
Abstract
Extracorporeal membrane oxygenation (ECMO) manages critical cardiac and pulmonary conditions. We hypothesized that ECMO utilization in trauma patients would result in overall favorable outcomes and sought to evaluate the factors leading to survival. We conducted a 10-year retrospective study at our Level One trauma center, including all adolescent and adult patients with traumatic injuries undergoing ECMO. We performed descriptive statistics and univariate analyses comparing survivors and non-survivors. Of the 28 patients who met our inclusion criteria, 42.9% survived. Non-survivors were cannulated on ECMO sooner and had a worse base deficit at time of cannulation. Most survivors discharged home (25%) or to a rehabilitation center (41.7%). High mortality in this population reveals the importance of understanding and following a standard selection criteria when cannulating trauma patients on ECMO. Further investigation is needed to evaluate what makes trauma patients appropriate to be cannulated on ECMO.
Polytrauma is a leading cause of mortality and continues to persist as a global public health issue. 1 One way to treat critical injury resulting in refractory respiratory and pulmonary issues is the utilization of extracorporeal membrane oxygenation (ECMO), a life support device which functions by oxygenating venous blood outside of the body and returning it through a pump. While ECMO utilization has been widely studied, 2 there is a paucity of literature regarding its use in trauma patients, and the benefits it may provide. We sought to evaluate the factors which contributed to survival in trauma patients who underwent ECMO cannulation. We hypothesized that specific variables could elucidate the effectiveness of ECMO use in trauma patients prior to cannulation, and that identifying these factors would be associated with survival among this population.
We conducted a 10-year retrospective analysis (7/1/2014-7/1/2024) of adult trauma patients who underwent ECMO at our level 1 Trauma Center. All mechanisms of injury were included. Descriptive statistics were conducted to summarize demographic variables and clinical outcomes. Univariate analyses were performed to compare survivors to patients who died to further investigate the factors associated with survival. A P-value <0.05 was considered statistically significant. All data analyses were performed using Stata statistical software v.16.
There were 28 patients who met inclusion criteria for the study and 42.9% (n = 12) survived. Of those patients, 22 (78.57%) sustained blunt injuries. Predominant mechanisms of injury were motorcycle collision (n = 9 [32.14%]) and fall (n = 8 [28.57%]). Veno-venous (VV) (16 [57.11%]), veno-arterial (VA) (4 [14.3%]), and extracorporeal cardiopulmonary resuscitation (eCPR) (8 [28.6%]) modalities were included. Most survivors utilized VV ECMO (10 [62.5%]). All patients utilizing eCPR and half of the patients utilizing VA ECMO died. Extracorporeal cardiopulmonary resuscitation patients were cannulated on ECMO faster than their non-eCPR counterparts (eCPR: .867 hour [.567-1.9], non-eCPR: 74.41 hours [12.46-220.78], P = 0.0002) and were cannulated for a shorter period (eCPR: 13.31 hours [SD: 2.94-30.63], non-eCPR 113.65 [50.29-321.58] P = 0.0014) and 75% of eCPR died within 60 hours of arrival to the hospital.
A pre-ECMO creatinine of <1.2 mg/dL was associated with survival (survivors: 11 [91.67%] v dead: 1 [7.14%], P < 0.001). Lactate levels (survivors: 2.5 mmol/L [Interquartile Range [IQR] .9-5.6] v dead: 4.8 mmol/L (IQR: 3-9.3 [P = 0.055]) were not significant but there was a significant difference in pH levels (survivors: 7.36 (IQR: 7.31-7.40) v dead: 7.23 (IQR: 7.11-7.28) [P = 0.018]) between survivors and those who died. Additionally, while there was no significant difference found in our study, survivors were younger than those who died (survivors: 27.5 years (IQR: 21.5-43.5) v dead: 33.5 years (IQR 23-52.5), [P = 0.070]).
Demographics of outcomes of patients by mortality
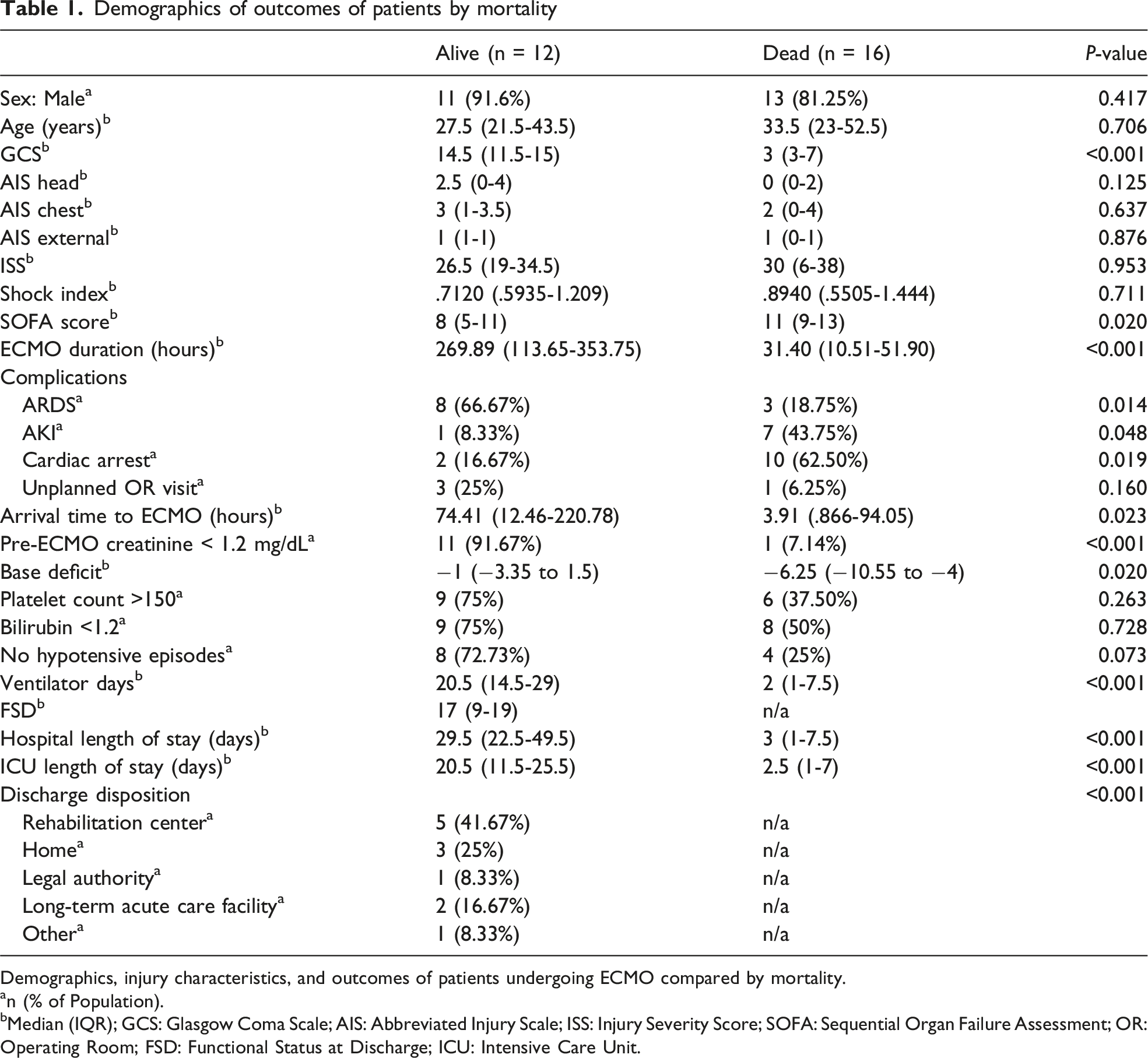
Demographics, injury characteristics, and outcomes of patients undergoing ECMO compared by mortality.
an (% of Population).
bMedian (IQR); GCS: Glasgow Coma Scale; AIS: Abbreviated Injury Scale; ISS: Injury Severity Score; SOFA: Sequential Organ Failure Assessment; OR: Operating Room; FSD: Functional Status at Discharge; ICU: Intensive Care Unit.
Despite a mortality rate of 57.1% (n = 16) in our study, over two-thirds of survivors were discharged to rehabilitation centers or home, suggesting meaningful survival in select cases. Of note, the survival rate in our study was lower than that of similar studies exploring the clinical use of ECMO in trauma patients.2-4 The study by Abate et al carefully considered criteria such as age and comorbidities prior to cannulation. This only further supports our hypothesis that selection criteria and timing to cannulation may be the key feature of survivability in trauma patients utilizing ECMO. Early cannulation on ECMO in our patient population indicated critical physiologic deterioration. Further, most eCPR patients died within 60 hours of arrival to the hospital and were cannulated sooner than those who did not undergo eCPR. A worse base deficit upon cannulation in those who died may be due to worsened ongoing shock which could not be mitigated by ECMO. In fact, a worsened base deficit may prove refractory despite ECMO cannulation.2,3 Base deficit and other surrogates for shock are crucial values for providers to consider when deciding whether to utilize ECMO. Additionally, early ECMO initiation was associated with increased mortality, which could reflect a patient’s increased physiological compromise upon arrival to the hospital.
These findings are echoed in larger studies wherein ECMO was used to treat younger patients with fewer comorbidities.3,4 The data in our study may indicate that the high mortality rate is a result of poor selection. A lack of standard guidelines can create a challenge for providers, leading them to make these critical decisions on a case-by-case basis. 3 Historically, the primary criteria for ECMO selection at our level 1 trauma center is a PaO2/FiO2 less than 100 for 6 hours or more, on maximum ventilator settings. However, there are other criteria that should be considered for ECMO use such as comorbid conditions and age. Age was not a significant variable in our study but, typically, younger patients have greater physiologic resilience. The lack of bleeding, cardiac, and renal complications among survivors in our study indicates that survivors were likely healthier at baseline. These findings were reflected in a study by Zhang et al who utilized ECMO as a supportive therapy upon careful consideration of patient symptoms and physiology, evidenced by survivors having more favorable lab values prior to cannulation. 3 A more comprehensive protocol surrounding cannulation could assist in the refinement of selection criteria of those trauma patients who may benefit from ECMO.
This study had multiple limitations, the most significant being its small sample size. The crucial conclusion we have come to demonstrates the need to re-assess, refine, and closely follow a clinical selection standard when considering ECMO as a treatment for severely injured trauma patients. Our study suggests that those who survived after ECMO cannulation had favorable outcomes upon discharge. Additionally, it suggests the need to create a standard process outlining variables which may impact survival rates among this population. Further research is needed to definitively determine these variables but considering timing to cannulation, comorbidities, and shock status may provide a solid foundation for predicting survivability in this population.
Footnotes
Author Note
This study was presented as a quickshot presentation at the 2026 Southeastern Surgical Congress Annual Meeting on February 22nd, 2025.
Author Contributions
MA was involved with statistical analysis, data collection, and writing. ILF was involved with data collection. JMR was involved with statistical analysis and writing. AT was involved in data collection. EB was involved with generation of the study idea. LLP was involved with generation of the study idea and writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.