
Abstract
Assessment of aerodigestive injuries in penetrating neck trauma (PNT) is currently left up to the discretion of physicians which can result in a lot of confusion and unnecessary testing. This study was performed at a level 1 trauma center to assess the role of computed tomography arteriogram (CTA) in evaluating for aerodigestive injury in PNT. A total of 242 patients met criteria, with ages ranging from 7 to 86 years. Computed tomography arteriogram, EGD, esophagography, and bronchoscopy were classified into positive, negative, and indeterminate results. Computed tomography arteriogram was then further analyzed for violation of the carotid sheath, investing, pretracheal, and deep cervical fascias. Results showed a high sensitivity and NPV (100%) of CTA in assessing aerodigestive injury. Computed tomography arteriogram is a reliable first-line screening tool for aerodigestive injury. EGD appears more useful than esophagography at identifying esophageal injuries. Esophagography and bronchoscopy should be reserved to aid in injury management decision-making rather than as screening studies.
Penetrating neck trauma (PNT), defined as full thickness breech of the platysma muscle, account for about 5-10% of all trauma cases, with a mortality of up to 10%. 1 The risk of PNT comes from potential damage to vital vascular and aerodigestive structures. Historically, the risk for vascular and aerodigestive injuries in PNT was categorized based on the entry site of injury based on the 3 anatomical zones of the neck that was first described by Monson et al in 1969. However, later studies demonstrated that the zone approach does not accurately predict injuries. 1
The current practice management guidelines for aerodigestive injuries in PNT from the Western Trauma Association, Eastern Association for the Surgery of Trauma, and World Society for Emergency Surgery vary and either call for multiple overlapping assessments or are dependent on physician discretion.2-4 The tests for aerodigestive injuries include bronchoscopy, esophagoscopy (EGD), and esophagography. For vascular injuries, computed tomography arteriogram (CTA) is obtained as it has been shown to be a sensitive and specific modality for assessing vascular neck injury. 1 The aim of this study was to evaluate the diagnostic yield of bronchoscopy, EGD, and esophagography relative to operative exploration and CTA in detection of aerodigestive injuries.
A retrospective study was conducted of all patients who presented to the emergency department at John H. Stroger, Jr Hospital of Cook County with penetrating neck injuries from January 1, 2017, to December 31, 2021. Patients found to have injuries from a non-penetrating mechanism were excluded. Patients who were too unstable for preoperative imaging and were immediately taken to the operating room, were deceased shortly after arrival, or absconded prior to receiving imaging were excluded.
Demographic data, clinical, imaging, and operative findings were collected from medical records. Data was collected and analyzed using Microsoft Excel (Chicago, IL). Computed tomography arteriogram, EGD, esophagography, and bronchoscopy were classified into positive, negative, and indeterminate results. Computed tomography arteriogram was then further analyzed for violation of the investing fascia, pretracheal fascia, deep cervical fascia, and carotid sheath.
Of 318 patients with PNT, 242 patients met study criteria. Patient age ranged from 7 years to 86 years, with a mean age of 31 years. 201 patients (83%) were male and 41 (17%) were female. 104 patient suffered stab wounds (43%) and 138 patients gunshot wounds (57%). Of the 242 patients who met criteria, 3 patients were found to have esophageal injuries, 2 had laryngeal/tracheal injuries, and 2 had pharyngeal injuries. 214 patients underwent CTA, 73 underwent EGD, 60 underwent esophagram, and 11 underwent tracheo-bronchoscopy. EGD was negative in 67 patients, positive for 3 esophageal injuries, 2 pharyngeal injuries, and 1 indeterminate result. Esophagography was negative in 56 patients, with no esophageal injuries, 2 pharyngeal injuries, and 2 indeterminate results. Bronchoscopy was negative in 7 cases, with 1 tracheal injury, and 3 indeterminate cases. The singular positive bronchoscopy was primarily therapeutic in removing a bronchial bullet in a known tracheal injury.
Diagnostic Accuracy of CTA. Comparing the Diagnostic Measures of CT Findings With the Gold-Standard Tests Used to Diagnose Aerodigestive Injuries: EGD, Esophagram and Bronchoscopy.
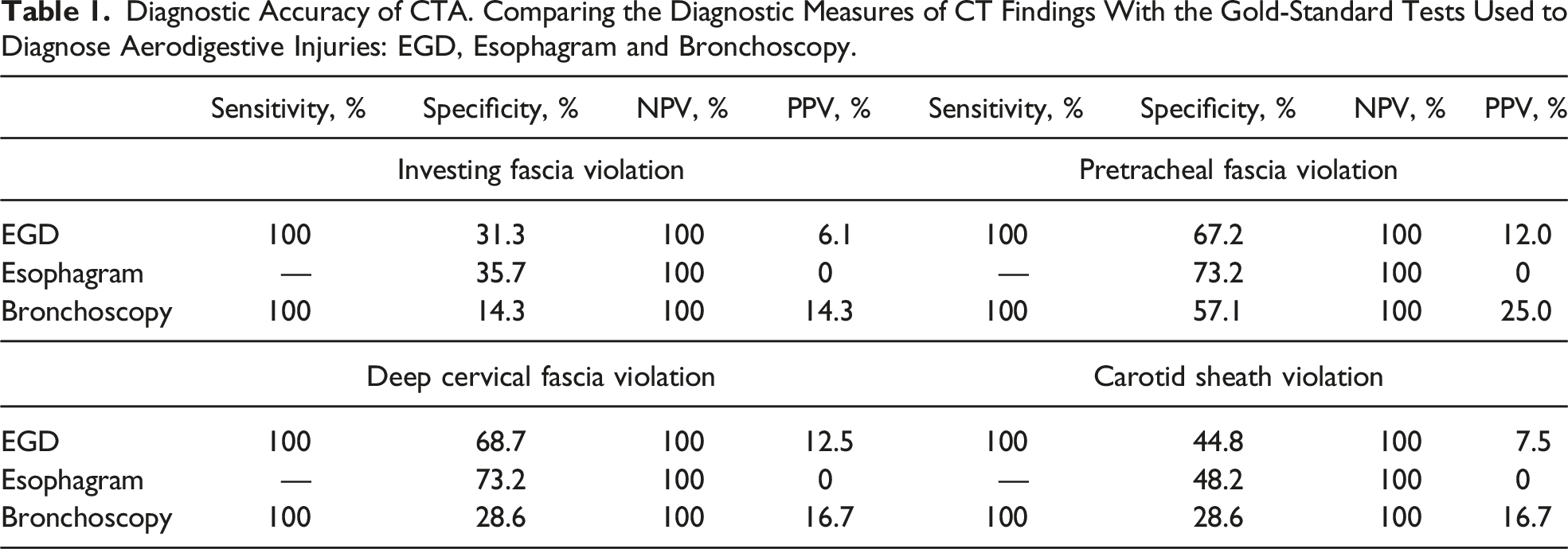
Due to the many vital structures in the neck, PNT can result in high rates of mortality. Furthermore, given the associated risk and the numerous diagnostic tests available, ruling out aerodigestive injuries can be worrisome, resulting in numerous, possibly unnecessary tests to be performed as it is left up to the discretion of the physician. Currently, CTA is performed as a reliable test for ruling out vascular and orthopedic injuries. In this study, CTA was also found to be reliable at evaluating for cervical aerodigestive injuries. As compared to EGD and esophagram, CT-derived information had 100% sensitivity and NPV in identifying aerodigestive injuries.
As such, if CTA is negative for violation of the pretracheal or deep cervical fascia, then aerodigestive injury can safely be ruled out and no further testing is required. However, given the low specificity, if CTA is positive for air in the pretracheal or deep cervical fascia, then further testing is required to rule out aerodigestive injuries. With its higher detection of injury and fewer indeterminate results, EGD appears more useful than esophagography at identifying esophageal injuries and should be first line after CTA. Esophagography and bronchoscopy should be reserved to aid in injury management decision-making rather than as screening studies.
Limitations of this study included the low number of patients with PNT who received EGD, esophagram, and bronchoscopy. However, despite this, the data demonstrated a high sensitivity for CTA as a screening test for aerodigestive injuries in PNT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.