
Abstract
Laparoscopic common bile duct exploration (LCBDE) has been recently introduced for management of CBD stone in patients with previous biliary surgery history. The aim of this study was to evaluate the safety and effectiveness of primary closure in patients with previous biliary surgery history compared to T-tube drainage. Eighty patients with previous biliary surgery history including laparoscopic cholecystectomy, open cholecystectomy, or open common bile duct exploration were enrolled in the retrospective study. The patients were divided into 2 groups according to the methods of choledochotomy closure. Group A: patients with primary closure after LCBDE (n = 51); group B: patients with T-tube drainage after LCBDE (n = 29). Group A exhibited a shorter postoperative hospital stay and lower hospitalization expenses compared to group B. There was no significant difference in conversion rate to open surgery, operating time, intraoperative blood loss, bile leakage rate, overall complication rate, and stone recurrence rate between the 2 groups. Biliary stricture was not observed in the 2 groups during the follow-up period. Primary closure following LCBDE is safe and effective for the management of CBD stones in patients with previous biliary surgery history.
Introduction
The development of common bile duct (CBD) stones after cholecystectomy or choledochotomy remains a troublesome problem. The incidence of CBD stone development is approximately 2%-5% after open and laparoscopic cholecystectomy 1 and 5%-15% after common bile duct exploration. 2 With the advance of laparoscopic techniques, laparoscopic common bile duct exploration (LCBDE) has been introduced for the treatment of CBD stone in patients with previous biliary surgery history. 3
T-tube drainage of CBD after laparoscopic choledochotomy is performed traditionally to prevent biliary complications including biliary leakage and stricture. Recently, several comparative studies have demonstrated that primary closure is at least as effective and feasible as T-tube drainage4-6 in emergency setting 7 and elderly patients. 8 However, it remains unclear whether or not to perform primary closure following LCBDE in patients with previous biliary surgery. Previous biliary surgery induces severe adhesion around hepatoduodenal ligament, which may hinder the identification of CBD, choledochotomy, and choledochotomy closure. The safety and feasibility of primary closure following LCBDE in patients with previous biliary surgery remain unelucidated. The aim of the study was to compare the safety and efficacy of primary closure following LCBDE with T-tube drainage in this particular group of patients.
Methods
Patients Selection and Grouping
Patients with previous biliary surgery history who received LCBDE from 2013 to 2018 were included in this study. The indications for LCBDE were as follows: (1) CBD stones are confirmed by preoperative abdominal ultrasonography or magnetic resonance cholangiopancreatography (MRCP) with no intrahepatic bile duct stone; (2) the diameter of CBD is more than 0.8 cm; (3) severe inflammation (acute suppurative cholangitis, acute necrotizing pancreatitis) at the porta hepatis is absent; (4) distal common bile duct obstruction is not observed.
This study was approved by the Institutional Review Board of The First Affiliated Hospital of Nanchang University. After we explained the advantages, disadvantages, and possible complications to the patients, the patients made their decisions to receive either primary closure or T-tube drainage. Patients also gave written informed consents for the operation and for their data to be used for research purposes. The demographic characteristics, perioperative outcomes, complications, and follow-up data were recorded and compared between the 2 groups.
LCBDE Procedure
After general anesthesia, the patient was placed in a supine position with both legs apart. Pneumoperitoneum was established with CO2 insufflation after a Veress needle was punctured through a 10-mm infra-umbilical skin incision. The infra-umbilical skin incision site should be more than 3 cm far from the previous surgical incision scar. Otherwise, Hasson technique was applied instead. Four laparoscopic ports were used: a 10-mm infra-umbilical port for laparoscope, a 12-mm main operative port in subxiphoid, and two 5-mm auxiliary operative ports in the right upper quadrant. Abdominal adhesions, especially adhesions formed around hepatoduodenal ligament, were dissected carefully using the Harmonic scalpel (Ethicon, USA). The anterior wall of CBD was exposed and incised longitudinally for 1.0-1.5 cm. Through the 5-mm flexible choledochoscope (Olympus, Tokyo, Japan), CBD stones were identified and removed by saline irrigation, Dormia basket (Cook, Bloomington, IN) extraction, or electrohydraulic lithotripsy. After all stones were retrieved, clearance of the proximal and distal bile duct was repeatedly confirmed by choledochoscopy. Intraoperative cholangiography was not performed.
After complete clearance of CBD stones, the choledochotomy site was primarily closed with 4-0 Vicryl interrupted suture or 4-0 Stratafix Spiral PDO (Ethicon) continuous suture in group A. For patients in group B, a T-tube of appropriate size (16-20 Fr) was inserted into the CBD incision site and choledochotomy was closed with 4-0 Vicryl interrupted suture. A cholangiography was performed on the 5th postoperative day. If there was no residual stone, the patients were discharged with T-tube in situ and the T-tube was removed 4 weeks later.
Follow-Up
Routine physical examination, liver function test, and abdominal ultrasound were performed at outpatient clinics. Further MRCP or abdominal computed tomography (CT) was required when indicated.
Statistical Analysis
The quantitative variables were expressed as mean ± standard deviation and compared by Student’s t test. χ2 test or Fisher exact test were performed for categorical variables. A level of P < .05 was considered statistically significant. Data analysis was performed using SPSS 17.0 software (SPSS Inc., Chicago, IL, USA).
Results
Eighty patients with previous biliary surgery history underwent LCBDE from January 2013 to January 2018 at our institution. The patients were divided into 2 groups: primary closure group (group A, n = 51) and T-tube drainage group (group B, n = 29). Patient characteristics are presented in Table 1. There was no significant difference in age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) score, clinical presentation, CBD diameter, number of CBD stones, and types of initial biliary operations performed between the 2 groups.
Clinical Characteristics.
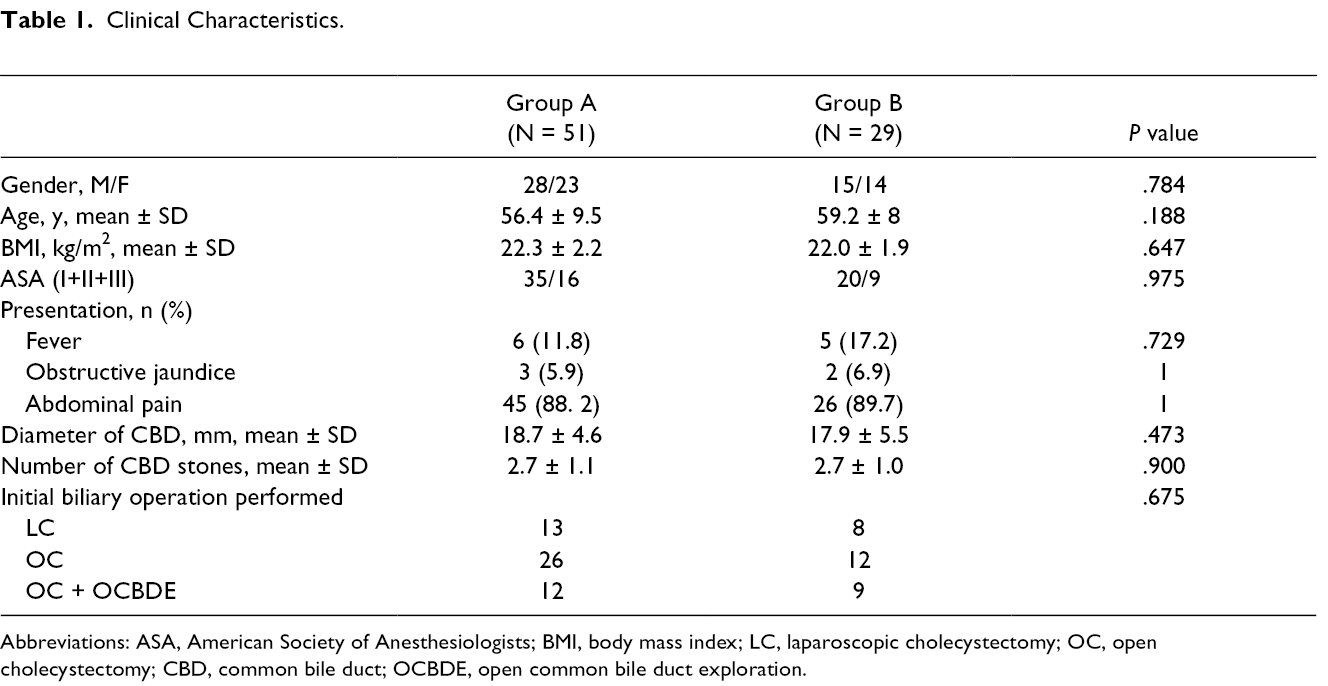
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; LC, laparoscopic cholecystectomy; OC, open cholecystectomy; CBD, common bile duct; OCBDE, open common bile duct exploration.
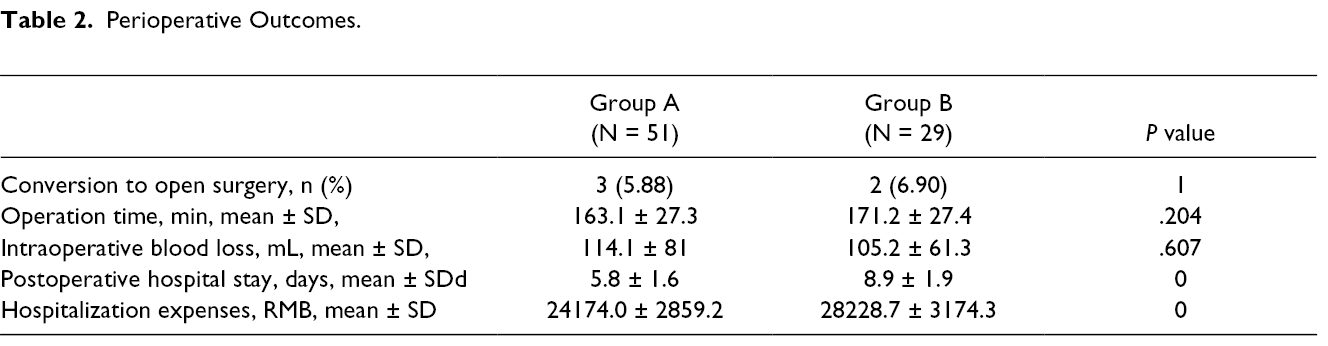
Five patients were converted to open surgery due to adhesions (n = 2), unclear anatomy (n = 1), and impacted bile duct stone (n = 2). There was no significant difference in conversion rate to open surgery between the 2 groups. The length of postoperative hospital stay was much shorter in group A than in group B. The hospitalization expenses were statistically lower in group A than in group B. No significant difference was observed in the operating time and intraoperative blood loss between the 2 groups (Table 2).
Perioperative Outcomes.
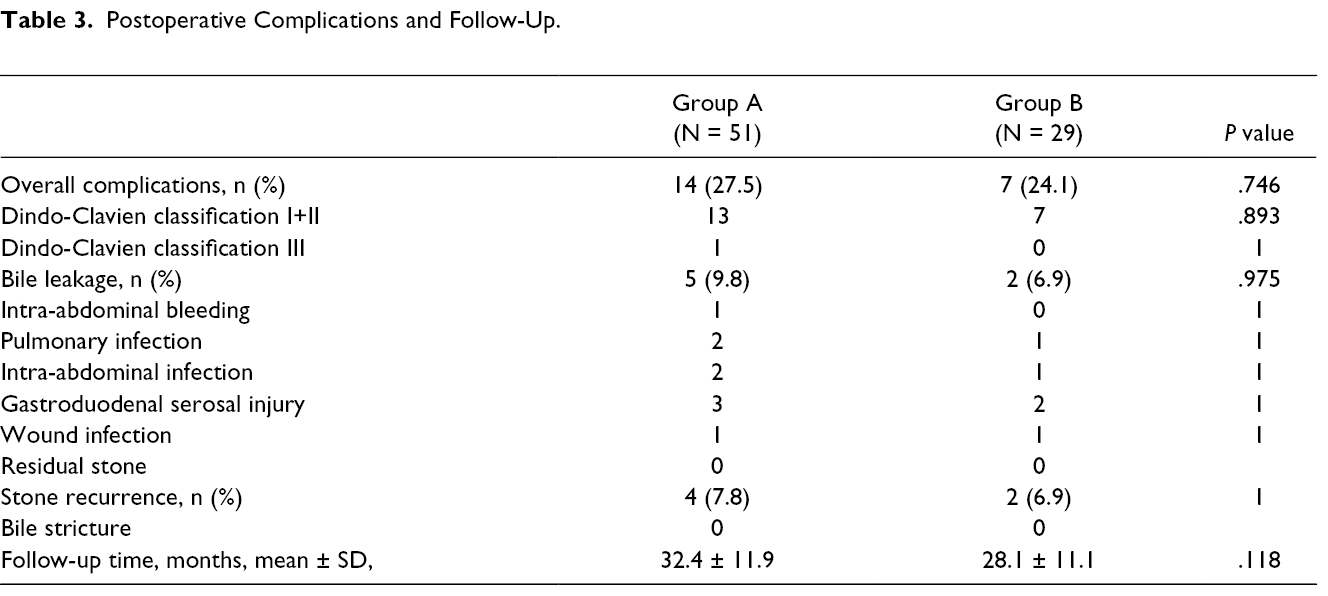
There was no difference in overall complication rate between the 2 groups (Table 3). The bile leakage rate after primary closure seemed higher than after T-tube drainage, but it had no significant difference. Complications associated with T-tube drainage, such as T-tube displacement, bile peritonitis after T-tube removal, and wound infection around the T-tube were not observed in the T-tube drainage group.
Postoperative Complications and Follow-Up.
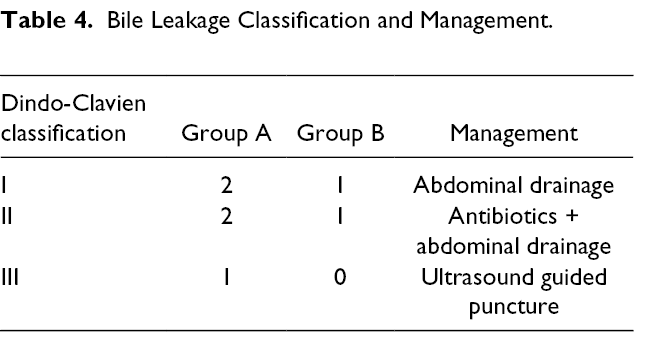
According to Dindo-Clavien classification, 3 cases of bile leakage were categorized as grade I and spontaneously resolved with prolonged abdominal drainage. Three patients developed grade II bile leakage and were successfully managed by antibiotic therapy and abdominal drainage. One patient (grade III) suffered localized biliary peritonitis and underwent ultrasound-guided percutaneous puncture (Table 4).
Bile Leakage Classification and Management.
Patients were followed up till March 2019 and there was no significant difference in follow-up time between the 2 groups. Residual stones were not found in both groups by MRCP and ultrasound examination. No significant difference was found in stone recurrence rate between the 2 groups. Three patients in group A and 2 patients in group B received endoscopic retrograde cholangiopancreatography (ERCP) for recurrent stones, and 1 patient in group A was treated by LCBDE with primary closure. No biliary stricture was observed during the follow-up period.
Discussion
LCBDE has been a challenge in patients with a history of cholecystectomy or choledochotomy. In the early laparoscopic era, previous biliary surgery history was considered a contraindication for laparoscopic surgery due to dense adhesions in the upper right quadrant of the abdomen. With rapid advances in laparoscopic equipment and technique, LCBDE exhibits superior advantages such as optical magnification, direct visualization, effectiveness for retrieving bile duct stones, and minimal invasiveness. Moreover, LCBDE preserves the integrity of the sphincter of Oddi and avoids bile juice regurgitation particularly relevant in young individuals. On the other hand, ERCP used widely for the treatment of CBD stones may lead to pancreatitis, perforation, hemorrhage, and even death. 9 ERCP also disrupts the integrity of the sphincter of Oddi and has a high stone recurrence rate. 10 Nowadays, LCBDE has been increasingly attempted in patients with previous biliary surgery.3,11-13
The optimal bile duct closure method following LCBDE (primary closure of choledochotomy vs T-tube insertion) in patients with previous biliary surgery remains controversial. 14 A randomized trial by Zhang et al 15 assessed the safety and effectiveness of laparoscopic primary closure versus T-tube drainage in patients without abdominal surgery history. LCBDE with primary closure has been performed in patients with previous upper abdominal surgery history including gastrectomy 16 and bowel resection. 17 However, dense adhesion around CBD is usually observed in the setting of previous biliary operation, which will induce CBD edema and inflammation after the dissection of CBD. Therefore, the study evaluated the feasibility and safety of primary closure following LCBDE compared with T-tube drainage in patients with previous biliary surgery history.
Seventy-five patients with previous biliary surgery including open cholecystectomy (OC), laparoscopic cholecystectomy (LC), and OCBDE underwent LCBDE successfully at our institution without perioperative death. The conversion rate to open surgery was 6.25%, which was not higher than that for patients with previous abdominal operation.18,19 The stone clearance rate in both groups was 100%, which was higher than the previously reported values.19,20 It might be due to intraoperative choledochoscopic exploration and repeated confirmation of bile duct clearance before the closure of choledochotomy.
The debate between primary closure of choledochotomy and T-tube drainage following LCBDE still continues. Several studies showed that primary duct closure did not increase overall complication risk and mortality compared to T-tube drainage.4,21 Our results demonstrated that stone recurrence rate was low and bile duct strictures were not observed after primary duct closure. 22 Recently, with the development of laparoscopic techniques, primary choledochotomy closure has been applied successfully in emergency patients, 7 elderly patients, 8 and patients with upper abdominal surgery history. 17 On the other hand, T-tube usage causes inconvenience to patients and may give rise to several complications, such as T-tube displacement, bile leakage after its removal, and wound infection around T-tube. In our institution, we also performed primary closure following LCBDE in patients with previous cholecystectomy or choledochotomy in the past 5 years. The present study revealed that there was no significant difference in the incidence of biliary-specific complications, overall complications, and stone recurrence between the primary closure group and T-tube drainage group. Adhesiolysis, retraction, and further dissection around CBD in patients with previous biliary surgery usually lead to mild to moderate edema and inflammation of CBD wall. Our study showed that while severe suppurative cholangitis, obstruction of distal bile duct, or bile duct remnant stone are not observed intraoperatively, primary closure is also safe and effective. 23 Prior biliary surgery history is not a contraindication for primary closure of choledochotomy. Moreover, the length of postoperative hospital stay and hospitalization expenses of the primary closure group were significantly lower than those of the T-tube drainage group. The results suggest primary choledochotomy closure is safe and effective, and can be performed as an alternative option to T-tube drainage.
Bile leakage is the most frequent postoperative complication for LCBDE with primary closure.24,25 It was reported that slender CBD (<8 mm) and residual CBD stone were 2 independent risk factors for biliary leakage. 26 In addition, LCBDE with primary closure is a technically demanding procedure. Surgeons’ laparoscopic experience was significantly related with bile leakage. In experienced hands, the incidence of bile leakage decreased from 17.1% to 5.6%. 27 Fifty-one patients with primary closure were included in this study. The diameter of CBD was 1.87 cm, which was much larger than 0.8 cm. All operations in our study were performed by experienced laparoscopic surgeons. Discouragingly, bile leakage occurred in 9.8% (5/51) of these patients. Although none of them developed severe biliary peritonitis and underwent reoperation, the bile leakage rate seems higher than previous reported. 26 Another retrospective study also revealed that a higher bile leak rate was observed in nonsevere acute cholangitis, a morbid condition with acute inflammation and infection in the bile duct. 28 The higher bile leakage rate in our study might be associated with CBD edema and inflammation subsequent to abdominal adhesiolysis and dissection of CBD.
The present study demonstrated that primary closure following LCBDE is safe and effective for the management of CBD stones in patients with previous biliary surgery. To the best of our knowledge, this is the largest study to investigate the safety and effectiveness of laparoscopic primary closure in patients with previous biliary surgery history. However, the study is a single-institution retrospective research. Further randomized trials are needed to explore the possible risk factors for bile leakage in patients with previous biliary surgery history.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grants from National Nature Science Foundation of China (No.81760137), Jiangxi Province Science Foundation for Youths (No.20161BAB215225) and Science and Technology Project Founded by the Education Department of Jiangxi Province (No.150131).