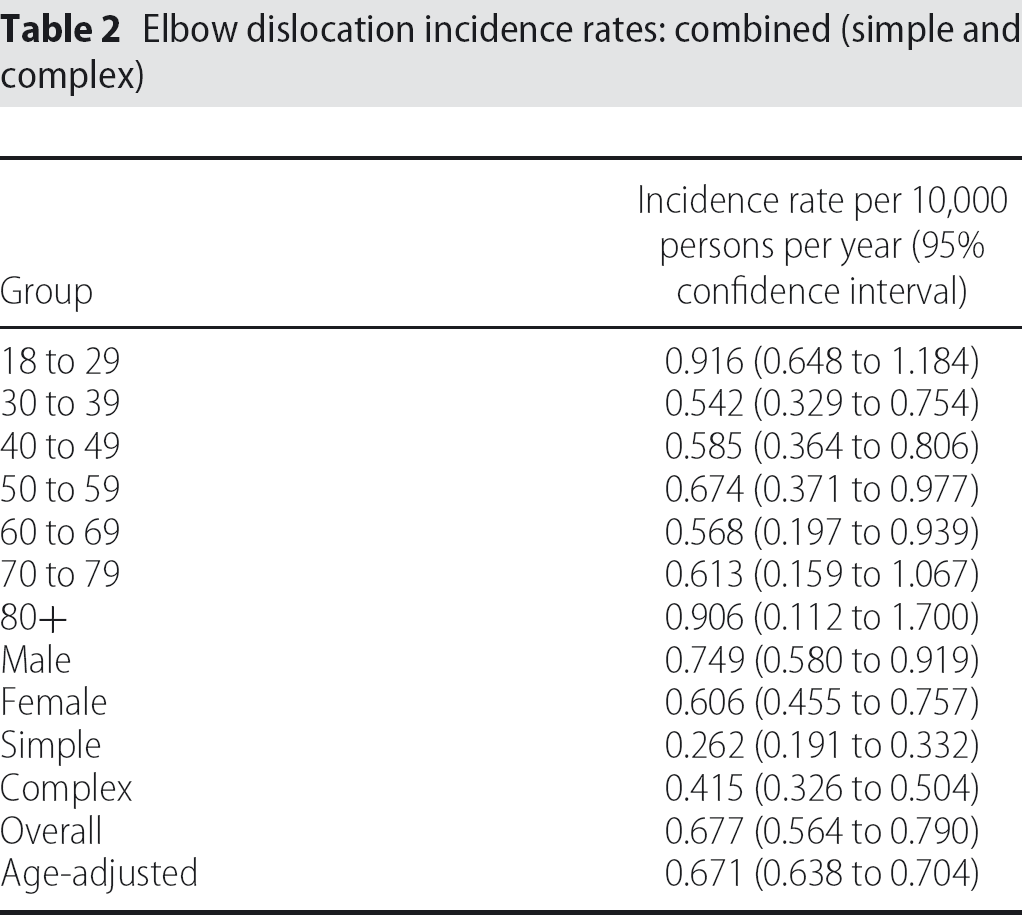
Data relative to the incidence of elbow dislocations are shown in Table 2. Overall results are presented along with the age- and sex-based statistics. The overall incidence of elbow dislocations, including both simple dislocations and fracture-dislocations, identified during the period under study was 0.677 per 10,000 persons per year (95% CI = 0.564 to 0.790). Simple dislocations occurred at a rate of 0.262 per 10,000 persons per year (95% CI = 0.191 to 0.332), whereas fracture-dislocations occurred at a rate of 0.415 per 10,000 persons per year (95% CI = 0.326 to 0.504). The incidence was similar in males and females, with a rate of 0.749 per 10,000 persons per year in males (95% CI = 0.580 to 0.919) and 0.606 per 10,000 persons per year in females (95% CI = 0.455 to 0.757). The age-specific incidence occurred in a bimodal distribution, with a rate of approximately 0.6 per 10,000 persons per year in most age groups, with the exception of the 18 years to 29 years and ≥80 years age groups where the rates were 0.916 (95% CI = 0.648 to 1.183) and 0.906 (95% CI = 0.112 to 1.700) per 10,000 persons per year respectively. The overall age-adjusted incidence, according to the 2001 Canadian census, was 0.671 per 10,000 persons per year (95% CI = 0.638 to 0.704).
Elbow dislocation incidence rates: combined (simple and complex)
Discussion
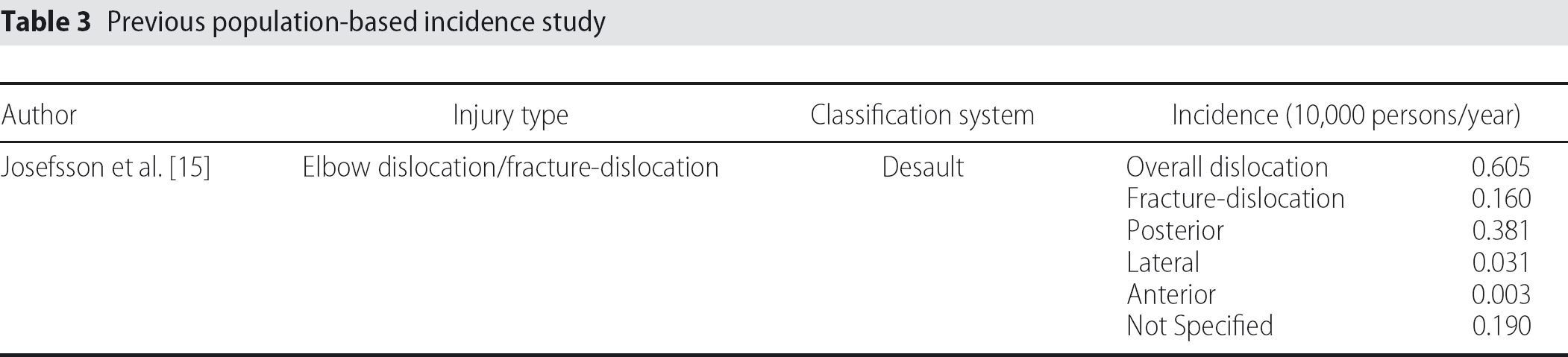
Previous work published in the English orthopaedic literature outlining the population-based incidence of elbow dislocations is limited to a single Swedish study published in 1986 (Table 3) [15]. The authors presented the results of a comprehensive case series of elbow dislocations identified in the city of Malmo between 1971 and 1982. Similar to the present study, injuries were classified according to the Desault classification system for elbow dislocations and included both simple dislocations and fracture-dislocations. The authors utilized the population of Malmo as the denominator in the calculation of the population-based incidence and identified an overall incidence rate of elbow dislocations, including both simple dislocations and fracture-dislocations, of 0.605 dislocations per 10,000 persons per year. The study identified a rate of 0.262 per 10,000 persons per year for simple dislocations and 0.415 per 10,000 persons per year for fracture-dislocations. The incidence of posterior dislocations was greatest at 0.381 per 10,000 persons per year, followed by unspecified dislocations at 0.190 per 10,000 persons per year, and lateral dislocations at 0.031 per 10,000 persons per year. Although these authors indicate that the data presented is complete, the study provided no means for assessing misclassification of cases. Furthermore, no CIs were reported, limiting the ability for the reader to assess the accuracy of the results. With respect to the direction of dislocation, 178 elbow dislocations demonstrated a posterior dislocation in 63% of cases (n = 112) in a previous study by Josefsson and Nilsson [15]. Although this is significantly lower than our reported percentage of posterior dislocations (89%), these results should be interpreted with caution because this previous study had a high percentage of cases (31%) where the direction of dislocation was not specified.
Previous population-based incidence study
Previous nonpopulation based studies [1], [16] have reported significant disparities in the incidence rates and percentages for various fractures and dislocations of the elbow. One potential reason for this may be that the two studies identified may reflect the practical experience of the individual surgeon associated with each study, rather than the population-based incidence in the associated region under study. Although these studies provide crude estimates of incidence and fracture percentages, their findings cannot be used to accurately determine the percentage of positive and negative outcomes, nor the number of complications, because they do not provide true population-based incidence. Furthermore, the results from these studies cannot be generalized beyond that particular institution or physician, and may not even be representative if a different period of time is chosen for study.
The counts of injuries and associated incidence rates of dislocations and fracture-dislocations of the ulnohumeral joint classified with the Desault classification system reflect the combined counts and associated incidence rates of the dislocations and fracture-dislocations described above. The bimodal distribution of the incidence rates, with a rate of approximately 0.9 per 10,000 persons per year in the groups age 18 years to 29 years and ≥80 years, and approximately 0.6 per 10,000 persons per year in all other age groups, reflects the higher rate of dislocations without fracture in younger individuals and the higher rate of fracture-dislocations in older individuals. The distribution of the type of dislocation is similar to the study by Josefsson and Nilsson [15], with the exception of a much greater number of unspecified dislocations in the Swedish study (27 versus 7). Posterior dislocations were by far the most common type, followed by lateral, in both studies. With the exception of unspecified dislocations, posterior dislocations occurred at a rate of 11.2 to 1 in the study by Josefsson and Nilsson [15], and 13.5 to 1 in the present study.
There are limitations to the present study that warrant discussion. These include (but are not limited to) potential data miscoding, misclassification of cases during initial treatment, errors in the population database that was used and the possibility of selection bias on the part of the authors.
First, we attempted to determine the presence of miscoding in the data set. Miscoding resulted from dislocations being categorized as ‘unspecified’ when the direction was clear from either the radiographs or information contained in the chart. In the majority of cases where cases were miscoded as ‘unspecified’, the direction of the dislocation was not clearly stated in the discharge diagnosis. Thus, these cases were placed in the ‘unspecified’ category, rather than a more appropriate direction specific category. This led to discordance between the code applied by the authors (the reference standard) and the code applied by the health records department. Furthermore, by also looking at fracture injuries, we were able to estimate the presence of misclassification. The data suggested that using the ICD-10 data alone would have created an over-estimation of the incidence of simple dislocations and an under-estimation of fracture-dislocations if the original ICD-10 code was the only means to determine cases. Although the study was successful at measuring the accuracy of the current coding system, it did not determine at what point the miscoding might have occurred. Miscoding may be the result of an incorrect discharge diagnosis with the correct associated code, a correct discharge diagnosis with an incorrect associated code, or both an incorrect discharge diagnosis and an incorrect associated code. Although the measured percent agreement provides an estimate of the degree of miscoding, the true source of the miscoding could not be determined. The present study was carried out as part of a larger project, where the percent agreement between the authors and health region's database coding system was determined to be 59.03%.
Second, as the classification of the radiographs and chart notes by the authors is the foundation upon which the estimates of the incidence rates are based, we attempted to identify sources of misclassification that may exist when identifying injuries from a database such as the region's health records database. However, misclassification may also occur during the authors' classification of the identified injuries. Although both authors can be considered experts in the field under study, the past clinical experience of the authors impacts upon the classification of the injuries based on the radiographs and chart notes. The relatively poor reliability of the classification systems would suggest that a percentage of the classified cases would be open for discussion, and that another set of observers may choose to classify the cases differently [17], [18]. Ultimately, this would lead to a degree of misclassification of the identified cases by the study authors, and would affect the estimated incidence rates. Because a reference standard for the authors was not used, this misclassification cannot be accurately measured.
Third, the denominator data used for the calculation of injury incidence rates was taken from the 2001 Canadian census, which provides estimates of the overall, age-specific (by decade) and sex-specific population of the city in the present study in 2001. During the period under study (from 2002 to 2005), there was a change in the population of the city, with an increase in the overall population and an increase in certain age ranges (most likely younger age ranges). Therefore, for the purposes of the present study, the use of the 2001 census data would result in an overestimation of the incidence rates because of the increase in the population of the city during the period under study. This would have resulted in an increase in the value of the denominator used in the incidence rate calculations, and thus a decrease in the calculated incidence rate. However, the presentation of the data with the associated 95% CIs provides the reader with a range of possible values for the estimates of the incidence rates and takes into account the uncertainty associated with the use of the 2001 census data as the denominator in the incidence rate calculations.
Finally, potential sources of selection bias in this study merit consideration. There were limitations in the health records database with respect to capturing all cases. For example, if a dislocation was managed by a primary care physician, a private practice orthopaedic surgeon or under the auspices of the Worker's Compensation Board, the health region's database may not capture that injury. This would have resulted in an underestimation of the actual incidence of some injuries. Because records outside of the region's health records database cannot be sampled for privacy and logistical reasons, it is impossible to measure the potential magnitude of this selection bias.
As illustrated above, the present study had several sources of potential error, including data miscoding and misclassification, the database used to obtain population-based incidence rates and selection bias on the part of the authors. Although the impact of these sources of error cannot be reliably estimated, previous European studies have obtained similar results. Given the similarities between the European and our present North American data, the validity of the data obtained in the present study is supported, which adds to the estimates of the true incidence of elbow dislocation in industrialized western populations. In summary, despite the limited existing population-based studies of the incidence of traumatic elbow injuries, the findings of the present study are in keeping with previously published results [1], [15], [16]. This finding suggests that the characteristics of the present study population are similar to those of previously studied populations, at least with regard to traumatic elbow injuries. This would also suggest that these findings could be generalized to other similar populations.
Conclusions
The present study comprises the first comprehensive North American population-based study to report the incidence of elbow dislocations utilizing expertise-based classification. The information presented in the study highlights the relative magnitude of the clinical burden of various elbow dislocations. This in turn raises many questions about the clinical outcomes of these injuries and brings greater attention to those injuries that are more common, such as posterior dislocations. The incidence rates presented provide a population-based denominator that may be used for future research on outcomes and complications, allowing for a better estimation of the percentages of positive and negative outcomes and of major and minor complications.
In addition to the clinical and research applications, the present study highlights the weaknesses of the existing system for classifying, recording and identifying injuries in a health records database. Although the present study is specific to elbow injuries, the degree of misclassification present may be extrapolated to other injury types within the health records database. This should alert researchers, administrators and policy-makers to the potential hazards of decision-making based on incidence and prevalence rates generated from an ICD-based health records system.
Footnotes
Conflicts of Interest
None declared
Acknowledgements
The authors would like to acknowledge Ms Sandy Doolaar, Quality Improvement and Health Information, for her assistance with data collection for this study.