
Abstract
Circulating C-reactive protein (CRP), reflective of systemic chronic low-grade inflammation, is a marker associated with cardiovascular disease (CVD). One of the mechanisms through which physical activity might promote cardiovascular health is by preventing changes in inflammation biomarkers, such as CRP. The present study examined the association of self-reported physical activity with an inflammation biomarker, high-sensitivity CRP (hs-CRP), in a population-based cohort of clinically healthy 58-year-old men. Compared with a sedentary lifestyle both moderate (1.81 [0.94-3.69] vs 1.28 [0.55-2.90] mg/L; P < .05) and vigorous physical activity (1.81 [0.94-3.69] vs 0.88 [0.42-1.81] mg/L; P < .001) were associated with decrease in hs-CRP levels. In summary, we identified an association between self-reported leisure time physical activity and hs-CRP in a cross-sectional study of healthy 58-year-old men, with decreased levels of CRP by increased intensities of physical activity.
Introduction
Circulating C-reactive protein (CRP), reflective of systemic chronic low-grade inflammation, is a marker associated with cardiovascular disease (CVD). 1 Baseline levels of CRP predict risk of future myocardial infarction, stroke, and peripheral atherosclerosis in healthy middle-aged men. 2 Further, the concentrations of CRP are reported to be affected by several lifestyle habits, such as smoking and physical activity. 1
Physical activity has been shown to be inversely linked to several CVD risk factors, such as high-density lipoprotein cholesterol (HDL-C) concentration, blood pressure, body mass index, glucose intolerance, and fibrinolytic activity. 3 Our research group has previously observed, in an initially healthy cohort of middle-aged men, that self-reported leisure time physical activity (LTPA) is associated with lower apolipoprotein (apo)B/apoA-I ratios 4 as well as with decreased prevalence of the metabolic syndrome, 5 which are both known as risk factors for CVD.
The cardiovascular protective effects of physical activity are most likely conferred by a number of mechanisms. One of the mechanisms through which physical activity might promote cardiovascular health is by reducing inflammation as seen by reductions in inflammatory biomarkers, such as CRP. 6 A number of articles have documented that self-reported physical activity or physical performance is inversely correlated with CRP, 6–9 although lack of association has also been reported, especially when adjusted for other factors. 9
The present study examined the association of self-reported physical activity with an inflammation biomarker, high-sensitivity CRP (hs-CRP), in a population-based cohort of clinically healthy 58-year-old men.
Material and Methods
Study Population and Study Design
From a total population sample of 58-year-old 1728 men, a stratified and randomly selected group with varying degrees of obesity and insulin sensitivity (n = 391) were included, as described previously. 10
All participants were of Swedish ancestry and lived in the Gothenburg region. Exclusion criteria were CVD, clinical diabetes mellitus, or other clinically overt disease, treatment with cardiovascular drugs (which might disturb the measurements performed in the study), and unwillingness to participate.
The participants received both written and oral information before they gave their consent to participate. The ethics committee at Sahlgrenska University Hospital approved the study.
Measurements
Previously described questionnaires were used to evaluate history of previous and current disease, smoking habits, and alcohol consumption. 10 A self-administered questionnaire was used to assess the level of LTPA. The total number of smoking years was multiplied by the number of cigarettes smoked daily and the product was termed “cigarette years.” 10
Body weight, waist and hip circumference, and sagittal abdominal diameter, that is, the distance from the back to the upper abdomen, midway between the top of the pelvis and the bottom of the ribs, measured in a supine position, were measured with participants dressed in underwear. Blood pressure (BP) was measured twice after 5 minutes supine rest. Heart rate was recorded from a 12-lead standard electrocardiogram (ECG).
Venous blood samples were drawn after a fasting period of at least 6 hours. Cholesterol and triglyceride levels were determined by enzymatic techniques (Thermo Clinical Labsystems, Espoo, Finland). High-density lipoprotein cholesterol was determined after precipitation of apoB-containing lipoproteins (Thermo Clinical Labsystems) and low-density lipoprotein cholesterol (LDL-C) was calculated as described by Friedewald et al. 11 High-sensitivity CRP was measured at the Wallenberg Laboratory, Göteborg, Sweden, with an ultrasensitive method using particle-enhanced immunoturbidimetry (Orion Diagnostica, Espoo, Finland).
Apolipoproteins (apoA-I and apoB) were measured on a Konelab 20 Auto-analyzer (Thermo Scientific, Vantaa, Finland) using a turbidimetric method. Using 2 different controls, the between-assay variation for repeated measurements have been shown previously 12 to be 5.2% and 5.8% for apoA-I and 2.5% and 3.2% for apoB, respectively. Corresponding figures within assay variation have shown to be 1.4% and 1.7% for apoA-I and 1.4% and 1.4% for apoB, respectively. 12
The study participants were divided into 3 groups according to their level of LTPA as described previously.
4
Sedentary lifestyle: spends leisure time mostly reading, watching TV, or other sedentary activities. Moderate physical activity: walking, cycling, or other mild physical activities such as gardening, fishing, or bowling at least 4 h/week Vigorous physical activity: running, swimming, tennis, cross-country skiing, or other exercise that leads to sweating several days per week.
This questionnaire has been evaluated in the Malmö Diet and Cancer study, Sweden.
13
Statistics
All statistics were performed using SPSS 17.0 for Windows. Results are presented as mean ± standard deviation (SD) unless otherwise indicated. The Mann-Whitney U test was used to compare continuous data. Comparison of nominal data was performed using Pearson chi-square test. The sedentary activity group was used as reference in the analyses. Multiple regression analysis was used in the covariance analyses. A P < .05 (2-sided) was considered significant.
Results
The characteristics of the participants divided into groups according to their level of LTPA are shown in Table 1 and has previously been described. 4 In brief, increasing levels of physical activity were inversely associated with waist circumference, waist–hip ratio, heart rate, serum insulin, triglycerides, hs-CRP, apo B, apo B/apo A-I ratio, and cigarette years, while HDL-C and apo A-I showed a positive association.
Characteristics of the Study Participants by Leisure Time Physical Activity

Abbreviations: LDL, low-density lipoprotein; HDL, high-density lipoprotein; ApoB, apolipoprotein B; ApoA-I, apolipoprotein A-I; bpm, beats per minute.
a P < .01 compared with sedentary lifestyle; Mann-Whitney U test.
b P < .05 compared with sedentary lifestyle; Mann-Whitney U test.
c P < .001 compared with sedentary lifestyle; Mann-Whitney U test.
d Geometric mean.
e Median (interquartile range).
Compared with a sedentary lifestyle both moderate physical activity and vigorous physical activity were associated with lower hs-CRP levels (1.81 mg/L [0.94-3.69] vs 1.28 mg/L [0.55-2.90]; P < .05) and (1.81 mg/L [0.94-3.69] vs 0.88 mg/L [0.42-1.81] P < .001), respectively (Figure 1 ). Table 2 shows the results from a regression analysis to explore possible covariates. Further, the regression analysis of hs-CRP according to physical activity adjusted for cigarette years, waist–hip ratio, serum insulin, and apo A-I showed that physical activity was significantly and independently associated with hs-CRP (β = −.189, P = .016).
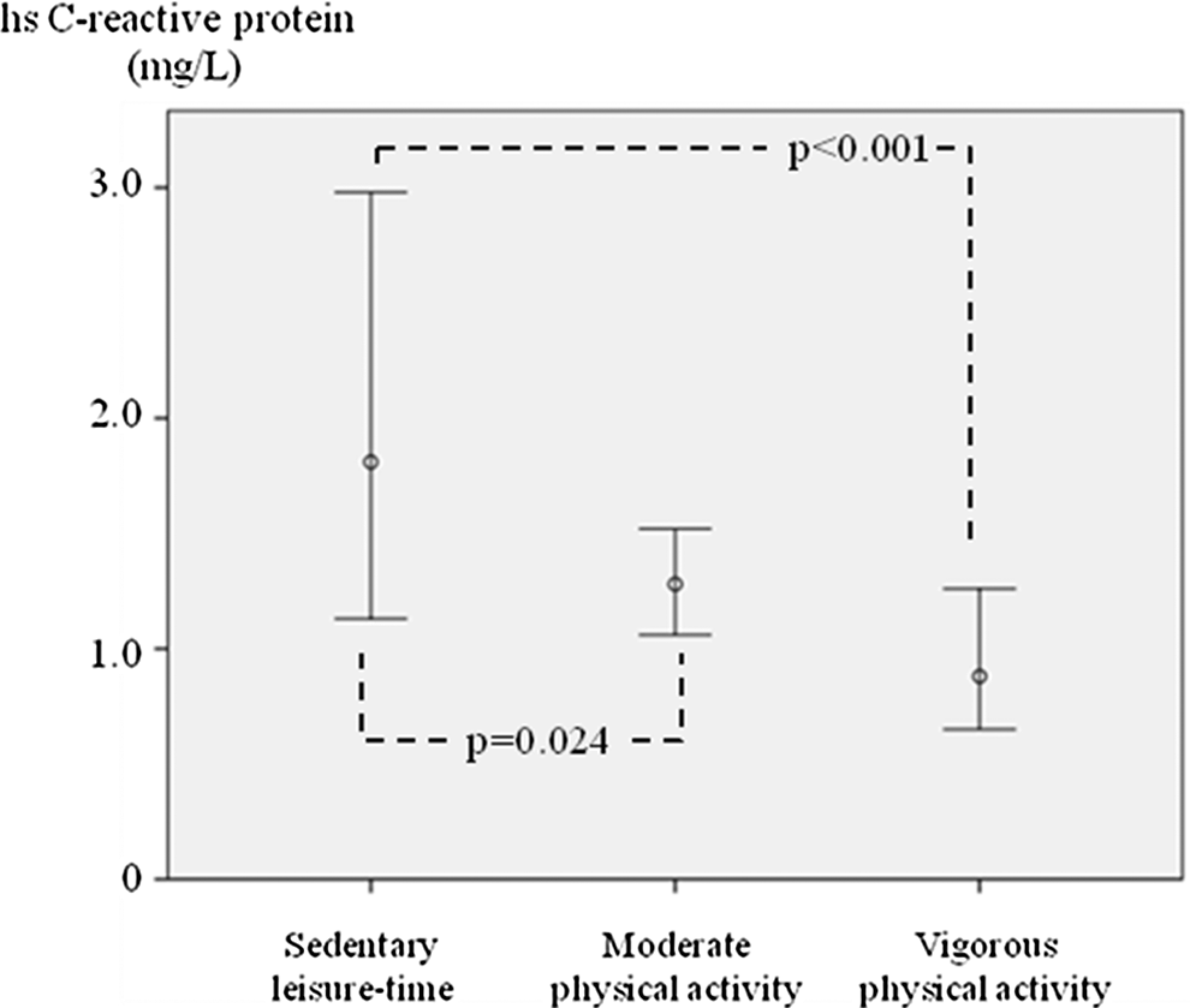
Simple bars illustrating median values of high-sensitivity C-reactive protein by groups of leisure time physical activity. The error bars represent 95% confidence interval. Mann-Whitney U test was used for the significance test.
Results From Multivariate Regression Analysis of CRP According to Physical Activity
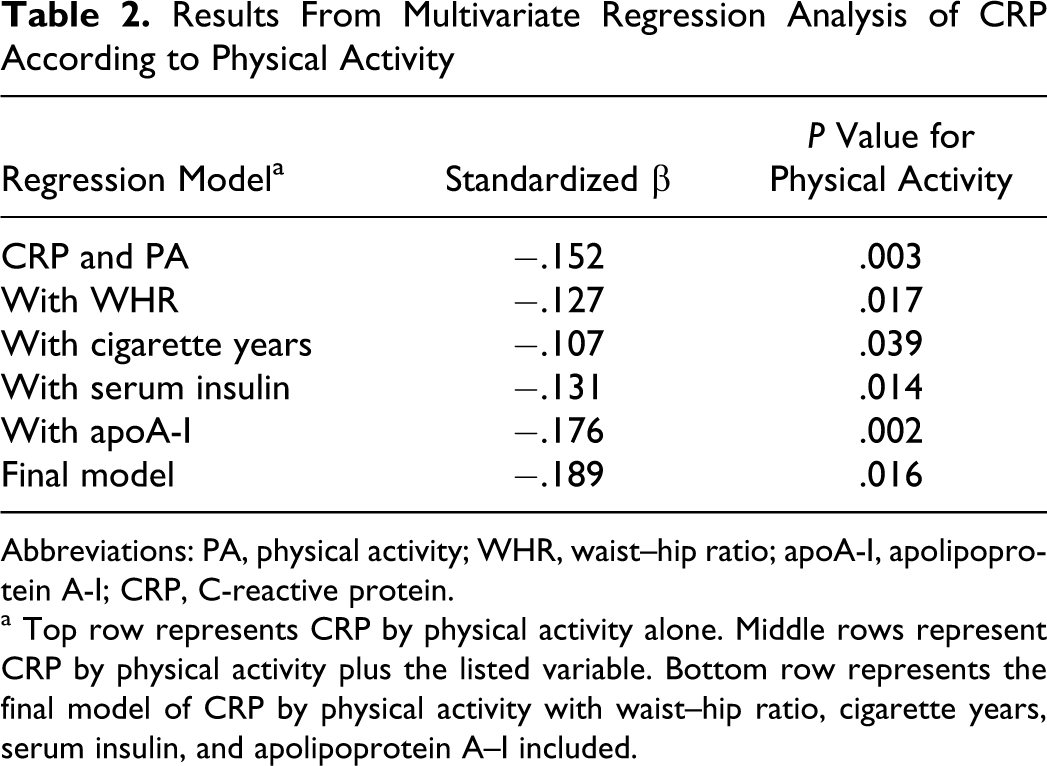
Abbreviations: PA, physical activity; WHR, waist–hip ratio; apoA-I, apolipoprotein A-I; CRP, C-reactive protein.
a Top row represents CRP by physical activity alone. Middle rows represent CRP by physical activity plus the listed variable. Bottom row represents the final model of CRP by physical activity with waist–hip ratio, cigarette years, serum insulin, and apolipoprotein A–I included.
Discussion
The main finding in this cross-sectional study in clinically healthy middle-aged men was an inverse relationship between hs-CRP and self-reported LTPA. The relationship was observed both before and after adjustments for covariates such as waist–hip ratio, cigarette years, and serum insulin. In addition, hs-CRP levels showed positive association with physical activity already at moderate levels, such as walking, cycling, gardening, or bowling. Inverse relationships between hs-CRP and self-reported activity levels have been demonstrated earlier. 8,14
Assuming that physical activity reduces inflammation, which mechanisms bring about this effect? Obesity is a factor that is strongly related to increased levels of CRP, 8 and it has been suggested that physical activity may reduce inflammation by decreased levels of obesity. 8 In the present study, waist–hip ratio, a measure of abdominal obesity, was inversely associated with physical activity. However, the multivariate analysis showed that physical activity was independently associated with decreased levels of hs-CRP also after adjustment for central obesity. This suggests that physical activity influences the inflammatory process not solely by reductions in obesity. 14
Further, physical activity has been shown to decrease insulin resistance, which suggests that improved insulin sensitivity associated with physical activity would also be associated with lower levels of inflammation. 8 In our study, we observed that serum insulin concentration was inversely associated with physical activity. In the multivariate analysis, when high-sensitivity CRP by physical activity was adjusted for serum insulin, physical activity was still independently associated with hs-CRP.
Exercise raises the level of HDL-C, which has been shown to neutralize the proinflammatory effect of CRP. 15 However, apoA-I is the major apolipoprotein in HDL and has been shown to be the most important determinant of the HDL level. 16 There are a few studies that have shown an inverse relationship between apoA-I and CRP. 17,18 In this cohort of men, we have previously observed an association between physical activity and apoA-I, with increasing apoA-I levels by increased intensities of physical activity. 4 Nevertheless, in the present study, physical activity was shown to be independently associated with hs-CRP also after adjustment for apoA-I. These results support the concept that the cardiovascular protective effects conferred by physical activity most likely works through a range of mechanisms.
This study has limitations. First, because of a cross-sectional design, therefore we cannot establish the long-term associations. Second, we used a single measurement of hs-CRP, which may not accurately reflect long-term low-grade inflammatory status.
However, there are also advantages of a cross-sectional study that have been mentioned previously. 4 Briefly, the studied variables are assessed at the same time of measurement, and therefore bias owing to variations between the studied variables is ruled out. While no causation can be inferred from a cross-sectional study, our results suggest that increased exercise is associated with reduced inflammation as measured by hs-CRP.
In summary, we identified an association between self-reported LTPA and hs-CRP in a cross-sectional study of healthy 58-year-old men, with decreased levels of hs-CRP by increased intensities of physical activity. Importantly, a favorable association between LTPA and hs-CRP was observed already at moderate levels of physical activity, supporting the concept that some activity is better than none.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grants from the Swedish Heart–Lung Foundation, the Swedish Medical Research Council (12270 and 10880), King Gustaf V and Queen Victoria’s Foundation, and Astra Zeneca, Mölndal, Sweden, supported this work.