
Abstract
Endothelial dysfunction (ED) plays a substantial role in the pathogenesis of atherosclerosis and some other vascular diseases. ED has been demonstrated in patients with hypercholesterolemia, diabetes, smoking, hypertension, and in patients with atherosclerotic disease. Besides classical risk factors, ED is affected by chronic inflammatory diseases and acute infections, particularly viral diseases. Causes of ED include oxidative stress, inflammation, and shear stress, which decrease the bioavailability of nitric oxide. Markers of ED have been sought, particularly circulating markers. Using these tests, it is possible to evaluate the response to harmful effects of risk factors and the effects of treatment on vessel wall function. Endothelial dysfunction is significantly and directly correlated with the occurrence of cardiac events and the risk of cardiac events increase as ED worsens. Because endothelial function plays a central role in atherogenesis it became a therapeutic target. Endothelial dysfunction is reversible and its improvement may be achieved by elimination of risk factors, inhibitors of endothelium-derived contracting factors (angiotensin-converting enzyme), smoking cessation, lipid-lowering drugs, diet, and physical exercise. By reversing ED, it is possible to restore vascular function.
Keywords
Introduction
Atherosclerosis is a chronic progressive vascular disease which starts early in life and has a long asymptomatic phase. 1 Risk factors initiate and accelerate the progression of the disease through deterioration of endothelial function (EF). 2 The endothelium is an active inner layer of the blood vessel and is the key regulator of vascular homeostasis. 3 Endothelial dysfunction (ED) is the earliest measurable deterioration of vessel wall in atherogenesis. 4 Endothelial dysfunction precedes the development of morphological atherosclerotic changes and contributes to the clinical events related to the progression of atherosclerosis. 5 Therefore, investigating EF provides not only insight into pathophysiology but also represents an opportunity to detect early phases of the disease, to stratify cardiovascular (CV) risk, and to assess the effect of treatments. 6,7 As ED is reversible with treatment of risk factors, it is a potential therapeutic target and measure of efficacy of preventive procedures.
Role of Endothelium in Vascular Homeostasis
The endothelium is an active organ that plays a crucial role in maintaining vascular homeostasis. It produces several factors that regulate vascular tone, adhesion of circulating inflammatory cells to the endothelium, smooth muscle cell proliferation, coagulation, and vessel wall inflammation.
8
One of the most important functions of the endothelium is maintaining the delicate balance between vasodilation and vasoconstriction. Vasodilation is mainly mediated by nitric oxide (NO) and prostacyclin, while vasoconstriction is maintained by substances such as endothelin-1 (ET-1), angiotensin II, and thromboxane A2.
9
Nitric oxide is not only the most potent endogenous vasodilator in the body but it inhibits platelet aggregation, inflammation, oxidative stress, smooth muscle cell proliferation, and leukocytes adhesion.
10
Nitric oxide is synthesized from
One of the most important underlying mechanisms for the development of ED is oxidative stress. 14 Most CV risk factors upregulate intracellular oxidative stress and reactive oxygen species (ROS). This leads to generation of hydrogen peroxide and NO inactivation. An imbalance between NO and ROS promotes ED and leads to CV complications. In healthy physiological conditions, eNOS is responsible for vascular NO production. However, in the pathological uncoupled state, eNOS becomes a ROS generator, which results in formation of peroxide. 15
Endothelial function is closely related to the endothelial glycocalyx (GCX), which plays a major role in the health and disease status. 16 It is vital for homeostasis and disruption of its structure and function plays an important role in several pathologic conditions and represents a potential surrogate marker for endothelial injury. 17 Glycocalyx covers luminal surface of vascular endothelium. It comprises membrane-bound negatively charged proteoglycans, glycoproteins, glycolipids, and glycosaminoglycans. 16 Therefore, the GCX determines the functional capability of the vascular endothelium. Dysfunction of GCX has been associated with disease status, such as diabetes and other risk factors for atherosclerosis, inflammatory conditions, and ischemia/reperfusion injury and as such may represent novel therapeutic target. 18
Inflammation and ED
Inflammation represents a common underlying mechanism of ED, and there is a close relationship between oxidative stress and inflammation. 19 Healthy endothelium controls vascular inflammation by releasing NO. However, a dysfunctional endothelium will promote ROS generation and aggravate vascular inflammation. Evidence suggests that there is an association between ED and inflammatory markers. C-reactive protein (CRP) directly contributes to the development of atherosclerosis by deposition on the endothelial intima, which precedes migration of inflammatory cells into the vessel wall. 20 In addition, CRP inhibits the synthesis of NO and affects its bioavailability, which increases oxidative stress. C-reactive protein also directly acts through oxidized low-density lipoprotein (LDL) receptor-1, which induces ED. 21 Involvement of inflammation in ED is also indicated by the relationship between levels of circulating inflammatory markers (interleukin-6 [IL-6], CRP) and markers of ED (von Willebrand factor [vWF], P-selectin). 22 In addition, inflammatory cytokines induce endothelial cells and leukocytes to express adhesion molecules, E-selectin, P-selectin, and IL-6, which worsen ED. 23 Consequently, monocytes adhere to the endothelium and transform into macrophages, which accumulate lipids and become foam cells; thus, formation of atheroma starts. Thus, ED plays a key role in the initiation and progression of atherosclerotic plaques. 24
Shear Stress
Atherosclerotic lesions usually occur at specific arterial regions, such as bifurcations, branching and in the inner aspect of curved segments of coronary arteries. 25 Local flow with disturbed shear stress modulates endothelial gene expression; consequently, bioavailability of NO and prostacyclin production is decreased, which results in ED and formation of atherosclerotic lesions. 26 Maintenance of physiologic, laminar shear stress is of crucial importance for normal vascular functioning and is atheroprotective. 27 Disturbed shear stress, which is a consequence of nonlaminar flow, causes damage of endothelial cells and leukocyte adhesion, as well as movement of inflammatory cells, LDL cholesterol, and other pro-atherogenic molecules into the vessel wall. 28
Therefore, decreased shear stress is considered as a harmful mechanism which damages the endothelium and CV system. High shear stress as found in laminar flow promotes endothelial cell survival and promote vasodilatation and anticoagulation. 29
Risk Factors of Atherosclerosis and ED
Endothelial dysfunction has been demonstrated in patients with different risk factors for atherosclerosis, such as hypercholesterolemia, hypertension, smoking, diabetes, and in patients with preclinical or clinical atherosclerotic disease. 30,31
Dyslipidemia
High levels of LDL cholesterol and low levels of high-density lipoprotein (HDL) cholesterol are independently associated with ED. Hypercholesterolemia is associated with impaired endothelium-dependent vasodilation of coronary and peripheral conduit and resistance vessels. 32 Dyslipidemia is associated with oxidative stress caused by increased reactive species production. 33 Consequently, bioavailability of NO is decreased. Decreased bioavailability of NO promotes oxidation of LDL and ED. 34
One of the mechanisms through which dyslipidemia induces ED includes oxidative stress, increasing plasma levels of asymmetric dimethylarginine (ADMA), and finally oxidation of LDL. Asymmetric dimethylarginine is an endogenous inhibitor of eNOS and competes with
Hypertension
A large body of evidence indicates that ED is a characteristic of patients with essential hypertension. 35,36 Endothelial dysfunction associated with essential hypertension is characterized by impaired NO bioavailability, determined by ROS, which causes NO breakdown. 37 Reactive oxygen species, mainly superoxide anions, combine and destroy NO, producing peroxide nitrates, which have several negative effects on vascular function and structure. 38 Further, an interaction between NO system and ET-1 can participate in the pathogenesis of ED. 39 Vasoconstrictor activity has been found to be increased in parallel with diminished NO availability. 40
Recently, inflammation has been reported as having a causative relationship with the development of hypertension, and it has been found that inhibiting inflammatory pathways can impede the process of developing of hypertension and ED. 41
The relation between level of blood pressure and EF is not completely elucidated. Namely, ED was not found in hypertensive patients without a family history of CV diseases and without other risk factors of atherosclerosis, but only in patients with hypertension, accompanied by other risk factors of atherosclerosis. 42
It is unclear whether ED is a primary abnormality or a consequence of the elevated blood pressure. Data in animal models are in favor of direct damage of endothelial cells secondary to a prolonged increase of the hemodynamic load and changes in shear stress. Endothelial dysfunction observed in hypertension appears to be a consequence of high blood pressure since some antihypertensive treatments normalize EF. However, in normotensive offspring of hypertensive parents, an early alteration of endothelium-dependent vasodilation in the forearm was observed. 43 We also found impaired EF in offspring of parents with essential hypertension, although their blood pressure was within the normal range. 44 These findings suggest a role for genetic mechanisms in the genesis of ED in hypertension.
Smoking
Experimental evidence has suggested that smoking induces ED. Different studies showed that endothelium-dependent flow-mediated dilation (FMD) of the brachial artery is significantly impaired in smokers compared with control patients. Endothelial dysfunction progresses with the duration of smoking and with the number of cigarettes smoked. 45 This dose-dependence of smoking-related ED and its reversibility after smoking cessation support the close interrelationship between smoking and EF. 46 Decreased FMD in smokers could be the result of inactivation of NO by oxygen-derived free radicals through activation of inflammation and enhanced release of ET-1, recognized as a potent vasoconstrictor. The exact components of the cigarette smoke responsible for ED and vasculopathy are not known, although nicotine and carbon monoxide have been implicated. Endothelial dysfunction is an acute phenomenon but is most probably a consequence of chronic influence of nicotine. 47,48
Therefore, smoking is associated with oxidative stress, inflammation, and the release of other circulating factors that are associated with endothelial injury. Furthermore, smoking has been reported to decrease HDL cholesterol levels, which is known to have antiatherosclerotic properties and improves EF. 49,50
Endothelial dysfunction caused by smoking is reversible and improves after smoking cessation. After 3 months of smoking cessation with nicotine replacement therapy, EF and arterial stiffness significantly improved and there was a decrease in inflammatory marker levels. 51 If healthy smokers continue smoking, vascular function could be further damaged.
Diabetes Mellitus
Evidence that ED occurs in diabetic patients is supported by an elevated plasma concentration of the vWF as well as impaired prostacyclin and plasminogen activator release. 52 Hyperglycemia impairs EF. 53,54 Even in normoglycemic patients who have higher risk for developing diabetes and insulin resistance, ED was observed during an oral glucose tolerance test. 53 In patients with diabetes, ED is a consequence of decreased synthesis of NO and increased production of vasoconstrictor substances. 54 Oxidative stress and eNOS uncoupling play an important role in developing ED. 55 Hyperglycemia also stimulates generation of advanced glycation of products which accumulate in the vessel wall and cause ED, which then impede NO activity. 56 Flow-mediated endothelial-dependent vasodilation capability of the brachial artery was shown to be related to microalbuminuria. It indicates that in diabetic patients, ED contributes to overt vascular complications, particularly at the microvascular level. 57
Metabolic syndrome is associated with increased risk for type 2 diabetes mellitus and vascular events. 58 All components of metabolic syndrome exert adverse events on the endothelium and ED most probably plays a role in the pathogenesis of atherosclerosis and might also increase the risk for insulin resistance. 59
Aging
Is an important determinant of CV risk. Increasing age and the associated processes have been considered as the main factors that cause ED in the elderly. The mechanism of ED during aging is most probably based on reduction in NO bioavailability and increased cyclooxygenase-derived constrictor factors. Studies showed that there is a reduced expression of activity eNOS and decreased bioavailability of NO in older animals. 60 With aging, there is also an increase of endothelium-derived contracting factors such as ET-1 and cyclooxygenase-derived prostanoids as well as ROS production. 61 Compromised EF is most probably a central mechanism by which aging promotes vascular pathology. The attenuation of EF, associated with the impairment of angiogenic process and pathological remodeling of the microcirculation, contributes to compromised tissue perfusion and causes functional decline of different organs in elderly people. 62
Different studies also reported ED in patients with other nonclassical risk factors of atherosclerosis, such as hyperhomocysteinemia (Figure 1). 63 Further, it was shown that brachial artery flow-mediated endothelium-dependent dilation capability is reduced in patients with metabolic syndrome 64 and in overweight patients. In obese patients, ED was closely related to systemic inflammatory markers (CRP, interleukins) and adhesion molecules. 65
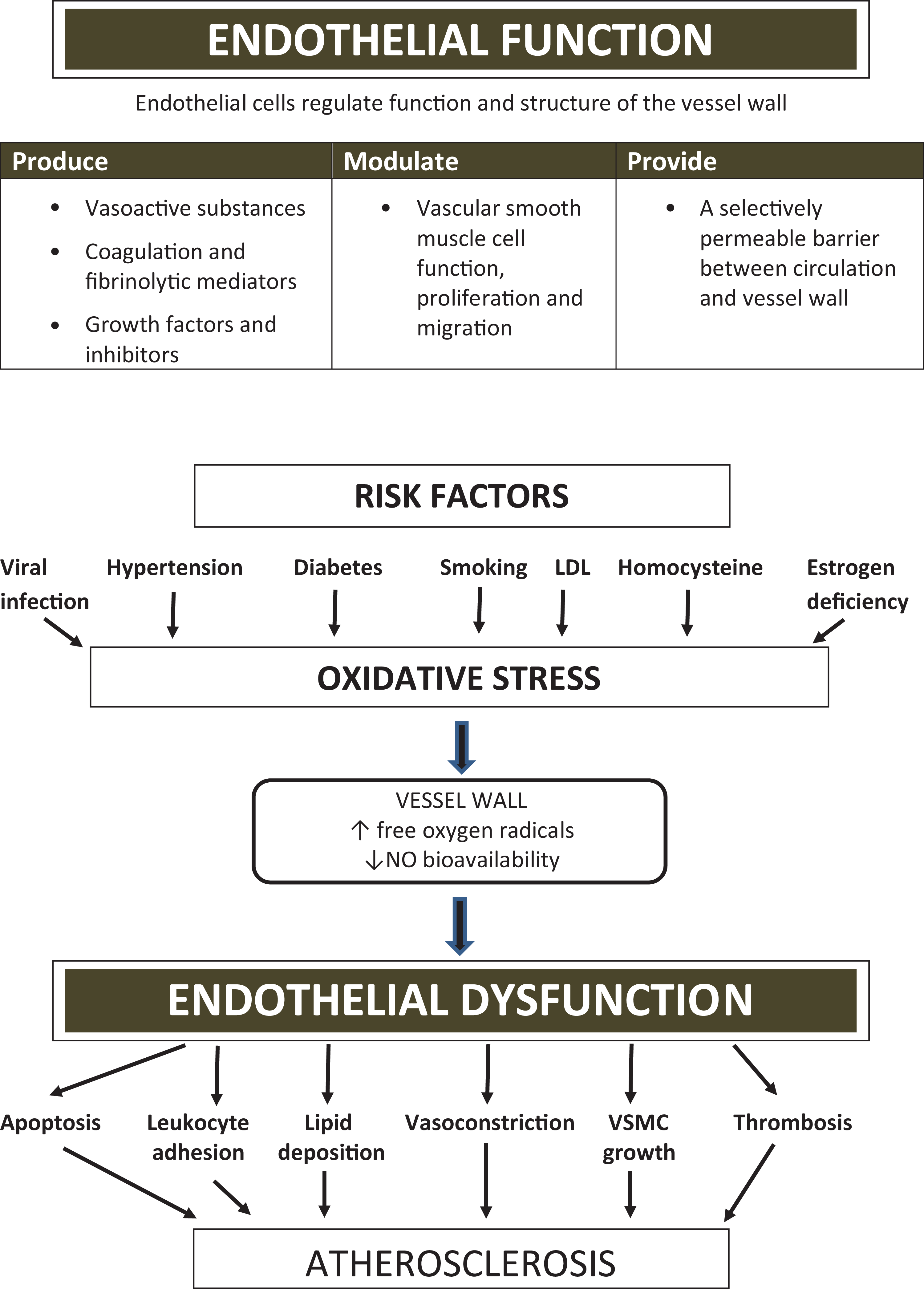
Schematic presentation of endothelial function and dysfunction. NO indicates nitrogen oxide; VSMC, vascular smooth muscle cells.
It was demonstrated that ED progresses with the duration of hypertension, diabetes, or smoking and that a close relationship exists between the intensity of an individual risk factor or the number of presented risk factors and EF. 44,45,66
Assessment of EF
Functional Methods for Investigation of EF
As ED is an index of risk factor burden and an early marker of atherothrombotic disease, there is considerable interest in the measurement and determination of EF. There are different invasive and noninvasive techniques for exploring various aspects of altered EF. Direct invasive techniques are used to investigate the functional capability of coronary macro- and microcirculation; this involves intracoronary infusion of endothelium-dependent vasodilatory substances. 67 However, because of invasiveness, these investigations are usually only performed during coronary angiography.
As ED is diffuse systemic disorder, it is expected that all territories of vessels are simultaneously affected. Therefore, peripheral arteries, because of their easy accessibility, represent the basis for noninvasive assessment of ED. Flow-mediated dilation of peripheral conduit arteries (brachial) is one of the most widely used tests of EF. 68 This technique measures endothelial-dependent vasomotor response, but it does not give insight into the control of arterial tone at rest.
Low-flow-mediated constriction (L-FMC) provides complementary information on vasodilatory capability of the investigated artery. It registers the decrease in the forearm conduit artery diameter that occurs in response to decreased blood flow during arterial occlusion. 69 Low-flow-mediated constriction response is not based on NO availability but it is most probably mediated by other substances. Simultaneous determination of FMD and L-FMC provides comprehensive information on vascular homeostasis. Peripheral arterial tonometry evaluates pulse valve amplitude, which is also an indicator of EF. Peripheral arterial tonometry measures flow response of hyperemia, which depends on the EF of small arteries. Therefore, it represents EF of the microcirculation. 70 Determination of venous EF is more complicated. Available techniques are invasive and have limited reproducibility. However, as EF is expected to be a systemic disorder, determination of the EF of peripheral arteries provides insight into EF of different arterial territories and venous functional status.
Circulating Markers of EF
Endothelial injury may result in the release of various factors that can be detected in circulation and can be potentially used as markers of ED.
Endothelin-1 is an endothelium-derived peptide that has powerful vasoconstrictor properties. Increased levels of ET-1 have been demonstrated in conditions associated with ED, such as atherosclerosis, hypercholesterolemia, and cigarette smoking. 71 ET-1 stimulates the NADH/NADPH oxidative system, which was identified as the major source of ROS in phagocytes and platelets. 72 Reactive oxygen species production is closely linked to NO generation and elevated levels of ROS lead to low NO bioavailability and ED. 73 Results of these investigations indicate that circulating ET-1 levels may represent a marker of ED.
Von Willebrand factor is a glycoprotein synthesized mainly by vascular endothelial cells. 74 It has important functions in hemostasis, particularly in coagulation and the formation of platelet aggregates at sites of endothelial damage. 75 Its levels are elevated in situations characterized by endothelial damage and it has been suggested that injured endothelial cells leak vWF, leading to increased plasma levels. 76 In patients with preexisting vascular disease, vWF is significantly predictive for adverse cardiac events including deaths. 77 Levels typically rise during the course of acute coronary syndrome and the level of vWF is an independent predictor of adverse clinical outcome in these patients. 78
Tissue plasminogen activator is a protein released by endothelial cells. It activates the reaction in which plasminogen is converted to plasmin. Tissue plasminogen activator regulates fibrinolytic activity of blood in balance with plasminogen activator inhibitor-1, another product of endothelial cells. 79 Therefore, different proteins involved in hemostasis are synthesized by endothelial cells and have been proposed as markers of ED. 80
Adhesion molecules stimulate binding of circulating leukocytes to the vascular endothelium and other inflammatory cells migration into the subendothelial space, which represent major processes in the development of atherosclerosis. 81 These events are mediated via diverse cellular adhesion molecules that are expressed on the surface of the vascular endothelial cells: vascular cell adhesion molecule-1 (VCAM-1), endothelial-leukocyte adhesion molecules-1 (E-selectin), intracellular adhesion molecule-1, and P-selectin. 82 The studies have suggested that circulating adhesion molecules may serve as markers of endothelial damage and/or atherosclerosis. 13
Asymmetric dimethylarginine has emerged as an independent risk factor and a promising marker of ED. It inhibits eNOS resulting in decreased bioavailability of NO. 83 Increased levels of ADMA and adhesion molecules have been documented in patients with different risk factors, including dyslipidemia, hypercholesterolemia, hypertension, and atherosclerotic CV disease. Therefore, ADMA might be a useful measure of endothelial status and a potential risk factor for CV disease.
Recently, new circulating markers are being explored, such as endothelial microparticles, endocan, and endoglin. Some of them are thought to be suitable for clinical setting. 84 Further, other biomarkers such as ischemia-modified albumin pentraxin-3, E-selectin, angiopoietin, endothelial cell-specific molecule-1 can be used to evaluate ED. 85
Involvement of ED in Different Diseases
Endothelial Dysfunction and CV Disease
In case of ED in atherosclerotic human coronary arteries, endothelium-mediated relaxation is impaired and shifts the balance in favor of vasoconstriction in response to a variety of stimuli, as for example, exercise, mental stress, and cold exposure. 86 Clinical studies demonstrated that abnormal constrictor responses to acetylcholine are not only observed in angiographically diseased epicardial arteries but also in patients with entirely smooth epicardial arteries in the presence of risk factors for coronary artery disease. 87,88
Coronary Artery Disease
Endothelial vasodilator dysfunction appears to render the atherosclerotic vessels more sensitive to the constrictive effects of catecholamines released by daily life stimuli and results in the pathogenesis of inappropriate vasoconstriction. This represents a fundamental functional disturbance in the vascular biology of atherosclerosis. 89,90
In addition to impaired FMD of the epicardial conductance vessels in atherosclerosis, the vasodilator function of the coronary resistance vessels is adversely affected. 91 A defective endothelium-mediated vasodilator function may therefore potentiate known trigger mechanisms of myocardial ischemia and thereby induce a mismatch between myocardial oxygen supply and demand. Even through the changes in luminal diameter produced by inappropriate vasoconstriction of the epicardial vessel in response to sympathetic activation are usually <30%, such an increase in the arterial tone might be enough to convert a subcritical stenosis into a critical one. An ensuing decrease in blood flow and impaired FMD of the resistance vessels will further reduce coronary flow reserve. 88,89
Endothelial dysfunction might also be related to circadian variation in transient ischemic episodes, being most frequent in the morning hours. 92 Indeed, vascular resistance caused by ED has been shown to be elevated in the morning hours. 93
In unstable angina pectoris, which is mostly caused by plaque rupture, a number of vasoactive substances are released into the coronary circulation, mostly notably serotonin and thrombin. 94 Both substances have been shown to exert potent vasoconstrictor effects in the presence of dysfunctional endothelium. 95 Thus, ED may cause a constrictor response and importantly magnify the ischemic response in the distal vascular bed. 96 Whatever the mechanism of acute myocardial infarction, inappropriate dilation of resistance vessels distal to the site of coronary thrombosis could influence the size of myocardial necrosis. 97 This is one of the reasons that acute events and consequences are unrelated to stenosis severity. Further, in the vascular bed of the non-infarct-related arteries in the presence of ED, enhanced response of resistance vessels to systemic and local neurohormonal constrictor stimuli could increase the extent of ischemia in the periphery of the infracted area and reduce collateral flow to the infarct-related arterial bed. Thus, ED is contributing to the acute impairment of ventricular function and to the extension of necrosis. 97,98
Endothelial dysfunction could also be responsible for the no-reflow phenomenon. Endothelial cells are at least as susceptible as myocytes to acute ischemic injury and reperfusion damage. This is evident from the profound loss of capacity of myocardium to be reperfused, following severe ischemia which is known as the “no-reflow phenomenon.” However, this inability to perfuse dead tissue also compromises perfusion of the immediately adjacent viable tissue, which is a region of “low flow” where, despite their dilation, many capillaries are incompetent. 99
Therefore, EF plays an important role in acute coronary events and determines clinical outcome of acute myocardial infarction.
Congestive heart failure is one of the most prevalent CV diseases. Patients with heart failure have reduced cardiac output, which results in reduced blood flow and negative shear stress. Consequently, the production of free-oxygen radicals is increased, and bioavailability of NO is decreased. 100 Besides increased oxidative stress and deteriorated blood flow, EF is provoked also by an increased systemic inflammatory response and neurohormonal activation. Therefore, ED is involved in the progression of heart failure and CV events. It is also an independent predictor of survival of patients with heart failure. 101 Heart failure is not a limited entity at the heart level but causes heterogeneous damage of organ function, including pulmonary, renal, peripheral vascular, and skeletal muscle dysfunction, and ED could be the common mechanism responsible for the functional deterioration of different organs in these patients. 4,102
Chronic Inflammatory Disease
Inflammation is responsible for ED in patients with atherosclerotic diseases and risk factors. As well as in other inflammatory diseases it was shown that ED is closely related to chronic inflammatory disease such as inflammatory arthritis and connective tissue disease. 103 In patients with connective tissue disease, the presence of inflammation and autoantibodies provokes endothelial cell activation and injury, which may provoke the development of atherosclerosis. 104 Chronic inflammation, together with the traditional risk factors, contributes to ED, which is most probably responsible for premature and accelerated atherosclerosis in patients with chronic inflammatory disease. 105 Decreased endothelium-dependent dilation capability of peripheral arteries was shown in patients with systemic lupus erythematosus and was closely related to increased levels of inflammatory markers: high-sensitivity CRP, fibrinogen, and VCAM-1. 106 Endothelial dysfunction is also considered one of the etiological factors of inflammatory bowel disease and is considered as an initial step in the pathogenesis of atherosclerosis in these patients. 107
Viral Infections
Viral infections cause acute inflammatory disease such as influenza and are involved in ED in different territories, including the pulmonary circulation. 108 In these patients, ED was shown by reduced endothelium-dependent FMD of peripheral arteries. 109 Endothelial dysfunction related to acute viral illness may also explain increasing incidence of acute myocardial infarction during influenza and other acute viral infections. Viral illness can cause or exacerbate coronary atherosclerosis by activating inflammatory pathways and deteriorating EF. 110
Finally, recent data indicate that CV and pulmonary complications in patients with coronavirus (COVID-19) infection may be a consequence of ED and that frequent comorbidities such as hypertension, diabetes, obesity cause increased mortality through ED as a common underlying mechanism. 111 In patients with coronavirus infection and development of acute respiratory distress syndrome, elevation of vWF was observed, which points toward endothelial stimulation and damage. 112 Interestingly, endothelial cells express angiotensin-converting enzyme 2 (ACE2)—the receptor for severe acute respiratory syndrome (SARS-CoV2), thus possibly mediating endothelial activation. 113 It seems that the virus is primarily targeting the endothelium, one of the largest and most active organs in the human body. Therefore, some researchers suggest that COVID-19 is a primary endothelial disease. 114
Endothelium-Therapeutic Target
Endothelial dysfunction is the earliest measurable functional deterioration of vessel wall in atherogenesis and it is potentially reversible. Therefore, treatment of ED may have important clinical implications. The main goal of this approach is elimination and treatment of risk factors of atherosclerosis that improve EF. Despite their diversity, most of risk factors have common pathophysiologic mechanisms that accelerate atherosclerosis. 115 These factors are commonly associated with activation of inflammation and reduced NO bioavailability.
Endothelial therapy should include lifestyle modification, including physical exercise, smoking cessation, diet, and management of the factors which represent major promotors of atherosclerosis—hypertension, dyslipidemia, diabetes, and obesity. Furthermore, in established CV disease, improvement of EF inhibits the progression of underlying disease.
Physical exercise
There is clear evidence that physical activity improves EF, particularly in individuals at increased CV risk. 116,117 Physical exercise improves EF and reduces CV risk in older individuals, postmenopausal women and patients with dyslipidemia. 118 In addition, exercise training leads to improved EF in patients with coronary heart disease and heart failure. 119 Also, weight loss in overweight patients improves ED. 120
Smoking cessation
Endothelial dysfunction provoked by smoking is a consequence of increased levels of reactive oxygen radicals and reduced NO bioavailability. 121 Cigarette smoking is associated with dose-related impairment of EF. 45,66 Endothelial dysfunction is reversible and it was shown that smoking cessation of 1 year significantly improved EF. 122 Also, passive smoking was shown to impair the EF in healthy patients, which proved to be reversible after cessation of smoking exposure. 123
Secondary endothelial therapy
The goal of secondary endothelial treatment is to improve and prevent progression of ED in patients with modifiable risk factors (hypertension, diabetes, dyslipidemia), nonmodifiable conditions (aging, sex, menopause, and in coronary or peripheral arterial disease, heart failure). Pharmacological treatment of underlying factors which represent the risk for atherosclerotic CV complications was shown to restore EF, and in some instances, reduce the risk for CV disease.
Angiotensin-converting enzyme inhibitors beyond inhibiting the renin–angiotensin system diminish the inactivation of bradykinin, thus leading to an augmentation of NO release. 124,125 Angiotensin-converting enzyme inhibitors, also through improvement of EF, prevent pathological vasoconstriction of the coronary arteries which reduce myocardial ischemia. 126 Improvement of EF was shown by treatment with perindopril in the substudy of the EURopean trial On reduction of cardiac events with Perindopril in stable coronary Artery disease (EUROPA) trial. 127 Calcium channel blockers, β-blockers, and thiazide diuretics are less effective in improving ED than ACE inhibitors. 128 In the Irbesartan and Lipoic Acid in Endothelial Dysfunction study, the ARB (irbesartan) demonstrated an improvement of EF and reduction in inflammatory markers. 129 Further, a meta-analysis showed that ACE inhibitors improve EF much more than calcium channel blockers and β-blockers. 130 Third-generation β-blockers, in particular nebivolol, are highly selective blockers of β-1 adrenergic receptors, and nebivolol is the only β-blocker known to induce vascular production of NO. Nebivolol induces NO production via activation of β-3 adrenergic receptors mediated production of NO in the heart. Consequently, nebivolol may reverse ED. 131
Renin inhibitors, which neutralize compensatory increased plasma renin activity and reduce angiotensin levels, also significantly improve EF. Aliskiren, a specific inhibitor of human renin, which is used for treatment of hypertension increased plasma NO bioavailability, improved EF, and suppressed atherosclerotic plaque formation. 132 Treatment of diabetes mellitus type 2 with new antidiabetic drugs does not only exert glycemic-lowering properties but also decreases CV risk; sodium glucose cotransporter-2 inhibitors significantly improve EF and reduce the CV risk and all-cause mortality. 133 Improvement in EF measured by arterial stiffness most probably represents one of the mechanisms for which these drugs exert their beneficial effects. 134
Lipid-lowering therapy
Numerous studies confirmed the beneficial effects of statins on EF. 135 Statin-induced improvement in EF is independent of lipid-lowering effects, but their protective effects on EF are most probably based on the anti-inflammatory and antioxidant properties. 136 Meta-analysis and systemic review of randomized controlled trials showed that statin therapy is associated with significant improvement in both peripheral and coronary EF. 137 It is unclear whether the improvement in EF independently contributes to the vascular risk reduction during lipid-lowering treatment and whether the assessment of EF would help identify patients who require more aggressive lipid-lowering treatment. 138 Statins were shown to improve EF, oxidative stress and inflammation in patients with arterial hypertension and normal cholesterol levels. 139 Therefore, patients with arterial hypertension benefit from statin administration, independently of their plasma lipid levels and independently of the influence on blood pressure. 140
Other drugs improving EF
Estrogens are able to improve EF through antioxidant properties that increase NO expression and degradation of ROS. 141 Growth hormone deficiency is also related to ED and early atherosclerosis. It was shown that growth hormone replacement in growth hormone deficient patients improved EF and could be a strategy for decreasing CV mortality in this high-risk population. 142 All these data show that ED is reversible and by lifestyle modification and treatment of risk factors it is possible to improve EF and prevent CV complications.
Conclusions
Functional integrity of the endothelium is a fundamental factor for vascular health. Endothelial dysfunction is an initiating and stimulating factor for the progression of atherosclerotic CV disease. It represents an early integrated index of the harmful effects of pro-atherogenic risk factors on the vessel wall. By measuring several biochemical markers and endothelium-dependent function, it is possible to estimate EF and monitor its deterioration. As ED is directly involved in atherogenesis and atherothrombotic complications it is an independent predictor of CV events in addition to traditional risk factors. Because of its central role in atherogenesis, the endothelium should be a therapeutic target for the prevention and treatment of atherosclerotic disease.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.