
Abstract
Background
Laparoscopic common bile duct exploration (LCBDE) is underutilized by surgeons to treat choledocholithiasis. We hypothesized that fellowship training in acute care surgery (ACS) vs minimally invasive surgery (MIS) results in different LCBDE practices and perceptions, thus producing unique barriers to implementation.
Methods
A survey was distributed by email to members of Society of American Gastrointestinal and Endoscopic Surgeons and the American Association for the Surgery of Trauma to assess surgeon demographics, surgeon-specific perceptions, practice patterns, and barriers to LCBDE utilization. Categorical data were compared with Pearson’s chi-square, and continuous parametric data were compared with a t test.
Results
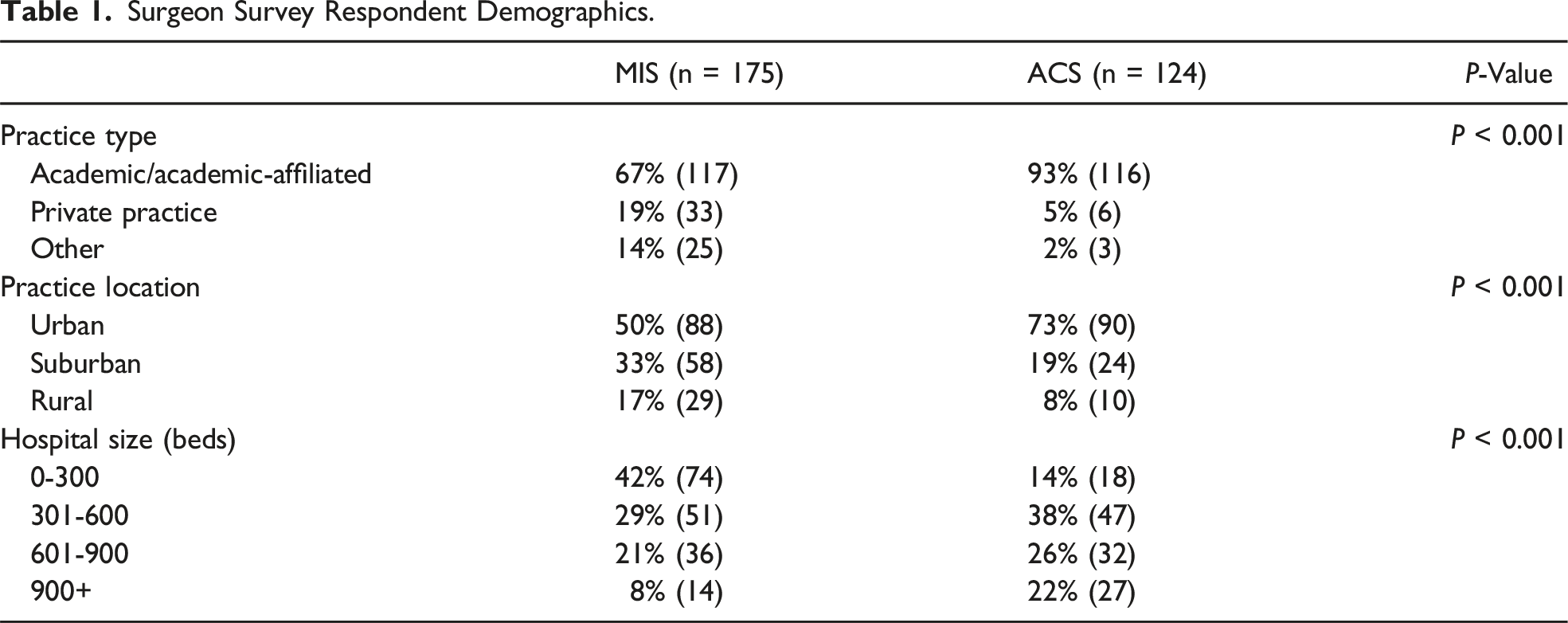
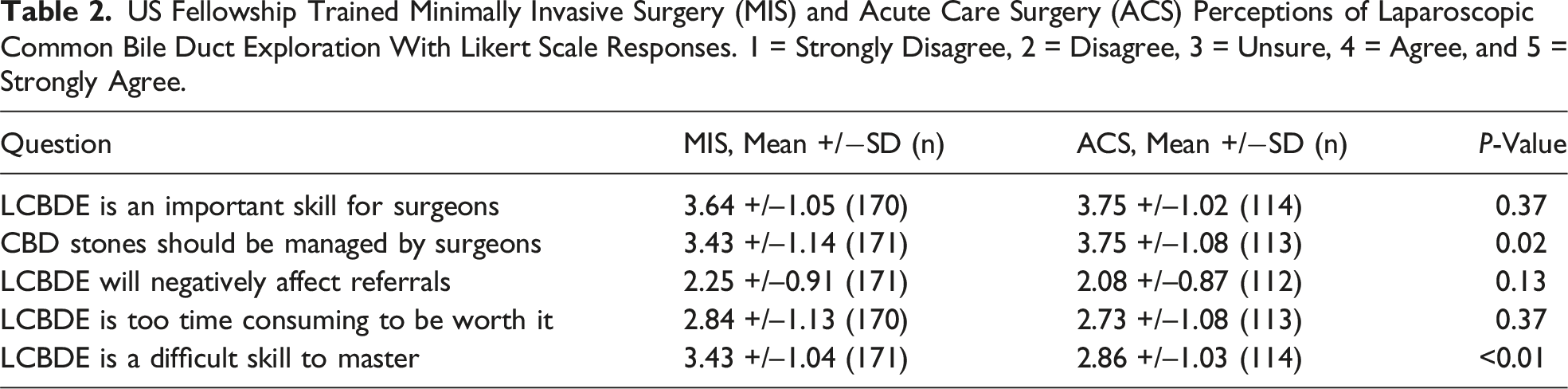
543 US surgeons who perform laparoscopic cholecystectomy completed the survey. Of all, 124 survey respondents were ACS trained and 175 were MIS trained. Similar proportions of MIS and ACS surgeons prefer to manage choledocholithiasis with LCBDE (28% vs 27%, P = 0.79). The most utilized LCBDE technique was choledochoscopy (71% vs 69%, P = 0.17). MIS surgeons more frequently perform intraoperative cholangiogram (IOC) compared to ACS surgeons (P = 0.02). A third of MIS surgeons felt that LCBDE is too time consuming to be of value, vs 25% of ACS surgeons (P = 0.37). When asked if LCBDE is difficult to master, 56% of MIS surgeons agreed compared to 32% of ACS surgeons (P < 0.01).
Discussion
Both MIS and ACS surgeons utilize LCBDE infrequently despite responding that choledocholithiasis should be managed by surgeons. Compared to MIS, fewer ACS surgeons consider time to perform LCBDE and difficulty as barriers. Understanding these barriers can influence education and efforts toward increasing adoption in both groups.
Keywords
Key Takeaways
• LCBDE is underutilized by surgeons to treat choledocholithiasis. • MIS and ACS surgeons have different LCBDE practices and perceptions. • Targeting differences and similarities can drive outreach, education, and adoption.
Introduction
Surgical management of choledocholithiasis with laparoscopic common bile duct exploration (LCBDE) has been associated with decreased length of stay and cost with equivalent morbidity and mortality as two-stage management with cholecystectomy and endoscopic retrograde cholangiopancreatography (ERCP).1,2 Although the advantages to the health care system and patient have been extensively described in the literature, utilization of this technique remains low among surgeons.3,4 There are many contributing factors to this underutilization including lack of training, resources, perceived time constraints, and system barriers.5,6
Recent literature has advocated for the acute care surgery (ACS) model to embrace LCBDE, as many of these barriers can be overcome by a well-positioned emergency general surgery service.7-9 Involvement of an ACS service has previously been shown to decrease length of stay and time to the operating room for other benign biliary disease such as acute cholecystitis and gallstone pancreatitis.10-12 Historically, minimally invasive surgery (MIS) societies such as the Society of Gastrointestinal and Endoscopic Surgeons (SAGES) have advocated for LCBDE use with practice management guidelines, but these guidelines have not been published in trauma and acute care surgery societies such as the Eastern Association for the Surgery of Trauma (EAST) or the American Association for the Surgery of Trauma (AAST).13,14 Due to different backgrounds, practices, and patient populations, we hypothesized that MIS and ACS fellowship trained surgeons would have different LCBDE practices and perceptions of technique utility. These differences, if present, may produce unique barriers to technique implementation in the respective surgeon groups. Understanding these barriers can influence outreach, education, and efforts toward increasing adoption.
Methods
Institutional Review Board review was completed at Atrium Health Wake Forest. Content experts who regularly perform laparoscopic cholecystectomy and common bile duct exploration designed a survey to assess LCBDE practice patterns, surgeon perceptions, and barriers. This was refined until a consensus was reached. The consensus survey was initially piloted with a small group of surgeons at a single institution who regularly perform laparoscopic cholecystectomy. The target audience for eventual survey dissemination was MIS and ACS surgeons who perform laparoscopic cholecystectomy, regardless of LCBDE experience. The survey underwent 6 rounds of refinement until finalization. The survey data was collected and maintained by REDcap (Research Electronic Data Capture) tools. The Society of American Gastrointestinal and Endoscopic Surgeon (SAGES) and the American Association for the Surgery of Trauma (AAST) societies were chosen strategically for survey dissemination via membership email, as these societies are comprised of a high percentage of fellowship trained MIS and ACS surgeons. This survey study was approved by the Institutional Review Board. Exclusion criteria included surgeons who practice outside the United States and surgeons who perform 0 cholecystectomies yearly.
The survey collected information regarding surgeon demographics (fellowship training type, practice setting and location, hospital size based on number of beds, and years in practice) along with surgeon-specific perceptions, practice patterns, and barriers. The survey questions assessing practice patterns inquired about the surgeons’ preferred choledocholithiasis management strategy, intraoperative cholangiogram utilization, and the specific LCBDE tools/techniques employed. Surgeon-specific perceptions and barriers were assessed by survey questions surrounding surgical choledocholithiasis management, referral relationships, and the difficulty and time constraints of LCBDE completion. Categorical data were compared with Pearson’s chi-square, and continuous parametric data were compared with a t test. A P-value <0.05 was considered significant.
Results
Surgeon Survey Respondent Demographics.
Similar proportions of MIS and ACS surgeons prefer to manage choledocholithiasis surgically with laparoscopic common bile duct exploration (28% vs 27%, P = 0.79). Transcystic exploration was predominantly favored over transcholedochal exploration in both groups, 94% vs 92%, respectively (P = 0.49). The most utilized LCBDE technique in both groups was choledochoscopy (71% vs 69%, P = 0.17), although, a significantly larger percentage of ACS surgeons reported balloon sphincteroplasty as their most utilized technique (15% vs 25%, P = 0.08). The MIS surgeons more frequently perform intraoperative cholangiogram (IOC) as compared to ACS surgeons (P = 0.02) (Figure 1). Forty percent of MIS trained surgeons report patients with choledocholithiasis are admitted to a surgical service rather than a medicine service for management, whereas 53% of ACS trained respondents admit choledocholithiasis to the surgical team (P = 0.02). US fellowship trained minimally invasive surgery (MIS) and acute care surgery (ACS) surgeons’ intraoperative cholangiogram utilization.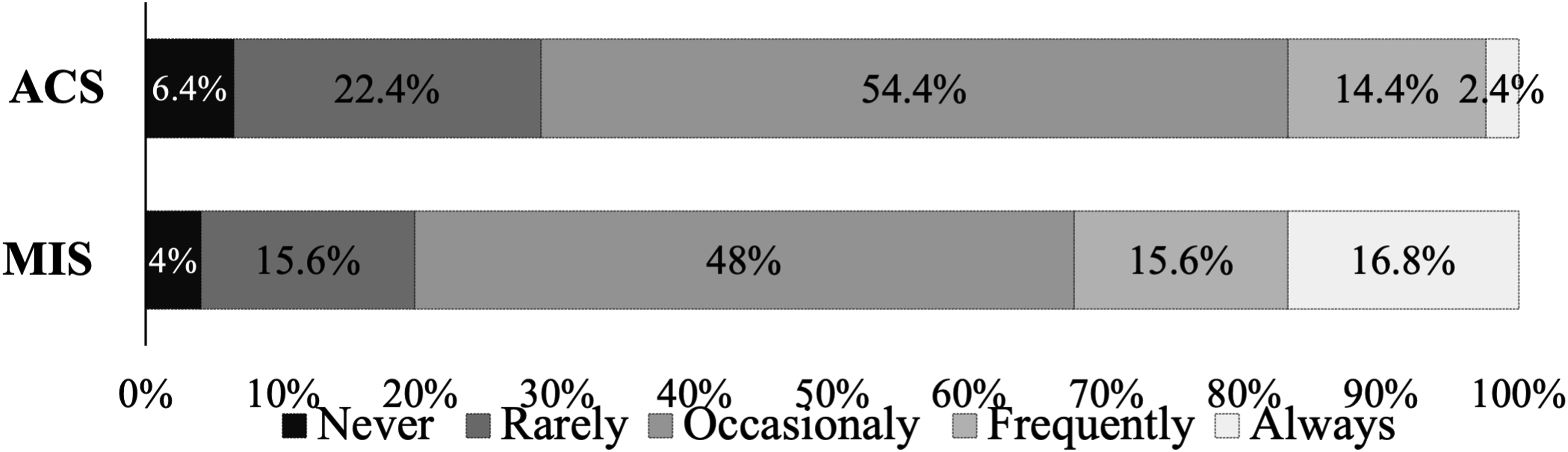
US Fellowship Trained Minimally Invasive Surgery (MIS) and Acute Care Surgery (ACS) Perceptions of Laparoscopic Common Bile Duct Exploration With Likert Scale Responses. 1 = Strongly Disagree, 2 = Disagree, 3 = Unsure, 4 = Agree, and 5 = Strongly Agree.
Discussion
Surgeons with fellowship training in minimally invasive surgery versus those who obtain fellowship training in acute care surgery regularly experience different disease pathologies and case mix.15,16 Due to differing training environments, practice settings, and patient populations, we hypothesized that MIS and ACS fellowship trained surgeons would have different LCBDE practices and perceptions of technique utility. Furthermore, identifying these differences could allow for targeted, unique interventions to increase adoption in each group. The survey revealed that both surgeon groups predominantly manage choledocholithiasis with laparoscopic cholecystectomy and ERCP, rather than with LCBDE. When the survey respondents do perform LCBDE, both ACS and MIS surgeons typically complete the operation transcystically with a choledochoscope. Neither group was concerned that performing LCBDE would impact their referral relationships with gastroenterologists. The main differences between groups were that acute care surgeons more often utilize fluoroscopic interventions for stone removal, admit choledocholithiasis patients to surgical services, and were more apt to agree that surgeons should manage choledocholithiasis. The MIS trained surgeons more often perform intraoperative biliary imaging with cholangiography but assert that LCBDE is a difficult skill to master. Difficulty of skill acquisition was less concerning to the ACS trained surgeons.
The survey was designed to define differences between two very specific surgeon populations: those who have been fellowship trained in acute care surgery versus those trained in minimally invasive surgery. This comparison regarding laparoscopic common bile duct utilization and adoption has not previously been defined in the literature. However, the common themes between both surgeon groups, such as low rates surgical management of choledocholithiasis, are consistent with previous survey studies. Baucom et al. administered an email survey to US general surgeons through the American Medical Association Physician Masterfile to determine choledocholithiasis management trends and variables that contributed to practice patterns. 6 Over 700 surgeons completed the survey and were included in the analysis. The survey found that about 30% of surgeons would perform LCBDE if common duct stones were discovered intraoperatively, which was consistent with our findings almost 10 years later providing evidence that minimal progress has been made in recent history toward the adoption of surgical management of choledocholithiasis. Baucom et al. also found that metropolitan areas based on zip code, performing IOC selectively, and having an available advanced endoscopist were associated with management of choledocholithiasis via preoperative ERCP. Interestingly, our survey revealed that the MIS trained surgeons more often perform intraoperative cholangiography but do not perform LCBDE at higher rates than ACS trained surgeons. The utility and indications for intraoperative cholangiography has long been debated in the literature.13,17,18 The Safe Cholecystectomy Multi-society Practice Guideline suggests “the liberal use of intraoperative cholangiography (IOC) during laparoscopic cholecystectomy to mitigate the risk of bile duct injury.” 18 While this practice guidelines specifically advocates for IOC to mitigate bile duct injury risk, much of the work done around safe cholecystectomy practices has been spearheaded through the SAGES surgical society. This clinical focus and advocacy may contribute to MIS trained surgeons more frequently employing IOC during their laparoscopic cholecystectomies. Thus, the intention behind performing more intraoperative imaging may be to define anatomy and prevent or recognize injury rather than to identify and treat common bile duct stones. This motivation could account for the discrepancy seen in increased frequency of IOC utilization by MIS surgeons, yet limited LCBDE performance.
One of the limitations of this survey study is its small sample size. While the survey was distributed to the SAGES and AAST surgical societies in effort to capture high percentages of ACS and MIS fellowship trained surgeons, not all members in either group are trained in these domains. The SAGES surgical society is specifically home to many other minimally invasive subspecialties that do not perform laparoscopic cholecystectomy. Thus, the limited response may be attributed to heterogenous membership despite the surgical societies being specifically selected. While the generalizability of the results may be debated, the commonalities between the two groups in addition to their differences highlight potential points of intervention to increase adoption.
The acute care surgery model is well-positioned for surgeons to manage choledocholithiasis. Medical admission for choledocholithiasis is often a barrier to adoption of LCBDE as many of the patients will have an ERCP before the surgical team is consulted. Surgical admission allows for the surgery team to drive the care and potentially take a surgery-first approach to LCBDE management.19,20 As evidenced by the survey and previous literature, ACS surgeons are apt to facilitate surgical admissions for benign biliary disease.9-11 By continuing to advocate for this admission pattern, the ACS model, as compared to the elective MIS practice, may be leveraged to increase surgical management of common duct stones.
Additionally, the compensation model for ACS surgeons is largely shift based whereas elective MIS trained surgeons are traditionally compensated via RVU productivity models. This difference may contribute to ACS surgeons’ willingness to spend additional time in the operating room to overcome the LCBDE learning curve rather than proceeding with the well-worn path of perioperative ERCP. Regardless of compensation models, the RVU benefits of laparoscopic common bile duct exploration with balloon sphincteroplasty and/or choledochoscopy are likely not known to many surgeons. The RVU reimbursement can be more than two times that of a standard laparoscopic cholecystectomy.
Irrespective of admission pattern, ACS surgeons perform less IOC as compared to MIS surgeons. While a possible explanation for the difference in utilization of IOC has already been described in the manuscript, it may represent an opportunity for growth of a skill set for the acute care surgeons. Efficiency and comfort with intraoperative bile duct imaging may lower the threshold for surgical choledocholithiasis intervention. Emphasis on the utility and potential benefits (anatomy definition, stone identification, and injury recognition) from prominent trauma and acute care surgical societies and in ACS fellowship curriculum may advance future IOC utilization. Additionally, ACS surgeons do not perceive LCBDE as a difficult skill to master. This perception may facilitate wide adoption, if the correct training programs are in place. More educational initiatives and courses are likely required in the acute care surgery realm.
Alternatively, the MIS surgeon respondents perceive LCBDE as a difficult skill to master. The survey MIS surgeons also overwhelmingly use choledochoscopy for explorations, while the ACS surgeons additionally use fluoroscopic interventions such as balloon sphincteroplasty. The simplified Seldinger technique of fluoroscopic balloon interventions may be a skill the MIS surgeons could employ to facilitate ease of intervention and decrease perceived difficulty. 7
Practice patterns among ACS and MIS surgeons were identified and seem to be specific to surgeon experience and fellowship training. Understanding barriers to LCBDE implementation can help tailor educational initiatives to each group and will increase utilization of this technique. Ultimately, increasing surgical management of common bile duct stones can help decrease length of stay and cost for patients and the health care system while maintaining efficacy.1,2
Footnotes
Ethical Approval
The Atrium Health Wake Forest IRB waived the requirement for approval for this survey study.
Author Contributions
Conception and study design: MEB, LPN, and RS. Literature review: MEB, LPN, and RS. Data acquisition: MEB, ECW, JS, GEC, and GDS. Data analysis and interpretation: MEB, ECW, JS, GEC, and GDS. Drafting of the manuscript: MEB, ECW, LPN, SLK, VCN, and RS. Critical revision: MEB, ECW, LPN, JS, GEC, GDS, SLK, VCN, and RS.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request.