
Abstract
Aim:
Instantaneous wave-free ratio (iFR) has emerged as the strategy of choice for the assessment of intermediate coronary lesions. The impact of preprocedural β-blockers therapy on the iFR was the aim of this study.
Methods:
We included patients undergoing functional assessment of intermediate (40%-70%) coronary lesions in 2 centers. The iFR measurement was performed by pressure-recording guidewire and calculated at the core laboratory using the manufacturers’ dedicated software. Minimal luminal diameter, reference diameter, percent diameter stenosis, and length of the lesion were measured. Positive iFR was considered for values <0.90.
Results:
We included 197 patients undergoing functional evaluation of 223 coronary lesions. Patients on β-blockers (69%) had more frequently hypertension (P = .05); previous myocardial infarction (P = .01); therapy with clopidogrel (P = .02), statins, and aspirin; and acute coronary syndrome at presentation (P < .001, respectively). Mean iFR values were slightly higher in patients on β-blockers (0.94 ± 0.06 vs 0.92 ± 0.06, P = .11). The rate of positive iFR was significantly lower with β-blockers (14.9% vs 27.5%, P = .04). On multivariate analysis, β-blockers use was a predictor of the significance of coronary stenoses (odds ratio [OR] = 0.48; 95% CI = 0.23-0.98; P = .05) together with lesion length (OR = 1.04; 95% CI = 1.01-1.07; P = .007).
Conclusion:
Among patients undergoing iFR, preprocedural β-blockers are associated with higher absolute values and a lower rate of positive iFR.
Keywords
Introduction
Optimal medical therapy represents the pillar for the management of patients with coronary artery disease (CAD). 1 –3 Among pharmacological agents, β-blockers are indicated as a first-line strategy in guidelines, 4 having demonstrated clinical and prognostic benefits, with the reduction of symptoms and long-term mortality, mainly in postmyocardial infarction or in patients managed without revascularization. 5,6 In fact, β-blockers can improve myocardial perfusion and reduce the extent of ischemic areas, by improving coronary flow reserve and microcirculation. 7 –9
Indeed, recent studies and meta-analyses have shown the superiority of ischemia-driven percutaneous coronary interventions (PCI) as compared to medical therapy in chronic coronary syndromes, and in particular when the revascularization is guided by the functional assessment of coronary lesions with fractional-flow reserve (FFR). 10,11
The instantaneous wave-free ratio (iFR) is a nonhyperemic method for the evaluation of the ischemic power of coronary stenoses, recently emerging over FFR for its easier assessment, increased tolerability, and larger reproducibility, not being affected by the variability of adenosine-infusion protocols. 12,13
Differently from noninvasive stress tests, where the use of β-blockers has been associated to a lower capability of detecting ischemia, 14 previous studies have suggested that preprocedural β-blockers do not alter the results of FFR. 15
In contrast, a larger impact of pharmacological therapy could be hypothesized for the evaluation of iFR, a resting ratio calculated during the diastolic phase of cardiac cycle, thus largely depending on heart rate, hemodynamic parameters, and peripheral resistances.
However, no study has ever evaluated the impact of preprocedural β-blockers on the assessment of iFR, and this was the aim of the present study.
Methods
In this prospective observational study, we included consecutive patients referred for coronary angiography and functional evaluation of intermediate coronary stenoses at the Division of Cardiology, “Maggiore della Carità” Hospital, Eastern Piedmont University in Novara, Italy, from February 2015 to September 2018 and at “Ospedale degli Infermi”, ASL Biella, Italy, from January 2019 to October 2020. Exclusion criteria were: (1) coronary stenosis >70% at quantitative coronary angiography; (2) unavailable or inconsistent data (instability of the signal of iFR, irregular heart rate, unreliable compliance to the therapy); (3) refusal to provide signed informed consent. The study was approved by our local Ethical Committee. Main demographic, clinical and angiographic data, together with the indication to coronary angiography were recorded at admission and included in a dedicated database, protected by password. Main cardiovascular risk factors were identified. Hypertension was defined as systolic pressure > 140 mm Hg and/or diastolic pressure was >90 mm Hg or if the individual was taking antihypertensive medications. The diagnosis of diabetes was based on a previous history of diabetes treated with or without drug therapies, fasting glucose >126 g/dL, or hemoglobin A1c > 6.5% at the moment of admission. Main chemistry parameters were assessed at admission, following a fasting period of 12 hours, as previously described. 16 Chronic renal failure was considered for history of renal failure or an admission glomerular filtration rate < 60 mol/min/1.73 m2 by Modification of Diet in renal Disease formula.
Coronary Angiography
Coronary angiography (carried out by Siemens AXIOM ARTIS dTC) was routinely performed by the Judkins technique using 6-French right and left heart catheters in patients fasting for >12 hours and having taken their morning pharmacological therapy, including the usual dose of β-blockers. Quantitative coronary angiography was performed by experienced interventional cardiologists, using an automatic edge-detection system for quantitative coronary angiography. 17 After a visual inspection of the coronary artery, the frame of optimal clarity was selected, showing the lesion at its maximal narrowing and the arterial silhouette in the sharpest focus. After the calibration of guiding catheter, the arterial segment with a coronary lesion was defined by moving the cursor from the proximal to the distal part of the coronary artery to ensure adequate determination of reference diameter (RD). Minimal luminal diameter, RD, percent diameter stenosis, and length of the lesion were measured.
In previously bypassed patients, both native arteries and grafts were taken into account in the evaluation of the extent of CAD (number of diseased vessels). A stenosis was considered significant if more than 70%, intermediate between 40% and 70%.
Instantaneous Wave-Free Ratio Assessment
In patients displaying intermediate coronary stenoses, functional evaluation was performed by iFR immediately after coronary angiography, as previously described. 18 Instantaneous wave-free ratio was automatically calculated by the use of the manufacturers’ software (Prime Wire, Volcano Imaging System).
A coronary stenosis was considered significant for iFR < 0.90 according to the previous literature. 19,20
Statistical Analysis
Statistical analysis was performed using SPSS 23.0 statistical package. Continuous data were expressed as mean
Results
We included in our analysis 197 patients undergoing functional evaluation of 223 coronary lesions. Among them, 136 (69%) received preprocedural β-blockers.
Baseline characteristics of the included patients are displayed in Table 1. Patients on β-blockers had more frequently hypertension (P = .05); previous myocardial infarction (P = .01); therapy with clopidogrel (P = .02), statins, nitrates, and aspirin; history of PCI or acute coronary syndrome at presentation (P < .001, respectively). Patients on β-blockers displayed lower white blood cells (P = .005) and total cholesterol (P = .03). Baseline heart rate was lower in patients treated with β-blockers (P = .02).
Main Clinical and Demographic Features According to Preprocedural β-Blockers Use.
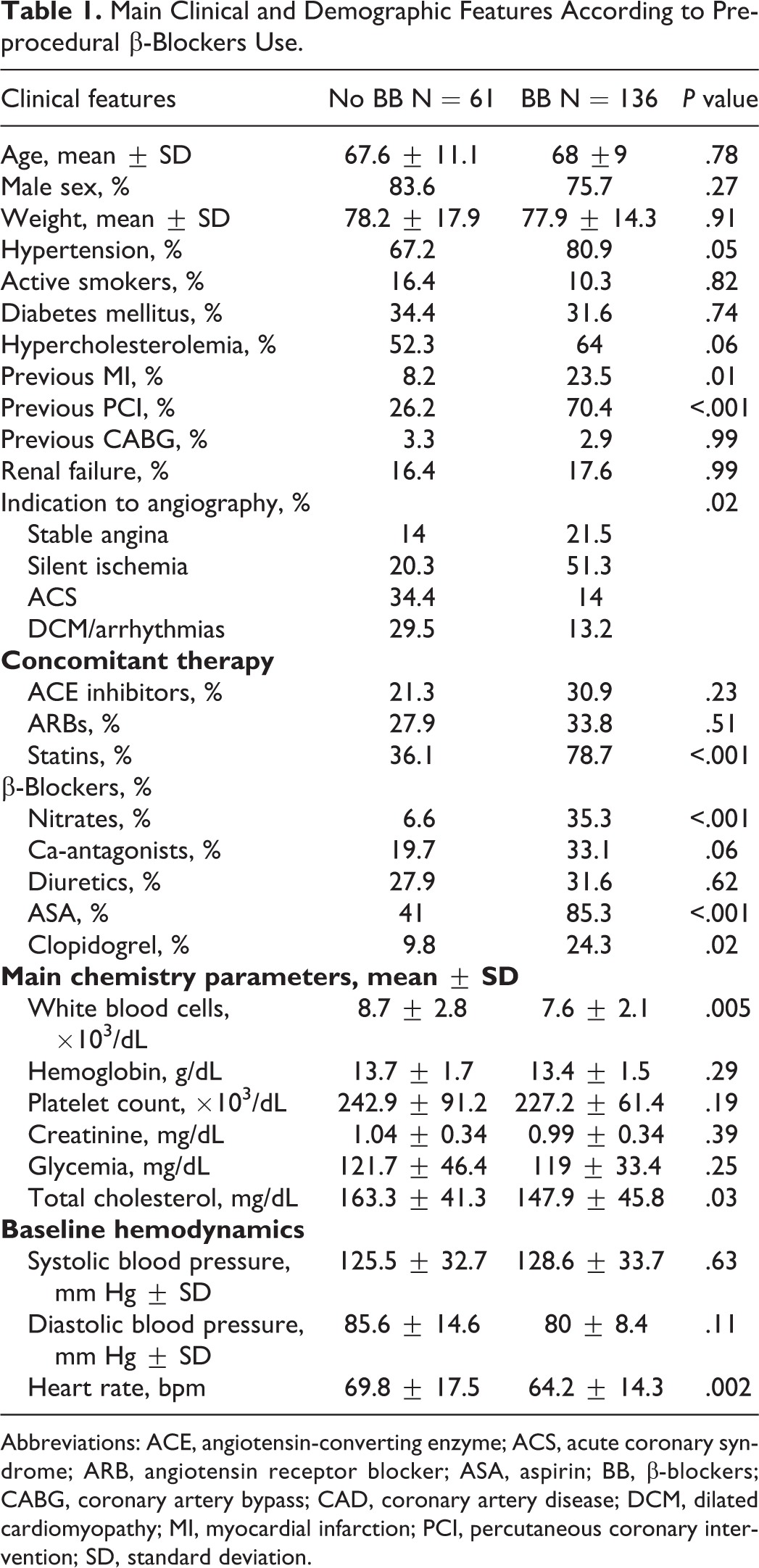
Abbreviations: ACE, angiotensin-converting enzyme; ACS, acute coronary syndrome; ARB, angiotensin receptor blocker; ASA, aspirin; BB, β-blockers; CABG, coronary artery bypass; CAD, coronary artery disease; DCM, dilated cardiomyopathy; MI, myocardial infarction; PCI, percutaneous coronary intervention; SD, standard deviation.
No difference in the quantitative parameters of coronary lesions were observed (Table 2). Mean iFR values were slightly more elevated in patients on β-blockers (0.94 ± 0.06 vs 0.92 ± 0.06, P = .11).
Angiographic Characteristics According to Preprocedural BB.
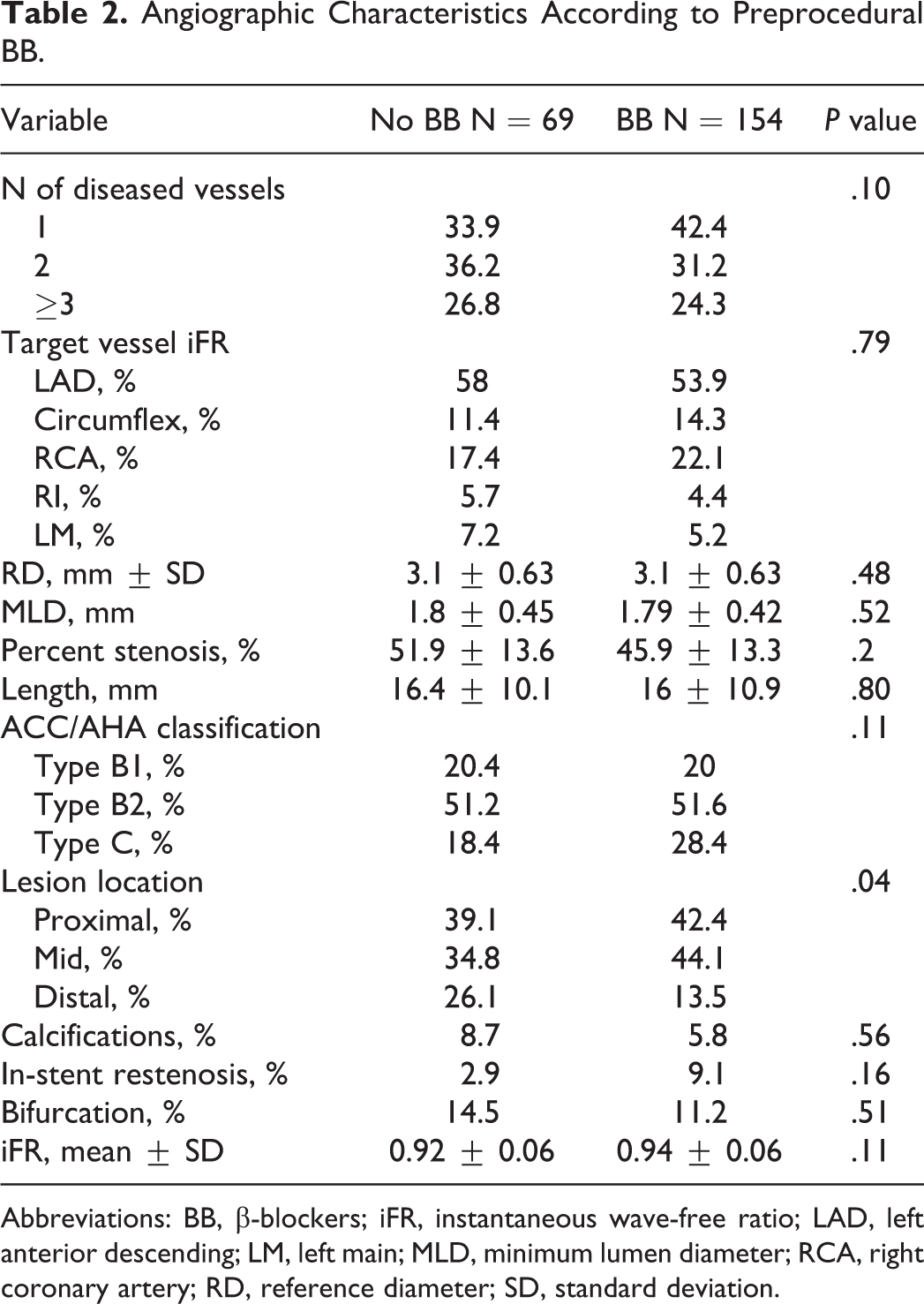
Abbreviations: BB, β-blockers; iFR, instantaneous wave-free ratio; LAD, left anterior descending; LM, left main; MLD, minimum lumen diameter; RCA, right coronary artery; RD, reference diameter; SD, standard deviation.
The rate of positive iFR was significantly lower among patients receiving β-blockers (14.9% vs 27.5%, P = .04), as depicted in Figure 1 and Table 3.
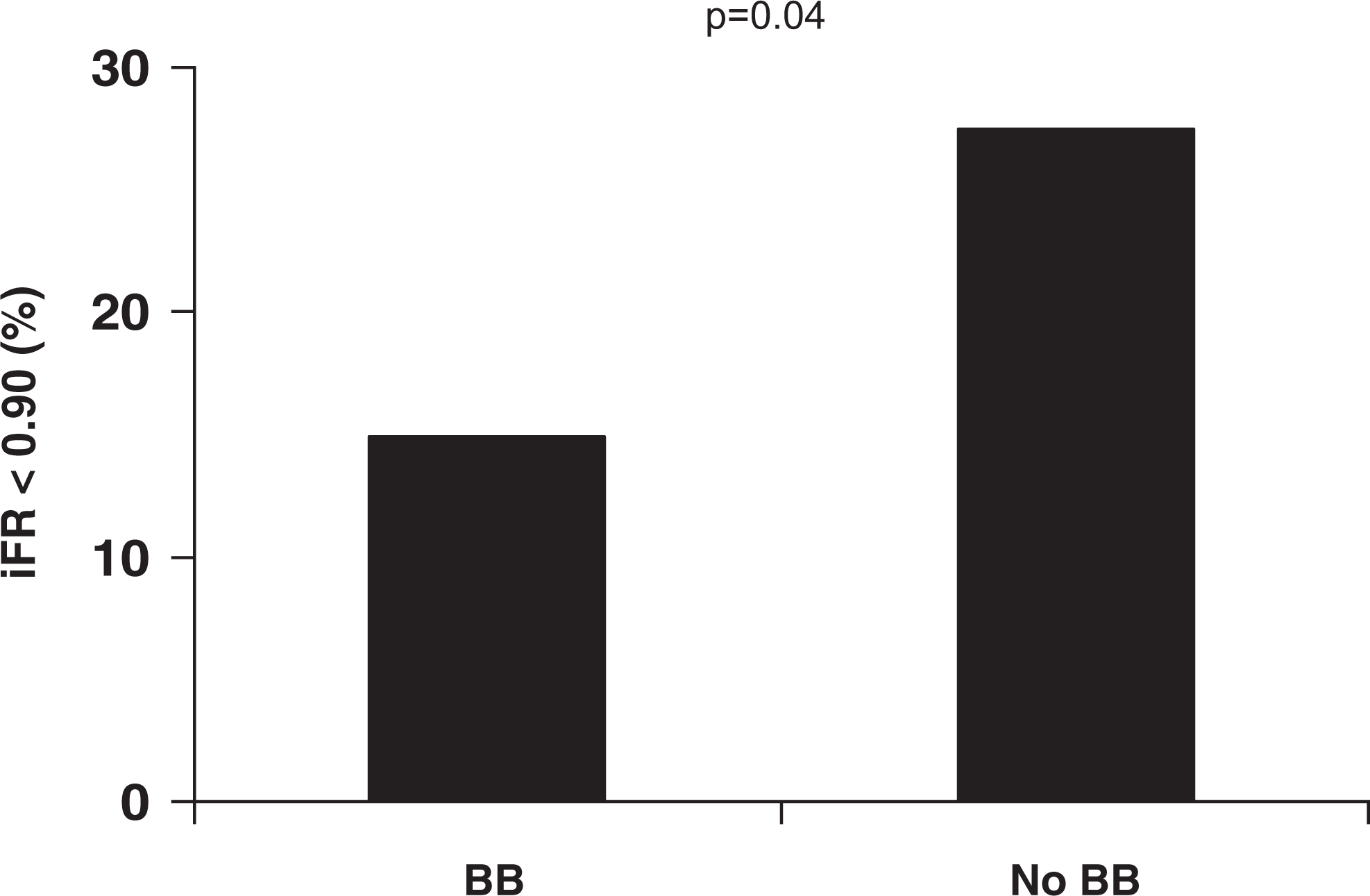
Bar graph showing the percentage of positive (<0.90) instantaneous wave-free ratio according to preprocedural β-blockers.
Multivariable Model for the Prediction of a Positive iFR (Instantaneous Wave-Free Ratio).
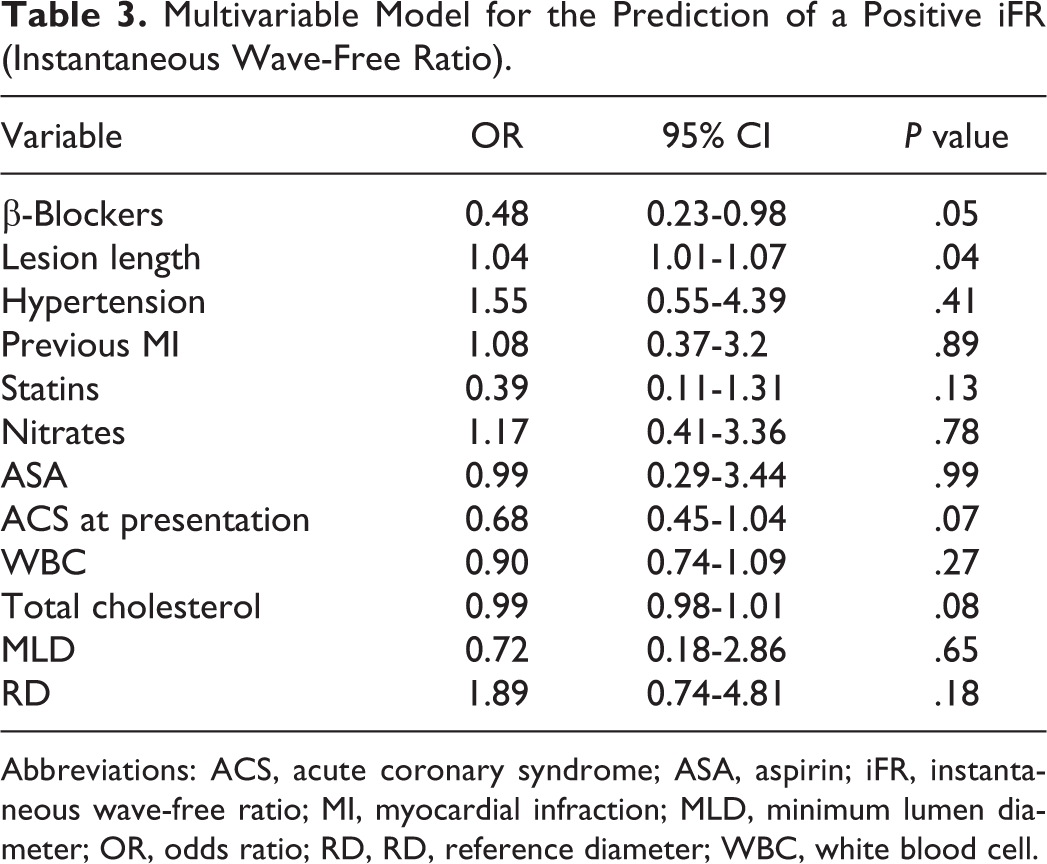
Abbreviations: ACS, acute coronary syndrome; ASA, aspirin; iFR, instantaneous wave-free ratio; MI, myocardial infraction; MLD, minimum lumen diameter; OR, odds ratio; RD, RD, reference diameter; WBC, white blood cell.
In fact, at multivariate analysis, the use of β-blockers emerged as the only nonlesion-related predictor of the significance of coronary stenoses (odds ratio [OR] = 0.48; 95% CI = 0.23-0.98; P = .05), together with lesion length (OR = 1.04; 95% CI = 1.01-1.07; P = .007).
Discussion
The present study represents the first attempt to assess the impact of β-blockers on the functional assessment of intermediate coronary stenoses with the use of iFR. We demonstrate that preprocedural β-blockers could reduce the rate of pathological positive iFR, representing the only nonlesion-related factor affecting the ischemic potential of intermediate lesions.
Pharmacological therapy represents a cardinal point in the management of patients with CAD, offering clinical and prognostic benefits either in patients with acute presentation or chronic coronary syndrome and irrespective of percutaneous or surgical coronary revascularization. 1,21
In particular, β-blockers represent a fundamental class of drugs, for their multiple effects on ischemia, symptoms, and prognosis. In fact, several studies have shown a reduction of mortality with β-blockers, especially in post-MI patients with their earlier initiation. 22 –24
Indeed, β-blockers can directly interfere with the pathophysiological mechanisms of ischemia, by decreasing heart rate, blood pressure, and myocardial oxygen consumption, but also conditioning coronary microvascular resistances and coronary flow reserve. In a previous study by Tagliamonte et al., transthoracic Doppler-derived coronary flow velocity during hyperemia was increased after the administration of bisoprolol. 25
A similar conclusion has been reached by Galderisi and D’Errico, demonstrating that coronary blood flow reserve could be increased especially with third-generation β-blockers, mainly in consequence of alpha-adrenergic blockade or to a nitric oxide-mediated effect. 26
Based on their anti-ischemic properties, it has been suggested that β-blockers may reduce the sensitivity of stress tests in the detection of ischemia. In particular, the positive effects of β-blockers on dipyridamole stress could be largely independent of the effect of heart rate, possibly involving a direct antisteal effect. 27
In a limited subset of patients, intravenous metoprolol did not show any significant impact on FFR, 14 despite causing a decrease in baseline heart rate, coronary vascular resistance, and increasing coronary flow. Similar results were achieved by Barbato et al, 28 documenting that alpha but not β-blockers could affect adenosine induced vasodilatation and FFR results. In fact, the latter drugs produced a similar decrease in aortic and distal pressure, resulting into an unaltered ratio.
However, different results could be expected with iFR, being largely dependent on the duration of the diastolic period and hemodynamic parameters. In fact, Ebihara et al 29 observed in 195 patients (259 lesions) that the diagnostic performance of the iFR, as compared to FFR, was strictly conditioned by the rate pressure product (RPP). In their study, the best cutoff value of the iFR for predicting a pathological FFR was 0.90, in accordance to guidelines, however in low-RPP group it raised to 0.93, while for the high-RPP group was at 0.82, thus risking underestimation and overestimation of the severity of ischemia in these patients.
In our study, preprocedural β-blockers were associated with a reduction of heart rate, and slightly more elevated mean values of iFR, and a significantly lower rate of positive iFR. In fact, at multivariate analysis, β-blockers and lesion length emerged as the only independent predictors of iFR <0.90. Similar results were shown in the multicentric CONTRAST study, where the absence of β-blockers and heart rate could condition the results of iFR, being associated with its higher values, discordant from FFR. 3
Anyhow, the French study 30 and the present study only represent hypothesis generating analyses, and further dedicated prospective studies for the evaluation of β-blockers are indicated to confirm these findings. Moreover, their role in conditioning the sensitivity of iFR and the prognostic implications of an eventual underestimation of ischemia still need to be further elucidated. Indeed, the majority of the trials so far conducted with iFR, enrolling a population with a larger use of β-blockers, showed no prognostic impact. Since silent ischemia and not the value of iFR is the major determinant of the outcomes, it might be argued that the avoidance of ischemia with β-blockers could have prevented any observations of prognostic difference.
Therefore, future larger randomized trials are indicated to define whether a discontinuation of β-blockers should be recommended before performing iFR or rather their use allows to prevent unnecessary, nonischemia-driven PCI and whether FFR should still be preferred over iFR in these patients.
Limitations
A limitation is the small sample size of the population and the imbalance between the groups with and without β-blockers, possibly contributing to the lack of significant difference when considering iFR mean values. However, our study was larger than previous studies evaluating the impact of β-blockers administration on coronary reserve and FFR.
In addition, we included a heterogeneous population, differing for major risk factors and cardiovascular history. In fact, the β-blocker group had a larger proportion of patients with previous PCI and stenting, which could have affected the physiology of the coronary circulation. However, despite that more extensive disease could be expected in these patients, the angiographic characteristics were similar in both groups. Similarly, the use of antiplatelet agents was higher in association with β-blockers. However, we did include a consecutive cohort of patients and also those undergoing coronary angiography for nonatherosclerotic indications, as patients with valvular heart disease, arrhythmias, and cardiomyopathy, in whom the indication to antiplatelet therapy is less stringent.
Another limitation can be represented by the lack of evaluation of coronary lesions by an independent method of functional assessment, as FFR. Therefore, we cannot define the correctness of the classification of coronary stenoses by the use of iFR in patients with or without β-blockers.
In addition, the type and dosing of β-blocker were not available for the overall cohort of the patients and, therefore, we could not provide any further stratification. Finally, we did not perform a systematic follow-up of our patients. Thus, we could not assess the prognostic impact of iFR and β-blockers on the risk of future cardiovascular events.
Conclusion
Among patients undergoing functional assessment of intermediate coronary lesions by iFR, preprocedural β-blockers were associated with higher absolute values and a lower rate of positive iFR. In fact, the use of β-blockers emerged as the only nonlesion-related factor conditioning the ischemic significance of coronary stenoses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.