
Abstract
Endovascular abdominal aortic aneurysm (AAA) repair (EVAR) procedures require lifelong patient surveillance for the detection of complications (eg, endoleaks or graft migration). This follow-up may be suboptimal. Between November 2010 and November 2011, a follow-up booklet was provided at hospital discharge to 42 consecutive patients undergoing EVAR for an infrarenal AAA. Each patient was given specific instructions for completion of the booklet at each follow-up examination whether this took place at our hospital or elsewhere. After a mean follow-up of 7 ± 3 months, all patients had fully complied with the instructions. This booklet may be useful for patients who find it difficult to attend follow-up appointments. Additionally, this booklet is useful for patients who move to another town/country or in cases of emergency when patients are admitted to another hospital.
Introduction
With the introduction of endovascular abdominal aortic aneurysm (AAA) repair (EVAR) procedures, the management of AAAs has undergone a “profound and sustained paradigm shift” 1 ; EVAR is nowadays used for the treatment of the majority of infrarenal AAAs. 1 A drawback of EVAR is the development of endoleaks which mandates the need for lifelong patient surveillance.
The follow-up surveillance of EVAR patients is often suboptimal. For example, in the European Collaborators on Stent-Graft Techniques for AAA and Thoracic Aortic Aneurysm and Dissection Repair (EUROSTAR) trial, only 1538 (35%) of the 4433 EVAR patients presented for all scheduled appointments. 2 The follow-up surveillance of EVAR patients in practice environments outside clinical trials may also be suboptimal. 3 Patients with incomplete follow-up have a severalfold higher incidence of major vascular events requiring urgent surgical intervention compared with patients with complete follow-up (6.1% vs 0.5%, respectively; P = .006), with many of these patients dying perioperatively. 3
We present a simple booklet that makes post-EVAR follow-up easier both for patients and for physicians not directly involved in the initial EVAR procedure.
Materials and Methods
Between November 2010 and November 2011, all consecutive patients (n = 42) undergoing EVAR for an infrarenal AAA in the Department of Vascular Surgery, “Konstantopoulio” General Hospital, Athens, Greece, were recruited in our study.
The details of the procedure and the need for lifelong follow-up surveillance were explained to all patients. After the procedure and prior to hospital discharge, each patient was given a booklet consisting of 16 pages. The name of the treating physician, his or her telephone numbers, and e-mail address were entered in the first page (Figure 1A) of the booklet. The characteristics of the patient’s AAA (eg, diameter, involvement of the iliac arteries, etc), the date, and a brief description of the procedure were described on page 2 (Figure 1B). The details of the device used, as well as any possible additional stent-grafts required were filled in the third page (Figure 1C). The results of the immediate post-EVAR clinical, laboratory, and imaging examinations, as well as the drugs prescribed at hospital discharge were entered in page 4 (Figure 1D). It was explained to the patients that each of the next 12 pages (Figure 1E) should be completed at the time of each follow-up examination. The patient should carry the booklet with him or her for the details of each follow-up examination and possible complications (eg, detection of endoleaks, persistent increase in AAA size, possible graft migration, etc) to be recorded. The date for the next scheduled follow-up appointment was also indicated.
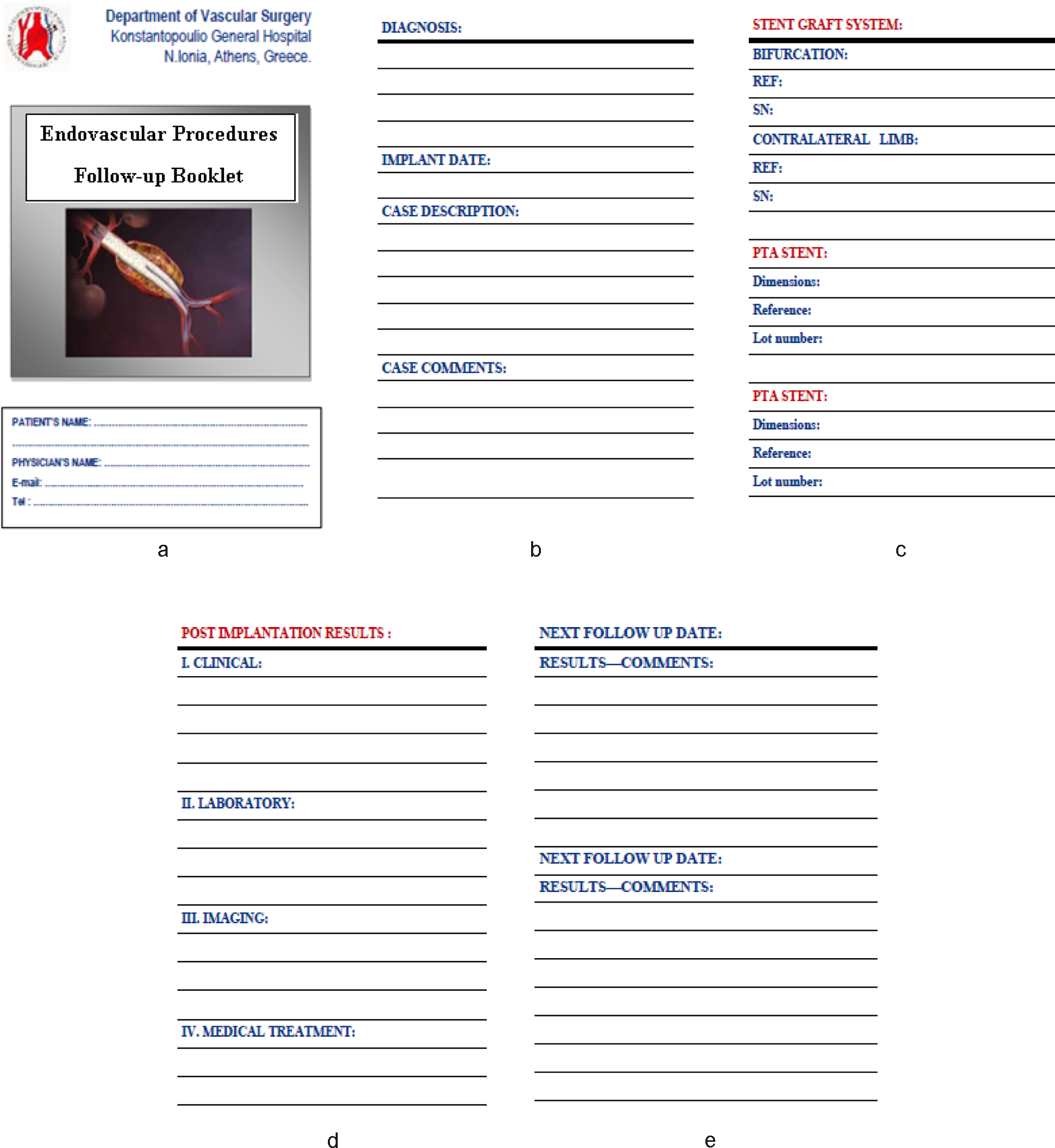
A, Page 1 of the follow-up booklet including the name of the treating physician, his or her telephone numbers, and e-mail address. B, Page 2 of the follow-up booklet including the characteristics of the patient’s AAA (eg, diameter, involvement of the iliac arteries, etc), the date, and a brief description of the procedure. C, Page 3 of the follow-up booklet including the details of the device used and any possible additional stent grafts required. D, Page 4 of the follow-up booklet including the results of the immediate post-EVAR clinical, laboratory, and imaging examinations, as well as the drugs prescribed at hospital discharge. E, Pages 5 to 16 of the booklet have the details of each follow-up examination to be completed. AAA indicates abdominal aortic aneurysm; EVAR, Endovascular abdominal aortic aneurysm repair.
During each follow-up examination, the vascular risk factors should also be recorded (ie, smoking status, hypertension, diabetes mellitus, and lipid levels). Abdominal aortic aneurysms are coronary heart disease equivalents. 4 –6 Appropriate measures for optimal risk factor management should thus be reinforced to reduce mortality and morbidity rates in these patients.
Results
During the study period, a total of 42 patients (39 males and 3 females; mean age: 71.8 years) underwent an EVAR procedure at our institution for an infrarenal AAA (mean diameter: 6.4 cm; range: 5.2-10.4 cm). Three different devices were used: Endurant, Medtronic Inc, Minneapolis, Minnesota (n = 34); Zenith, Cook Indianapolis, Indiana (n = 6); and Excluder, W.L. Gore and Associates, Flagstaff, Arizona (n = 2). All procedures were performed successfully with 0% mortality. All patients were discharged on the third postoperative day.
All patients were scheduled for postoperative follow-up at 1, 6, 12 months, and yearly thereafter. After a mean follow-up of 7 ± 3 months, all patients have fully complied with the instructions for completion of the booklet.
Discussion
This preliminary report presents the details of a simple and practical booklet to optimize post-EVAR patient surveillance.
Many patients undergoing EVAR may live far from the hospital where their operation takes place or in assisted-living facilities. Furthermore, several patients are referred from other towns or villages. Many AAA patients are old and may have several health problems making it difficult for them to attend the follow-up appointments at the clinic where their EVAR procedure takes place.
In a retrospective study, a total of 136 EVAR patients were stratified as living within or outside a 100-mile radius of the treatment center. 7 The follow-up of these patients included clinic visits and computed tomography scans at 1 month after discharge, every 6 months for the first 2 years and yearly thereafter. After a mean follow-up of 52.1 ± 25.9 months, there was no difference in the adequacy of follow-up between patients in the 2 groups. The conclusion reached was that the distance from a tertiary care center is not a limiting factor for patient adherence to follow-up, patient graft-related morbidity, or patient survival. 7 However, it should be noted that 15% of the patients in each group had incomplete follow-up. Furthermore, and as mentioned earlier, surveillance in “real-world” clinical practice may be worse compared with that within trials. 3
With the use of the described booklet, EVAR patients do not need to attend the clinic where their operation took place for their scheduled follow-up. Furthermore, this booklet may be useful when a complication occurs (eg, AAA rupture) and the patients need to be admitted urgently to another hospital. A similar situation occurs when the patients move to another town or even to another country; the new managing physician gets informed of all the necessary details regarding the initial EVAR procedure, as well as the follow-up course of the patient until that point. Finally, the name, e-mail, and telephone numbers of the physician performing the initial EVAR procedure are provided if further information is required.
This booklet is not a substitute for the patient records. The information it contains is also stored in the database of our clinic. The advantage of this booklet is that the patient has a copy of the treatment and the follow-up he or she received. As mentioned above, this information may prove valuable on several occasions.
Conclusions
The introduction of a simple and practical booklet may help optimize patient follow-up surveillance after EVAR. This booklet may be useful for patients living far from the hospital their initial operation took place or for those unable for various health or other reasons to attend the scheduled follow-up appointments at the hospital where they were managed. Finally, this leaflet is useful for patients moving to another town/country or in cases of emergency when the patients are transferred to a hospital other than the one where the initial procedure took place. This booklet may potentially be used for the follow-up of patients undergoing any endovascular procedure.
Footnotes
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.