
Abstract
Acute appendicitis is a leading cause of emergency abdominal surgery, with laparoscopic appendectomy (LA) established as the gold standard treatment. Notwithstanding its extensive utilization, there is no agreement on the most effective method for closing the appendiceal stump and dividing the mesoappendix. This review sought to assess existing treatments in terms of surgical duration, hospital length of stay (LOS), complications, and cost-effectiveness. A comprehensive review of 53 studies was performed. Eligible studies included adult patients undergoing appendectomy and examined various procedures for appendiceal stump closure and mesoappendix division. The primary outcomes were surgical duration and LOS; the secondary objectives were postoperative complications and cost-effectiveness. For appendiceal stump closure, clips and staples were frequently linked to decreased surgical duration in comparison to ligatures or sutures, although outcomes varied. Clips were also associated with a reduced length of hospital stay. Cost-effectiveness analyses consistently found clips to be the most economical option for stump closure, with staples the most expensive. Complication rates were largely comparable, though loop ligatures were linked to more organ/space infections, and clips showed higher rates of surgical site infections in some studies. For mesoappendix division, electrocautery and energy devices generally shortened operative time compared with mechanical methods. Electrocautery was the least costly for mesoappendix division, while energy devices tended to increase costs. Division of the mesoappendix and appendiceal stump closure can be achieved with a wide range of techniques and tools. The optimal treatment strategy varies significantly based on the outcome investigated.
Introduction
Acute appendicitis is among the most prevalent abdominal emergencies, with an incidence of 233 cases per 100 000 annually and a lifetime risk of 6.7% in women and 8.6% in men.1,2 Laparoscopic appendectomy is the gold standard treatment in high- and middle-income countries. 3 Various techniques exist for appendiceal stump closure and mesoappendix division, including ligatures, clips, staples, electrocautery, and ultrasonic or energy-based approaches. 4
While numerous publications have investigated individual procedures, there is a paucity of thorough comparisons among various methods for appendiceal stump closure and mesoappendix division.5-7 This disparity underscores the necessity for a systematic examination. This review seeks to assess and compare different surgical procedures employed in appendectomy, concentrating on surgical duration, length of hospital stay, cost-effectiveness, and complications to inform intraoperative decision-making.
Methods
Eligibility Criteria
Out of the initial 529 articles found, 53 articles were deemed to meet the search criteria. Articles that met the following inclusion criteria were included in the review: (a) the study design was either a randomized controlled trial, meta-analysis, case-control, or an observational cohort study investigating the techniques for appendiceal stump closure or mesoappendix division transection in patients who underwent appendectomy for acute appendicitis; (b) patients were managed using laparoscopic or open appendectomy; (c) the experimental group and the control group received different treatments; (d) the study recorded data on median/mean surgical duration, mean/median hospital length of stay (LOS), surgical/anesthetic costs, or intra- and postoperative complications; and (e) the study included solely adult patients. Articles were excluded based on the following criteria: (a) duplicate articles; (b) irrelevant articles; (c) articles not accessible in English or lacking English translations; (d) data that is not accessible within the manuscript; (e) articles for which the full text was not accessible; (f) studies not indexed by PubMed; (g) previous systematic reviews (without a meta-analysis component), reviews, case reports, and letters; (h) studies present in one of the included meta-analyses; (i) low evidence papers; (j) conference abstracts; and (k) studies not comparing relevant techniques.
Search Methodology
The PubMed and MEDLINE databases were methodically searched from March 2024 to April 2024 for articles published between 2000 and 2024. The search terms were a combination of medical subject headings terms and the subsequent terms: appendicitis, appendix, mesoappendix, appendix resection, mesoappendix transection, stump closure, appendectomy, laparoscopic appendectomy, clips, loops, endoloop, ligatures, staples, sutures, electrocautery, energy device, ultrasonic and bipolar vessel-sealing systems (eg, LigaSure) (see Supplemental Table 1 for complete search strategy). 8
Because this review focuses on a highly specialized surgical topic, a narrowed search strategy was employed. PubMed and MEDLINE were selected as they provide the most comprehensive and clinically relevant coverage of biomedical and surgical literature, particularly for operative techniques and outcomes related to appendectomy. Preliminary scoping indicated that expanding the search to additional databases produced predominantly duplicate citations or studies outside the scope of surgical technique evaluation, without improving yield or methodological completeness. Therefore, concentrating the search on these 2 platforms ensured both rigor and reproducibility while maintaining relevance to the clinical question.
Study Selection
The following information was retrieved: PubMed unique identifier, authors’ names, publication year, the country where the study was conducted, study design, study subjects, the number of participants, the number of male and female participants, the range of years covered by the study, case and control procedure, the number of patients who underwent the case and control procedure, the number of patients lost to further analysis, the number of patients with and without any complication for the case and control procedures, the number of patients with and without a specific complication for the case and control procedures, and mean and SD or median and IQR for surgical duration and hospital LOS.
Outcomes
The primary outcomes of interest were the surgical duration and total hospital LOS. The secondary outcomes of interest were complications as well as the cost of the procedures.
Terminology
In this review, terminology related to management of the appendix base has been standardized for consistency. Although the original studies variably described this step as appendix base division, appendix resection, transection of the appendix base, or appendiceal stump closure, these descriptions have been unified under the collective term “appendiceal stump closure.” This term is used to denote the operative management of the appendiceal base during appendectomy, irrespective of the specific technique employed. While there are technical differences in how appendiceal stump closure is achieved, such as single-step closure and division with staples vs sequential closure followed by sharp division when using loop ligatures or sutures, outcomes were analyzed according to the method used to manage the appendiceal base rather than the number of procedural steps.
Results
Appendiceal Stump Closure
Surgical Duration
Management of the Appendix Base—Surgical Duration
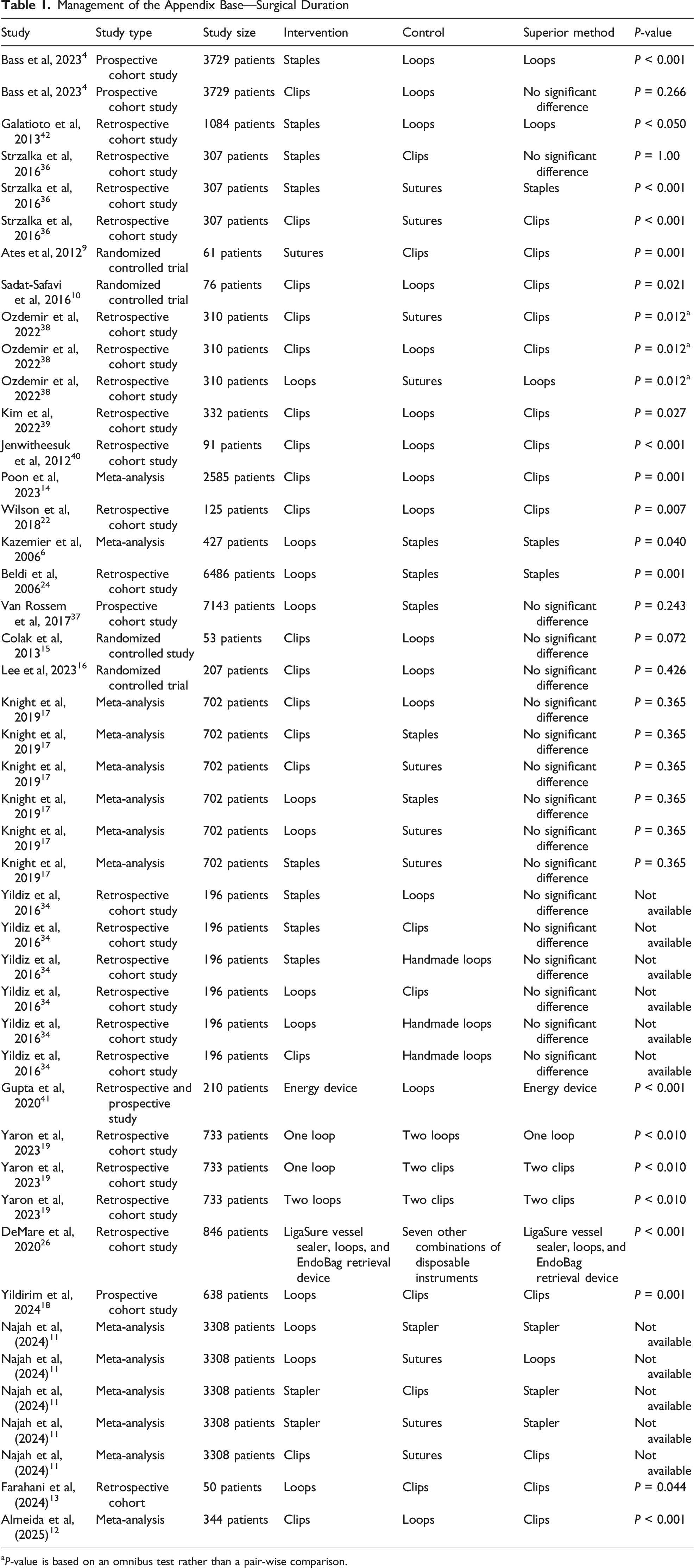
aP-value is based on an omnibus test rather than a pair-wise comparison.
In contrast, Kazemier et al (2006) analyzed 4 randomized controlled trials (n = 427) and found stapling reduced surgical time by 9 minutes vs loop ligatures (P = 0.040), though findings were heterogeneous (I2 = 73%). 6 Ates et al (2012) reported that clips were significantly faster than sutures (41.27 ± 12.2 min vs 62.81 ± 15.4 min, P = 0.001). 9 Similarly, Sadat-Safavi et al (2016) found clips faster than loop ligatures (21.5 vs 23.3 min, P = 0.021). 10 Consistent with previous evidence, Farahani et al (2024), Almeida et al (2025), and Najah et al (2024) each reported faster procedures with clips compared with loops.11-13 In addition, Najah found that suture closure was associated with a significantly longer surgical duration than clip application. A meta-analysis by Poon et al (2023) demonstrated appendiceal stump closure time reduced by 2 minutes and 7 seconds with clips compared to loops, and combined results from 6 RCTs showed an overall 5.15-minute decrease in surgical duration (95% CI −2.05 to −8.24 min, P = 0.001). 14
However, Colak et al (2013) and Lee et al (2023) found no significant differences in mean surgical duration between clips and loops.15,16 Knight et al (2019) reported similar mean surgical durations across clips (37 min; range 26-65), loops (39 min; 44-76), staples (51 min; 40-63), and sutures (33 min, no range) [F (2.17) = 1.078, P = 0.365]. 17 Yildirim et al (2024) demonstrated a shorter surgical duration for clips vs handmade loops (40.53 ± 11.63 min vs 48.76 ± 16.16 minutes; P = 0.001) without significant variations in other clinical parameters such as ASA scores, symptom duration, length of hospital or ICU stay, preoperative laboratory findings, histopathological outcomes, mortality, or morbidity (P > 0.05). 18
Length of Stay
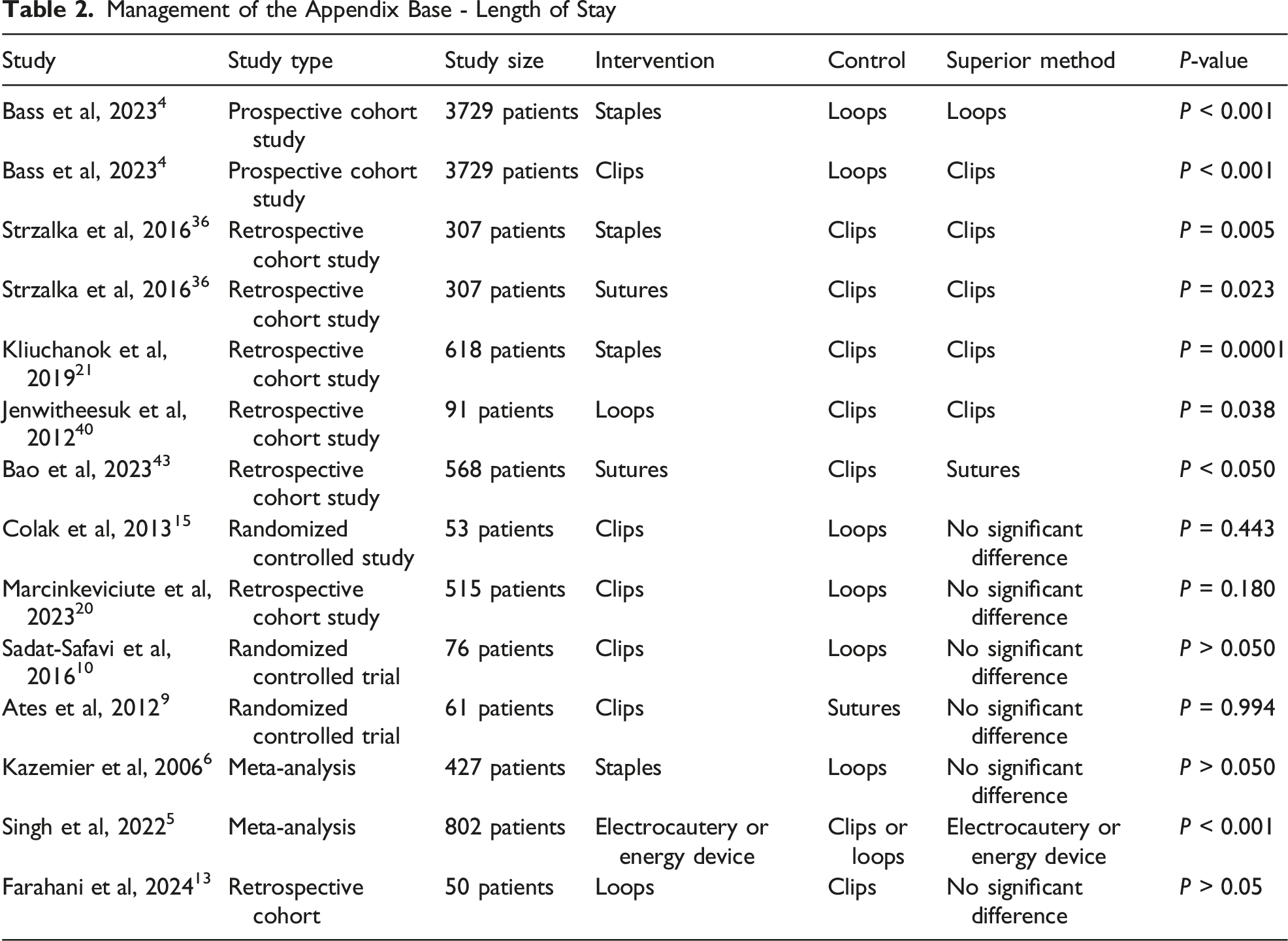
Management of the Appendix Base - Length of Stay
Cost-Effectiveness
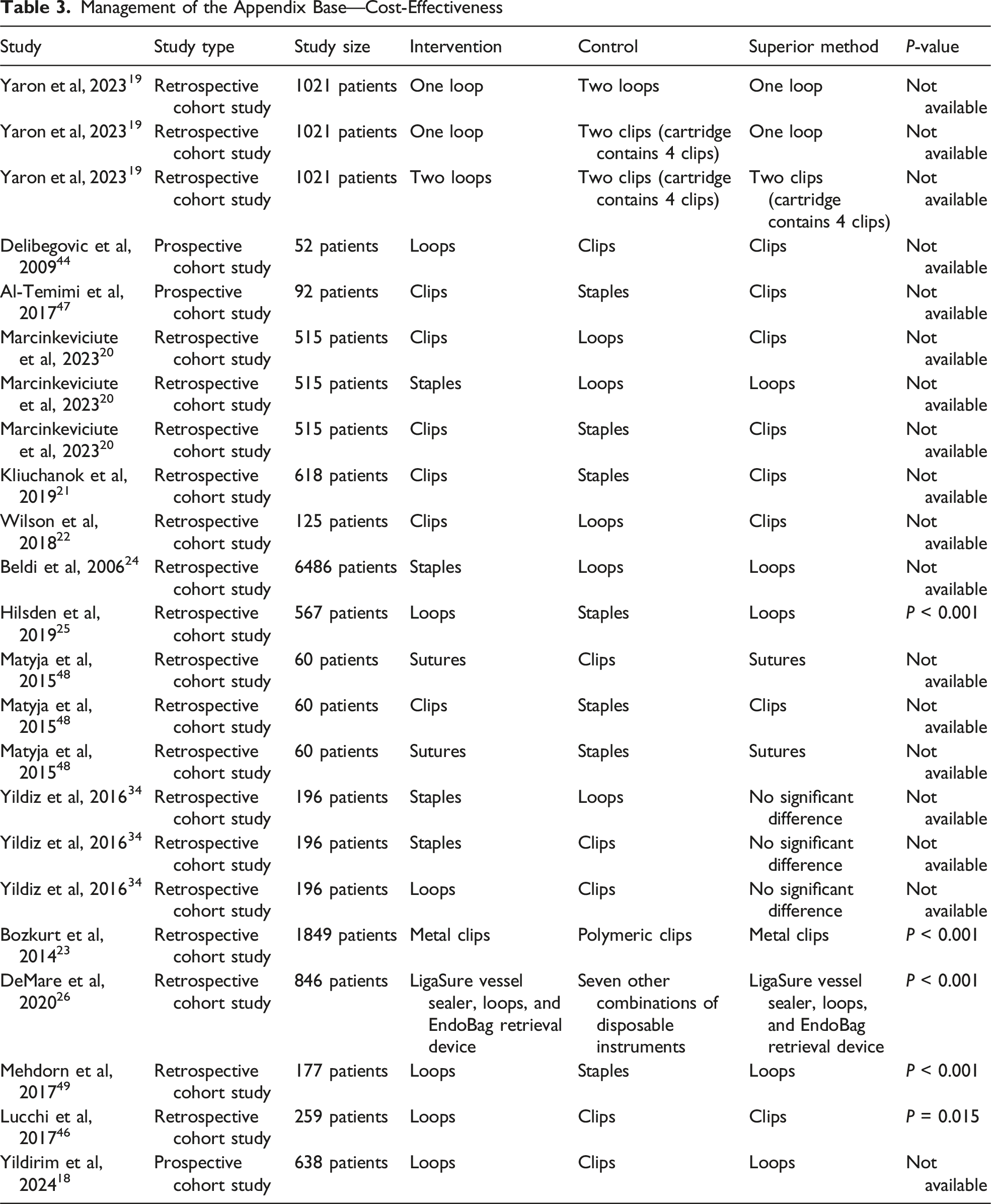
Yaron et al (2023) compared 1021 appendectomies and found double-loop ligatures ($220) were costlier than clip closure ($180 for a cartridge of 4 clips, excluding reusable applier cost) and single-loop ligature ($110). 19 Marcinkeviciute et al (2023) reported the lowest cost with clips (7.69€) followed by loops (91.35€) and staples (514.50€). 20 Kliuchanok et al (2019) similarly reported substantial cost savings with clips compared to staples (19.94€ vs 348.70€), 21 while Wilson et al (2018) found polymeric clips to be less expensive than loop ligatures (£21 vs £49 per surgery). 22 Moreover, Bozkurt et al (2014) found significant cost variation between clips types used, with titanium, metal, and polymeric clips costing $7, $10, and $50 per case, respectively. 23
While Beldi et al (2006) noted a 1.7-minute reduction in surgical duration with staples, the inclusion of other material costs led to an overall increase of $248 compared with loop closure. 24 Hilsden et al (2019) and DeMare et al (2020) confirmed lower total operative and disposable costs with loop ligatures.25,26 Yildirim et al (2024) found clip closure 25.8 times costlier than loops ($31 vs $1.20). 18
Management of the Appendix Base—Cost-Effectiveness
Complications
Management of the Appendix Base—Complications
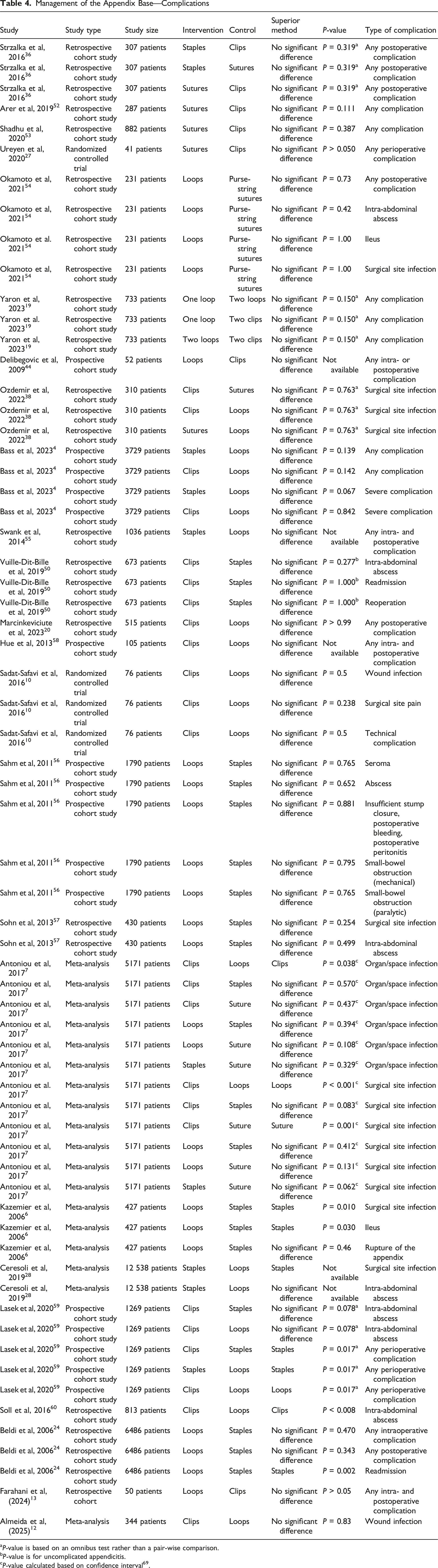
aP-value is based on an omnibus test rather than a pair-wise comparison.
bP-value is for uncomplicated appendicitis.
cP-value calculated based on confidence interval 69 .
Antoniou et al (2017) (meta-analysis of 43 RCTs) identified suture ligation as most effective, with lower risk of superficial and organ/space infections. 7 Sutures were associated with fewer operative site infections than clips [OR (95% CI): 0.20 (0.08-0.55)], while clips carried a higher infection risk than loops [OR (95% CI): 2.22 (1.56-3.13)]. Conversely, clips were linked to a lower risk of organ/space infection compared to loops [OR (95% CI): 0.56 (0.32-0.96)]. Kazemier et al (2006) and Ceresoli et al (2019) demonstrated lower infection rates with staples than loops.6,28
Mesoappendix Division
Surgical Duration
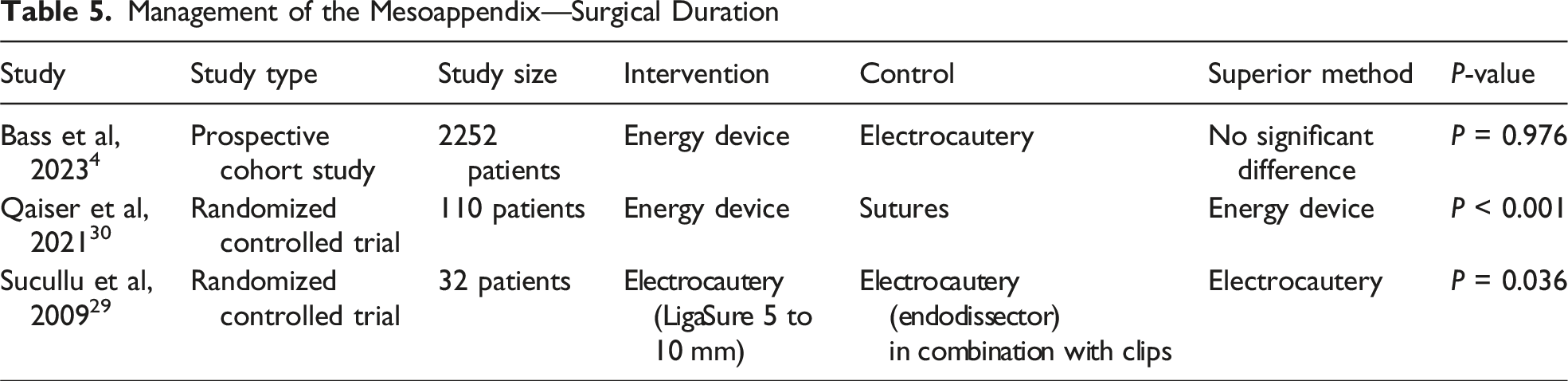
Management of the Mesoappendix—Surgical Duration
Length of Stay
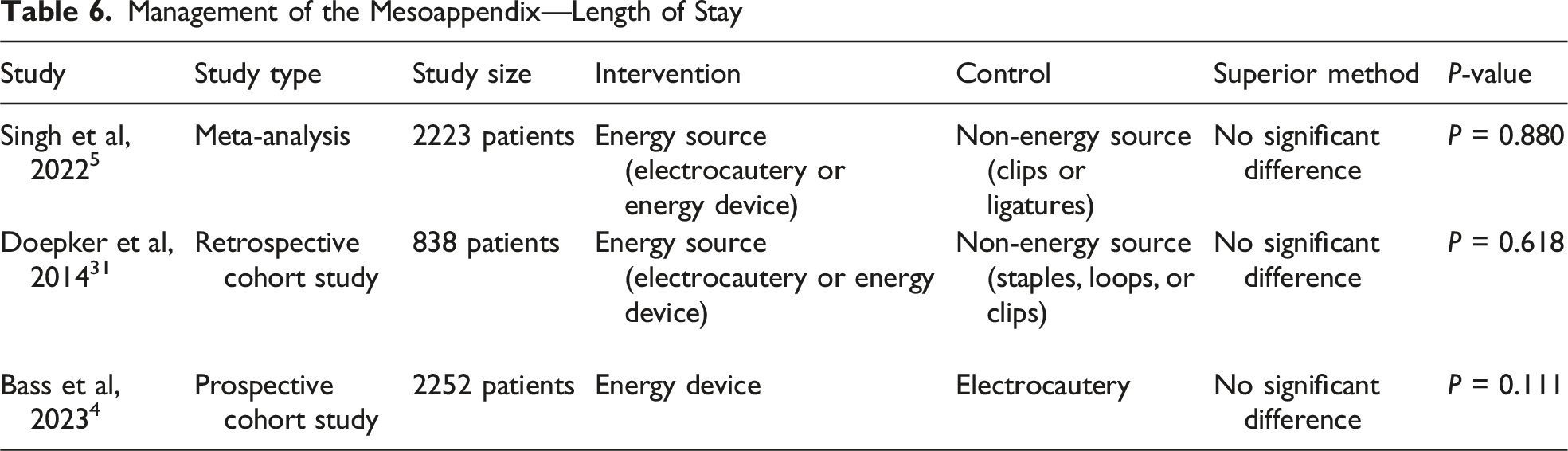
Management of the Mesoappendix—Length of Stay
Cost-Effectiveness
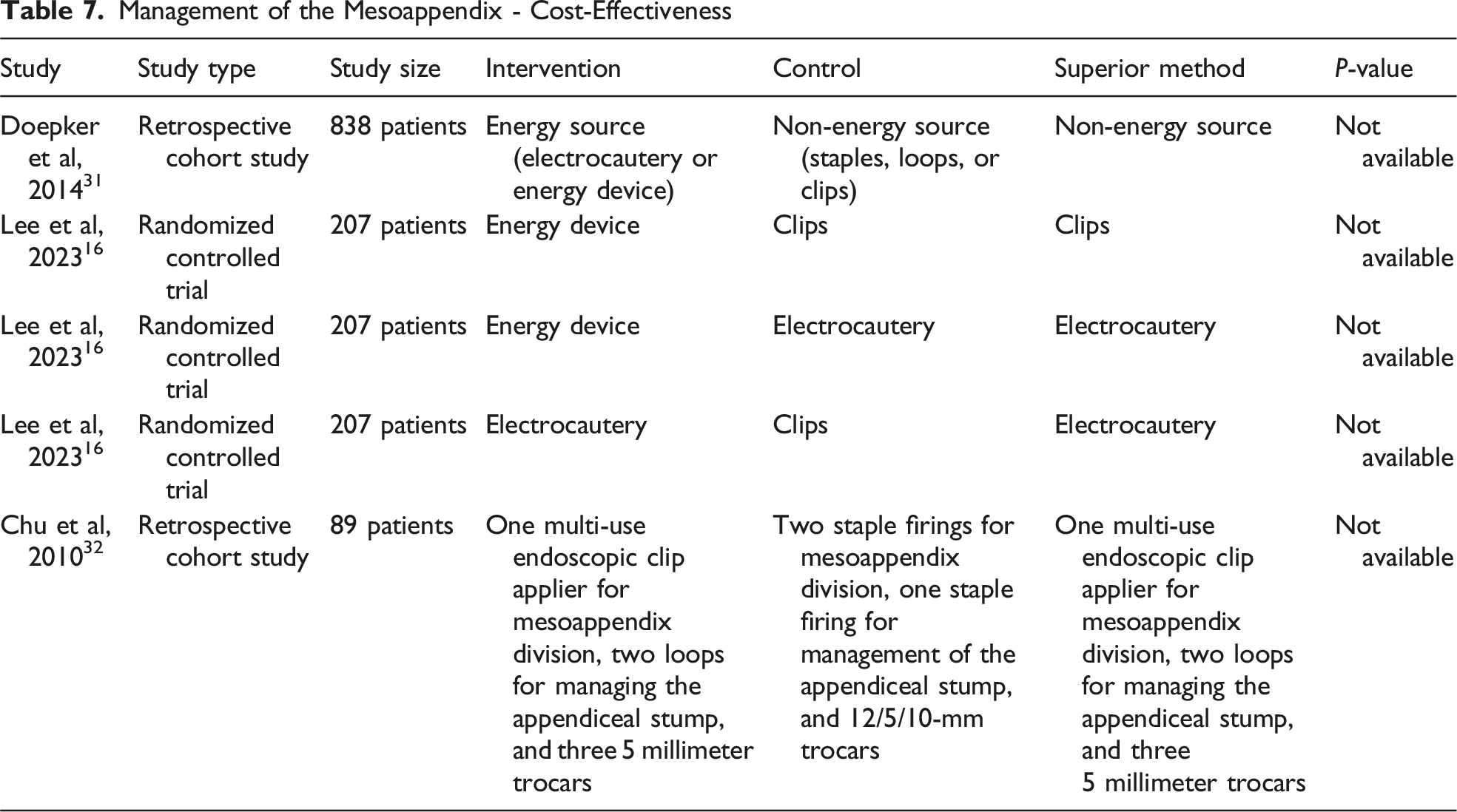
Doepker et al (2014) identified a significant cost disparity between energy sources (electrocautery and energy devices) and non-energy techniques (staples, loop ligatures, or clips), with energy devices adding approximately $700-1000 per case due to device expenses. 31 Lee et al (2023) found mean costs of $959 for the energy devices, $571 for clips, and $452 for electrocautery. 16 Chu et al (2011) also showed wide cost variation depending on surgeon’s choice of technique: the most economical surgeon used 1 multi-use endoscopic clip applier for mesoappendix division, 2 loops for managing the appendiceal stump, and three 5 millimeter trocars, equivalent to $299, whereas the least economical relied on 2 staple firings for mesoappendix division, 1 staple firing for management of the appendiceal stump, and 12/5/10-mm trocars, corresponding to $552. 32
Management of the Mesoappendix - Cost-Effectiveness
Complications
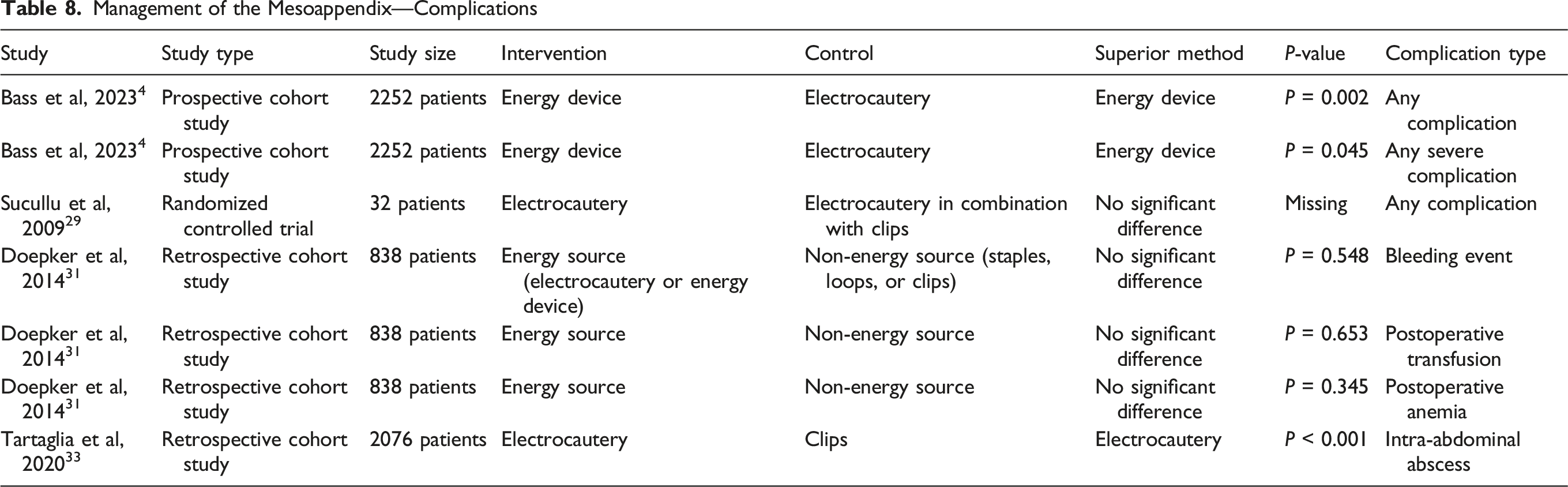
Management of the Mesoappendix—Complications
Discussion
Evidence regarding the effect of appendiceal stump closure technique on surgical duration remains inconsistent. Several studies, including randomized controlled trials (RCTs) and meta-analyses,15,17 found no significant difference between clips and loops,4,15-17,19,34 clips and staples,17,35,36 loop ligatures and staples,22,34,37 sutures and loop ligatures, 17 sutures and clips, 17 or sutures and staples. 17 Conversely, other investigations, including a randomized controlled trial and 2 meta-analyses,6,10,14 demonstrated that loop ligatures were slower than clips,10,12-14,38-40 staples,6,24 and energy devices 41 ; sutures exhibited similar delays.9,36,38 Bass et al (2023) and Galatioto et al (2013), however, reported the opposite trend, with loop ligatures being faster than staples.4,42 This discrepancy may be attributable to study design, as the observational nature of these studies and lack of case-selection data suggest potential bias. Staples may have also been reserved for more complex cases.
For mesoappendix division, electrocautery and energy devices appear superior to clips, loops, and sutures, with respect to surgical duration, as supported by 2 RCTs and 1 meta-analysis.29,30 However, Bass et al (2023) observed no significant difference between electrocautery and energy devices after adjusting for confounders. 4 Future research should prioritize patients with complicated appendicitis, since most current evidence, derived primarily from uncomplicated cases, demonstrates minimal differences in key outcomes across devices. Trials focusing on complicated cases are more likely to determine whether specific techniques provide meaningful clinical advantages in settings where inflammation, contamination, and anatomical challenges may affect device performance.
Findings regarding the correlation between appendiceal stump closure technique and total hospital stay are similarly heterogeneous. Several studies detected no association between closure technique and hospital LOS.6,9,10,15,20 Among studies reporting differences, clips were generally associated with the shortest LOS,4,21,36,40 whereas staples were associated with longer LOS compared with clips and loops.4,21 Comparative evidence regarding sutures, electrocautery, and energy devices remains limited. 43 For mesoappendix division, no significant differences in LOS were identified among any techniques.4,31
Most studies identified clips as the most cost-effective method for appendiceal stump closure,20-22,44-47 while staples consistently represented the most expensive option.20,21,24,25,44,47-49 The cost of loop ligatures typically fell between these choices.20,22,25,26,46 For mesoappendix division, electrocautery was the least expensive technique, followed by staples or clips, with energy devices representing the most expensive option.16,31,32 However, several limitations affect the interpretation of these findings. Some comparisons in the source studies are inconsistently reported, a limitation that cannot be fully resolved without access to the underlying data. Cost-effectiveness results are also difficult to interpret across studies due to multiple currencies and nearly 2 decades of economic change. Converting all costs to a single standardized currency and year was not feasible, which inherently limits comparability and precision. Additionally, familiarity bias may have influenced outcomes, whereby results tend to favor operative techniques most routinely performed by the surgeons in each study. This well-recognized phenomenon in procedural research may further limit the generalizability of comparative findings.
Overall intra- and postoperative complication rates appear broadly comparable across most closure techniques.4,19,24,27,36,38,44,45,50-58 Among studies reporting differences, loop ligatures were associated with higher overall complication rates than staples.6,24,28,59 In a meta-analysis of RCTs, Antoniou et al (2017) found that clips were linked to a greater incidence of surgical site infections compared with loops and sutures. 7 Additionally, 2 studies showed an increased risk of organ/space infections and intra-abdominal abscesses with loops compared to clips.7,60
For mesoappendix division, most studies reported no significant differences in bleeding, transfusion requirement, postoperative anemia, infection rate, or reoperation frequency across techniques.4,29,31 Nevertheless, Bass et al (2023) found electrocautery to be associated with higher rates of overall and severe complications compared to energy devices after adjustment for confounders. 4 Tartaglia et al (2020) reported that clips were more frequently correlated with intra-abdominal abscesses compared to electrocautery. 33
Recent innovations in appendiceal stump closure, minimally invasive access, and digital integration are advancing appendectomy toward greater efficiency, safety, and patient-centered care. A 2025 meta-analysis comparing single-incision (SILA) and conventional laparoscopic appendectomy (CLA) found no significant differences in hospital stay, surgical duration, or complication rates, confirming both as viable options. 61 Another randomized trial comparing a modified single-port approach using needle-type grasping forceps (mSLAN) with conventional three-port laparoscopic appendectomy demonstrated comparable short-term outcomes and surgical duration but superior cosmetic results, supporting its potential for wider clinical use. 62
Indocyanine green (ICG) fluorescence angiography (FA) provides real-time visualization of tissue perfusion, improving intraoperative assessment and surgical decision-making. 63 Zorzetti et al (2023) showed that ICG-FA reliably evaluates appendiceal stump vascularization, allowing perfusion-guided adjustments that may reduce postoperative complications. 63 Moreover, robotic-assisted appendectomy has emerged as a feasible alternative to conventional laparoscopy. Comparative studies report equivalent safety and efficacy, though robotic procedures may offer shorter hospital stays and faster recovery at higher cost and with longer surgical duration.64,65
Digital technologies further enhance perioperative care. Artificial intelligence models now outperform traditional methods in predicting postoperative complications, mortality, and wound-related events, as highlighted in a 2025 BJS abstract. 66 Deep learning–based approaches for surgical instrument annotation also show promise in improving intraoperative precision, surgical training, and overall patient outcomes. 67
As value-based healthcare gains focus, comprehensive cost evaluation has become integral to surgical innovation. While clips remain the most economical option for appendiceal stump closure and staples the most expensive, such comparisons overlook total procedural costs. Time-Driven Activity-Based Costing (TDABC) provides a more complete framework, encompassing surgical duration, personnel, anesthesia, and instrument reprocessing. A pediatric TDABC study reported a mean total cost of $2753.39 per case, primarily driven by personnel and operating room expenses. 68 Efficiency improvements were linked to triage-based delegation, advanced practice provider integration, and same-day discharge. No comparable adult analyses exist, but similar evaluations could identify opportunities for cost and resource optimization through standardization, scheduling, and staffing strategies. Incorporating sustainability metrics, such as carbon footprint, waste reduction, and device reusability, will further align appendectomy practices with economic and environmental efficiency.
Conclusion
Appendiceal stump closure and mesoappendix division can be performed using various techniques, and instruments, each offering distinct advantages depending on the outcome assessed. While this review outlines important differences in specific perioperative and postoperative outcomes, the available evidence does not allow for firm recommendations at this stage. No single technique emerges as universally superior. Consequently, decisions should be individualized, with surgeons, and institutions weighing operative efficiency, cost, and complication risk in the context of their own experience, patient characteristics, and local resources.
Supplemental Material
Supplemental material - Techniques for Mesoappendix Division and Appendix Resection: A Comparative Review
Supplemental material for Techniques for Mesoappendix Division and Appendix Resection: A Comparative Review by Lovisa Ekestubbe, MD, Maximilian P. Forssten, MD, Sebastian P. Forssten, MD, Gary A. Bass, MD, MSc, MBA, PhD, Yousef AlHussaini, MD and Shahin Mohseni, MD, PhD in The American Surgeon
Footnotes
Author Contributions
Conception and Study Design: Lovisa Ekestubbe, Maximilian P. Forssten, Gary A. Bass, Shahin Mohseni; Literature Review: Lovisa Ekestubbe, Maximilian P. Forssten, and Yousef AlHussaini; Data Acquisition: Lovisa Ekestubbe and Maximilian P. Forssten; Data Analysis and Interpretation: Lovisa Ekestubbe, Maximilian P. Forssten, and Sebastian P. Forssten; Drafting of the Manuscript: Lovisa Ekestubbe, Maximilian P. Forssten, and Gary A. Bass; Critical Revision: Sebastian P. Forssten, Yousef AlHussaini, and Shahin Mohseni.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online.