
Abstract
The optimal strategy for assessing the ischemic significance of intermediate coronary stenoses with adenosine-induced fractional flow reserve (FFR) and instantaneous wave-free ratio (iFR) is still debated. Few studies have previously assessed the impact of age on FFR and iFR, which was the aim of our study. Patients undergoing FFR and iFR evaluation for intermediate (40%-70%) coronary lesions were included and divided according to age. Fractional flow reserve was performed by intracoronary boluses of adenosine (60-1440 μg). Instantaneous wave-free ratio was automatically calculated. Among 148 patients undergoing FFR measurement of 166 lesions, 45.3% were ≥70 years. Elderly patients had higher minimal lumen diameter (P = .03). We also observed a linear relationship between iFR and FFR independently of age. Fractional flow reserve values were higher in the elderly patients, whereas iFR was not related to age. A total of 33 lesions had a positive iFR with no difference for age (17.3% vs 22%, P = .56), while FFR <0.80 was more infrequent in the elderly patients (17.1% vs 34.8%, P = .02). In intermediate coronary stenoses, iFR and FFR correlation is unaffected by age. Fractional flow reserve is higher in the elderly patients, whereas iFR is less affected by age. Future large-scale studies are needed to define whether iFR should be the preferred choice in elderly patients.
Keywords
Introduction
Revascularization based on anatomic thresholds have not reduced the rate of cardiovascular (CV) events among patients with coronary artery disease (CAD), offering no clear prognostic benefit compared with optimized medical therapy in large-scale randomized trials. 1,2 Therefore, the functional evaluation of the ischemic burden of coronary stenoses has progressively overcome their visual evaluation and especially for intermediate (40%-70%) lesions at angiography. 3
In fact, the measurement of fractional flow reserve (FFR), after the induction of maximum hyperemia with adenosine, has been indicated as the first-line strategy, 4 providing an outcome advantage for the guidance of percutaneous coronary interventions (PCIs). However, the protocol for hyperemia induction with adenosine still lacks standardization, 5,6 being additionally weighted by interindividual variability of response and poor tolerance. Among adenosine-free measurements, the instantaneous wave-free ratio (iFR) is a nonhyperemic pressure-derived ratio that is obtained as a diastolic resting measure, 7 recently incorporated in guidelines as a tool for the functional evaluation of coronary stenoses based on the noninferiority data of randomized trials. 8 -10 However, studies have shown a 20% rate of discordance between iFR and FFR, which may result in lesion underestimation and increased risk of CV events. 11
Clinical, angiographic, and hemodynamic factors have been shown to contribute to iFR/FFR discordance, with a potential role being played by age. 12 In fact, older patients display a greater degree of microvascular dysfunction reducing the response to adenosine, and a gradual increase in coronary flow velocity and reduction in coronary diastolic filling, that could impact of the assessment of FFR or iFR in advanced age. 9,13 However, no studies, so far, have assessed the impact of aging on the functional evaluation of coronary stenoses with the 2 different methods; this was the aim of the present study.
Methods
In this prospective observational study, we included consecutive patients who underwent coronary angiography and functional evaluation of intermediate coronary stenoses, from February 2015 to September 2018 at the Division of Cardiology, “Maggiore della Carità” Hospital, Eastern Piedmont University, Novara, Italy. Exclusion criteria were (1) allergy to adenosine (self-reported in case of previous exposure to the drug), (2) baseline bradycardia (heart rate <50 bpm) and hypotension (blood pressure <90 mm Hg), and (3) refusal to provide informed consent. All patients signed the informed consent to participate in the study. The study was approved by our local ethical committee. The main demographic, clinical, and angiographic data, together with the indication to coronary angiography, were recorded at admission and included in a dedicated database, protected by password. The main CV risk factors were identified. Hypertension was defined as systolic pressure >140 mm Hg and/or diastolic pressure >90 mm Hg or use of antihypertensive medication. The diagnosis of diabetes was based on previous history of diabetes treated with or without drugs fasting glucose >126 g/dL, or HbA1c >6.5% at the time of admission. The main chemistry parameters were assessed at admission, following a fasting period of 12 hours, as previously described. 14 Chronic renal failure was considered as a history of renal failure or an admission estimated glomerular filtration rate <60 mL/min/1.73 m2 using the Modification of Diet in Renal Disease formula. 10,14
Coronary Angiography
Coronary angiography (carried out by Siemens AXIOM ARTIS dTC) was routinely performed by the Judkins technique using 6F right and left heart catheters in patients fasting (in particular without caffeine intake) for >12 hours. Quantitative coronary angiography was performed by 2 experienced interventional cardiologists, using an automatic edge-detection system for Quantitative Coronary Angiography (Siemens Acom Quantcor QCA). 11 After a visual inspection of the coronary artery, the frame of optimal clarity was selected, showing lesions at maximal narrowing and arterial silhouettes in sharpest focus. After calibration of the guiding catheter, the analyzed arterial segment with coronary lesion was defined by moving the cursor from the proximal to the distal part of coronary artery to ensure adequate determination of reference diameter (RD). Minimal luminal diameter (MLD), RD, percent diameter stenosis, and length of the lesion were measured.
In previously bypassed patients, both native arteries and grafts were taken into account in the evaluation of extension of CAD (number of diseased vessels). A stenosis was considered significant if >70% and intermediate if between 40% and 70%.
Fractional Flow Reserve Assessment
In patients displaying intermediate coronary stenoses, functional evaluation was performed by iFR and FFR immediately after coronary angiography, as previously described. 15 Instantaneous wave-free ratio was automatically calculated by the use of the manufacturers’ software (Prime Wire, Volcano Imaging System).
For the measurement of FFR, all patients received intracoronary adenosine boluses with a progressive increase to high-dose adenosine, if tolerated (60, 120, 180, 360, 720, and 1440 μg). Each bolus was followed by a saline flush. Measurement of FFR was started 3 seconds after bolus administration. Each bolus was administrated at least 1 minute after the previous one (in all cases until pressure curves returned to baseline values). In order to minimize and standardize fluid volume infusion, we prepared the drug with a special dilution of 60 and 360 µg/mL.
For each adenosine dose, we measured the absolute values of the arterial and distal poststenotic pressure (P a and P d, respectively) and the value of the FFR that was defined by the formula FFR = P d/P a. Fractional flow reserve was considered pathological at values ≤0.80. 15 A coronary stenosis was considered significant for FFR values ≤0.80 or iFR ≤ 0.90 according to the previous literature. 16 The most recently updated definition of iFR ≤ 0.89 was also applied. 17
Statistical Analysis
Statistical analysis was performed using the SPSS version 23.0 statistical package. Continuous data were expressed as mean ± SD and categorical data as percentage. Analysis of variance and the χ2 test were used for continuous and categorical variables, respectively. Patients were grouped according to age (<70 or ≥70 years). Multiple logistic regression analysis was performed to evaluate the relationship between age and positive FFR and iFR after correction for main baseline differences that were entered in the model in block. A 2-sided P < .05 was considered significant.
Results
We included 148 patients undergoing FFR and iFR evaluation of 166 lesions. Among them, 67 (45.3%) were aged ≥70 years. Baseline characteristics of the population are displayed in Table 1.
Main Clinical and Demographic Features According to Age.
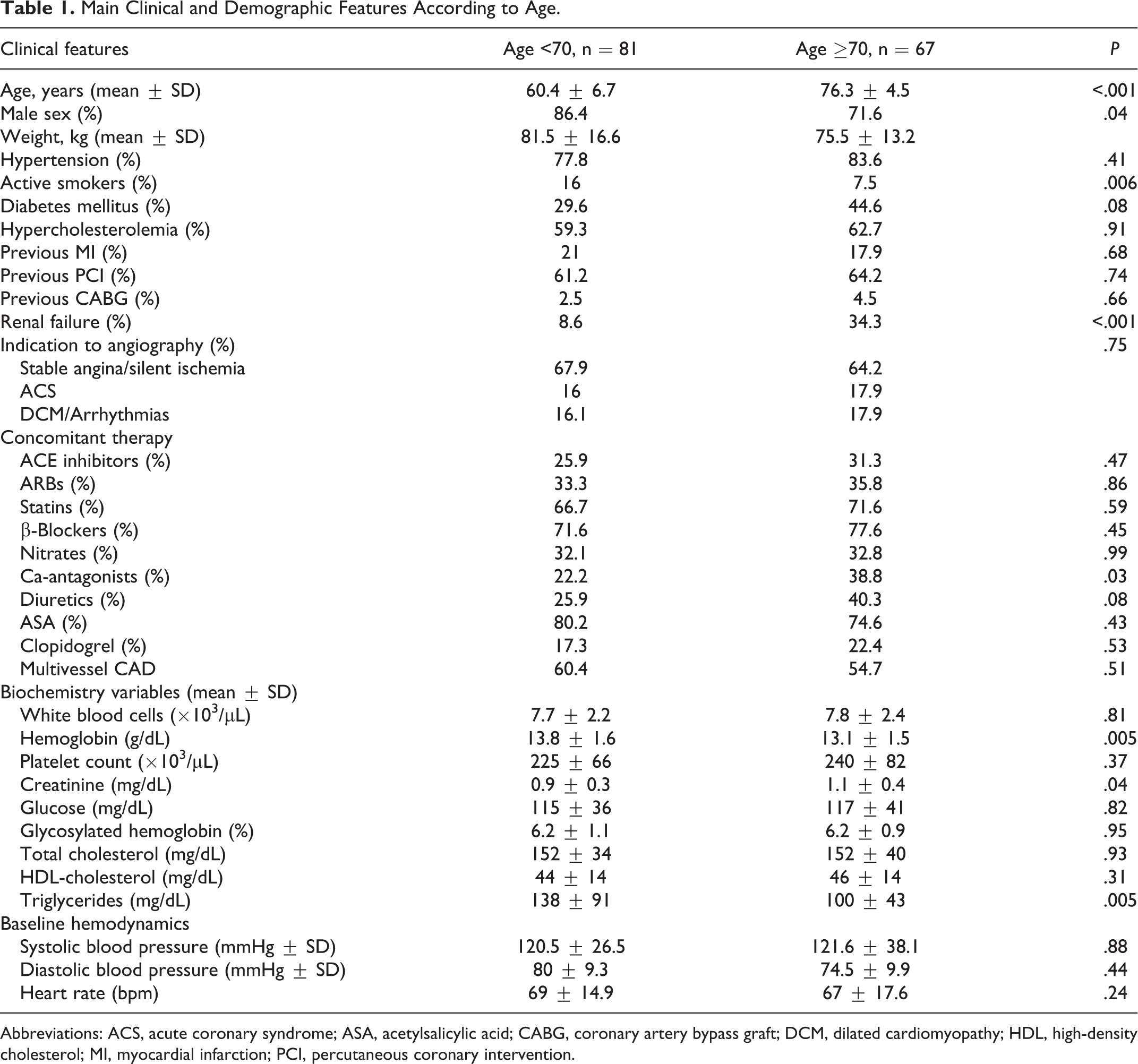
Abbreviations: ACS, acute coronary syndrome; ASA, acetylsalicylic acid; CABG, coronary artery bypass graft; DCM, dilated cardiomyopathy; HDL, high-density cholesterol; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Elderly patients were more often females (P = .04), with higher rates of renal failure (P < .001), use of calcium channel blockers (P = .03), lower active smokers (P = .006), body weight (P = .02), and triglycerides and hemoglobin (P = .005).
Angiographic features of target lesions are displayed in Table 2 and were comparable in the 2 groups but for a higher MLD in patients ≥70 years (P = .03).
Angiographic Characteristics.
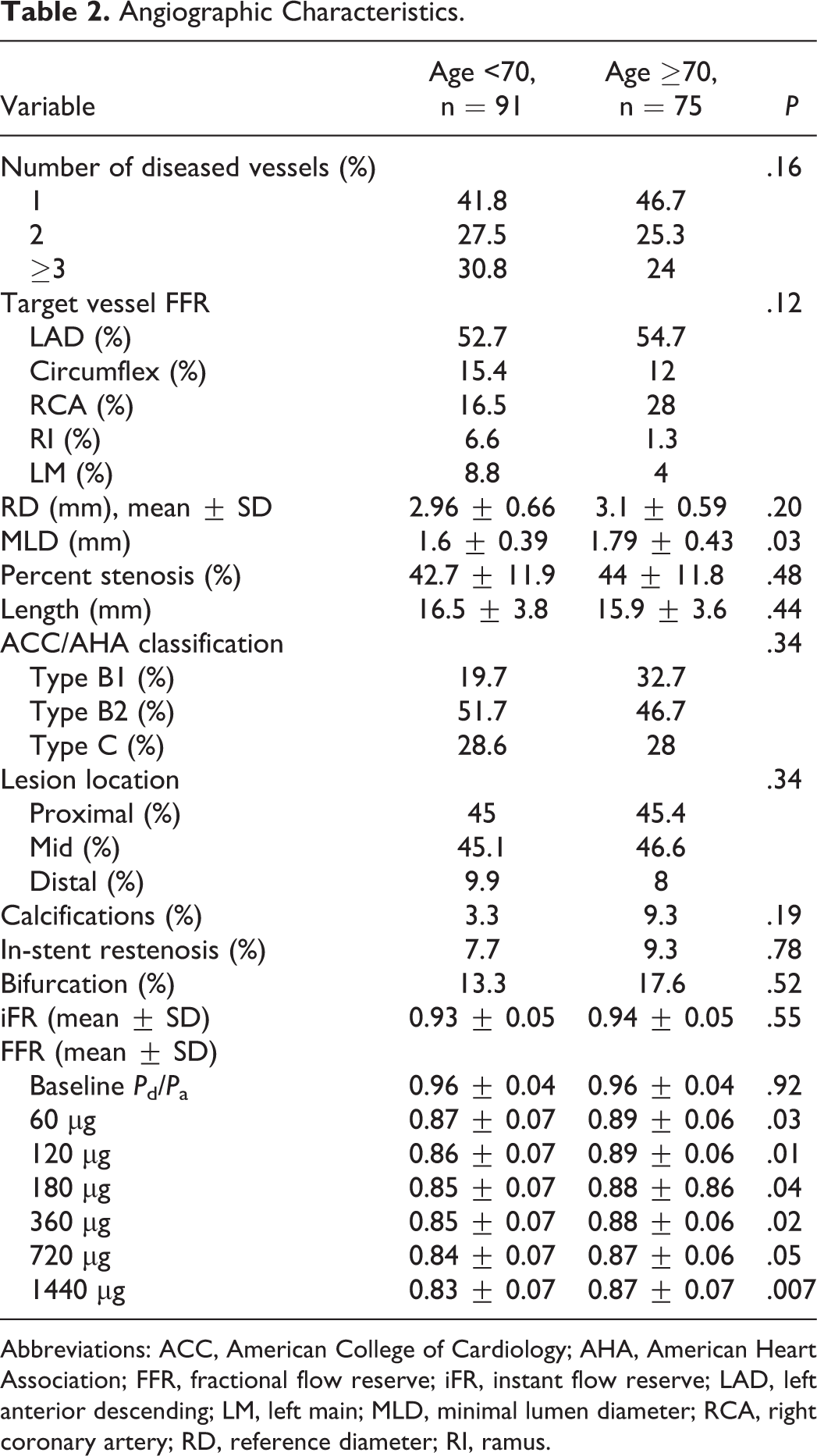
Abbreviations: ACC, American College of Cardiology; AHA, American Heart Association; FFR, fractional flow reserve; iFR, instant flow reserve; LAD, left anterior descending; LM, left main; MLD, minimal lumen diameter; RCA, right coronary artery; RD, reference diameter; RI, ramus.
We observed a linear relationship between iFR and FFR (baseline and after hyperemic stimulation with adenosine) that was maintained in both patients <70 and ≥70 years of age and for increasing doses of the adenosine boluses (Table 3). There were no procedure-related complications. Adenosine elicited a transient atrioventricular block with ventricular pauses >5 seconds requiring a discontinuation of the FFR protocol before the completion of all the adenosine boluses in 11.4% of the patients.
Correlation Between Instantaneous Wave-Free Ratio and Fractional Flow Reserve According to Age Groups.
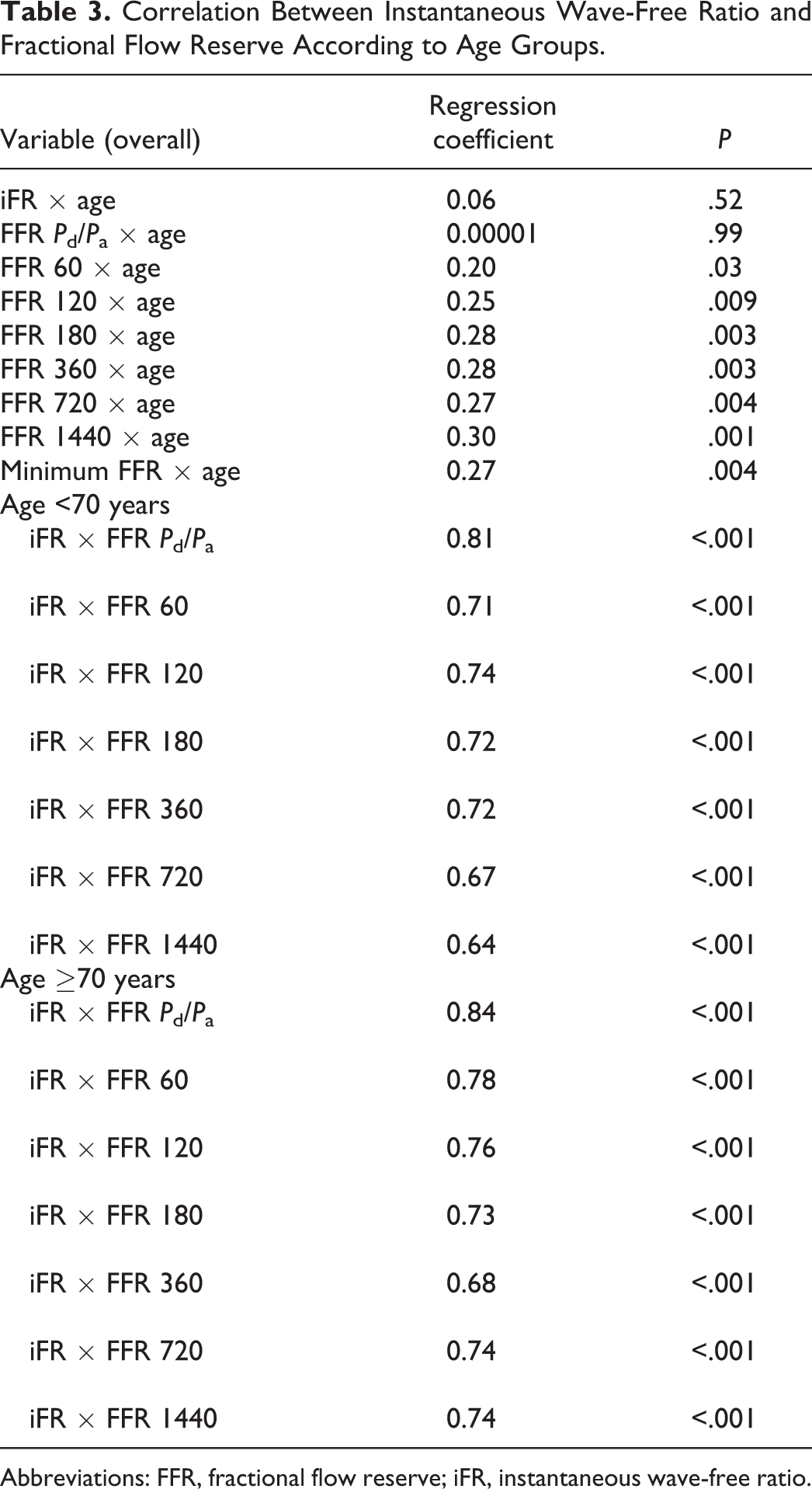
Abbreviations: FFR, fractional flow reserve; iFR, instantaneous wave-free ratio.
A total of 33 lesions displayed a positive iFR with no difference according to age (17.3% vs 22%, P = .56, Figure 1), while an FFR ≤ 0.80 was observed in 37 (23.4%) lesions with a significantly lower rate in advanced age (17.1% vs 34.8%, P = .02, Figure 2). Concordance in the positivity of iFR and FFR was observed in 20 lesions (60.6% of the positive iFR and 54% of the positive FFR). When considering the most recent cutoff of iFR ≤ 0.89, 27 lesions displayed a pathological iFR, with no difference according to age (13.9% vs 19.3%, P = .40).
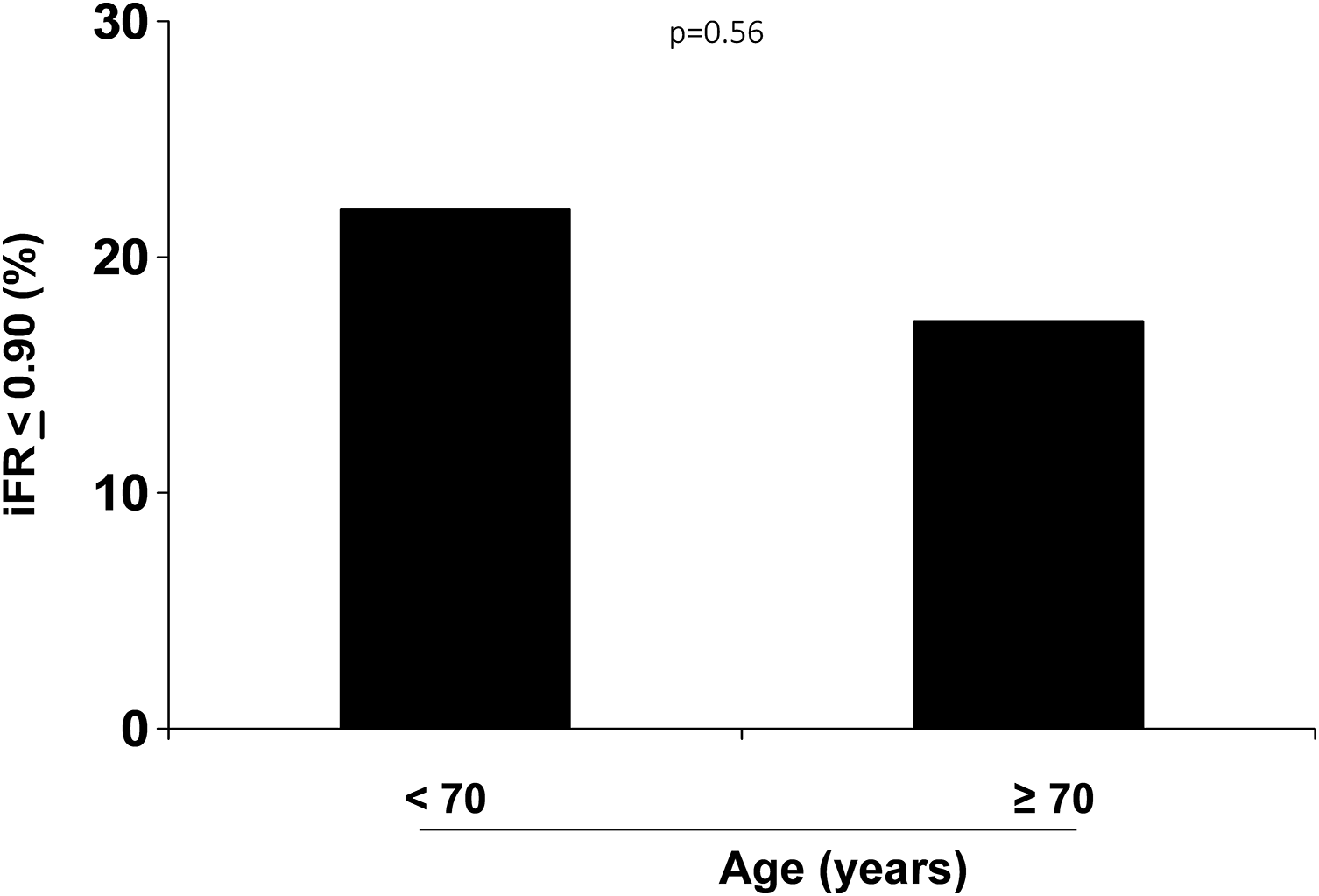
Bar graph showing the percentage of positive (
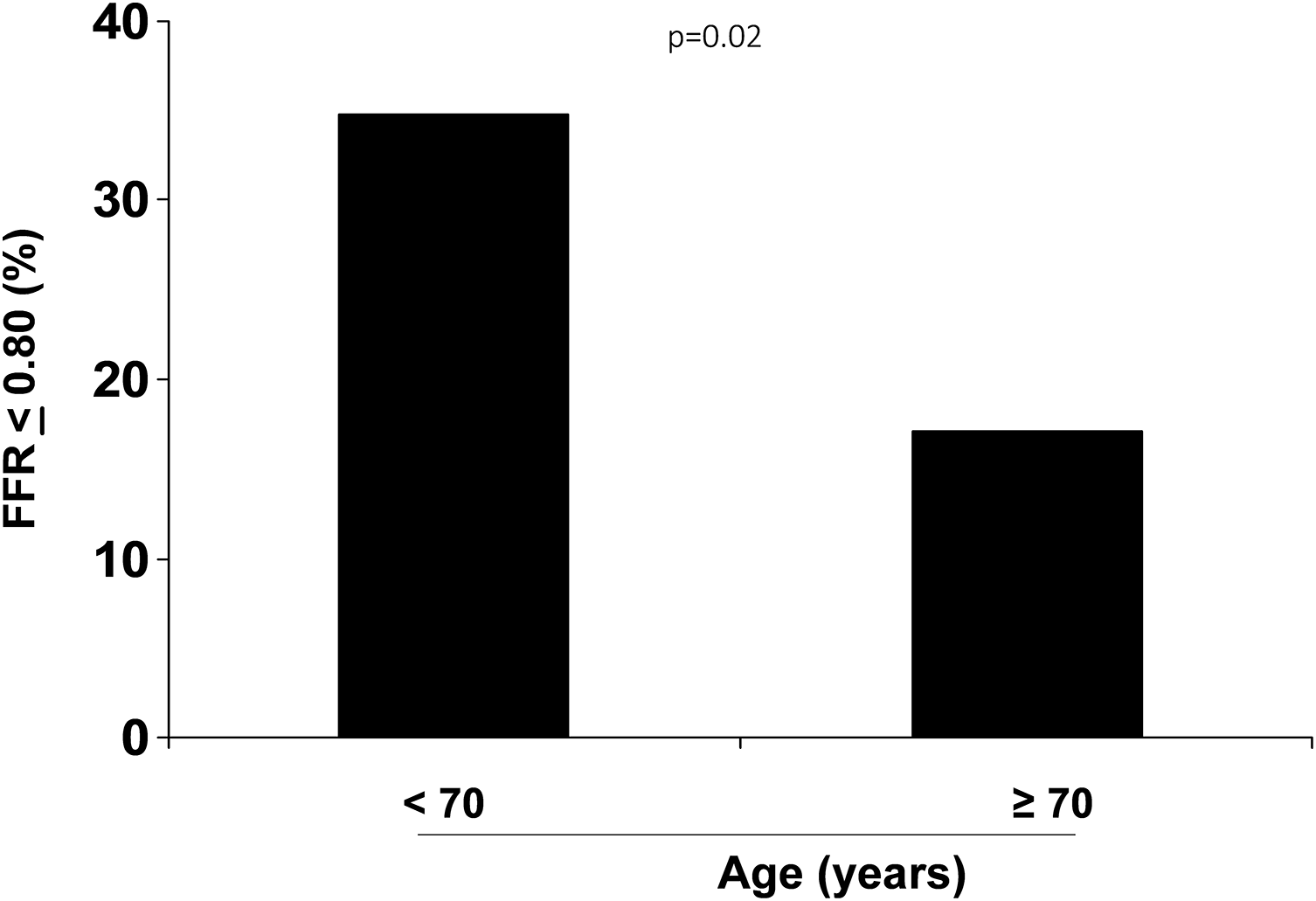
Bar graph showing the percentage of positive (<0.80) fractional flow reserve according to age.
Our results were confirmed after correction for baseline differences for both iFR (adjusted OR [95% CI], 0.96 [0.35-2.6], P = .93) and FFR (adjusted OR [95% CI], 0.56 [0.29-1.09], P = .09).
In fact, the values of iFR were not related with age, whereas the mean values of FFR were higher among elderly patients (Figure 3A and Table 2), with a linear relationship between FFR and age being confirmed at all the different doses of adenosine boluses (Figure 3B and Table 2). A similar relationship between iFR and FFR with age was observed when considering separately patients according to the median values of MLD (<1.69 mm, n = 82: r = 0.06, P = .64 for iFR and r = 0.20, P = .09 for FFR; ≥1.69 mm, n = 84: r = −0.03, P = .79 for iFR, r = 0.29, P = .014 for FFR, respectively). Results did not change when restricting our analysis to the 57 (34.3%) lesions involving left main or LAD (iFR: r = 0.10, P = .47; FFR = 0.41, P = .002).
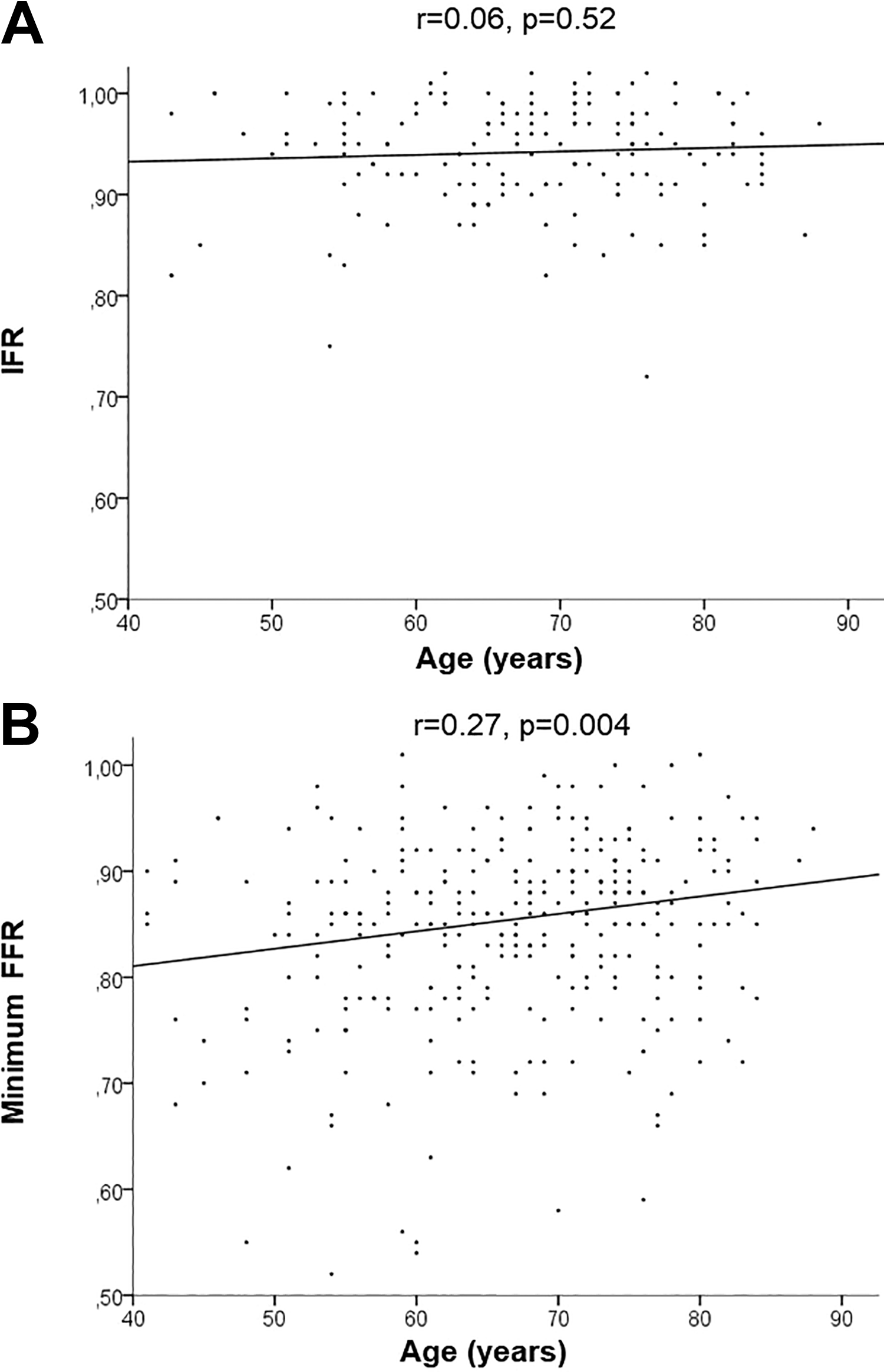
Relationship between instantaneous wave-free ratio (A, upper graph), and minimum fractional flow reserve (B, lower graph) according to age.
Discussion
Our study is one of the first cohorts of patients where we investigated the impact of age on the measurement of both FFR and iFR. Our main results showed no statistically significant impact of advanced age on the evaluation of iFR, whereas the vasodilatory response to adenosine was reduced among the elderly patients, resulting in higher values of FFR, despite similar degree of percent stenosis and lesion length in younger as compared with older patients.
Despite the improvements in stent technologies and techniques for coronary revascularization have dramatically lowered the rates of thrombotic complications and repeated revascularization, improving the outcomes of patients undergoing PCI, yet increasing attention has been focused on the importance of limiting the treatment to those clinically significant lesions with a substantial ischemic burden. 1 –4 In the FFR versus coronary angiography for guiding PCIs (FAME) 2 trial, among patients with stable CAD, PCI was superior to medical therapy alone, in the reduction of the primary composite end point of death, myocardial infarction, or urgent revascularization at 5 years, when PCI was guided by FFR to assess the functional ischemic effect of a lesion. 15 Similar conclusions were confirmed in a meta-analysis. 18
However, the exact cut point for the definition of severe coronary stenosis is still matter of debate, ranging from 0.75 to 0.80, pointing at the existence of a “gray zone” with borderline FFR results, whose underestimation could translate into potential negative consequences in terms of clinical outcome. 18 In addition, the protocol for the achievement of maximal hyperemia of the coronary vessel for the assessment of FFR, still lacks standardization since adenosine-induced vasodilatation has been described with either intravenous infusion or intracoronary boluses, including different adenosine dosing. 19 -21
The interindividual variability in the response to adenosine and reduced tolerance to the drug has progressively favored a shift toward adenosine-free methods for the assessment of coronary ischemia. The iFR is a pressure-only index of coronary stenosis severity measured at rest, without pharmacological vasodilatation, using an automated offline algorithm that accounts for the ratio of distal to proximal coronary pressures during the diastolic period of the cardiac cycle, when distal intracoronary resistance is stable and minimal. 9,22 Good concordance between iFR and FFR has been reported in >80% of assessed lesions, resulting in noninferior guidance of PCI and offering additional advantages in terms of procedural time and patient tolerance, 7 However, several clinical and angiographic factors have emerged as potentially affecting the accuracy of iFR, accounting for the about 20% non-concordant measurements between iFR and FFR. 11,23
Indeed, a reduction in resting coronary flow can be associated not only with a significant epicardial coronary artery stenosis but also to coronary microvascular disease or even the presence of atherosclerotic risk factors, such as diabetes or hypertension. These factors could condition impaired ventricular diastolic relaxation and exogenous compression or increase peripheral microvascular resistance. 24,25
In particular, a reduction in coronary flow has been previously described in elderly patients mainly due to a gradual increase in resting velocities. A study comprising 335 patients with normal coronary arteries 13 reported that coronary flow reserve (CFR) was progressively reduced with aging while hyperemic velocities remained unaffected. Moreover, ventricular mass, diastolic blood pressure, total cholesterol, blood glucose, and male gender were independent determinants of CFR in the whole population, factors that are per se more frequent in elderly patients. 26,27
However, the increased velocity of coronary flow, resulting in a loss in perfusion pressure, could lead to microcirculatory vasoconstriction and therefore to a rise in distal resistance and may be sufficient to attenuate trans-stenotic gradients during stable hyperemia, thus resulting in lower iFR as compared to FFR. 28 In fact, in the prospective multicenter Can cONTrast Injection better Approximate FFR compared to Pure resting Physiology study, 12 advanced age emerged as an independent predictor of a positive iFR, discordant from FFR, therefore suggesting potential underestimation and undertreatment of these lesions.
In contrast, previous studies have documented higher values of FFR among elderly patients, in consequence of an age-related decrease in absolute coronary vasodilator reserve, mediated by a lower response to endothelium-derived relaxing factors in a dysfunctional endothelium 29,30 but also by a lesser effect of adenosine on vascular smooth muscle due to desensitization. In fact, experimental models have shown a greater local release of adenosine in the coronary microcirculation of older animals; this could potentially impair the effectiveness of an exogenous administration. 31
Indeed, the subanalysis of the FAME 2 trial 32 comparing patients <65 or ≥65 years of age, showed that older patients have fewer functionally significant lesions, despite a similar angiographic appearance, although the prognostic advantages of FFR-guided PCI were independent of age.
However, despite both iFR and FFR have been associated with the risk of inadequate estimation of the functional impact of coronary stenoses, the role of age in these measurements and the best strategy for the assessment of coronary stenoses among elderly patients are still largely unexplored.
The present study represents one of the first studies comparing the impact of age on both FFR and iFR in the evaluation of intermediate coronary stenoses. Contrasting with Dérimay et al, 12 we documented that the linear correlation between iFR and FFR was maintained in both patients aged <70 and ≥70 years and for the evaluation of resting and postadenosine evaluation.
However, despite similar baseline P d/P a values, elderly patients showed an impaired hyperemic response, even with very high doses of adenosine, while the measurement of iFR was affected to a lesser extent by advanced age compared with younger patients. In fact, in our study, the iFR was less predictive of the functional impact of coronary stenoses in patients aged <70 years since many lesions achieved an FFR < 0.80 despite a negative iFR.
Analogous conclusions were reached by Jin et al, 33 comparing the FFR values of 91 lesions in patients aged <65 years with those of 87 patients aged ≥65 years. They showed that elderly patients with intermediate CAD were more likely to have higher FFR and lower delta, despite a similar degree of epicardial stenosis confirmed with the use of intravascular ultrasound. They concluded that the integration of functional and imaging evaluation of coronary lesions could provide prognostic benefits among these patients, overcoming the risk of underestimation with FFR alone. A similar elevation in FFR values with age was observed, concluding that age is a strong and independent predictor for angiographic overestimation of the severity of coronary stenosis. 34
Nevertheless, iFR was not performed in a Korean study or in other studies dedicated to the elderly patients. 32,33 The increased stability of this measurement reported in our population, as much as the greater tolerability, that could be of advantage among more frail patients, certainly paves the way to a potential greater preference of a resting measure over FFR in this specific subset of patients. However, larger dedicated trials are needed to confirm our findings and better define whether the prognostic role of iFR-guided PCI could be conditioned according to age.
Limitations
The relatively small size of our population is a limitation. However, since our study was able to detect a significant difference in FFR, we expect that an eventual difference in terms of iFR would have emerged, if there had been one.
Another limitation may be the definition of elderly patients as >70 years of age. In fact, our population included elderly patients, resulting in older age than in previous studies. Only few patients could be included in the extreme decades of age, thus limiting the power of our study. However, similar data were confirmed when considering age as a continuous variable.
Moreover, since, at the time of starting the study, functional assessment of coronary lesions was not indicated in the settings of acute coronary syndromes, and our population is represented mainly by patients with stable coronary disease. No patient undergoing staged procedures after a recent ST-segment elevation myocardial infarction was included, thus limiting the interpretation of our results.
Finally, we did not perform a systematic follow-up of our patients. Therefore, we could not definitely evaluate the impact of FFR/iFR estimation of the severity of a stenosis on the risk of future CV events.
Conclusion
In patients undergoing functional assessment of intermediate coronary stenoses, the good correlation between iFR and FFR was not affected by age. However, the rate of significant coronary lesions detected by iFR was significantly lower than with FFR, especially among younger patients. Advanced age was associated with a reduced vasodilatory response to adenosine and higher FFR values, whereas affecting to a lesser extent the measurement of iFR. Future large-scale studies are needed to define whether iFR should be preferred above FFR in elderly patients and to define its prognostic role in this higher risk subset of patients.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.