
Abstract
This work addresses the practical anesthesiologist scheduling (AS) problem motivated by the needs of an academic anesthesiology department. The AS problem requires the department to plan and deploy providers to adequately meet clinical demand and institutional protocols of various clinical units over a planning horizon of up to several weeks. A data‐driven two‐step AS framework is developed by exploiting the historical demand data of anesthesia cases. The first step is a shift design which obtains the optimal shifts considering clinical demand under uncertainty using conditional value‐at‐risk constraints, and the second step is provider assignments that generate the schedule considering optimal and equitable workload distribution and provider availability using multiobjective mixed‐integer programming models. Moreover, the AS framework incorporates the provider specialties, and clinical and lifestyle preferences and aligns with the existing scheduling practices. An ɛ‐constraint solution method is applied for multiobjective optimization, and an iterative solution method is developed to improve solution quality for workload equity in clinical applications. Computational experiments are performed to evaluate the performance of three alternative forms of the workload equity objective function, and the results show that the minimization of the sum of the absolute deviations of provider workloads best balances solution runtime and quality. In the concerned academic anesthesiology department, two clinical problems, the budget and hiring planning and the monthly scheduling, are addressed via the application of the proposed AS framework. For budget and hiring, decision‐makers can make trade‐offs based on their preference using the nondominated frontiers obtained via the ɛ‐constraint method. For monthly scheduling, the iterative solution method can accommodate preassigned shifts capturing institutional requirements while improving workload equity. The workload variance has been substantially reduced from 2.92 to 1.39 after the implementation based on the historical schedule data. The provider schedule satisfaction is improved from 3.13/5 to 3.44/5, and at least 82% of scheduling burden on department leaders is relieved. The developed AS framework is generic and can be extended to the scheduling of other types of care providers, including nurses and residents.
Keywords
INTRODUCTION
Facing the ever‐increasing healthcare demand and financial pressure due to rising costs and changes in reimbursement policies (Lan et al., 2022), hospitals and healthcare systems have been experiencing shortages of anesthesiologists and certified registered nurse anesthetists (CRNAs) in most industrialized countries (AAMC Report Reinforces Mounting Physician Shortage, 2021; Ringo, 2021). The scarcity of available care providers and increasing costs force healthcare managers to focus on finding efficient planning and scheduling tools.
This work addresses the practical anesthesiologist scheduling (AS) problem for an academic anesthesiology department. AS assigns shifts to anesthesiologists, referred to as providers, so that they can meet clinical demand and institutional requirements at different clinical units. The academic anesthesiology department considered in this study is the largest anesthesiologist group in the region. It employs 50+ anesthesiologists as faculty members, 50+ residents, and 40+ CRNAs to cover 10+ unique clinical units, including operating rooms (ORs), intensive care units (ICUs), and a Level I1 Trauma Center.
Both coverage‐driven and demand‐driven shifts are used in the AS practice. Coverage‐driven shifts have fixed durations and are designed to cover clinical and other demands with relatively stable levels, and demand‐driven shifts have flexible durations and are designed to cover clinical demands with uncertainty and fluctuating levels. Although the anesthesiologists in the department have coverage‐driven fixed‐shift roles in pain clinics, acute pain service, ICUs, hospital management, teaching, research, and other essential services, ORs constitute the majority of anesthesia cases (Mets, 2018). Furthermore, on top of the regular shifts, anesthesiologists must provide on‐call, either “in house” or “at home,” services to handle emergencies in off‐hours at night, during weekends, and on holidays. The clinical demand varies widely within a day and from one day to another (Dexter et al., 2015). Unlike common shift‐based personnel, for example, nurse and resident, scheduling (Kim & Mehrotra, 2015; Topaloglu, 2009), anesthesiologists are dedicated to anesthesia services in the ORs driven by surgical cases, resulting in “flex‐end” demand‐driven shifts that do not end until demand is fulfilled. As the clinical demand for anesthesia is complex and changes frequently, a data‐driven approach is used to estimate the workload, and then multiobjective optimization is used to schedule the providers, for the practical AS problem in this study.
Anesthesiologists represent one of the most valuable and expensive resources in hospitals (Rath et al., 2017), and their preferences and specialties need to be incorporated into the AS procedure to promote job satisfaction (Aiken et al., 2002). Having undergone extensive training, anesthesiologists are qualified and specialized employees who are usually difficult to replace (Rath & Rajaram, 2022). For these reasons, anesthesiologists are often given the opportunity to embed their preferences concerning shift choices and sequencing with high autonomy into the AS process. However, this practice often exacerbates inequity in workload distributions across providers as well as across specialties and across seniority and leadership positions. It often leads to consecutive lengthy demanding shifts without a balanced workload and/or off days. Furthermore, AS is restricted by collective agreement requirements and individual customized provider contracts. These factors also lead to suboptimal workload distribution across anesthesiologists. A suboptimal schedule very likely leads to workforce turnover, as providers monitor their workload and benefits closely, compared to their peers inside and outside the organization. It is essential to effectively optimize the anesthesiologist schedules to assign equitable workloads to providers while meeting demand.
In clinical practice, AS is a time‐consuming task. It is mostly a manual or semimanual process conducted by highly qualified physicians and department leaders combined with provider self‐scheduling. The manual process usually leads to schedules with limited consideration of equity, feelings of bias, job dissatisfaction among providers, and overlooked regulations. Although automated anesthesia scheduling software, such as QGenda,2 exists, it is difficult to fully incorporate all provider specialties and preferences, account for uncertainties, embed regulations, and consider multiple objectives with restrictions in such commercial platforms. Furthermore, automating the AS process in clinical practice faces common challenges in healthcare organizations. For example, resistance to change in scheduling workflows (Nilsen et al., 2020), and the collaboration among multiple clinical units and other clinical resources, for example, surgeons, nurses, and residents, can limit the implementation of automated scheduling. Stakeholder engagement and buy‐in should be prioritized from the start by designing the automated AS process to align with current practice, which has been shown to be effective in previous studies (Scheinker & Brandeau, 2020).
To address these challenges, this study develops, implements, and deploys an AS framework focusing on the clinical AS practices for this large anesthesiology department and makes the following contributions to the literature. First, a two‐step AS framework with models and solution methods is developed that is aligned with the clinical AS practice. The proposed AS framework provides guidelines for implementation and has proven to be an essential element for strategic, that is, budget and hiring planning, and tactical, that is, monthly AS, decisions. Second, demand uncertainty is integrated into the AS framework by leveraging data‐driven optimization based on historical clinical demand data. Third, three forms of the workload equity objective function are proposed and studied to find the most suitable formulation for the AS problem. Fourth, two solution methods are proposed, that is, an ɛ‐constraint method to generate approximate nondominated frontiers for the decision‐makers to make trade‐offs among multiple objectives and an iterative solution method to improve each provider's schedule while accommodating their specialties and preferences and aligning with the current practice of the department.
The remainder of the paper is organized as follows. Section 2 reviews the literature and characterizes the problem in the context of personnel scheduling (PS) in the healthcare domain. In Section 3, the problem is described by contrasting the status quo AS process with the proposed AS process, the data‐driven two‐step AS framework is presented, and the models are constructed for the two steps. In Section 4, the solution methods for the multiobjective mixed‐integer programming model in Step 2 are described. In Section 5, the results of data‐driven shift design and analysis of alternative forms of the workload equity objective function are provided, and then two clinical applications, that is, the budget and hiring planning and the monthly AS, are presented. Section 6 discusses the managerial implications. Conclusions, limitations, and extensions of this work are in Section 7. Supplemental information is also provided.
LITERATURE REVIEW
AS is essentially a special case of PS. In general, PS is concerned with allocating employees to specific shifts to satisfy work demands based on employee qualifications and preferences and on‐the‐job requirements (Al‐Yakoob & Sherali, 2007). There is a vast literature on PS, for example, the review by Bergh et al. (2013), but the review in this section is limited to the most relevant works in the healthcare domain.
According to the literature (Stolletz & Brunner, 2012), the AS problem can be characterized as a combination of the following four modules: (a) demand forecasting, (b) days‐off scheduling, that is, interspersing off days between duty days, (c) shift scheduling, that is, determining shifts to cover the demand over a certain planning horizon according to general and individual work requirements and preferences, and (d) staff assignment, that is, assigning employees to shifts. Planners typically consider these modules sequentially. AS, or more generally physician scheduling, exhibits many characteristics that differentiate it from other topics within the realm of PS. Erhard et al. (2018) summarized that the special considerations of preferences, equity, flexible shifts, break assignments, and stochastic demand are the specific characteristics of physician scheduling derived from the literature. While all these characteristics make physician scheduling stand out from the general PS, there are indeed small subsets of service industries that have some of these characteristics in common within the healthcare domain. However, the presence of all these characteristics is unique, which creates complexity for physician scheduling problems that are outstanding in the field of PS. The following discussions focus on the three key characteristics of AS, that is, scheduling under uncertainty, workload equity, and multiobjective optimization.
Scheduling under uncertainty
Uncertainty is often overlooked in previous studies (Bergh et al., 2013) and has been integrated into healthcare PS problems in recent years (Kim & Mehrotra, 2015; Rath et al., 2017). Robust optimization methods are used in OR staffing and scheduling (Rath et al., 2017) to handle uncertainties. However, the robust solutions, that is, those under the worst‐case condition, are excessively conservative in day‐to‐day clinical operations, and the optimized solutions under the average condition (expected value) can be suboptimal with extreme uncertainties. Two‐stage stochastic optimization approaches were used to create schedules under uncertainty by combining here‐and‐now and wait‐and‐see decisions assuming further information, for example, case length estimation (Batun et al., 2011) and nursing demand (Kim & Mehrotra, 2015), is available at a time closer to the surgical date. The wait‐and‐see decisions from two‐stage models have the capability to adapt to the realized uncertainty and reduce the conservativeness (Nohadani & Roy, 2017). Unfortunately, the inaccurate case length estimation, high cancelation rates, large number of add‐on cases, and rescheduling and resequencing are all sources of uncertainties in the partner hospital that are not realized prior to the surgical date. To capture these sources of uncertainty simultaneously, historical demand that measures the number of concurrent active cases is utilized and conditional value‐at‐risk (CVaR) is used to hedge against demand uncertainty. Comparatively, on the spectrum of conservativeness, CVaR fits in between the robust and stochastic models, protecting against both expected and the worst‐case uncertainties.
CVaR was introduced in data‐driven portfolio optimization as a risk measure to control the loss within certain confidence levels (Rockafellar & Uryasev, 2002). CVaR has been introduced in healthcare research in the recent literature (F. He et al., 2019). F. He et al. (2019) developed a nurse scheduling model minimizing a weighted cost function using CVaR‐based constraints to account for demand uncertainty. However, unlike in nurse scheduling, where the providers have similar skills and the demand for a predefined shift is relatively stable, the AS problem requires precise demand inputs, for example, demands at every half hour, to assign shifts with flexible durations to providers to accommodate specialties and preferences.
Scheduling equity
Scheduling equity, considered synonymous with “fairness” in the literature, is one of the major objectives of PS in the healthcare domain because providers have fairness concerns (Fügener et al., 2015; Rea et al., 2021; Stolletz & Brunner, 2012). Equity can be interpreted as evenly distributed workloads, including the assignment of unpopular shifts and the balancing of employee‐specific shift requests (Erhard et al., 2018). Lapègue et al. (2013) and Prot et al. (2015) developed methods to address the flexible shift‐design PS problem with an equity criterion. More specifically, the objective is to minimize the difference between the highest and the lowest nurse gap values, where the gap value is defined as the difference between the targeted and the assigned clinical workloads. Baum et al. (2014) used shift preferences to model workload equity, that is, maximizing the overall workload equity by minimizing the average discrepancies in individual preferences concerning the schedule. Fügener et al. (2015) formulated a multicriteria optimization model considering the maximization of the number of assignments, and the minimization of the penalty costs derived from violations of the equity constraints. The optimal number of providers can be considered jointly to improve the equity in the schedules, as Barrera et al. (2012) proposed. However, these competing objectives are yet to be explored in the AS problem.
Multiobjective optimization
Multiobjective optimization, composed of workload equity and other objectives in this work, is essential for healthcare PS problems. In an optimization model, solely considering one objective, such as equity or preference, may lead to undesirable solutions because of the ignorance of the other competing objectives, such as the total workload of all providers and the number of providers needed. Erhard et al. (2018) listed the typical objectives of physician scheduling, including the minimization of overtime hours (Ganguly et al., 2014), patient handoffs (Kazemian et al., 2014), and patient waiting times (Naderi et al., 2021). Because there is no unique solution that optimizes all the objective functions simultaneously in a general multiobjective programming problem, preference information is needed from the decision‐makers in the solution process to judge the quality of the candidate solutions and to make trade‐offs. It is a quite common approach in healthcare literature to solve multiobjective programming problems by solely optimizing a weighted sum of the objective functions. However, such an approach is not considered to be a good method (Steuer, 1986; Sun, 2014). Commercial mathematical programming software packages for single objective optimization problems stop after finding the first optimal solution and may not give the decision‐makers options to make trade‐offs (Sun, 2014).
In the ɛ‐constraint method, one of the objective functions is optimized and the other objective functions are treated as constraints by assigning acceptable values to them (Chankong & Haimes, 2008; Cohon, 2004; Sun, 2014). Mavrotas (2009) and Pourrezaie‐Khaligh et al. (2022) summarized the advantages of the ɛ‐constraint method over the weighted sum method. However, the solution time and effort needed by the ɛ‐constraint method increase as the number of objective functions increases. Pourrezaie‐Khaligh et al. (2022) applied the ɛ‐constraint method to optimize a healthcare facility location/network design problem and claimed that the ɛ‐constraint method had advantages over the weighted sum method. Chen et al. (2023) applied the ɛ‐constraint method to optimize emergency medical resource allocation. However, hardly any research using the ɛ‐constraint method is found in the healthcare PS literature.
As far as known, no AS model and solution method reported in the literature considered all features of demand uncertainty, flexible shifts, and fairness using multiobjective optimization. Although some physician scheduling methods in the literature included the modeling of equity and preference using different optimization techniques, hardly any of them fully considered all the characteristics of the problem pertaining to detailed physician specialties and lifestyle preferences with multiobjective optimization models under demand uncertainty, especially in clinical applications. The data‐driven multiobjective two‐step AS framework is developed to fill in this gap.
PROBLEM DESCRIPTION AND MODEL FORMULATION
For the concerned anesthesiology department, the goal of AS is to generate a schedule to cover various clinical services contracted with different clinical units and to satisfy demand while meeting institutional protocols such as provider educational and administrative duties. The purpose of automating the AS process is to reduce the burden of scheduling while keeping stakeholders engaged in and supportive of the proposed process. Stakeholder engagement was intentionally prioritized from the start by designing the automated AS process to align with current practice and is done by developing a two‐step AS framework that resembles current practice in the concerned department. Before the model formulation of the AS framework, a detailed problem description is provided by contrasting the original and the proposed AS processes.
Problem description
The original AS process. In ORs of the partner hospital, which make up most of the clinical demand in the anesthesiology department, surgical cases are booked following both block scheduling and open scheduling policies until the morning of surgery. In block scheduling or block allocation, a block of time in an OR is assigned to a specific surgeon or surgical group to book cases up to 12 months in advance, and this block is unavailable to other surgeons. In open scheduling, a surgical case is booked by any surgeon in an OR with open time available on a first‐come‐first‐served basis. Open scheduling is followed when a surgical block is released. For trauma services, a block is released on the morning of surgery. For nontrauma services, a block is released a week in advance if it is fully available and is released 2 days in advance if it is partially available. The staffing decisions of different clinical resources, that is, nurses, surgical technologists,3 residents, CRNAs, and anesthesiologists, occur 1–2 months in advance and cover the surgical blocks, whether the blocks are released or not. The schedules of different clinical resources and block allocation must be coordinated. A scheduler assigns a starting time and an OR to each case and reassigns cases when schedule disruptions, for example, add‐on cases, delays, and cancelations, happen. Block scheduling and open scheduling of the partner hospital are similar to those in B. He et al. (2012).
In this anesthesiology department, the original AS process is hierarchical, centered around the AS module, as shown in Figure 1. It takes block allocation and open scheduling information from the partner hospital as input. The provider self‐scheduling, including time‐offs, on‐call shifts, and professional development, is reserved 1–12 months in advance. The scheduling of specialties and on‐call shifts occurs 2–3 months before surgery. The subschedules for specialties are finished before the AS module executes. The AS module creates and publishes the monthly schedule 1–2 months in advance. The original AS module includes two steps. In Step 1, the clinical demand and the required number of generic OR shifts are empirically estimated. A provider may supervise multiple cases concurrently with department internal secondary anesthesia clinicians, that is, residents and CRNAs. The estimated demand and required shifts must align with departmental internal schedules and hospital clinical resources. To simplify the process, the clinical demand was estimated based primarily on hospital nurse schedules incorporated with block allocation. Generic OR shifts are assumed to have uniform durations in the original AS module. The original AS is coverage‐driven to assign generic OR shifts to cover ORs from open to close, the same as the nurse schedules. After coordinating the staffing decisions of different clinical resources, the anesthesiologist shifts are confirmed and ready to be assigned to providers. In Step 2, generic OR shifts and other required shifts are assigned to providers, ensuring the availability of enough providers in each clinical unit on the day of surgery. Given scheduled cases and provider shift assignments, the board runner, that is, a senior managing anesthesiologist, assigns providers to specific surgical blocks the business day before surgery. On the day of surgery, the board runner reassigns providers to changing and new surgical cases, relieves or preserves providers assigned generic OR shifts when the clinical demand changes, and tries to keep the shift durations uniform for workload equity. On the day of surgery, a generic OR shift, that is, a “flex‐end” shift which ends when demand permits, is scheduled. Ignoring the actual duration of a generic OR shift may lead to excessive clinical time, unexpected overtime, exacerbated workload equity, and breaking supervision rules stated by Burns et al. (2022).
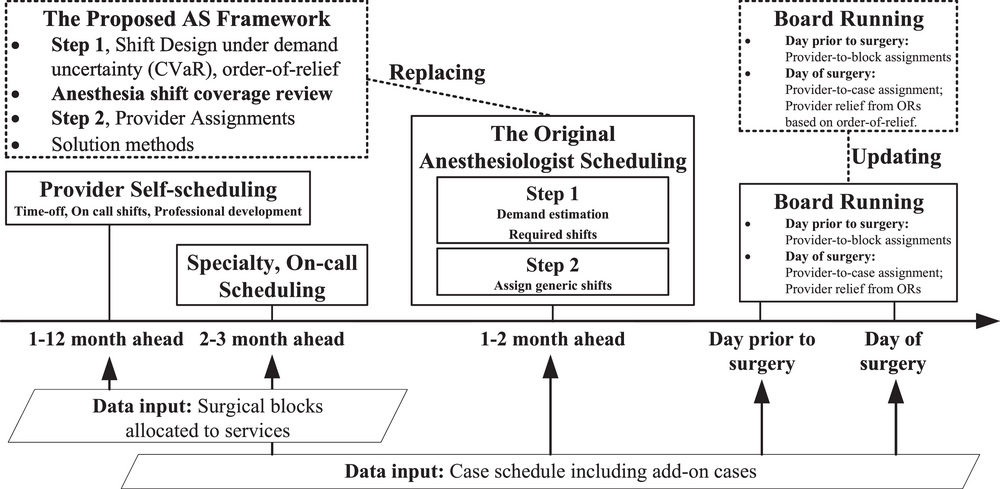
The original and the proposed AS processes. AS, anesthesiologist scheduling; CVaR, conditional value‐at‐risk; ORs, operating rooms.
The original AS process faces difficulties beyond the usual challenges associated with a Level I trauma center. First, the ORs have a bottom fifth percentile4 case length accuracy, where less than 50% of the cases finish within ±30 min of the scheduled duration. Second, almost 10% of the prescheduled cases are canceled (30th percentile4). Third, about 40% of the cases are added on to the schedule (20th percentile4) after publication. Because of the volatility and uncertainty in demand, cases and anesthesia coverage regularly change rooms throughout the day, exacerbating the provider workload equity and increasing the board runner management burden.
The proposed AS framework. To address the challenges in the original AS process, the proposed AS framework replaces the original AS module and updates the boarding running according to the additional information in the AS output, as shown in Figure 1. The AS framework is a two‐step process with models and solution methods. The proposed AS process integrates stakeholders in the loop to coordinate the schedules in the department and the partner hospital. Shift design, as Step 1, generates the daily required shifts and durations based on clinical demand under uncertainty. An order‐of‐relief mechanism is applied to assign a priority index to each generic OR shift to indicate its priority of being relieved from ORs when the demand permits. In this way, the coverage‐driven generic OR shifts are converted to demand‐driven. The historical clinical demand, measured by the number of concurrent active cases, is used to estimate the actual demand under uncertainty. The objective of shift design is to minimize total working time for all providers, and the output of shift design is a set of daily required indexed shifts and estimated durations to cover the clinical demand under uncertainty. The clinical demand data used to estimate the duration of the demand‐driven OR shifts have a month lag allowing time for performing an anesthesia coverage review. Based on the block allocation information, the department leaders first verify the shifts and durations with the specialty and on‐call subschedules and the secondary anesthesia clinician schedules. Then, the anesthesia schedule is reconciled with hospital clinical resource schedules to finalize the anesthesiologist shifts to be assigned on each day. Provider assignments, as Step 2, assign these shifts to providers considering the required number of providers and workload equity over time and across providers. The schedule sequences the provider daily shifts with the shift starting times and durations. The output anesthesiologist schedules are finalized, reviewed by the department leaders, and then published. On the day before surgery, the board runner assigns the providers to blocks according to the available case schedule, provider shift assignments, and estimated shift durations. On the day of surgery, the board runner systematically relieves the provider with the highest indexed shift from the ORs when the demand permits, following the order‐of‐relief mechanism, and reassigns blocks if necessary.
AS is a medium‐term tactical scheduling problem where rosters up to several weeks are generated, according to the categorization by Erhard et al. (2018). The AS prioritizes the two subschedules, that is, provider self‐schedule and clinical specialty and on‐call schedule. This framework supports strategic and detailed tactical decisions. At the strategic level, AS is expected to support departmental staffing decisions, that is, budget and hiring planning. At the detailed tactical level, unlike board running focusing on provider‐to‐room assignments, monthly AS facilitates board running by allocating the right number of providers at the right time and ensuring optimal and equitable provider schedules beyond the board runner shift.
Ultimately, the proposed AS framework generates equitable schedules minimizing the clinical time, evenly distributing the workloads across providers and over time for each provider, and minimizing the number of providers needed. The overall problem consists of a set of providers ℙ who are scheduled over a set of days





Shift design
The Step 1 model generates the daily required shifts and their estimated durations while minimizing the provider total working time with a data‐driven optimization approach. This step replaces the estimation of demand and required shifts in Step 1 of the original AS process as discussed above. Provider excessive clinical time is reduced by replacing the original coverage‐driven shifts with demand‐driven shifts. The estimated shift durations are used as a reference for the anesthesia shift coverage review shared with other clinical units.
To achieve contracted clinical coverages and meet institutional requirements and provider satisfaction, three designated types of shifts are considered with different degrees of flexibility for various services. Administrative shifts, represented by Let


















According to regulatory guidelines and case complexities, each anesthesiologist may direct anesthesia for one or more concurrent surgical cases with secondary anesthesia clinicians. Hence, the following assumptions are made: (a) provider transitions in a case are allowed, and the transition does not impact the workload and quality of care; and (b) the postanesthesia and documentation time is included in the case time. The shift duration is defined in Definition 2 below. For a shift
















where conditions in (1) and (2) ensure the determination of the shift status indicator, the ideal condition in (3) restricts the sum of the active shifts to be sufficient to cover the actual clinical demand


An order‐of‐relief mechanism is embedded in the proposed AS framework, as discussed in Subsection 3.1. Different ending priorities are given to eligible shifts at each time point









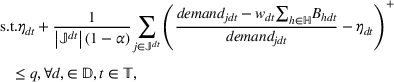
Although administrative and coverage‐driven shifts have fixed durations, the demand‐driven shifts have flexible durations, which are subject to the clinical demand, that is, typically unpredictable. The clinical demand varies significantly due to unpredictable case length, frequent cancelations, add‐on cases, and trauma cases in the ORs of the partner hospital, as described in Subsection 3.1. One way to account for the demand uncertainty is to use CVaR to control the stochastic behavior of demand using historical data (F. He et al., 2019). For AS, CVaR is determined by the weighted average of the “extremely” high demand in the upper tail of the demand distribution beyond the value‐at‐risk (VaR) cutoff point. As a risk measure, CVaR has superior mathematical properties compared with VaR. It can be used as either an objective function or a constraint in optimization models to control the risk of loss. In both cases, it can be reduced to a set of linear functions, which are easy to handle in mathematical programming models (Sarykalin et al., 2008).
According to Rockafellar and Uryasev (2002), a CVaR constraint in a model can control the loss under a user‐specified risk‐tolerance level q in the general form
















The Step 1 model of the AS framework has three sets of decision variables, that is, shift status indicators










The objective function (5) of the Step 1 model minimizes the total shift time. Because the objective function is minimized, only the durations of the required shifts can have positive values. Requirements for shift durations


The output of shift design is a set of daily required shifts with their order‐of‐relief indices and estimated durations to cover the clinical demand under uncertainty, ensuring minimum clinical time. As the decision process discussed in Subsection 3.1, the anesthesia shift coverage review is performed by the leaders from both the anesthesiology department and the perioperative services at the partner hospital to ensure the designed shifts have to be reconciled with the departmental internal and external hospital schedules. Then, the anesthesiologist shifts to be assigned each day are finalized for provider assignments.
Provider assignments
To meet clinical coverage and improve equity, the goal of provider assignments, that is, the Step 2 model of the AS framework, is to assign shifts to providers so as to consider three objectives, that is, the minimization of inequality in workload, consecutive intensive workloads, and number of providers.
In the anesthesiology department, administrative and coverage‐driven shifts are all considered to have the same workloads and require the assigned providers to perform their duties throughout the duration of a shift. These shifts can be assigned in the Step 2 model or preassigned to providers on given days based on the provider's requests and preferences. Demand‐driven shifts cover most of the clinical demands, and their workloads and durations vary from shift to shift and from day to day due to the high variability in demand. Two approaches are employed to minimize the inequality in workload allocations. First, constraints are set up to distribute coverage‐driven hard, including overtime, overnight, and weekend, shifts equally. Second, the variation of the workload is minimized among all providers. The workload is parameterized using an hourly workload index representing the required effort or burden per hour. The workload index

The Step 2 model uses the set of daily required shifts





Objective function (13) minimizes the maximum workload among the providers, referred to as MinMax, which is of the highest importance to the concerned department with regard to workload equity. Objective function (14) minimizes the maximum 2‐day average workload, aiming to achieve workload equity over time for each provider, referred to as MinMaxTDAvg, following the protocol of postcall assignments where an intensive shift should be followed by an easy shift on the next day (Millar & Kiragu, 1998). Objective function (15) minimizes the number of required providers, referred to as ProNum, that represents the efficient allocation and utilization of the scarce anesthesiologist resource.
Besides MinMax defined in (13), the workload equity objective function can be defined in alternative forms. One such form in (16) minimizes the sum of the absolute workload deviations from the average of all providers, referred to as TotalAbs,
Constraints of the Step 2 model are listed in (18)–(39) in the following:



















Constraints (18) define auxiliary binary variables




Constraints (31)–(37) capture the expected timing of the assigned shifts. Constraints (31) and (32) ensure that an administrative shift is finished during the provider working day. Constraints (33) sequence provider daily shifts based on shift starting times and durations. Constraints (34) set the fixed starting times for the coverage‐driven and demand‐driven shifts. Constraints (34) and (35) together force the decision variable to


SOLUTION METHODS
The solution methods for the AS problem are presented in the following. The required concepts from multiobjective optimization are reviewed first. The details of the ɛ‐constraint method are then discussed for the Step 2 multiobjective optimization model. An iterative solution method to improve solution quality for the application of the AS framework in the anesthesiology department is finally presented. The objective functions in (13) and (14) and the alternative equity objectives in (16) and (17) are reformulated for easier mathematical manipulation in the solution process. The details of the reformulations are described in Supporting Information EC.2. All solution methods are implemented using Python 3.10 and Gurobi™ 9.5,5 and all experiments are conducted on a desktop workstation, Dell Precision 3431, with an Intel® Core™ i5‐9600 CPU @ 3.10 GHz and 16.0 GB RAM.
Background on multiobjective optimization
According to the Step 2 model of the AS framework, let


















The ε‐constraint method
The best practice in solving a multiobjective optimization problem is using an interactive procedure that elicits and incorporates the decision‐makers’ preference information into the solution process, if the decision‐makers are willing to cooperate and participate (Steuer, 1986; Sun, 2014). A typical interactive procedure has two alternating phases with a phase of computation alternating with a phase of preference information elicitation and decision. A practical approach of eliciting preference information is through pairwise comparisons among the representative nondominated solutions (Sun et al., 1996, 2000).
However, it is difficult for the decision‐makers, that is, department leaders and all providers in this context, to be fully involved in an interactive solution process of a multiobjective optimization problem (Sun, 2014). Alternatively, the AS framework uses the ɛ‐constraint method to find representative nondominated solutions for the Step 2 model. In an ɛ‐constraint method, one of the objective functions, usually the most important one, of the problem is optimized, and the rest are converted to constraints by assigning each of them an acceptable value (Chankong & Haimes, 2008; Cohon, 2004; Sun, 2014). Therefore, assuming MinMax (13) is the most important objective function, the Step 2 model is







An iterative solution method
In the current practice of the anesthesiology department, preassigned shifts are considered in the AS process due to the provider specialties, and healthcare continuity, clinical and lifestyle preferences. Providers may have multiple preassigned shifts fixed on their schedules. To align with this practice, the preassigned shifts are included as an extra set of constraints in the optimization model as defined in constraints (27). These preassigned shifts usually have high associated workloads for which the equity objectives, that is, MinMax and TotalAbs, produce suboptimal schedules. Specifically, some providers with extremely heavy workloads and fixed schedules restrict the model in optimizing other providers’ schedules. An iterative solution method is developed to overcome this limitation. It consists of two modules: Module 1 identification of a blocking provider and Module 2 iterative improvement of each provider's schedule.
A “blocking” provider is indexed with

























APPLICATIONS
The results of Step 1, shift design, and the analysis of the proposed alternative forms of the workload equity objective function are provided. Then, two clinical applications, budget and hiring planning and monthly AS, are discussed. Both applications use the result of Step 1, shift design, based on the historical clinical demand. In budget and hiring planning, the Step 2 model is solved using the ɛ‐constraint method. In monthly AS, the Step 2 model is solved using the iterative solution method to optimize the schedule of each individual provider with preassigned shifts in clinical operations.
Step 1 results and analyses
The historical demand data of surgical time, room time, and anesthesia time from September 1, 2020 to December 31, 2020 are taken as the input of the Step 1 model. This period was selected as it was between surges of the COVID‐19 pandemic when the surgical block was fully active and demand data well represented historical demand data over a sufficiently long‐time frame. The output of shift design includes daily required shifts and durations, as shown in Figure EC.1 in Supporting Information EC.3. In general, the Step 1 results match decision‐makers’ experience and daily clinical activities at the anesthesiology department. As shown, the shift durations, and ultimately workloads, vary from shift to shift and from day to day, demonstrating a need to balance the workloads among providers and over time. Additional results and discussions from the Step 1 model are provided in Supporting Information EC.3. Furthermore, a comprehensive analysis of the risk‐tolerance level of the CVaR constraints used in the Step 1 model is provided in Supporting Information EC.4. The AS framework uses CVaR because it is less conservative than the robust optimization approaches that consider the worst cases only. CVaR considers the demand uncertainty as a distribution and accounts for the risk at the tail of the distribution with a confidence level, for example, 
The alternative forms of the workload equity objective function, MinMax (13), TotalAbs (16), and Variance (17) of the Step 2 model proposed in Subsection 3.3 are reformulated for implementation as detailed in Supporting Information EC.2. An open AS problem without preassigned shifts for a 1‐week scheduling horizon is used in the analysis (see Supporting Information EC.5). The results show that, for the open AS problem, runtime and solution quality can be best balanced by using TotalAbs among the three alternative forms of the workload equity objective function. However, department leaders have used MinMax as the primary measure for workload equity in the original AS process, especially due to its ease of computation. Therefore, both MinMax and TotalAbs are used for further comparisons in the proposed AS process, aligning with existing works (Alkaabneh & Diabat, 2022).
Budget and hiring planning
In this application, the Step 2 model is solved for an annual budget and hiring planning analysis to find the ideal number of providers to be deployed at the ORs of the partner hospital, considering workload equity and consecutive intensive workdays. The weekly schedule of the open AS problem discussed in Subsection 5.1, and Supporting Information EC.5 is generated to cover the daily required shifts obtained in Step 1 in Supporting Information EC.3, based on the historical demand data. MinMax is used for the workload equity objective function by the decision‐makers of the department. A convergence analysis on the workload equity objective functions is provided in Supporting Information EC.6. Approximate nondominated frontiers generated with the ɛ‐constraint method, as shown in Figures 2 and 3, are provided for the decision‐makers to make trade‐offs. Each solution is associated with a sample schedule to provide the decision‐makers with an intuitive perception of the shift assignments for them to evaluate the feasibility of the staffing plans and to provide in‐depth feedback.
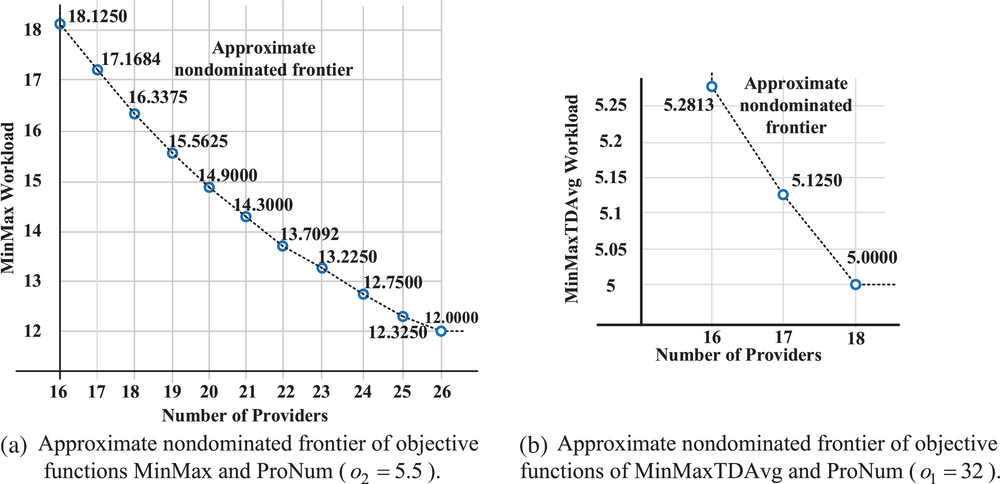
Two‐dimensional nondominated frontiers.
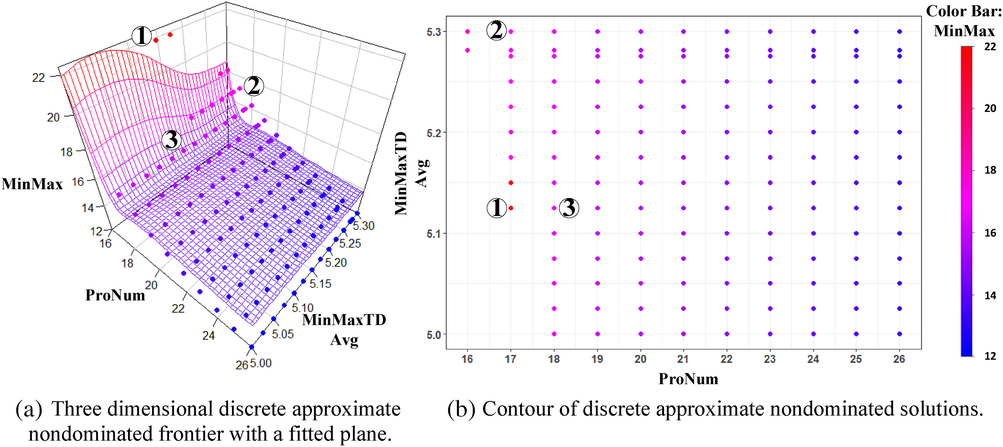
Three‐dimensional nondominated frontiers.
According to the decision‐makers, a provider's maximum allowable workload and the maximum allowable 2‐day average workload index are restricted to 









Three‐dimensional nondominated frontiers can be generated according to the reformulations in (40)–(42) and in (43)–(45) discussed in Subsection 4.2. Figure 3 is plotted when the Step 2 model optimizes the objective function (40). By parametrical variation in the right‐hand sides of the two constraints converted from the two objective functions, that is, o 2 and o 3 in (41) and (42), representative nondominated solutions on the nondominated frontier are obtained. In Figure 3, the color scale on the points indicates the value of MinMax z 1, and the fitted plane in Figure 3a is the approximate nondominated frontier.
The nondominated frontiers have the following connotations. The consecutive intensive workload objective cannot be further improved after the number of providers reaches 18, establishing a useful critical minimum number of providers for the department. The workload equity objective becomes significantly worse when the number of providers is reduced from 18 to 17 or fewer and cannot be further improved after the number of providers increases to 26 or above. The nondominated frontiers can be used for the department leaders to make trade‐offs and to select the most preferred solution when creating budget and hiring plans. When sacrificing the objective values of consecutive intensive workloads and the number of providers, z 2 and z 3, better workload equity, that is, smaller z 1, can be achieved due to the increased scheduling flexibility. For example, in Figure 3, the department leaders may choose ② over ①, so that a 23.3% improvement in workload equity can be achieved by making a 3.4% sacrifice in consecutive intensive workdays. Similarly, the department leaders may choose ③ over ①, so that a 27.1% improvement in workload equity can be achieved by making a 5.9% sacrifice in the number of providers. Using this information, leadership can truly weigh the costs and benefits of the number of providers, recruitment, retention, and scheduling optimization investments.
Monthly AS
The AS framework is applied to generate the monthly schedule for the anesthesiologists in the concerned academic anesthesiology department. The Step 2 model sequences and assigns the preassigned shifts and the other daily required shifts obtained by the Step 1 model to generate a schedule satisfying the clinical demands. In this application, only the provider workload equity objective is considered for the following reasons. First, it is unnecessary to include ProNum (15) since monthly AS utilizes all available providers after completing the budget and hiring planning. Second, the coverage‐driven preassigned shifts limit the efficacy of MinMaxTDAvg (14) because the long fixed shifts on consecutive days with heavy workloads are typically in the preassigned shifts. However, constraints (29) and (30) ensure that no hard shifts in the set 
Four optimization approaches considering different forms of the workload equity objective function and solution methods, that is, TotalAbs, TotalAbsIte, MinMax, and MinMaxIte, are applied and compared. To evaluate their performance, the following objective function,
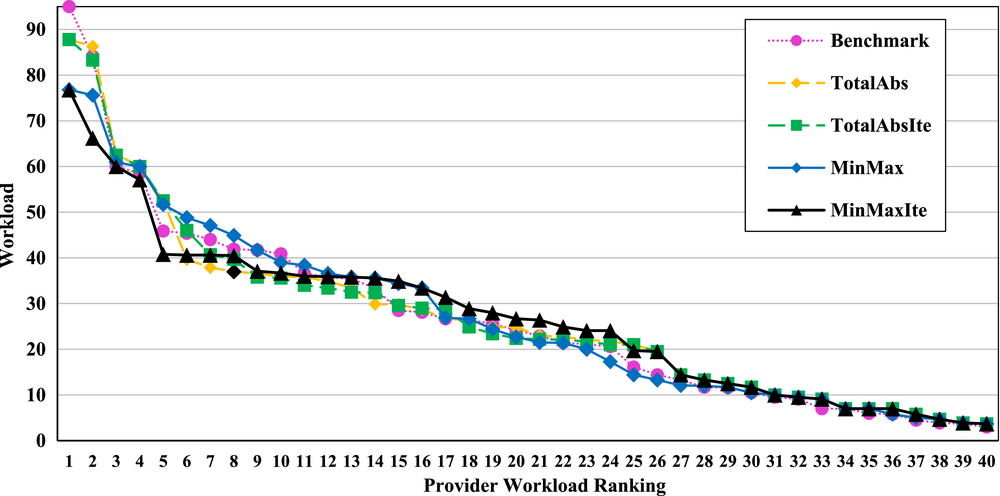
Workloads and rankings by using five different approaches in the academic department.
Figure 5 illustrates the solution quality of the five approaches on three workload equity criteria, that is, workload standard deviation, the total workloads of the top five providers, and the total workloads of the top 10 providers. In this clinical application, the standard deviation serves as the overall performance measure for workload equity, while the total workloads of the top five and the top 10 providers are of importance to department leaders in practice. For workload standard deviation, the solution with MinMaxIte has 7.7% and 11.5% improvements over the solutions with MinMax and Benchmark, respectively. For the total workloads of the top five providers, the solution with MinMaxIte has 7.4% and 12.4% improvements over the solutions with MinMax and Benchmark, respectively. For the total workloads of the top 10 providers, the solution with MinMaxIte has 9.2% and 10.9% improvements over the solutions with MinMax and Benchmark, respectively. Solutions with TotalAbs and TotalAbsIte have unsatisfactory quality because the total absolute deviation is less sensitive to extreme values than the maximum deviation. In general, MinMaxIte obtained the least standard deviation and the least total workloads of the top five and the top 10 providers among all the five approaches.
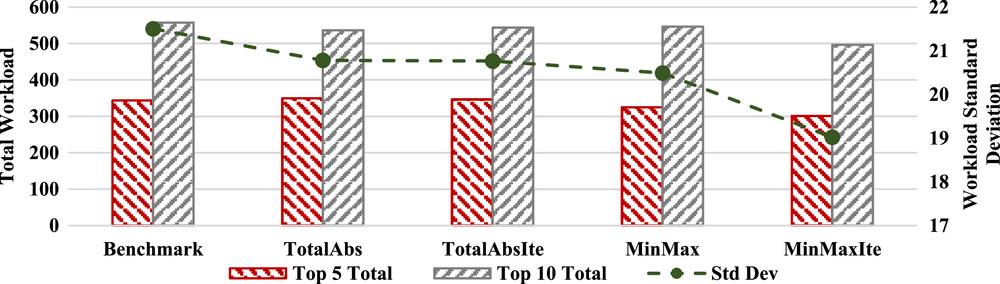
Performance of workload equity of the five approaches.
MANAGERIAL IMPLICATIONS
This work addresses the practical AS problem for a large academic anesthesiology department to aid managers with their operations and staffing decisions. Managerial implications and potential benefits from the successful implementation of the proposed framework are presented.
Engagement and buy‐in. Engaging stakeholders and obtaining buy‐in is an essential component of the successful implementation and operationalization of a data‐driven decision‐making process (Scheinker & Brandeau, 2020). Three steps were deliberately taken to ensure stakeholder engagement and buy‐in. First, due to the inherent complexity of PS within the healthcare domain, engagement and buy‐in highly depend on the partnership between the stakeholders and the modeling team. Dedicated physician leaders, who are responsible for the anesthesia schedules and clinical operations, were partnered to guide the development and execution of the AS framework. The leaders helped in messaging all anesthesiologists to create engagement and buy‐in, which provided the feedback that allowed the modeling team to adjust the models as required. In addition, a focus group of faculty anesthesiologists helped in evaluating the proposed changes to the original AS process to ensure seamless development and deployment. Full collaboration of physicians, administrators, and operations management researchers at the early stage ensured two key elements for successful development and implementation: (i) development of meaningful modeling requirements and goals that led to the constraints and objectives in the models and (ii) a thorough description of the AS workflow that explains the upstream, for example, the definition and formats of inputs, and downstream, for example, the feedback collection process, of the AS framework. Second, the AS framework was developed to minimize the stakeholders’ effort to adopt the new AS process. Consequently, the proposed AS framework was aligned with the original AS process, but automated tasks that were a burden before, that is, removed the effort of the managing physicians to balance workloads and alleviated the effort of the board runner on the day of surgery. Third, aligning with the original practice, the two‐step AS framework allows for the review of shift durations and coverage by the department and hospital perioperative leaders. Engagement in model development and deployment enabled a successful implementation and continuous improvement and expansion of the AS framework, as observed in previous works (Lal et al., 2015). Furthermore, the AS framework provided insights for the contract negotiation with the partner hospital and a budget proposal for a new ICU site in 2021. The estimated clinical demand, shifts and durations, on‐call obligation assignments, and provider workloads were used as evidence to support the new budget plans.
Iterative and incremental development. The proposed AS framework was designed following an iterative and incremental development practice to allow for flexibility, continuous improvement, and expansion (Larman & Basili, 2003). The requirements from administrators and providers were not clear until a preliminary AS prototype was first deployed for feasibility verification in September 2020, based on which, feedback was gathered, and the next iteration of development was initiated. Consequently, modifications were made to fit into isolated modules for easier updates. Feedback was constantly collected, and requirements were iteratively updated. As time evolved and the iterations progressed, modifications became easier, requiring lesser and lesser postprocessing. In fact, the postprocessing schedule changes were reduced from 21% (first iteration) to less than 1% (12th iteration). The AS framework has gone through monthly iterations and has been deployed in AS practice since the preliminary AS prototype. Prior to implementation, the manual process of the monthly AS required the managing physicians to make over 1500 assignment decisions by trial and error while considering workload equity only for a few extreme cases. The optimal schedules as well as the time and cost savings achieved by automating the AS process played a key role in motivating the managing physicians, analysts, and administrators to engage stakeholders and help in data retrieval, feedback collection, and clinical implementation. The automated AS process is estimated to relieve a managing physician 23 hours per month and a perioperative informatics director 20 hours per month, working exclusively on the monthly AS. Compared to the original AS process, this automation achieves approximately 82% and 95% time savings for the managing physician and the perioperative informatics director, respectively, that they would otherwise dedicate to AS.
Workforce management. For the department to fulfill the clinical demand at the contracted medical units, budget and hiring planning are critical to ensure competitiveness in the “tight” market for anesthesiologists and CRNAs and to ensure clinical coverage. The nondominated frontiers provide the flexibility for the department leaders to make trade‐offs. This trade‐off structure is based on the clinical, workload, and fairness concerns of the departmental leaders and providers. From the nondominated frontiers obtained using the ɛ‐constraint solution method, workload equity can be improved by sacrificing the consecutive intensive workdays and/or increasing the number of deployed providers due to the increased scheduling flexibility. However, excessive resources may cause slackness and provider idleness. The nondominated frontiers demonstrate the critical points that should be watched carefully in the budget and hiring planning. These critical points exist when a slight change in the value of one objective function causes large changes in the values of the other objective functions, such as a one‐unit change in the number of providers leads to large changes in the workload equity and in the maximum 2‐day average workload. The nondominated frontiers are also used as references to optimize the use of the limited anesthesia resources, that is, reducing the administrative shifts and opening the volunteering postcall/precall shifts, and/or reduce the OR coverages, at different levels of labor shortages.
Improved equity. Two distinct comparisons are made to reveal the benefits of the proposed AS process. First, the workload equities in the schedules generated by the proposed AS framework and the original AS process are compared. An F‐test for the equality of two variances of the provider monthly workloads using samples of the most recent schedule and the schedule generated by the original AS process produced a one‐tailed p‐value of 0.0168, showing significant improvement. However, minor schedule modifications are often made closer to the day of surgery in the clinic. Hence, a second comparison is made to verify the improvement in the actual provider workloads on the day of surgery. Historical schedule data from September 2019 to March 2023 was collected and analyzed for each provider's schedules and workloads. Providers’ 3‐month average daily workloads pre‐ and post‐implementation were compared. As shown in Figure 6, the extreme workloads for providers were mostly reduced, and the workload variance was reduced from 2.92 to 1.39. By performing an F‐test for the equality of the two variances of the two sets of workloads, a one‐tailed p‐value of 0.0088 is obtained, showing significant improvement.
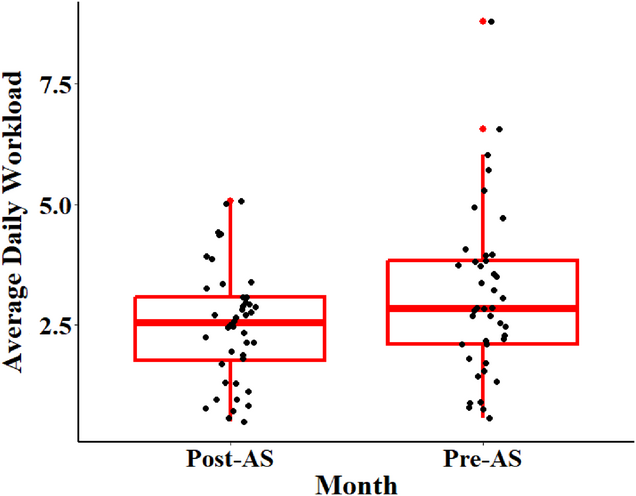
Three‐month average daily workloads of pre‐ and post‐AS framework implementation.
Job satisfaction. The AS framework supports equitable anesthesiologist schedules, which is a key factor in physician job satisfaction (Williams & Skinner, 2003). The original process, often being considered biased, might lead to conflicts regarding workload, reduced job satisfaction, and even workforce turnover. According to two surveys conducted among all faculty anesthesiologists on March 17, 2021 and April 19, 2021, satisfaction with the monthly AS results improved from 3.13/5 to 3.44/5. As Ajayi et al. (2021) pointed out, physicians pay close attention to competitive pay and benefits, employee perks and incentives, and performance reviews and perceive the prioritization of workload equity as a key to provider recruitment and retention. Moreover, by promoting equity, the AS framework has become an incentive for hiring and retention purposes from the fiscal year 2021.
CONCLUSIONS
This work addresses the AS problem motivated by the needs of a large academic anesthesiology department. By exploiting historical demand, a data‐driven AS framework is developed to determine the schedules of the anesthesiologists. Factors considered in the schedules include the variations in workloads among providers, the balancing of the intensive workdays, the number of providers needed, satisfaction of the demand coverage and accommodation of the provider specialties, and clinical and lifestyle preferences. The AS framework uses a two‐step approach to mimic the preexisting manual process. The first step, shift design, computes the optimal shifts considering clinical demand under uncertainty using historical demand data and CVaR. The second step, provider assignments, generates schedules considering optimal and equitable workload distribution and provider availability using multiobjective mixed‐integer optimization.
An ɛ‐constraint method is implemented to generate representative nondominated solutions so as to construct approximate nondominated frontiers for the decision‐makers to make trade‐offs. An iterative method iteratively minimizing the maximum workload deviation among the providers is developed to further improve the schedules with preassigned shifts. To efficiently deploy the framework, the performances of the alternative forms of the workload equity objective function are compared. Among the three alternative forms, TotalAbs best balances between runtime and solution quality, while MinMax uses the least runtime. Two clinical applications, budget and hiring planning, and monthly provider scheduling, are explored using the AS framework. The former suggests that a limited sacrifice on consecutive intensive workloads or on the number of deployed providers can significantly improve the workload equity of the resulting schedule. The latter suggests that the MinMaxIte approach achieves the most desirable results in the clinical applications with preassigned shifts. The proposed framework is generic and can be integrated with case scheduling activities to improve coverage and service quality.
The following limitations in this work are acknowledged and serve as future research opportunities and extensions. First, although the solution methods in the AS framework are feasible in the applications, the high computational costs in solving the nonlinear multiobjective mixed‐integer programming model can be improved for a broader extension of this work. Metaheuristic procedures, such as tabu search and particle swarm optimization, may be designed to achieve approximate/optimal solutions under reasonable runtime. Second, although the AS framework achieves workload equity and reduces scheduling burden, its impacts on clinical performance in the ORs, especially on the day of surgery, remain unknown. An empirical analysis has been initiated to evaluate the clinical impact of the proposed AS framework, which will explore the clinical, billing, scheduling, and human resource data to evaluate whether the AS framework considering workload equity improves clinical performance, quality of care, and job satisfaction. Finally, the AS framework will be extended to consider other activities, such as CRNA and resident scheduling, and other divisions, such as a preoperative clinic, trauma surgery, and an affiliated pain clinic.
Footnotes
ACKNOWLEDGMENTS
The authors thank the editors and two referees for their valuable comments and suggestions provided during the review process. The authors also acknowledge the faculty and staff of the Department of Anesthesiology at UT Health San Antonio for their feedback and support in improving the AS process.
1
2
3
4
The percentiles are from the AI & Analytics of Epic, benchmarking of the peer ORs tracking performances at
5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.