
Abstract
We evaluated the safety and efficacy of second-generation drug-eluting stents (DES) fully covering a coronary artery aneurysm (CAA) and stenosis lesion. Patients (n = 33) with CAA and stenosis lesion (>60%) were enrolled between January 2014 and December 2017. Baseline characteristics and biochemical variables were recorded during hospital admission. Changes in CAA resolution (the reduction on CAA size), minimal lumen diameter (MLD), and diameter stenosis (DS) were determined before, just after, and 1 year after percutaneous coronary intervention (PCI). After DES implantation, MLD and DS after PCI were improved compared with those before PCI (P < .01). Also, thrombolysis in myocardial infarction blood flow was significantly enhanced after PCI (P < .01). One year after PCI, maximal CAA diameter in patients with CAA and stenosis lesion was significantly reduced compared with those just after PCI (P < .01). Meanwhile, CAA resolution ratio in these patients were more than those just after PCI (P < .01). Furthermore, there was a significant reduction about CAA length in these patients (P < .01). Last, there were no clinical events (including cardiac death, myocardial infarction, and revascularization) in the study. Second-generation DES implantation fully covering CAA and stenosis lesion was safe and effective.
Introduction
Coronary artery aneurysm (CAA) has been defined as a focal expansion of a coronary artery segment, with a transverse diameter of the lesion segment 1.5 times larger than the normal adjacent segment, identified by coronary angiography (CAG) and/or intravascular ultrasound (IVUS).1,2 The first case of a CAA was reported by Bougon in 1812. 3 The incidence of CAAs fluctuates between 0.3% and 5.3%. 2 Causative factors include atherosclerosis, arteritis, congenital diseases, Kawasaki disease, and percutaneous coronary intervention (PCI). 2 Atherosclerotic CAAs (ACAAs) account for 73% to 90% of all CAAs in pathological autopsy series.4,5
Second-generation drug-eluting stents (DES) have a lower incidence of stent thrombosis, target vascular revascularization, major adverse cardiac events (MACEs), stent-related aneurysms than bare metal stents (BMS), and first-generation DES.6–9 The reason was that they improve the stent strut platform (thinner cobalt base alloy) and polymer (inert and noninflammatory). 10 No stent thrombosis was observed after 1 year in 6 patients with ST-segment elevation myocardial infarction (STEMI) caused by CAA with proximal or distal lesions and treated with everolimus-eluting stent. 11 This study just also showed the second-generation DES implantation was effective to treat severe stenosis lesions in these patients.
Coronary artery aneurysm can lead to thrombus formation, resulting in distal embolism and acute MI. 12 Also, CAA rupture can cause acute pericardial tamponade. 13 Until now, the medical interventional treatments of CAA include covered stent implantation, stent-assisted coiling, thrombectomy, intracoronary thrombolytics, and balloon angioplasty.2,14 However, their therapeutic effects have not yet been confirmed. Therefore, this retrospective study aimed to evaluate the safety and therapeutic effect of second-generation DES implantation to fully cover CAA and moderate or severe stenosis lesion.
Materials and Methods
During January 2014 to December 2017 in the Centre of Cardiology, Nanjing First Hospital (Nanjing, Jiangsu, China), 33 patients underwent CAG with confirmed CAA and moderate or severe stenosis lesion (>60%). All the patients received second-generation DES to fully cover the CAA and stenosis lesion.
Coronary artery aneurysm was defined as focal expansion of coronary segments, with a transverse diameter 1.5 times larger than normal adjacent segments.2,14 Based on the CAG, CAAs were classified into 2 types: (1) Saccular aneurysms were defined as aneurysms with a transverse diameter that exceed its length; (2) Fusiform aneurysms were defined as aneurysms with a transverse diameter shorter than their length. Major adverse cardiac event was a composite end point defined as cardiac death, MI, and urgent/ischemia driven revascularization.
Inclusive criteria of patients were with CAA complicated with moderate and severe stenosis (>60%) fully covered with second-generation DES. Patients had stable angina pectoris (SAP), unstable angina pectoris (UAP), non-ST-segment elevation myocardial infarction (NSTEMI), or STEMI. Baseline characteristics such as history, blood biochemical indicators, and stent information at target vessel of all patients were recorded during hospital admission. This observational study protocol was approved by the ethics committee of Nanjing First Hospital Affiliated to Nanjing Medical University. Written informed consents were obtained from all patients before PCI procedures were performed.
Standard selective CAG was performed via a radial approach with a 6F catheter without side hole according to routine practice. CAGs were analyzed with a quantitative coronary angiographic analysis (QCA) system (CAAS II 5.0) by one experienced observer at an independent core laboratory in the Nanjing cardiovascular center. By using the guiding catheter for calibration after 200-µg nitroglycerin injection into coronary artery (left main [LM] coronary artery), left anterior descending [LAD]), left circumflex [LCX]), and right coronary artery), target vessel, aneurysm classification, location of stenotic lesion with CAA, stent diameter after stent deployment, and post-dilation were recorded. Minimum luminal diameter (MLD), the proximal and distal reference vessel diameter (RVD), lesion length, the percentage of diameter stenosis (DS), thrombolysis in myocardial infarction (TIMI) flow, CAA length, maximal CAA diameter (CAAD), and CAA resolution ratio were measured before PCI, immediately, and 1 year post-PCI. 15 The formula for CAA expansion ratio was maximal CAAD/distal RVD. The formula for CAA resolution ratio was (maximal CAAD before PCI − maximal CAAD just after PCI) × 100/distal RVD just after PCI or (maximal CAAD just after PCI − maximal CAAD 1 year after PCI) × 100/distal RVD 1 year after PCI. Distal RVD, MLD, and DS in patients with STEMI were performed after thrombus aspiration. A typical patient with CAA and UAP was evaluated by CAG before PCI, immediately, and 1 year after PCI (Figure 1).
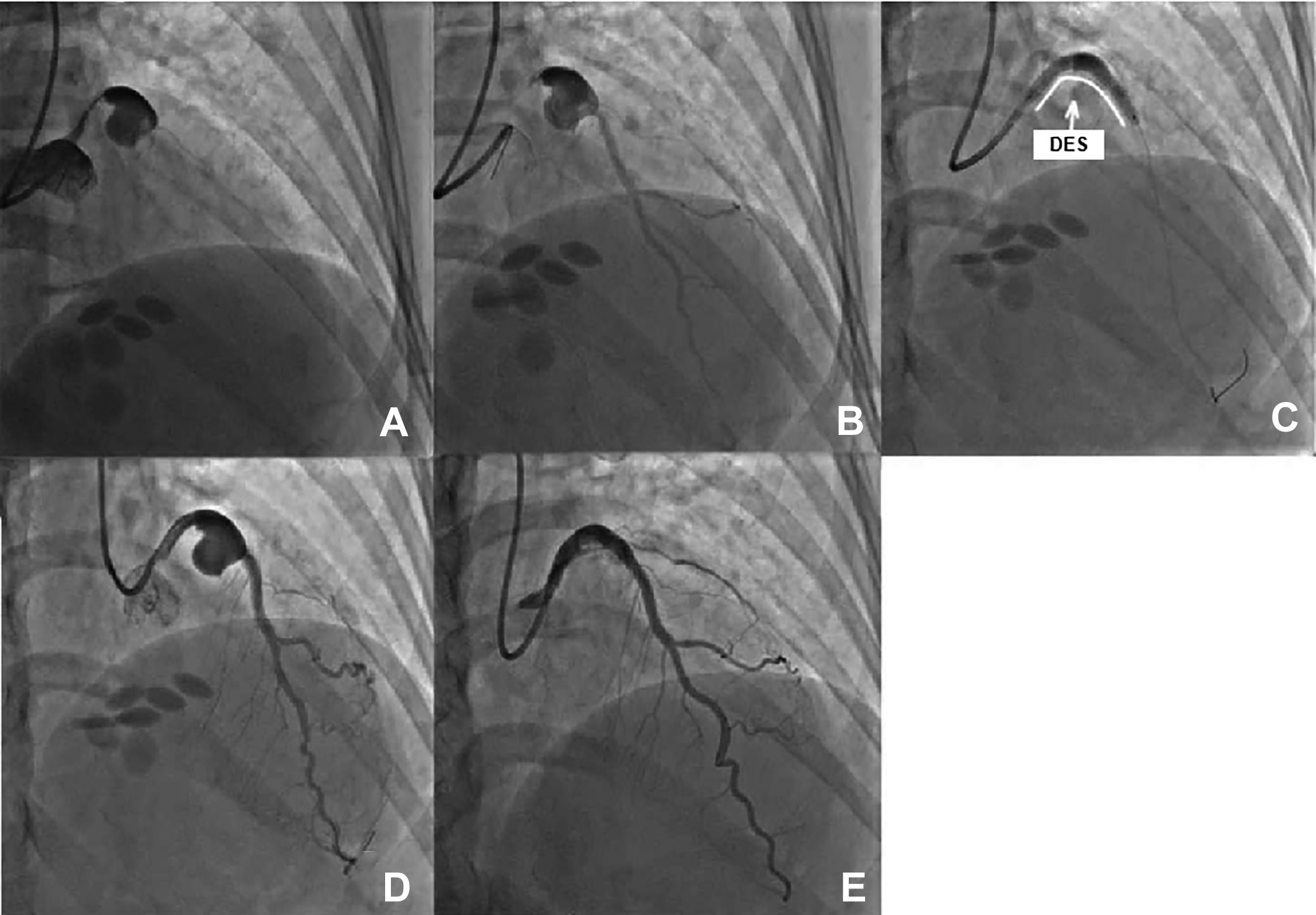
Preoperative, postoperative, and follow-up CAG images of saccular CAA in a female patient with CAA and UAP (RAO 20°, CRA 30°). A, CAG analysis of saccular aneurysm before PCI: Saccular CAA was complicated with proximal severe stenosis (>70%), and maximal CAA transverse diameter and CAA length were 12.57 and 11.77 mm, respectively. B, Distal RVD was 3.43 mm. C, Everolimus-eluting stent (3.5 × 33 mm) was implanted to fully cover CAA and proximal and distal lesion. D, After the second-generation DES implantation, maximal CAA transverse diameter and CAA length CAA were 12.55 and 11.75 mm, respectively. E, After 1-year follow-up, maximal CAA transverse diameter and CAA length were 4.85 and 8.75 mm, respectively. There was no in-stent restenosis. CAA indicates coronary artery aneurysm; CAG, coronary artery angiography; CRA, cranial; DES, drug-eluting stent; PCI, percutaneous coronary intervention; RAO, right anterior oblique; RVD, reference vessel diameter; UAP, unstable angina pectoris.
Statistical Analysis
All the data were expressed as mean ± SD for continuous variables and frequency for categorical variables. The paired t test was used to compare the QCA results before PCI, just after PCI, and 1 year after PCI. A 2-sided P < .05 was considered significant.
Results
The age of 33 patients (65.8 ± 11.1 years; 69.7% males) with CAA with stenosis lesion was relatively old, prevalence of smoking (42.4%), and previous disease history (such as hypertension [81.8%] and hyperlipidemia [36.4%]). The majority of patients had acute coronary syndrome (ACS; including UAP [54.5%] and NSTEMI [24.2%]). Most patients were under standard treatments (such as antiplatelet and plaque stabilizing drugs). Previous CABG (3.0%) and cerebral stroke (9.1%) were relative low (Table 1).
Baseline Clinical Characteristics in Patients With Focal Coronary Artery Aneurysm With Stenosis Lesion.a
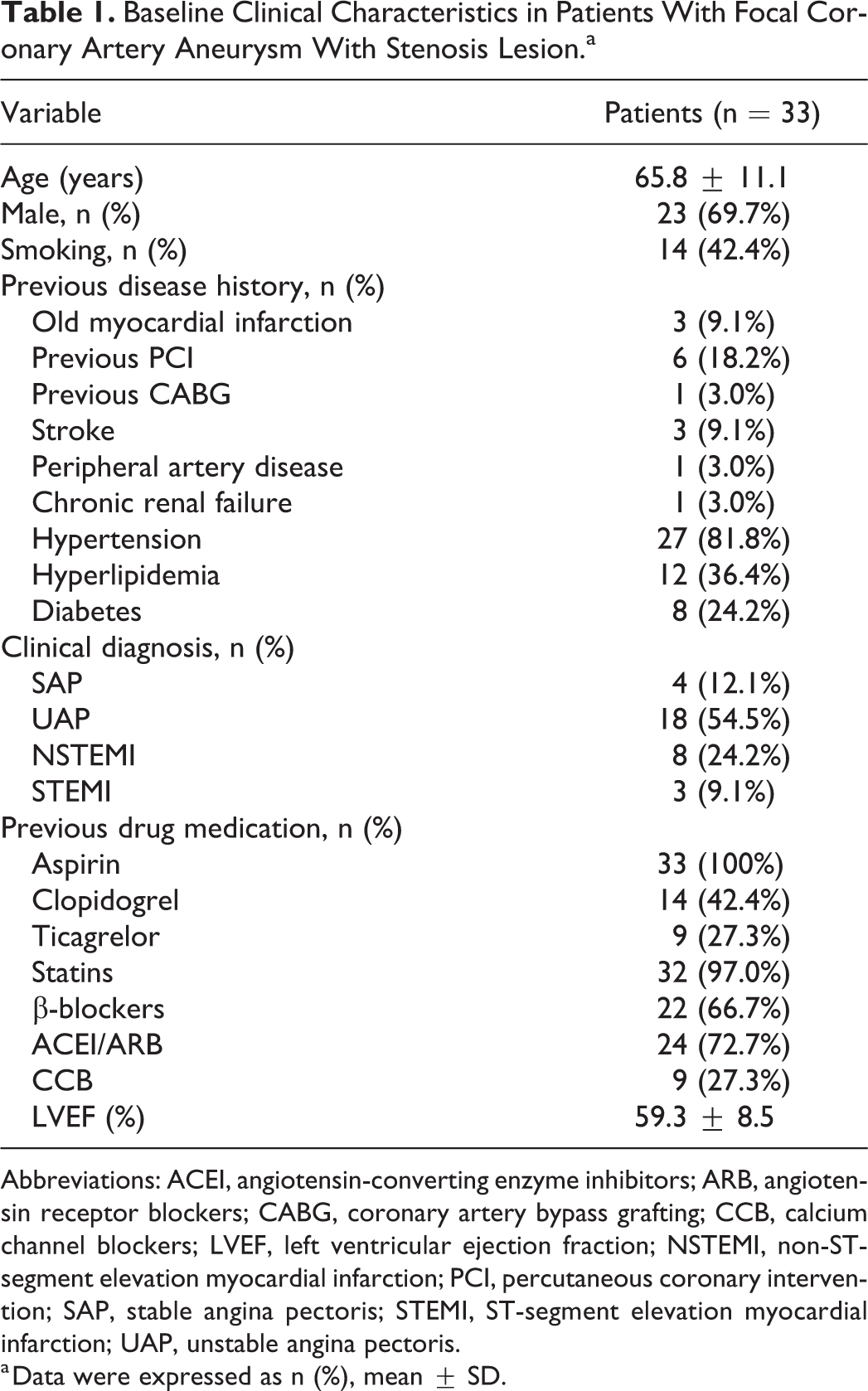
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; CABG, coronary artery bypass grafting; CCB, calcium channel blockers; LVEF, left ventricular ejection fraction; NSTEMI, non-ST-segment elevation myocardial infarction; PCI, percutaneous coronary intervention; SAP, stable angina pectoris; STEMI, ST-segment elevation myocardial infarction; UAP, unstable angina pectoris.
a Data were expressed as n (%), mean ± SD.
Due to the majority of patients having ACS, white blood cell count (7.00 ± 2.20 × 109/L), neutrophil count (4.86 ± 2.14 × 109/L), and levels of creatine kinase-MB (CK-MB; 52.9 ± 88.8 U/L), cardiac troponin-I (6.43 ± 13.87 ng/mL), and high-sensitivity C-reactive protein (6.3 ± 6.5 μg/mL) were relatively high. Although 97.0% patients were on statins, levels of total cholesterol and low-density lipoprotein cholesterol remained relatively high. However, other blood indexes such as red blood cell count and lymphocyte count were relatively normal (Table 2).
Baseline Blood Biochemical Indexes in Patients With Focal Coronary Artery Aneurysm With Stenosis Lesion.a
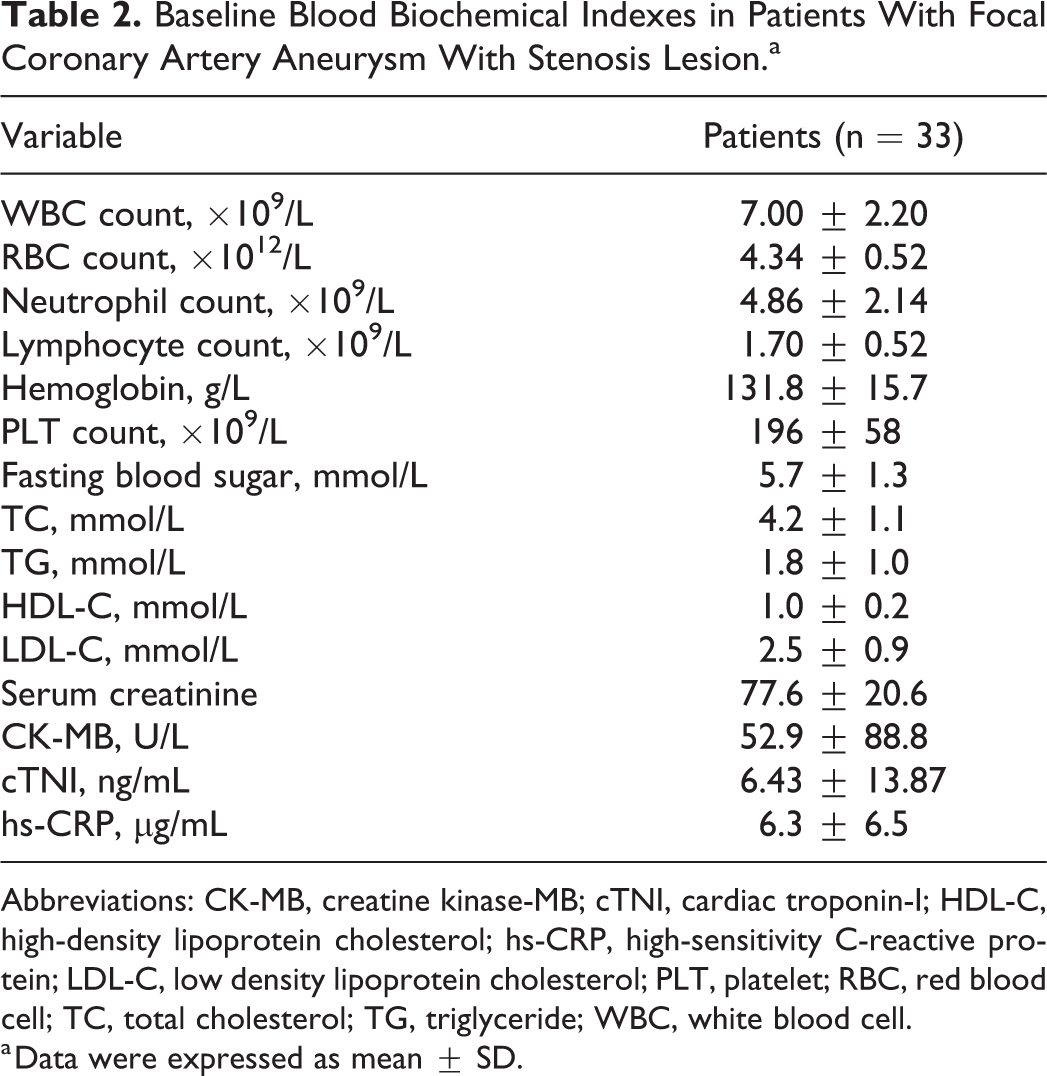
Abbreviations: CK-MB, creatine kinase-MB; cTNI, cardiac troponin-I; HDL-C, high-density lipoprotein cholesterol; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low density lipoprotein cholesterol; PLT, platelet; RBC, red blood cell; TC, total cholesterol; TG, triglyceride; WBC, white blood cell.
a Data were expressed as mean ± SD.
Most CAAs and moderate or severe stenosis lesions (75.8%) were located in the LAD artery. Coronary artery aneurysm expansion ratio in all 33 patients (including SAP, UAP, NSTEMI, and STEMI) were >1.5. The value of the CAA expansion ratio was 1.85 ± 0.53 mm. The incidence of fusiform CAA (84.8%) was relative high, and the locations of stenosis lesion with CAA were similar (Table 3). The lengths of CAAs and stenosis lesions were less than those of the total stents, indicating that the CAAs and stenosis lesions were fully covered with the stents (Table 3). Everolimus- or zotarolimus-eluting stents were used to treat patients with CAA and moderate or severe stenosis lesion. Results of successful second stent implantation at CAA and moderate or severe stenosis lesion are shown in Table 3. In these patients, there were no unsuccessful stenting to fully cover CAA and stenosis lesion.
Quantitative Coronary Angiographic Analysis of Target Coronary Artery in Patients With Focal Coronary Artery Aneurysm With Stenosis Lesion Before and Immediately Post-PCI.
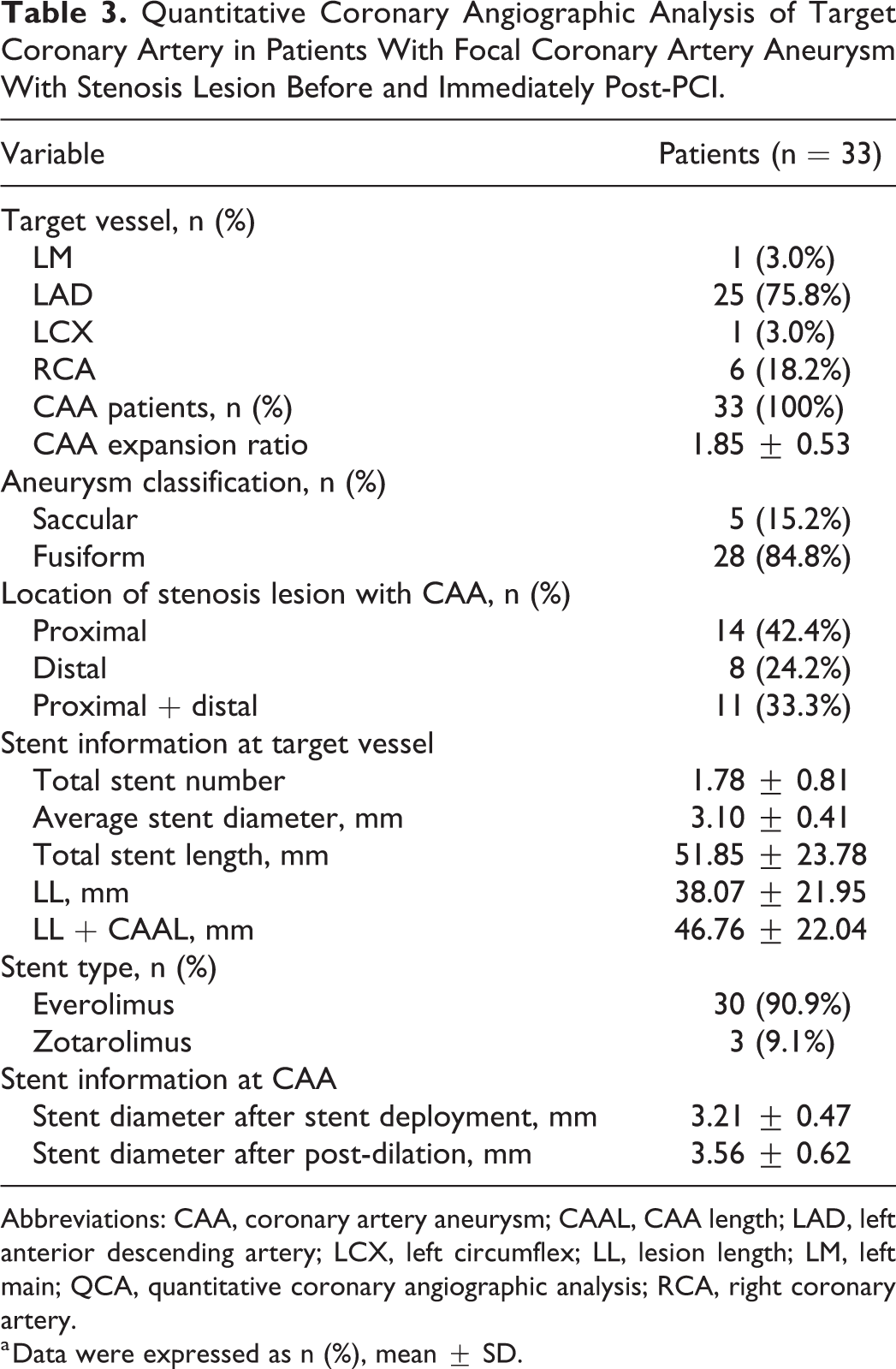
Abbreviations: CAA, coronary artery aneurysm; CAAL, CAA length; LAD, left anterior descending artery; LCX, left circumflex; LL, lesion length; LM, left main; QCA, quantitative coronary angiographic analysis; RCA, right coronary artery.
a Data were expressed as n (%), mean ± SD.
Diameter stenosis in 4 SAP patients were all >70%, and DS in other UAP, NSTEMI, and STEMI patients were all >60%. After DES implantation, MLD and residual DS in 33 patients were improved compared with those before PCI (P < .01). Also, TIMI flow of these patients after PCI were significantly enhanced (P < .05; Table 4). According to proximal and distal RVDs and CAA length, this provided a suitable indication for the second DES to fully cover CAA and stenosis lesion in these patients. After 1-year follow-up, maximal CAAD in patients with CAA and stenosis lesion were significantly reduced compared with those just after PCI (P < .01). Meanwhile, CAA resolution ratio in these patients were more than those just after PCI (P < .01). Furthermore, there was a significant reduction in CAA length in these patients as compared with those just after PCI (P < .01; Table 4).
Dynamic Observation of CAG Results Before, Just and 1 Year After PCI in Patients With CAA and Stenosis Lesion (n = 33).
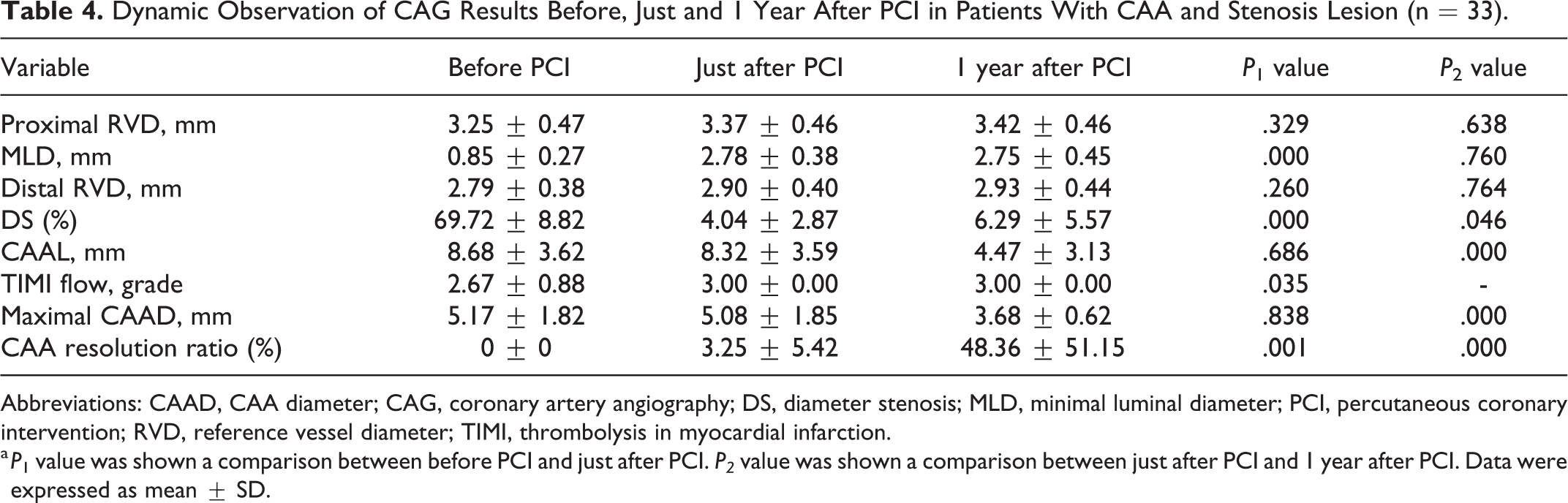
Abbreviations: CAAD, CAA diameter; CAG, coronary artery angiography; DS, diameter stenosis; MLD, minimal luminal diameter; PCI, percutaneous coronary intervention; RVD, reference vessel diameter; TIMI, thrombolysis in myocardial infarction.
a P 1 value was shown a comparison between before PCI and just after PCI. P2 value was shown a comparison between just after PCI and 1 year after PCI. Data were expressed as mean ± SD.
There were no any clinical events (including cardiac death, myocardial infarction, and revascularization) in our study.
Discussion
With widespread use of coronary tomography angiography and CAG, and increasing awareness, more patients have been found and diagnosed with a CAA.2,14 Most of them have coronary atherosclerosis and even severe stenosis. 16 The main causes of symptoms are:12,13,17,18 (1) Thrombus in large CAA leads to distal embolism and acute MI, (2) rupture of coronary atherosclerotic plaque causes acute thrombosis possibly leading to distal embolism, (3) coronary aortic stenosis lesion leads to imbalance of myocardial oxygen supply and demand, and/or (4) CAA rupture results in acute pericardial tamponade. Lim and his coworkers have reported that the incidence of MACE was higher in patients with CAA compared with patients without CAA after DES implantation during a median follow-up period of 1164 days. 8 Slow blood flow and disorder in CAA lumen is an important factor for thrombus formation, which means that if a CAA is shrunk, the risk of acute MI and even cardiac death may be significantly reduced.2,14 Therefore, the optimal treatment for these patients is to safely and efficiently reduce CAA size and expand moderate or severe stenosis lesion.
It has been reported the use of covered stents still exist and should also be considered in CAA patients, but this kind of stent shows a poor deliver ability, risk of restenosis and thrombosis, and occlusion of side branches compared with second generation DES. 19 Another percutaneous option in the management of wide-necked CAA is coil insertion.2,14 However, coil herniation can cause parent vessel occlusion, and therefore, stent-assisted techniques are preferred.2,14 The manipulation of the microcatheter, coils, or wires can also increase the risk of CAA rupture. 20 Qiao et al reported that using double-layer BMS to cover CAAs can make it thrombose and achieve a therapeutic effect; CAA in these patients resolved with no obvious adverse events. 21 However, the follow-up period of the study was only about 6 months. Currently, there is no consensus on the optimal management of CAAs.
The high definite stent thrombosis rate observed in CAA patients (16.5% at 1 year) may be secondary to stent malapposition, residual thrombus, or blood flow disorder through a metallic-jailed CAA. 14 A second-generation DES can reduce stent malapposition, improve lesion coverage, and may be useful in this setting. 22 In our study, we used second-generation DES to treat proximal and/or distal moderate or severe stenosis lesion in patients with CAA. We found that there was no stent thrombosis, intra-stent restenosis, or disturbed blood flow after 1-year follow-up. These results were similar to a previous report. 11 In the present study, proximal and distal RVDs and CAA length were suitable for 1 stent fully crossing over and expanding after post-dilation. Therefore, we used the second-generation DES to fully cover CAA and stenosis lesion. The length and maximal CAAD were significantly reduced in 33 patients after 1-year follow-up, which was unreported elsewhere. Three possible reasons explaining this result are (1) the hydrostatic forces on the vessel wall caused by a stenosis proximal and/or distal to the CAA that cause the CAA. When the severe stenosis of coronary artery was relieved, the CAA shrunk significantly.1,2,6 (2) After the second-generation DES fully covered CAA, the steel strut blocked blood flow to form turbulence and blood flow became slow. Additionally, destroyed CAA’s inner membrane promoted thrombus formation. However, the newly formed thrombus was blocked in the CAA by the stent strut, 23 and/or (3) local turbulence and shear stress of the vessel wall made some stent struts to be covered by neointima, leading the ostium of the stent strut to become gradually smaller and to a certain extent, closed the CAA entrance, and played a similar role as the covered stent. 24 However, in our study, there was no substantial change in CAAD immediately post-PCI, possibly related to heparin use during the PCI procedure, stent implantation for a short time, and unformed neointima between stent struts.
The most common cause of CAAs is atherosclerosis.1,2,6,25 Of course, the risk factors of atherosclerosis may be associated with the development of CAAs. In our study, the incidence of risk factors (including older age, smoking, hypertension and hyperlipidemia) in 33 patients with CAA and stenosis lesion were also relatively high. Regarding limitations, this is a retrospective and observational study of a rare disease in a single center and the number of cases and clinical data are limited. Due to economic factors, only 2 patients in this study underwent IVUS. Therefore, the result can only be considered exploratory.
In conclusion, the use of second-generation DES to fully cover CAA and moderate or severe stenotic lesions was safe and effective to reduce CAA size and in-stent restenosis after 1-year follow-up.
Footnotes
Authors’ Note
Zhiming Wu and Chen Xu contributed equally to this work. All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Nanjing Municipal Science and Technology Bureau (grant number: 201803008).