
Abstract
The coracoid process of the scapula is a vital landmark in shoulder surgery and has become increasingly popular as a basis for acromioclavicular joint (ACJ) stabilizations and bone transfer in the treatment of shoulder instability (Bristow–Latarjet procedure). As such, it is important that the anatomy and anatomical aberrations are well understood. We describe an aberrant structure noted during routine ACJ stabilization of a 24-year-old man using a coracoclavicular sling technique.
Introduction
Normally, the pectoralis minor tendon takes its origins from the third to fifth rib and inserts into the medial and upper border of the coracoid. A review of the literature revealed a number of reports of aberrant structures passing over the coracoid process. These included forms of the pectoralis minor tendon, first described by Le Double in 1897 [1], which have been found to divide and pass over the coracoid process to insert into the glenohumeral joint capsule [2], [3]. Another recently documented case reported an unusual insertion of the aberrant muscle pectoralis minimus, first described by Testut in 1896 [4], lying beneath pectoralis major and medial to pectoralis minor. When present, this muscle usually runs between first costal cartilage and coracoid process [5], although it has been documented passing over the coracoid as a tendinous slip to insert into the glenohumeral joint capsule [6]. There are no reports in the literature of any aberrant brachial plexus cords or any vascular abnormality that pass over the coracoid process.
The majority of these cases have been discovered during cadaveric dissection and the origins and insertions of these aberrant structures could be pursued and identified. In the living subject, this is not always possible and so an accurate differential for such aberrant structures that may be encountered during routine procedures is important.
Case Report
Elective acromioclavicular joint (ACJ) stabilization was undertaken in a 24-year-old man for a Rockwood grade 4 acromioclavicular disruption. We used a braided polyester material that had been modified into a purpose built ligament, providing secure fixation as well as tissue in-growth. This procedure involves looping the ligament around the coracoid and then attaching it to the reduced lateral end clavicle with a screw. When preparing the coracoid, we came across a cord-like structure looping over the coracoid base, traversing in a medial to lateral direction (See Fig. 1). This was in addition to (and separate from) the classically described pectoralis minor tendon. The structure was enveloped in a small sheath over the coracoid process and appeared to create a smooth indentation over the coracoid. Its appearance was akin to a nerve. This was precisely at the site where the artificial ligament would loop around the coracoid after stabilization of the ACJ; hence, it was important that a compressible structure, such as an aberrant nerve, was ruled out. We used a nerve stimulator but no response was obtained to the stimulus provided via the electrode. We then dissected this cord-like structure laterally where it appeared to merge in to the rotator interval tissue. Careful medial dissection was undertaken, being mindful of the medial neurovascular structures. Further medially, we could see muscle fibres coming off from this cord that were directed inferomedially towards the chest wall. We then continued with the stabilization procedure as planned, having surmised that the cord-like structure was an aberrant tendon. The patient made uneventful recovery and there was no neurological deficit postoperatively. Three months post surgery, he had returned to work. He reported no issues of pain, especially anterior shoulder pain or coracoid-related pain, at his follow-up check.
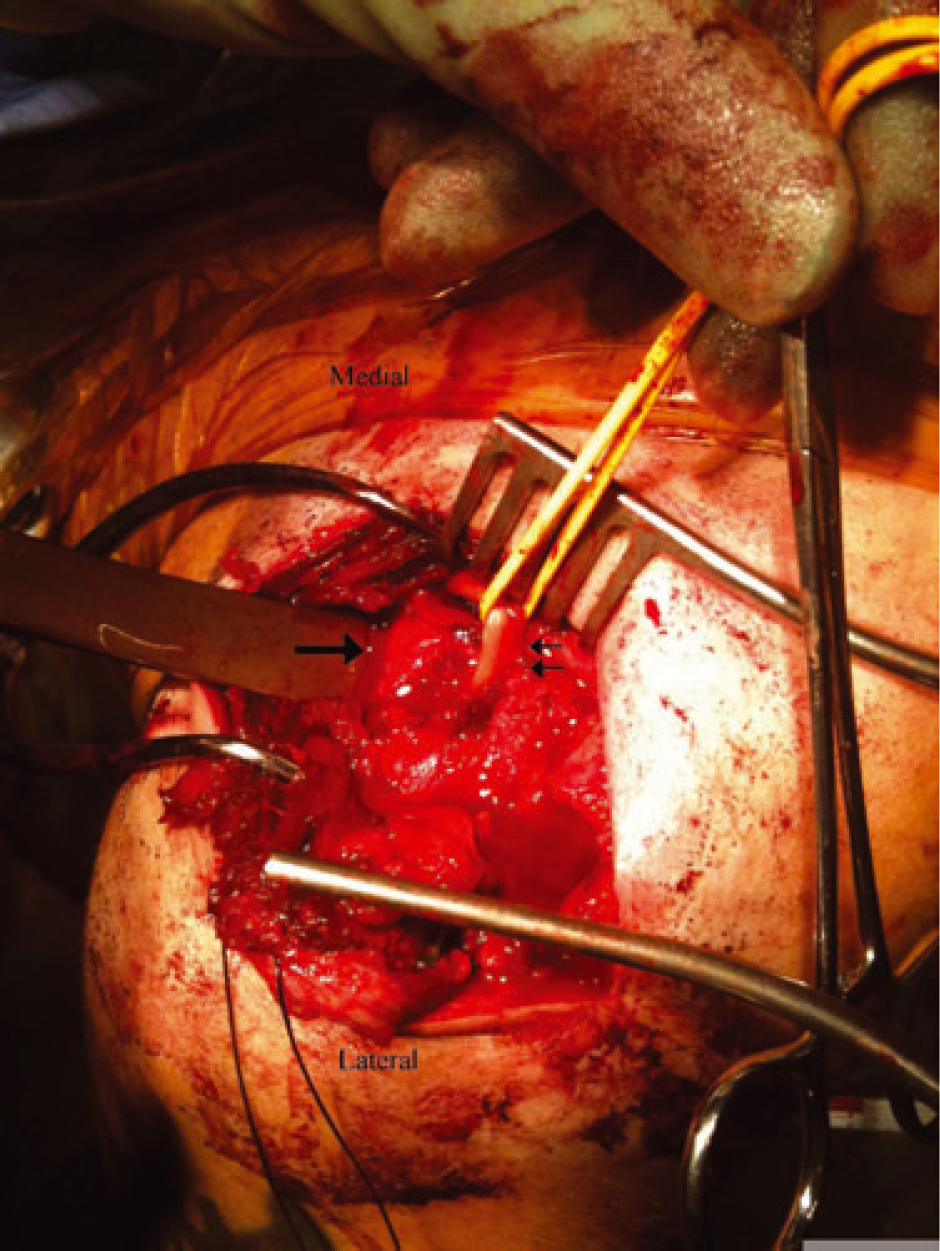
Intra-operative photograph of patient's left shoulder. Thick arrow, coracoid process with osteotome beneath. Thin arrows, aberrant tendon with elastic loop around it.
Discussion
The literature quotes an approximately 10% incidence of this abnormality based on ultrasound findings [3], [7]. The coracoid is not only an important land mark in shoulder surgery, but also is being utilized increasingly in procedures that involve ACJ stabilizations and coracoid transfer (Bristow–Latarjet) in shoulder instability surgery. Our patient did not report any shoulder problems before his ACJ injury. We faced the dilemma of using the coracoid as an anchor for our fixation in the presence of this cord-like structure that initially appeared to be a nerve. We were able to proceed to our planned stabilization only after we had conclusively ruled out the possibility of the aberrant structure being a nerve. A literature review was undertaken in response to our findings in this case and we concluded that the tendon was very likely to be an aberrant insertion of pectoralis minor, as described over the past decade [2], [3], [6]. The insertion of a tendinous structure into the glenohumeral joint capsule also has possible implications when investigating the origin of shoulder pain and stiffness because it may be a factor in cases of coracoid impingement [8] or contracture [9]. Indeed, a case report of a woman with a 2-year history of shoulder pain and stiffness was published by Moineua et al. who he described a pectoralis minor tendon inserting over the supraspinatus that was tensioned by external rotation of the shoulder [9]. Arthroscopic capsular release was performed with no effect and improvement in external rotation was only achieved when the aberrant tendon was detached from the supraspinatus. It is advised that this pathology be suspected in patients with shoulder stiffness who experience anterior thoracic pain with passive external rotation, as well as in all cases of shoulder stiffness that are poorly corrected by anterior capsulotomy and rotator interval release. If found, a tenotomy can be performed during arthroscopy with or without subsequent re-attachment to the coracoid.
Conclusions
Aberrant structures may be encountered in the vicinity of the coracoid during surgery. These are of obvious potential concern for surgeons who are operating around the region of the coracoid, which may ultimately prolong surgery or influence surgical technique. We feel obliged to share our experience with upper limb surgeons who should be aware of the possibility of encountering such a tendon during exposure of the coracoid. It can be easily retracted away and a ligament loop can be passed safely around the coracoid without any compromise. It may also prove to have clinical significance in patients experiencing shoulder pain and stiffness in whom the commoner pathologies have been ruled out.