
Abstract
This article examines how time both exacerbates and destabilizes existing inequality by stratifying agency. Drawing on five years of fieldwork in nine cancer clinics and 196 in-depth interviews with 96 patients navigating a terminal cancer diagnosis toward the end of life, we show the centrality of “temporal misalignment”—a mismatch between the temporalities enacted by individual actions and those imposed by institutional contexts structuring when and how action is possible. A combination of ethnographic data and multiple correspondence analysis (MCA) reveals how effective use of resources requires cancer patients to (1) triage conflicting demands of treatment, work, family, and bureaucratic schedules; (2) reconcile mismatched trajectories of disease progression and healthcare institutions; and (3) anchor uncertain decisions at present in an anticipatable future. These efforts to manage temporal misalignment not only reproduce resource disparities, but also create new, imminent, and often embodied constraints on agency that even the most advantaged patients find resource-draining and goal-displacing as the disease progresses. Reconceptualizing time as a ruptured relationship between agency and contexts offers important sociological insights into how resources, institutions, and culture operate and intertwine to shape inequality in healthcare and beyond.
Introduction
Sociological research has long examined how inequality shapes individual life chances in time and over time. Despite important contributions across subfields that chart the relationship between inequality and time, such as how (dis)advantages accumulate over the life course (DiPrete 2020; DiPrete and Eirich 2006; Torche and Nobles 2024) and how gender, race, and class shape time use in labor and at home (Goldin 2014; Hochschild 1989; Nelson et al. 2023; Offer and Schneider 2011; Schneider and Harknett 2019), time remains loosely theorized in many explanations of how inequality works and why inequality matters.
The significance of time in understanding inequality becomes evident when people find themselves caught between compressed and misaligned temporalities. Patients and caregivers managing chronic or terminal illnesses, for example, often have to juggle competing demands on their time, both from the challenges of everyday life and the effects of disease and treatment (Altomonte 2016, 2022; Bontemps 2025; Livne 2021; Lutfey and Freese 2005; Paust et al. 2023). This juggling not only reflects prior disparities in resources and experience, but also unequal access to care at their convergence (Abramson 2015; Carr 2019; Gengler 2020; Link and Phelan 1995; Lutfey and Freese 2005; Shim 2010). In an institutional context where individuals have to actively strategize against their disadvantages—even just to receive a diagnosis, access treatment options, and utilize insurance benefits—it is often through the ability to accommodate the institution’s intricate and sometimes paradoxical temporalities that inequality is acutely felt.
Being subject to conflicting temporalities translates structural inequalities into pragmatic problems that people have to respond to and act upon (Emirbayer and Mische 1998; Gross 2009; Sewell 1992). When the temporality required for individuals to construct purposeful action does not align with the temporality allowed by the institutional context, individuals must first manage such misalignment in their temporal relationship with the institution before they can reclaim a sense of agency to act (or not act), often exacerbating existing disadvantages in the process. Prior work hints at this relational feature of time, but how it connects institutions, agency, and inequality has not been conceptually and empirically clarified.
To understand how time creates dynamic forms of inequality, we draw on the experience of people navigating time between a terminal cancer diagnosis and the end of life. Our data come from five years of fieldwork at two research-intensive cancer centers in the metropolitan West Coast and Midwest United States, and 196 longitudinal interviews with 96 terminal cancer patients. To explain the diverse ways patients understand and activate resources to navigate the everyday and existential challenges of cancer, we leverage the concept of temporal misalignment—a mismatch between the temporalities enacted by individual action and those imposed by institutional contexts—which people who seek to maintain or activate their resources often have to overcome.
We find three types of temporal misalignment to be central in the lives of those in our study—schedule conflict, trajectory mismatch, and anticipation uncertainty. Combining rich ethnographic data with multiple correspondence analysis, we show that who experiences what type of misalignment, what decisions they make in trying to manage this misalignment, and how their efforts shape outcomes down the road, cannot be reduced to the unequal distribution of resources. On the contrary, each type of temporal misalignment presents unique, pragmatic, and potentially action-inhibiting dilemmas requiring patients to make decisions that not only reproduce existing resource disparities, but also create new, imminent, and often embodied constraints on their agency. Even for the most advantaged patients, efforts to manage temporal misalignment inevitably become resource-draining and goal-displacing as the disease progresses. In this way, the meaning of resources and the possibilities of agency are conditioned by a ruptured temporal relationship between individuals and the institution, which may exacerbate or destabilize existing inequality. Our findings show why the temporal entanglement between agency, resources, and institutions is significant in ways often underestimated, yet crucial for a sociological understanding of inequality in healthcare and beyond.
From Unequal Resources To Unequal Agency
Sociologists have shown how unevenly distributed economic, cultural, and social resources shape a myriad of outcomes over the life course. Yet, even when resources are equally distributed, they are not always equally used. Resources only become meaningful and valuable (i.e., they become capital [Bourdieu 1986]) when valued and used in institutional contexts like schools, labor markets, hospitals, or neighborhoods (Bourdieu 1990a; Bourdieu and Wacquant 1992). Scholars have argued that reducing individual agency to the distribution of resources in the field is a selective and over-deterministic reading of Bourdieu’s theory (see Hall 1992; Sallaz and Zavisca 2007; Sewell 1992). Nevertheless, even in many Bourdieu-inspired analyses, when and how resources become activated—what Lareau (2003) calls the “capital activation problem”—remains a challenge to explain. Why do some resources get activated while others remain dormant? Developing theoretical models that explain how, when, and to what end individuals put their resources to action is central to our understanding of why inequality persists and how it can be mitigated (Lamont and Lareau 1988; Lareau 2003; Small, Harding, and Lamont 2010).
Time is a critical yet under-theorized dimension of how unequal resources become unequal agency—disparities in individuals’ capabilities to mobilize their resources toward valued ends such as longevity, care, or a sense of hope. In his later work, Bourdieu sought to destabilize the seemingly overstructured relationship between capital and agency by foregrounding time. Purposeful action in a social world not only presupposes possession of capital recognized by that world; it also requires individuals to develop a practical, often embodied, understanding of time—one that aligns with the timing, rhythms, and objective chances of that world—so that investment can be made at the right moment and toward a conceivable future (Atkinson 2019; Bourdieu 1990b, 1993, 2000; Strand and Lizardo 2017; Tavory and Eliasoph 2013). When people lose touch with institutional time altogether, as in mass unemployment or extreme poverty, they may find themselves “living at the mercy of what each day brings” (Bourdieu 2000:221). But what happens to people living in between—those who remain embedded in an institutional context but must act against its ruptured temporality?
Theorizing Temporal Misalignment
Contemporary scholarship has shown a renewed interest in understanding agency by charting the underlying temporal dynamics (Emirbayer and Mische 1998; Flaherty 2003; Hitlin and Elder 2007; Mische 2009; Tavory and Eliasoph 2013). Emirbayer and Mische’s (1998) seminal article conceptualizes agency as a process in which individuals, temporally embedded in the flow of time, engage with the social world by purposefully switching between iterating habits from the past, projecting possibilities into the future, and evaluating the demands and contingencies of the present. Tavory and Eliasoph (2013) further articulate theoretical tools for analyzing how individual actors coordinate their immediate, short-term, and long-term projections of the future to make sense of actions and interactions in the present (see also Mische 2009).
Meanwhile, empirical research has focused more on the unevenness of the temporal landscape we face as temporal actors. Time may be understood as a resource that some have more of and others have none (Abramson 2015; Burgard and Ailshire 2013; Cornwell, Gershuny, and Sullivan 2019; Gerstel and Clawson 2018; Offer and Schneider 2011; Perlow 1999; Schneider and Harknett 2019; Yu and Kuo 2022), or as an experience that some find fluid and customizable and others find sticky, pressed, racialized, and oppressive (Auyero 2012; Griffiths 2014; Mahadeo 2019; Sharma 2014; Wajcman 2016; Willis 1977). These theoretical and empirical advancements across multiple subfields highlight how individual agency can take the form of skillful steering and creative relationships within a heterogeneous temporal landscape, laying the groundwork for understanding unequal time not just as an effect, but as a cause of inequality in its own right.
Temporal misalignment, as both a concept and an object of study, helps further bridge this long-implied connection among time, agency, and inequality. Temporal misalignment occurs when there is a mismatch between the temporalities enacted by individuals in constructing purposeful action and the temporalities imposed by institutional contexts structuring when and how action is possible. No resource, for example, can be converted to institution-specific capital if the individual always makes the right move at the wrong time. Yet individuals with their own goals often cannot afford to fully subscribe to institutional time; nor can they entirely disengage with it when access to institutional means and resources is instrumental to viable action. Instead, actors have to reclaim a sense of agency and control over the experience of time by negotiating their temporal relationship with the institution. The need to manage temporal misalignment, by resynchronizing when it inhibits action and maintaining it when it facilitates action, motivates individuals to make decisions while also constraining which decisions they can make in solving the most imminent problems at hand.
With the concept of temporal misalignment, we build on prior theoretical work on temporal agency (Emirbayer and Mische 1998; Flaherty 2003; Tavory and Eliasoph 2013), but we further problematize how inequality is enacted and reshaped in individuals’ ruptured temporal relationship with institutions. For institutions, temporal misalignment is an important form of power, making certain actions more convenient or feasible, while cutting short, disrupting, delaying, or stretching others into a future longer than individuals can envision or wait. For example, enacting a state of emergency temporally bounds all policy responses to COVID-19 to the short term and delinks them from underlying mechanisms of inequality operating on a longer time scale (Decoteau 2024). In contrast, educational reforms and ideological campaigns in Malawi helped young village girls extend their imagined futures and sense of agency beyond the compressed timeline of marriage imposed by the institution of village life (Frye 2012).
For individuals, managing temporal misalignment requires more than cognitive effort. People often invest a wealth of capital, not to resolve misalignment, but to sustain their capacity to wait, keeping the windows open until institutional time aligns with their means and ends. These efforts can be so consuming they obscure or displace the original purpose. Cabdrivers, for example, frequently forgo earning opportunities in order to maintain a routine that aligns with the city’s rhythms (Serafin 2019). Even highly-paid technical contractors, in preserving the independence and flexibility of their work schedules, often end up working longer and less flexible hours to accommodate market cycles (Evans, Kunda, and Barley 2004). Through diverse individual efforts to synchronize or unsynchronize with institutional time, individuals sometimes exacerbate their own disadvantages, but they may also destabilize inequality.
The Case of Terminal Cancer
How does temporal misalignment shape inequality by shaping individual agency? Terminal cancer offers a revealing case where temporal misalignment, usually working in the background, receives heightened attention. Social scientists have long used biographical disruptions caused by chronic and incurable diseases to understand stratification in the life course (Bury 1982; Kerr et al. 2018; Maines 1983; Perry and Pescosolido 2012). Examining radically unsettled lives offers insights hidden during periods of stability (Swidler 1986, 2001). Medical sociology, in particular, offers sophisticated accounts of how structural inequality manifests through clinical interactions and as a fundamental cause of unequal access and unequal outcomes as people face radically shortened life spans, disrupted temporal experience, and practical challenges that expand beyond healthcare to family, work, and the very meaning of the future (Anspach 1997; Gengler 2020; Heimer and Staffen 1998; Link and Phelan 1995; Lutfey and Freese 2005; Shim 2010). Despite an emerging interest in the multiplicity of temporal order in the healthcare context, many excellent works either treat temporal misalignment as an organizational idiosyncrasy of the hospital as a total institution, or hint at the unequal experience of time without explicitly connecting it to patients’ relational agency in managing these experiences (Altomonte 2016, 2022; Bontemps 2025; Ihlebæk 2021; Kaufman 2006; Menchik 2014; Paust et al. 2023; Wang 2019; Whooley 2024). By reconceptualizing temporal misalignment in explicitly relational terms, this article helps generalize these important insights within and beyond medical sociology, to how we understand time and inequality in the discipline as a whole.
Terminal cancer in particular forces people to confront incommensurate temporalities: of existing work and family responsibilities, the symptoms and progression of disease, rigid schedules and transient options of treatment, timelines imposed by the healthcare industry, and the weight of life’s end. Consider someone just diagnosed with terminal cancer, like many in our study, who now seeks to convert whatever economic, cultural, and social capital they have into better chances at survival, or a better quality of life before options close at each stage of the disease. Yet the earliest available appointments may be months away. Insurance may erroneously deny pre-authorizations for a necessary CT scan, which could take weeks to appeal. Searching information online, seeking a second opinion offline, and recovering from the side effects of chemotherapy all require taking more time off work, which in turn jeopardizes one’s full-time employee status and insurance coverage. Even for people who have the resources and flexibility to find a way out of waiting, investments in better timing are not always effective. For some diseases, there are simply too few options at this moment in time; for others, a promising new drug may be a decade away from FDA approval, and no one knows for sure how much time they have left. Long before they reach the limits of their resources, time is a person’s first and foremost concern.
The case of terminal cancer allows us to zoom in on several ideal types of temporal misalignment, which can take many possible forms. Mische (2009) proposes nine cognitive dimensions along which individuals project and experience temporality as they construct future-oriented actions. Paust and colleagues (2023) identify schedules, sequences, agendas, efficiency, and pace as dimensions of unaligned time between patients’ temporal capital and healthcare organizations’ and professionals’ operating rhythms. In this article, we focus on three types of temporal misalignment that individuals seeking to activate their capital in a healthcare context most likely confront.
Schedule Conflict
One can only be in one place at a time. In the short term, capital-activating actions must be fit into the one and only schedule. Conflicting demands for slots on cancer patients’ schedules from cancer symptoms, everyday life, and unpredictable delays throughout the healthcare system could significantly disrupt the continuity of care and constrain patients’ agency. Individuals who work swing shifts, for example, frequently have difficulty complying with tight control over eating, exercising, and insulin injection schedules (Bury 1982; Lutfey and Freese 2005; Paust et al. 2023). Caregivers, too, have to shoulder the burden of unpredictable schedules and consistent interruption (Altomonte 2016). Even in organizational settings designed to maximize control over one’s time, such as neonatal intensive care units, parents who cannot accommodate the inflexible organizational schedules miss opportunities to be socialized into competent caregivers (Heimer and Staffen 1998) or to activate their cultural health capital in interactions with healthcare providers (Gengler 2020). The ability to prioritize or reschedule has become a prerequisite for contemporary actors to live at the intersection of multiple fields but “stay in every game” (Atkinson 2019). Terminal cancer patients have to invest their capital in negotiating schedule conflict between chemotherapies, surgeries, doctor visits, side effects, acute symptoms, and medical bills, as well as their work life and family life, before regaining a sense of agency to make decisions about their treatment.
Trajectory Mismatch
One also cannot put the cart before the horse. In the medium term, capital-activating actions must be situated in meaningful sequences of events (Mische 2009, 2014; Tavory and Eliasoph 2013). Post-acute care providers, for example, frequently try to align patients’ trajectories of recovery with those of insurance coverage to avoid potential financial burdens on both the organizations and the patients as a result of mismatch (Altomonte 2022). Compared to schedule conflicts, individuals often have more room to maneuver between multiple, coexisting, or sequential trajectories, rather than synchronizing or collapsing them all into one. Egg freezing, for example, helps women disentangle the trajectory of finding romantic partners from the trajectory of childrearing and reclaim a sense of agency over their life courses (Brown and Patrick 2018). In cancer care, insurance coverage, regulatory approval, and clinical trials are critical institutional resources that too often follow their own trajectories and lag behind individual trajectories of disease progression. An enormous research apparatus seems to offer unlimited options (Timmermans and Berg 2003), but for individuals, science makes uneven and unpredictable progress, and on a different timescale than how fast their bodies deteriorate, disrupting the treatment trajectories they have planned.
Anticipation Uncertainty
It is also hard to act when there is no future to act upon. In the long term, patients must hold onto a sense of certainty and a future worth investing in, to anchor their capital-activating actions in the present (Beckert 2013, 2016; Emirbayer and Mische 1998; Frye 2012; Mische 2009; Sendroiu, Álvarez-Benjumea, and Winter 2025; Tavory and Eliasoph 2013). Although anticipations tend to be more malleable and flexible than trajectories, patients whose ability to anticipate the future is severely constrained, or whose timeline for “what constituted the future was compressed” (Abramson 2015:79; Heimer and Staffen 1998; Livne 2021), could see the future as “something over which they have no control” (Atkinson 2013:654) and be reluctant to take responsibility and plan for long-term outcomes (Heimer and Staffen 1998:86). The ability to anticipate a future in which their children would be well, even one that is “packaged and sold in the modern healthcare system,” provides crucial motivations and scaffolding for parents of critically ill children to activate their cultural health capital (Gengler 2020:181). Prognosis, “a form of anticipation about disease, treatment, and the patient’s future life span” (Kaufman 2015:197), also sets the stage for not only the decisions patients have to make about their treatment, but also how physicians have to communicate in ways that are “responsive to the needs of the patient for hope” (Kaufman 2015:214). Terminal cancer brings significant uncertainty and anxiety, and patients often have to first rebuild their ability to anticipate a future that is compatible with what the institution can promise before any decisions can be made.
Data and Methods
So how do people from various social positions navigate the temporality of terminal cancer given the resources available to them? To answer this question, we draw on ethnographic data from the Patient Deliberation Study, a longitudinal field-based study of terminal cancer patients making decisions about their treatment plans in nine cancer clinics across two National Cancer Institute-designated, comprehensive cancer centers in the West Coast and Midwest of the United States (Abramson and Dohan 2015).
These academic cancer centers, specializing in providing cutting-edge treatment and clinical trials for patients with incurable, late-stage cancers who had exhausted or would soon exhaust standard therapies, offer a unique vantage point for examining how time, inequality, and agency interact. Patients treated at academic centers are, on average, more resourced than those in community-based settings, but we selected our sample to ensure heterogeneity in socioeconomic status, race, gender, age, and clinical profiles (Small and Calarco 2022). As nexuses of institutional resources and networks, these centers ensured that patients were exposed to a wide range of treatment options and their decision-making was not overdetermined by foreclosed access to care, which remains a first barrier, especially for patients in the most disadvantaged communities and outside urban areas (Link and Phelan 1995).
Data collection was conducted primarily between 2010 and 2015 by a team of five fieldworkers, including two of the authors. The team operated across both sites, with researchers rotating systematically between clinics to balance continuity for longitudinal follow-up with individual patients with opportunities to triangulate and identify any missed patterns or researcher effect. Researchers entered the field and presented themselves to both clinicians and patients as university-affiliated social scientists studying advanced illness and its organizational contexts. Researchers would introduce themselves to clinicians, patients, and family members, explain the purpose of the study, and obtain consent for the researcher’s presence. The fast pace of clinical interactions and the large size of clinical teams, including multiple physicians, trainees, and staff, in an academic setting, made the presence of an additional researcher in the room seem normal and less disruptive than in a community setting where patients interact with a single clinician.
A total of 306 complete field visits produced 4,860 paragraphs of field notes. Each visit lasted five hours, on average, and typically involved observing four to eight patients across clinical spaces as well as clinical staff in the backstage areas where clinicians met with their teams. The researchers also attended “tumor boards,” meetings where specialists, including oncologists, radiologists, and others, discussed complex cases. These field visits allowed us to observe directly how patients and providers negotiated scheduling, sequencing, and synchronization in real time, and situate interview accounts within the institutional and interactional contexts in which temporal misalignments emerged. Informal talks with providers and caregivers throughout the clinical settings also helped inform our interpretations.
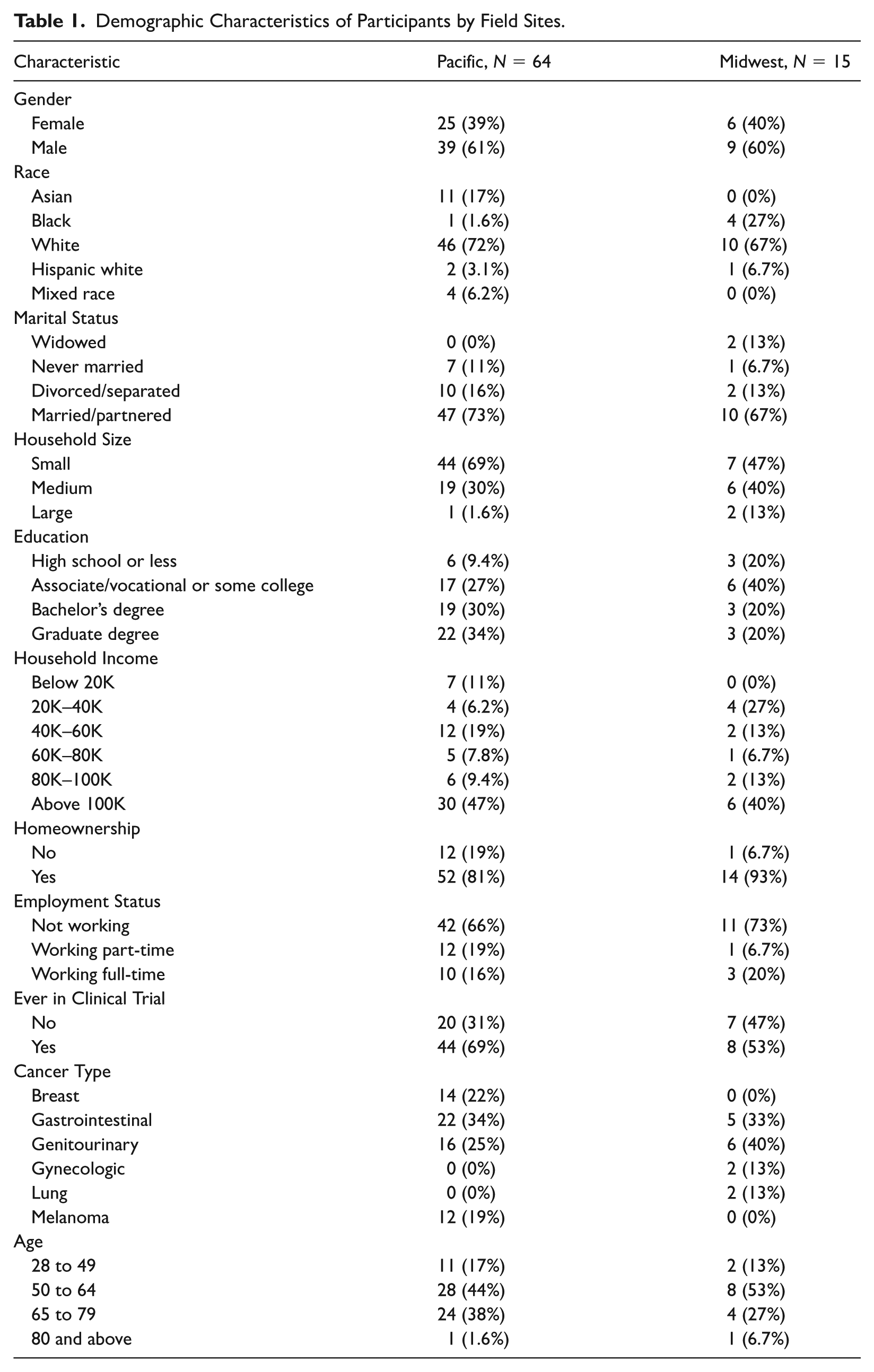
A total of 96 people with late-stage cancer, plus their 44 caregivers and 38 clinicians, were recruited for longitudinal follow-up interviews within our sample of clinics. Table 1 provides summary statistics on 79 participants who agreed to share demographic information on categories in this study. Patients who agreed to participate were observed and interviewed at different stages of disease progression, with their clinicians and caregivers also interviewed at least once. These interviews typically lasted 30 to 90 minutes and were held in clinical spaces, homes, or other settings, based on participant preference and comfort.
Demographic Characteristics of Participants by Field Sites.
The interview guide included modules on treatment decision-making, resources, experiences of illness, social networks, and life experiences, leaving room for emergent themes and observational notes from repeated encounters. Time was a common topic during interviews, and our ethnographic observation allowed us to identify temporal dilemmas as they emerged in situ during clinical interactions. For instance, patients referenced temporal dilemmas when they discussed logistical and financial challenges; support they received from family, friends, and healthcare providers; and decisions to seek aggressive treatment and clinical trials.
Interviews were professionally transcribed, and then coded by the research team together with fieldnotes using an iterative combination of deductive and inductive methods leveraging computer-assisted indexing in ATLAS.ti (Deterding and Waters 2021), compiled as a computational data frame and arranged for narrative and visual comparison (Abramson et al. 2018). Analytic memos and case summaries provide a holistic view of each participant’s trajectory through the study, situating individual experience within broader social inequality, in ways responsive to the ecological context (Cicourel 1982). Linking summaries and codes to underlying data connected more abstract interpretations to original text, prevented numeric reduction, and allowed evidence and explanation to coevolve over the course of the project (Sánchez-Jankowski and Abramson 2020; Tavory and Timmermans 2014).
Coding was conducted as a team, with a Krippendorff’s alpha of 0.80 maintained throughout the project via regular calibration and refinement. Project-wide, top-level domain codes included LOG (logistics), NET (networks), PER (patient perceptions), EVA (patient evaluations), PRF (patient preferences), PI (patient information), COM (communication), NAR (narratives), DEC (decision-making), EMO (emotions), and TRI (trials) with TMP (time and temporality) running across domains. This workflow produced a rigorously vetted corpus of coded text, anchored in longitudinal case comparisons, that allowed us to track how individuals navigated both the immediate demands of serious illness and the longer institutional timelines shaping their end-of-life trajectories. Part B of the online supplement provides a sample of coded data, a case summary template, and the interview guide. 1
We pair traditional qualitative methods with Multiple Correspondence Analysis (MCA) to further contextualize our interpretations of the data, connect levels of analysis, and map ethnographic findings onto observable resource distributions as a form of mixed-method analysis combining data types and analytic strategies (Small 2011). MCA translates complex statistical associations between cases and categories into geometric representations by clouds of points on a two-dimensional plane that allows for visually intuitive yet statistically precise interpretation (Breiger 2009; Greenacre 2007; Le Roux and Rouanet 2010). In the sociology of health and medicine, MCA has been used to map health-related inequalities and practices in a Bourdieusian social space (Burnett and Veenstra 2017; Gatrell, Popay, and Thomas 2004). For qualitative research, MCA offers a useful toolkit that leverages distributional information gathered about individuals during fieldwork to explore, present, summarize, and contextualize ethnographic evidence for transparency and triangulation (Murphy, Jerolmack, and Smith 2021; Sánchez-Jankowski 2002) alongside other approaches to validating qualitative patterns (Abramson et al. 2018; Abramson et al. 2024; Hanson and Theis 2024). MCA also helps researchers move beyond predetermined categories and allows groupings to emerge from empirical data and interact in ways not overdetermined by theoretical priors (see also Nelson 2020).
MCA helps us further adjudicate whether patterns of temporal misalignment are reducible to resource disparities within and between groups. We coded episodes of temporal misalignment observed during the interviews and used MCA to map the presence and absence of each type of temporal misalignment alongside demographic characteristics (gender, race, age, and cancer type), and indicators of economic (household income), cultural (level of education), and social (marital status and family size 2 ) capital. Our combination of ethnographic observations, semi-structured interviews, and statistical techniques provides a powerful vantage for understanding how terminal cancer patients navigate their disease, healthcare, and time.
Results
We found that temporal misalignment motivated and constrained individual agency for people across a variety of different backgrounds. Before resources could be activated or further action could be envisioned, participants and their care teams worked to realign patients’ plans of action not only with available resources but also with the temporalities of disease and healthcare institution. In other words, patients’ agency—whether seeking new treatment options or planning for continuity in everyday life—was predicated on their effort to triage conflicting demands of treatment, work, family, and bureaucratic schedules; reconcile mismatched trajectories of disease progression and healthcare institutions; and anchor uncertain decisions at present in an anticipatable future.
Schedule Conflict
For participants already at the clinics, it was often through their ability to accommodate treatment schedules, not the affordability of treatment options, that inequality became most evident. Few patients could afford the hefty price tags of cancer treatment out-of-pocket, so they also had to navigate bureaucratic schedules imposed by their insurance coverage as they converged with the schedules of the disease, treatment, and the demands of everyday life.
Treatment of advanced-staged, metastatic cancer typically involves regular monitoring, continuous medication, and in some cases draining and periodized procedures such as radiotherapy, immunotherapy, and chemotherapy. Many chemotherapeutic drugs, for example, are administered in repeating cycles of two to six weeks, with follow-up blood tests, CT scans, and appointments with oncologists to check for their effectiveness and unpredictable side effects. However, except for periods of hospitalization, where the hospital time takes over, other short-term priorities almost always demand spots on individuals’ schedules. Treatment preferences varied, but agency to pursue different options was unequal: participants’ ability to resolve conflicts between personal schedules and treatment plans shaped whether they could activate resources when opportunities arose.
Full-time, benefit-protected jobs gave many participants access to cutting-edge treatments at elite cancer clinics, but these patients often had to juggle work and family responsibilities in precarious ways—preserving their main sources of economic and social capital while facing treatment schedules that demanded rigid compliance. Bobby Vaughn [7073],
3
a 51-year-old house painter being treated at one of the top melanoma clinics thanks to his unionized job, constantly felt he did not have any choice in his treatment plan. Bobby had to work 32 hours per week to maintain full-time status, as required by his employment-based insurance. When asked why he passed on the opportunity to go to another cancer clinic his oncologist recommended as more promising for him medically, Bobby explained it was not even an option given how much conflict the commute would create with his family’s already loaded schedule: I mean, six hours, [versus] two hours. The only option was [this clinic]. . . . We have two sons, my wife works, I work. It just—for right now we’re just going to take our chances with [this clinic]. The [other clinic] is just going to throw our family in disarray.
Participants who were not more financially resourced, but were given better opportunities to negotiate treatment schedules, had a better chance of taking advantage of treatment options that became available and fit their goals of care. The following exchange between June Joseph [10008], a 48-year-old forklift driver diagnosed with pancreatic cancer, and her care team in the exam room illustrates how even a decision to continue chemotherapy is never just medical or economic, but temporal:
I can’t work with the pump.
No, I don’t think you can. And that’s a day of lost work. I know you have Fridays off.
I want to continue the treatment. Would I have [to spend] two hours here? I’d be home Saturday and Sunday with the pump.
So, it’s two days per month you’re going to miss. [to oncologist] She’s pretty much exhausted her benefits.
If we treated you today could you work?
No, not with the pump. . . . Can I take a week [off treatment] and then start [the next cycle]?
Yes.
We could hook you up on this day and have a nurse take it off on this day and play with your cycle a little bit.
Both June and her oncologist agreed it would be in her best interest to keep the infusion port implanted and start a new cycle of chemotherapy right away, but as June ran out of sick leave, the challenge became how to fit the new treatment cycle and subsequent side effects into her work schedule, rather than the other way around. In June’s case, the nurse, who had developed not only a close relationship with her but also an understanding of her temporal dilemma, was able to count the days she would have to miss, carefully calculate how many days she could delay chemotherapy, and help her negotiate schedule conflict with both the clinic and her employer, before she could act on what seemed like a straightforward decision. For most participants, schedule conflict was rarely a one-time thing they could maneuver out of, but a constant struggle to “play with the cycle,” which could accumulate into significant deviance from the intended treatment plan.
Conflict that arose from the inflexibility of treatment and work schedules was further intensified by systematic yet unpredictable temporal misalignment throughout the healthcare system. When bureaucratic delays at the hospital or insurance company struck participants with an already overloaded schedule, even a few days’ wait could extend into significant constraints on participants’ agency to act. During an appointment we observed with Aaliyah Jackson, a Black single mother taking care of her teenage son who had renal cancer, the oncologist asked if her son had started the new medication on time:
I had a problem. [Insurance company] said they had no record of me or him.
It all should have cleared.
Yes, but they said they did not have a record. This was in the middle of everything, he was having surgery, and they were saying we did not have insurance. It was a bad time. . . . They tell me [about the error] as he is about to go into surgery, and I [think] “how am I going to pay for the surgery?” I didn’t want to deal with this.
One framing might cast this predicament as a chronic lack of cultural health capital, but such a view risks discounting Aaliyah’s success in securing treatment for her son at a top cancer clinic, and obscures the temporal underpinnings of the problem. Hospital visits provided protected time for Aaliyah to consider treatment options, but the timing of the call from the insurance company—between an upcoming surgery and an already full schedule as work, life, and her son’s cancer converged in her everyday life—left her little room to respond to a new problem.
State-sponsored welfare programs not only incur wait times for eligibility verification and transition between jurisdictions, but they also impose categorical restrictions on patients’ everyday schedules. Nicolas Fields [4021], a 47-year-old musician on disability-based Medicaid, decided to move to another state so that his best friend, a nurse in pediatric oncology, could become his caretaker. He found out, however, that he had to reestablish his eligibility for Medicaid in the new state before he could continue his treatment. In the meantime, his disability-based eligibility for Medicaid effectively prevented him from working. As a result, to activate his social capital for better-quality care at home, he had to endure not only a lapse in treatment but also “many idle hours on my hands . . . hours of like trying to figure out what to do with myself,” a period he described as extremely stressful and mentally devastating.
Even for participants who could afford private insurance and had more control over their work schedules, living with rigid treatment regimens still brought significant constraints on their agency, as scheduling became increasingly resource-draining to reconcile with other aspects of life. Scheduling issues were especially challenging for individuals in high-paying professions like technology and finance, who relied on working long and flexible hours to maintain not only a high level of economic and social capital (Goldin 2021; Yu and Kuo 2022), but also an identity beyond being a cancer patient and a sense of agency not defined by the disease.
Peter Curtis [4040], a 71-year-old banker, at first liked to brag about how he enjoyed traveling between Hawaii and Colorado to get involved with deals and investments, cruising on his sailboat from time to time, while making himself available for any treatment opportunities anywhere for his pancreatic cancer: In fact, I’ve been flying back and forth from Hawaii coming over here to take [chemotherapy], then I fly back on Thursday, then I take this Friday and fly back Saturdays. . . . Yeah, I just decided I wasn’t going to let it interrupt the way I lead my life, other than I have to do this flying.
Even with all the resources and flexibility Peter had to prioritize quality of life, reconciling an increasingly demanding treatment schedule with quality of life outside the cancer clinic only became more and more difficult over time. Three months later, when we interviewed Peter again, he admitted: “finally I just thought this is too much traveling back and forth.” However hard Peter tried to prioritize quality of life, he eventually had to stay longer and longer at the clinic for radiation and checkups. As another participant Chris Mitchell [7036] explained, sooner or later, terminal cancer patients became “bound” to the hospital. In this way, schedule conflict exacerbated existing disadvantages for patients who were dependent on institutions that imposed their own rigid temporalities, and it created significant constraints on agency for actors who had flexible schedules and resources to spare.
Trajectory Mismatch
Even when participants were ready, and sometimes desperate, to activate their capital, treatment options might not align with the trajectories they had projected and hoped their investment would set in motion. We observed three intertwined forms of trajectory mismatch: (1) treatment options that participants saw as their last hope could take years to receive regulatory approval and become commercially available; (2) treatment options that were available as clinical trials could be gatekept by physician-researchers to prioritize collecting high-quality data and complying with study protocols; and (3) treatment options could require participants to maintain their capital beyond what the temporality of their terminally ill body would allow.
The extent to which participants could remedy this mismatch—between individual trajectories of disease progression and the institutional trajectories governing treatment availability—shaped their agency to activate capital and pursue the care they valued. Capital could be reliably activated only insofar as treatment options were available on the market or through clinical trials. Yet, science makes uneven progress across different types of cancer, and on a different timescale from individual trajectories of disease. Participants constantly juggled between the urgency to switch treatment as their current plans failed, and the stalling of progress when they needed it most. Although a terminal disease was, by definition, incurable, many participants were motivated to make up for such mismatch between institutional and individual trajectories by aggressively planning and searching for opportunities to bypass the institutional timeline and find next-in-line treatment that fit into the trajectories they had projected.
Celia Chang [7069], an Asian American software engineer who retired in her early 50s after being diagnosed with an aggressive type of breast cancer, decided that instead of waiting blindly for her next scan to tell her if the treatment worked or not, she should become an avid researcher and hope to get ahead of institutional trajectories. Celia and her partner, a biologist working in the biotech industry, read peer-reviewed journals and conference papers, and they crowd-sourced information on online forums. “This is my plan,” as Celia explained: I’m going to just get the information as much as I can, learn more, because I have another six weeks before I know whether this [is] working or not. If it doesn’t work, we have to switch. Maybe at that point I have to make—we can make some decision whether go for the trial or go do other, see what’s other options [there are].
Even for participants with ample and flexible cultural capital, being an active but amateur consumer of cutting-edge research and searching for “magic bullet” options for survival was a daunting effort. Phase 1 trials entail high risk of toxicity and low response rates (Chihara et al. 2022). Any next-in-line options participants did find had to remain accessible within the right time window for them to realize their planned treatment trajectories. Even when researchers made progress on their disease, regulatory approval and market rollout still ran their own course. A paper that showed promising results in killing cancer cells could take years to translate into an FDA-approved, commercially available drug—a wait few participants could afford.
Pat Agarwal [4022], an affluent, college-educated, professional middle-class immigrant, hoped that by activating his transnational networks, he could access alternative institutional trajectories outside of the United States: We sat down and my sister was here from India, and she has quite an influence in India. She knows a lot of people and they are pretty well off and they know people. And like there is a big institute in Mumbai and lots of people from U.S. and Western countries, they go over there for surgeries when they cannot do it right here.
One year later, after mobilizing extended family for an extensive search, Pat still had not found a viable treatment option that could get him out of waiting, and he eventually became too ill to travel. The family pushed for more aggressive treatment at local clinics, hoping that new options would become available, but none did by the time Pat entered hospice.
Clinical trials, which participants desperately looked for, follow a very different trajectory that rarely matches that of individual disease progression. Despite being widely advertised and understood as treatment opportunities for terminal cancer patients, clinical trials are designed to produce evidence about potential treatment tomorrow, not net benefits for every participant (Fisher 2008; Kaufman 2015; Keating and Cambrosio 2012; Nurgat et al. 2005). Participants were locked in a race against the disease and counted on their physicians to secure spots in trials, but physician-researchers had to screen out patients who were not best candidates for securing funding and results. As a physician explained in a meeting we observed, having to consider too many patients for limited spots in a clinical trial could jeopardize the timeline of the entire research. Eligibility criteria had to be set carefully to screen out more patients and avoid delays: “We need some kind of screening mechanism because a lot of people come to us for the study but it would behoove us to get that test done because so many patients are not eligible.”
For participants, the stakes were even higher: life itself. Failing to meet the screening criteria for one trial could mean missing the recruitment window for another; rushing to enroll in one trial could disqualify a person from better trials that were coming up. One participant paid $18,000 out-of-pocket for additional diagnostic tests to establish eligibility for enrollment in a clinical trial, only to eventually be determined ineligible. In the end, no amount of capital could guarantee finding one’s way into clinical trials and out of institutional trajectories.
Not all forms of capital were as effective in managing trajectory mismatch as cancer patients expected from navigating other parts of the healthcare institution. Depending on who set the plans and timelines of clinical trials in the organizational context, participants might find their localized knowledge and networks more transposable than economic and cultural capital when it came to jumping institutional waiting lines. The experience of Meghan O’Brien [7029], who had widely metastatic omentum cancer, illustrates how getting access to the trajectory-setting backstage of local healthcare organizations could be more effective: I actually went to Dr. Knowles for a second opinion [be]cause I’ve worked [in the same hospital system] for 30 years. . . . Dr. Knowles happened to have a clinical trial that he was opening that would give me the same chemo as they would’ve given me over here, which he agreed would be the second line to try.
Meghan’s cultural health capital as a nurse-turned-patient did put her in an advantaged position in clinical interactions. However, it was the combination with local, personal ties she had developed working for the hospital, an often less transposable form of social capital that Small (2009) terms “organizational embeddedness,” that allowed her to connect with a former colleague overseeing local institutional trajectories and eventually fast-track access to clinical trials when she needed to switch treatment.
The struggle to manage this fundamental mismatch between the trajectories of treatment and research might also be compounded by a third form of mismatch—between the trajectory of disease progression and the need to maintain economic capital beyond what people’s bodies would allow. Because eligibility for insurance coverage remained tied to full-time employment, many participants had to navigate the conflict between their trajectories as patients facing disease progression and deteriorating health, and trajectories as employees having to sustain full-time status. Participants who were initially able to work often lost full-time employment sooner than the institution had assumed, making underprepared transitions to unemployment, disability, or retirement insurance, disrupting treatment trajectories they had planned for but few could afford out-of-pocket. Some participants described spending as much time researching new coverage and overcoming new bureaucratic obstacles as they did researching actual treatment options.
The timing of these transitions as a result of trajectory mismatch led to diverging strategies even when resources seemed comparable to start, as demonstrated by a comparison between Bobby Vaughn [7073] and Julia Kim [7037]. Like Bobby the housepainter, Julia enjoyed secure employment and good health benefits working for a multinational retailer. But unlike Bobby, who was able to maintain full-time employment, Julia lost her ability to work soon after her cancer progressed, and she had to invest economic, social, and cultural capital in navigating an unwanted transition to disability and bureaucratic hurdles that came with the new status: My treatment is being paid [now] because I was able to go on retirement. . . . I was afraid I was going to go into a transition [from full-time to disability] where I have to pay COBRA, which is like five or six hundred dollars a month. And then my cousin says, “You know, why don’t you try and see if you can get early retirement?” . . . I just turned 55. I read on it and I called and sure enough, I could. But then I found out after four or five months . . . [when] I got all my bills and there’s a difference. . . . A lot of the copay. If I have procedures done, you know, intervention radiology, I’m still liable for 25 percent of it. And by the end of May, it was like $2,000 that I had to shell out.
Many participants had a reliable source of insurance coverage, but for Julia, insurance became a constraint on her agency to make treatment plans. Unexpected disease progression toppled not only her ability to work, but also her existing treatment plan predicated on stable, matching insurance coverage. Julia had to divert time and resources to re-create treatment plans that would match the new coverage. In other words, much capital was invested, not to strategize for the best available care, but simply to catch up with institutional trajectories to make treatment possible.
Anticipation Uncertainty
Taking action in the short and medium terms requires individuals to have calculable, or at least conceivable, futures. Yet, as the disease threw participants into extraordinary anxiety about both the length and quality of their time left, the institution offered limited certainty. On the one hand, the extent to which the future was anticipatable to participants depended on the uneven institutional trajectories and unpredictable future of cancer research. On the other hand, even for participants with types of cancer for which more treatment options were available, or significant progress was being made, the institution’s promise of a cure in the near future did not automatically translate into an anticipatable future, as “individualized prognoses about the timing of death [were] difficult if not impossible to pin down” (Kaufman 2015:196). As a result, when participants still had resources to invest toward the later stages of disease, they often invested in anchoring their present decisions in futures imagined but not necessarily realized by the institution.
A number of participants, especially those with economic and cultural capital, who sought the remote prospect of remission for an incurable cancer indicated they were not necessarily looking for immediate medical benefits, but to regain a sense of certainty about the future and thereby agency in the present. Alan Day [7528], a 66-year-old business owner, despite not finding a feasible option or having a concrete plan, continued to aggressively search for clinical trials and discuss with his oncologist every remotely relevant study he found online: “[T]he idea of doing trials, in the sense of the long-term benefit is appealing so it’s worth a little extra effort just in that sense. Plus, maybe it’ll help me. Who knows?” By searching for information that had no immediate benefit, resourced participants like Alan invested their cultural and social capital in a sense of connection to future breakthroughs in medicine, which in turn anchored and motivated their continued investment in present treatment.
Participants who had limited resources to spare often could not afford to manage uncertainty about the future. Many relied on their oncologists, who were incentivized by the institution to recruit and retain patients, for a tangible, imagined future in which clinical trials were framed as waiting for a new drug that could put their cancer into remission. An exchange we observed between an oncologist and a patient with prostate cancer not responding to the current treatment provides an illustration. Asked about the lack of remaining treatment options moving forward, the oncologist appeared to sense frustration in the patient’s question and reassured him that continuing treatment could open more options soon: We have another option with a medication that doesn’t even have a name yet. . . . It’s in the process for FDA approval now. By the time you have done 10 cycles, you’ll likely be able to [switch to] this in 20xx. . . . From the beginning of time until 20xx, there were only a handful of treatments available. After 20xx, there were a lot more tools to help us not just buy time but put the disease into remission.
In reality, most drugs fail at this stage of development (Sun et al. 2022). Yet, by repackaging an experimental treatment of ambiguous medical value and indeterminate timeline into a concrete relationship to a remote yet seemingly certain breakthrough in science, the oncologist successfully shifted the anchor of the participant’s decision: away from the grim trajectory of disease progression and the risk of over-treatment, toward continued treatment and engagement in clinical trials as providing a sense of agency.
Even in cases where participants have made peace with their own futures, anticipation uncertainty can take alternative forms that extend beyond the patient’s own life course. Researchers estimate that 5 to 10 percent of all cancers are hereditary (Garber and Offit 2005; Jahn et al. 2022). As a result, a cancer diagnosis can trigger concerns about the cancer “running in the family” or a more general elevated risk for the next generation. Lorena Benjamin [7064], a young mother diagnosed with a rare, highly metastatic type of melanoma, described anxiety over her two daughters’ future as her motivation to search aggressively for clinical trials: So if it raises my daughters’ risk of getting a melanoma and if there [was] melanoma and if there was actually like a gene linkage between melanoma and breast cancer, I mean, I’m not thinking about it [for] me but I’m thinking about it for the fact that I’ve got a 21-year-old and a 16-year-old. I would want to know what are the best options for my girls. And that’s probably, I would say, the number one reason for me picking a clinical trial.
For Lorena, the hereditary risk of her cancer presents a unique dilemma: her participation in clinical trials, while helping develop targeted therapies that had significantly improved survival rates in melanoma, did not necessarily offer immediate benefit for herself. However, by anchoring her decisions in the anticipated cancer risk in her daughters’ future, Lorena gained a sense of agency despite her limited resources and dire prognosis. In other words, for capital-activating decisions to feel meaningful and worthwhile even under profound uncertainty about one’s own future, participants learned various ways, not necessarily altruistic, to build a relationship with a more anticipatable future.
Relationships between Temporal Dilemmas and Resource Disparities
Now that we have shown how schedule conflict, trajectory mismatch, and anticipation uncertainty played important roles in the lives of individuals managing a terminal disease, we can connect these ethnographic findings to unequal resources among our participants. Were the patterns of temporal misalignment we observed reducible to the unequal distribution of resources, or is temporal misalignment something more than another dimension where fundamental causes play out?
Our analysis was suggestive of some associations between individual efforts to manage different forms of temporal misalignment and disparities in economic, cultural, and social capital, but multiple correspondence analysis (MCA) helps us situate our findings about time more precisely in the distribution of resources among all our participants. If patterns of temporal misalignment could be adequately explained by resource disparities, we would expect temporal misalignment to explain an insignificant amount of variation where resource disparities are present in the MCA space.
The MCA results show a more nuanced picture where resource disparities and temporal misalignment appear to be distinct dimensions of variation among our participants. Figure 1 visualizes the associations between participants (in number IDs), demographic and socioeconomic variables, and the presence and absence of temporal misalignment in our data. Along the horizontal axis (Dim 1), participants are most distinguishable by indicators of their economic (household income), cultural (level of education), and social (marital status and family size) capital, and the presence of anticipation uncertainty. Along the vertical axis and weakly associated with most variance in economic and cultural capital (Dim 2), participants are most distinguished by employment status, family size, and the presence of schedule conflict and trajectory mismatch. In other words, while the presence of anticipation uncertainty is more strongly associated with markers of resource disparities, schedule conflict and trajectory mismatch appear to contribute significantly to a distinct dimension of inequality, not only independently of Dim 1 where resource disparities are most significant but also weakly associated with most other demographic variables. We also considered whether temporal misalignment might be associated with age and cancer types, but we found that only the youngest age group (28 to 49) was marginally associated with the first three dimensions. Part A of the online supplement presents these results in more detail.
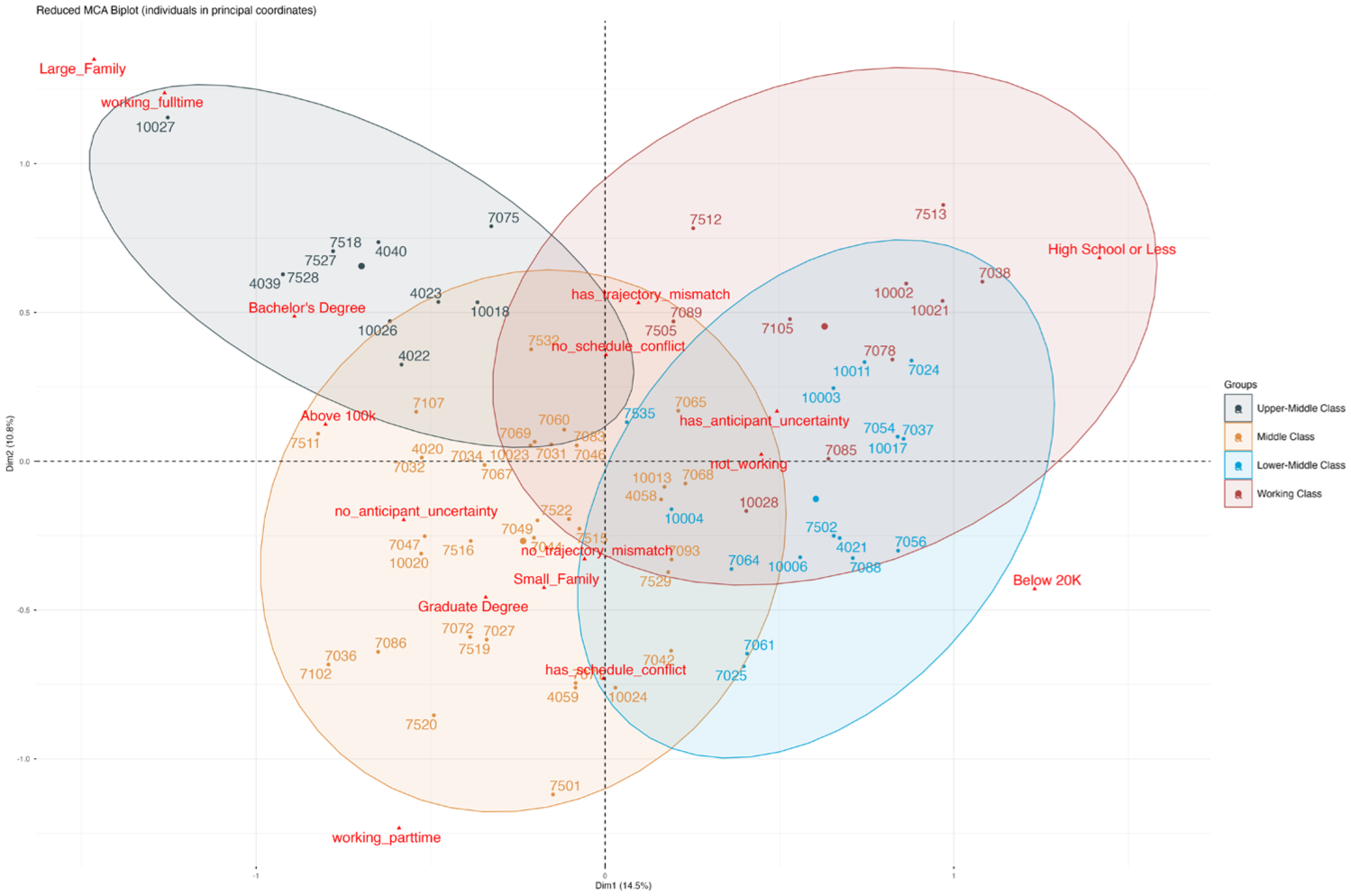
Reduced Multiple Correspondence Analysis Biplot of Associations between Individuals, Selected Demographic Variables, and the Presence of Temporal Misalignment in Their Accounts (n = 79).
A hierarchical clustering of the MCA space further validates how we grouped our participants in qualitative analysis. First, on the top left of Figure 1 are upper-middle-class participants high on economic, cultural, and social capital, like Peter [4040] and Pat [4022]. These participants occupied the top income bracket, enjoyed the most support from family members and social networks, continued to work full-time with substantial financial and temporal flexibility, and were less likely to experience schedule conflict or anticipation uncertainty. However, they often invested considerably in outrunning institutional trajectories and searching for nonstandard treatment options. On the bottom left are the majority of middle-class white and Asian patients who, like Chris [7036] and Celia [7069], had the economic and cultural capital to stay on top of the latest research and treatment options and remain positive about their future. Yet, working as professionals and living with smaller families, they did not have as much flexibility with their schedules. To reconcile schedule conflict, they often had to reduce to working part-time as their disease progressed.
On the right of Figure 1 are working- and lower-middle-class participants low on economic and cultural capital, who were also most likely to be Black women, without college education, and in the lowest income brackets. These participants struggled the most to anticipate what their future would look like with cancer. Positioned on the bottom right, participants who worked full-time jobs in manufacturing and service were more likely to struggle in the short term to balance work and family responsibilities, and they were more likely to encounter bureaucratic delays in trying to maintain their insurance coverage. Positioned on the top right, participants who worked in precarious jobs, did not go to college, and often had to stop working altogether soon after the diagnosis, were more likely to confront trajectory mismatch that disrupted their agency to manage treatment options and welfare benefits, and that they, unlike the more resource-rich patients, could not buy their way out of.
While reflecting accurately the slightly uneven but still diverse distribution of participant characteristics among those we observed in these clinics, the patterns are both consistent with our qualitative findings and provide added support that temporal misalignment is a distinct mechanism that extends resource-centric theories and connects the diverse temporal experiences of terminal cancer patients we met. Specifically, while disparities in economic and cultural capital along the horizontal axis may be significant factors in shaping anticipation uncertainty, participants’ efforts to manage schedule conflict and trajectory mismatch between the disease, one’s personal life, and the healthcare institution are independent drivers of inequality that cannot be reduced to unequal resources.
Discussion
To summarize, we examined the connections between time, agency, and inequality through the case of terminal cancer patients. Integrating ethnographic observations, in-depth interviews, and multiple correspondence analysis, we developed a temporal-relational account of how people experience their agency in stratified ways, not only through their resources, but also through how these resources are motivated and constrained by temporal misalignment between individual action and the institutional context in which they are embedded. We identified three types of temporal misalignment—schedule conflict, trajectory mismatch, and anticipation uncertainty—which best illustrate how inequality arises dynamically and relationally from our patients’ efforts to manage temporal misalignment. Our findings have implications for future sociological research on inequality, time, culture, health, and end of life, as well as for understanding cancer experiences and diagnosis that will affect one in two Americans in their lifetime and become increasingly consequential for society as a whole.
Table 2 summarizes our key empirical findings. On the one hand, a robust form of inequality arises from patients’ struggles with temporal misalignment, which constrained agency to activate capitals for the care they desired. Schedule conflict and trajectory mismatch between treatment, work, family, and insurance coverage often resulted in extended waits for diagnosis and treatment, delays in making treatment decisions, and missed opportunities to take advantage of therapeutic options. The necessity of triaging conflicting demands for spots on their schedules and navigating treatment and insurance disruptions after disease progression locked individuals with the fewest resources into a constant struggle with short-term unpredictability of local institutional contexts, which in turn limited their ability to anticipate and invest in a conceivable future.
The Pragmatic Dilemmas and Stratifying Consequences of Temporal Misalignment That Participants Most Likely Confront in Maintaining and Activating Their Resources.
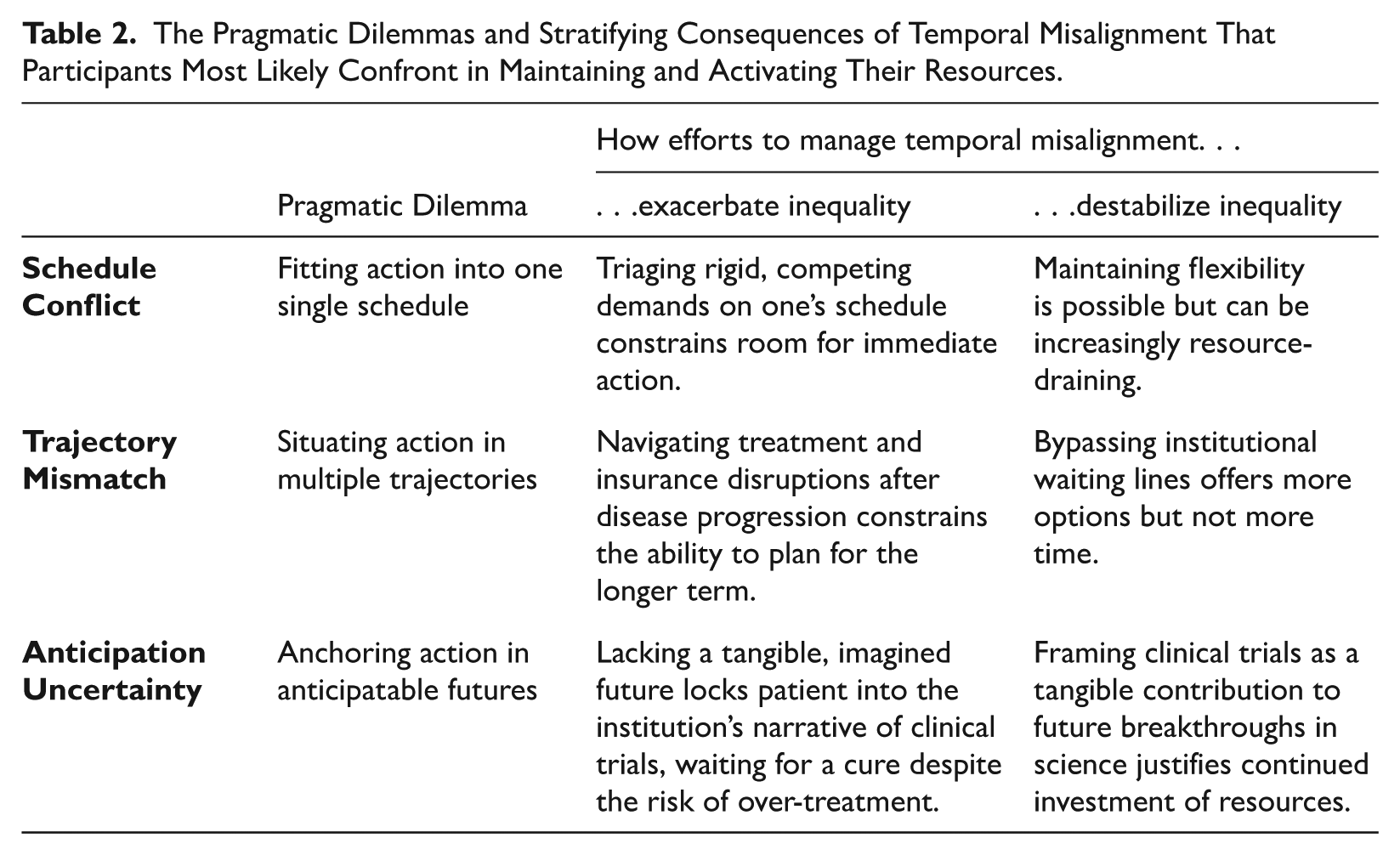
On the other hand, even well-resourced patients, who were most able to use wealth to minimize schedule mismatches, still struggled to manage temporal misalignment in the longer term. Many drained their economic, social, and cultural capital to bypass institutional waiting lines. Only some were able to restore a sense of certainty after aggressively searching for experimental and sometimes non-FDA-approved treatment and accessing early-stage clinical trials in the organizational backstage. While their investment did seem to offer a sense of certainty, if not optimism, about the future, the institutional trajectory of biomedical research almost always lags behind the individual trajectory of disease progression. In the end, many treatments pursued had uncertain, ambivalent, or even negative physiological consequences. Often, having resources to invest only stretches the time windows just enough so patients can keep investing, sometimes in the hope of a broader shift in possibilities, and sometimes as a form of maintaining a sense of continuity from earlier in life.
Implications for Research on Inequality
Our account has implications for understanding inequality, not just in the arena of serious and chronic illness, but in relation to agency, resources, and institutions more broadly. Our findings highlight the central role of time, not only as a resource unequally distributed in existing inequalities, but also as a family of mechanisms that connect individual agency to institutional contexts in shaping when and how resources can be used. On the one hand, institutions create a dynamic form of inequality by maintaining institutional order through imposing temporalities at the cost of individual agency. On the other hand, individuals experience these inequalities acutely in their efforts to manage their temporal relationship with institutional contexts and reclaim a sense of agency in navigating institutional resources and opportunities. Explanations of inequality that do not account for temporal entanglement between resources, agency, and institutional context may over-simplify the relational, dynamic, and temporally mediated nature of inequality, especially in such complex and time-sensitive cases as healthcare.
Cancer funnels individuals into an institutional context that foregrounds temporal dilemmas in a way that mirrors many other milieus of temporal instability. Immigration, for example, can impose decades of waiting in visa queues, court backlogs, and even detention centers for an arbitrary adjudication on one’s legal status and possible futures (Cwerner 2001; Fee 2022; Griffiths 2014; Parreñas 2021). Eviction, too, can perpetuate trajectory mismatch between stagnant wages and welfare payouts, rising housing costs, and a rigid payment schedule that poor tenants in low-income neighborhoods have few ways to reconcile (Desmond 2012). The disruption that COVID-19 created also had a temporal aspect: working mothers disproportionately shouldered the responsibility to resolve conflicts between work-from-home and school-at-home schedules (Augustine and Prickett 2022; Collins et al. 2021), small businesses disproportionately struggled with mismatch between business cycles and lockdown cycles (Bartik et al. 2020), and our expectations for a return to normalcy in the near future constantly clashed with the fear of prolonged restrictions.
In a stronger sense, temporal misalignment contributes to inequality even without the magnifying effect of biographical disruption. Consider education. The distinction Lareau (2003) observed between the “natural growth” of working-class children and the “concerted cultivation” of middle-class children hinges not only on disparities in economic and cultural capital, but also on different temporal dilemmas that parents have to manage. For white middle-class parents, prescheduled activities create a highly predictable schedule that matches their own, but their perfect plans may still be toppled by last-minute school closure due to bad weather. On the other hand, working-class, and especially racial minority, parents who have to routinely triage immediate, unexpected demands for their time (often from surveilling institutions) to get the family through the day, simply cannot afford to micro-manage their children’s free time. Or consider queer time. Queer people bear the additional burden of articulating and managing temporal misalignment as many institutions of modern capitalism are predicated on its subjects assuming a stake in a reproductive future (Edelman 2004).
In these ways, the temporal approach to inequality we advance in this article has potential to bring together a diverse range of cases to help us better understand intersectional inequality. As methodological advances allow sociologists to leverage the increasing availability of large-scale time-use and time-stamped behavioral data (Cornwell et al. 2019; Golder and Macy 2014), as well as computational approaches for measuring temporal expressions in text data (Stuhler, Tavory, and Wagner-Pacifici 2026), future research will benefit from more explicitly theorizing these dynamic, fine-grained, and intersectional temporal mechanisms of inequality.
Implications for Understanding Time Sociologically
Our study also shows the value in integrating work on inequality while continuing to articulate time as a sociological concept. Building on a fast-growing literature on temporality and agency (Atkinson 2019; Emirbayer and Mische 1998; Hitlin and Elder 2007; Tavory and Eliasoph 2013), our analysis reaffirms the utility of both theorizing time explicitly and measuring time with nuance. Following scholars such as Brown and Patrick (2018), we call for more studies that use the relational nature of time to link the concept of agency to the lived experience of inequality. We also further extend the scope of a temporal approach by offering a cross-section of how temporal misalignment not only affects individuals from diverse social backgrounds but also crosscuts institutional domains such as healthcare, workplaces, and the welfare state.
Building on foundational work by Emirbayer and Mische (1998), Tavory and Eliasoph (2013), and Atkinson (2019), we show how elements of Bourdieu’s theory serve as a fruitful starting point for moving beyond situations to institutions. Explaining how participants in our study managed the everyday and existential challenges they faced requires understanding how cancer patients’ temporal dilemmas not only delimit possible outcomes but also exacerbate resource disparities and influence their decisions to activate some form of capital. While this article draws selectively on Bourdieu’s concept of capital as used in medical sociology, a robust model of understanding temporality in institutional contexts is central to his widely used theory of fields and habitus and should interest scholars across subfields. Future research might continue to explore the underappreciated relevance of the sociology of time to our discipline’s longstanding interests in connecting levels of analysis between individuals and institutions, biography and history, as well as culture and structure.
Implications for Cultural Sociology
A longstanding debate in cultural sociology concerns how to reconcile institutional orders and individual agency as conflicting sources of action (Emirbayer and Mische 1998; Sewell 1992; Swidler 1986). On the one hand, institutions appear to impose obdurate and internally coherent logics of intertwined practices and meanings (DiMaggio and Powell 1983; Meyer and Rowan 1977). On the other hand, we rarely subscribe to institutional logics in their entirety (Hallett 2010), but draw on cultural and organizational resources to resist, negotiate, inhabit, and reengineer institutions (Hallett 2010; Swidler 1986, 2001; Zietsma and Lawrence 2010). Empirical applications of these models, while incorporating agency into sociological explanations, have been criticized for reducing decision-making to the mechanistic response of cultural dopes enacting existing scripts, or the overgeneralized agency of abstract agents pursuing the same objectives. In reality, the ways individuals experience, confront, and embed their agency in institutional contexts are diverse, dynamic, and multidimensional.
In our case, we zoom in on how time gives the healthcare institution a tangible and actionable form in patients’ decision-making experiences. The healthcare institution appears to terminal cancer patients as neither dogmas nor scripts, but practical challenges grounded in ruptured temporal relationships to which they devise diverse and specific responses. These responses do not rely on the prophetic visions or tautological purposes of the institution, but are motivated by a pragmatic disposition to make sense of one’s temporal experience while maximizing one’s room for future action against any temporal constraints. The power of institutions, in turn, may also manifest in their use of time as a means of control and discipline over individual action. Our focus on time not only offers a useful vantage point that connects agency to inequality, but it also lays groundwork toward a theory of action that will benefit from more large-scale, time-use, and time-stamped data.
Implications for Medical Sociology and Health Policy
Our findings show how time is an essential ingredient of both inequality and policies that address inequality in the arenas of health and medicine. Access to resources and treatments remains a necessary condition of more effective and equitable healthcare, yet it is far from sufficient. To be sure, very few people can afford to pay for chemotherapy out-of-pocket, and diagnoses for complex conditions, ranging from cancer to Alzheimer’s disease, are rarely straightforward. On top of this reality, time is rarely in the favor of those who face progressing challenges at the intersection of health and society. Our healthcare system’s intricate and marketized temporalities of scheduling, billing, insurance coverage, and clinical trials often introduce more misalignment than individuals can manage, and prevent people from converting resources into effective action. The Patient Protection and Affordable Care Act, for example, while effectively narrowing inequality in insurance coverage (Gutierrez 2018), does not automatically translate into health equity without individual efforts to fit oneself into misaligned temporalities between healthcare organizations and the welfare state (Altomonte 2022).
Likewise, the tensions between under- and over-regulation, often adjudicated politically rather than through evidence-based policymaking, only expand temporal constraints on patient-physician collaborations that have proven effective in combating many diseases (Epstein 1995; Eyal 2013; Marcus 2023). A deeper sociological understanding of how people manage temporal misalignment embedded in their relationships with healthcare institutions and over the course of a disease can provide a more accurate picture of the effectiveness of resource provision and facilitate the incorporation of time into the making of policy interventions.
Supplemental Material
sj-pdf-1-asr-10.1177_00031224261448220 – Supplemental material for Temporal Misalignment and Unequal Agency: What Terminal Cancer Patients Teach Us about Time and Inequality
Supplemental material, sj-pdf-1-asr-10.1177_00031224261448220 for Temporal Misalignment and Unequal Agency: What Terminal Cancer Patients Teach Us about Time and Inequality by Zhuofan Li, Daniel Dohan and Corey M. Abramson in American Sociological Review
Footnotes
Acknowledgements
We would like to first thank the people who participated in this research. We are also grateful to those who provided feedback that greatly improved the manuscript, including Ron Breiger, Ann Swidler, Martín Sánchez-Jankowski, Laura Halcomb, and Peter Ore, as well as the ASR editors and five reviewers. We thank the members of the Medical Cultures Lab at the University of California San Francisco, the New Mixed Methods+ Working Group at the University of Arizona, and the Computational Ethnography Lab at Rice University, as well as participants of the “Culture in Unsettled Times” panel at ASA 2022 for feedback and support. We thank Sarah Garrett, Alma Hernandez, and Melissa Ma for their work on the broader project.
Funding
This research was supported in part by National Institutes of Health (NCI/NIH) awards R01CA152195 (PI: Dohan) and DP1AG069809 (PI: Dohan, Co-I: Abramson), and a Research, Discover, and Innovation Faculty Seed Grant from the University of Arizona (PI: Abramson). The content and views expressed are those of the authors and not of NIH or other funders.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.