
Abstract
The left internal mammary (thoracic) artery (LIMA), when used as a pedicle graft at the time of coronary artery bypass grafting, is effective and durable. Data concerning the rate and causes of LIMA failure are scant. The aim of this paper is to explore the modes and frequency of sub-optimal LIMA grafts. We examined all cases of invasive graft angiography performed in our cardiothoracic center 2016–2020 and analyzed the quality of the LIMA graft. Of 551 cases, 323 had undergone isolated coronary artery bypass grafting including a LIMA since 2001; of those, 59 (18%) appeared sub-optimal; 16 (5%) being totally occluded, 26 (8%) exhibiting a “string sign” (i.e., atretic or cord-like), 12 (4%) being focally stenosed, and 5 (1.5%) being patent but placed on a diseased portion of the left anterior descending artery or other vessel. The commonest cause of failure were poor-quality left anterior descending artery target and non-flow-limiting disease. This paper highlights the low rate, and likely modes, of failure of this valuable treatment in contemporary practice.
Keywords
Background
The first use of the left internal mammary artery (LIMA) to provide additional blood supply for patients with coronary insufficiency was by Vineberg who, in 1946, tunneled it into the myocardium. 1 The first coronary artery bypass grafting (CABG) was by Goetz, using a right internal mammary artert (RIMA) to the right coronary artery (RCA), in 1960, followed by Sabiston using an saphenous vein graft (SVG) to the RCA in 1962, Kolessov with a RIMA to the RCA in 1967, Favoloro with an SVG to the RCA in 1967, and Green with a LIMA to the left anterior descending artery (LAD) in 1968.2,3 Uptake was, however, slow until cardiopulmonary bypass became commonplace. From the earliest experience, the LIMA graft was observed to have a long-term patency of >90%4 –10 and, in combination with other grafts, long-term patient survival was 80%–90%.9,11 –17 The graft seems impervious to adverse patient factors,7,18 exhibiting resistance to atherosclerosis when compared with vein grafts. 19 Despite the lack of randomized trials of LIMA versus SVG, the data from retrospective studies are sufficiently persuasive to endorse a LIMA-LAD graft in current European Society of Cardiology (ESC) and European Association for Cardio-Thoracic surgery (EACTS) guidelines.20,21 An example of an excellent LIMA graft is shown in Figure 1.
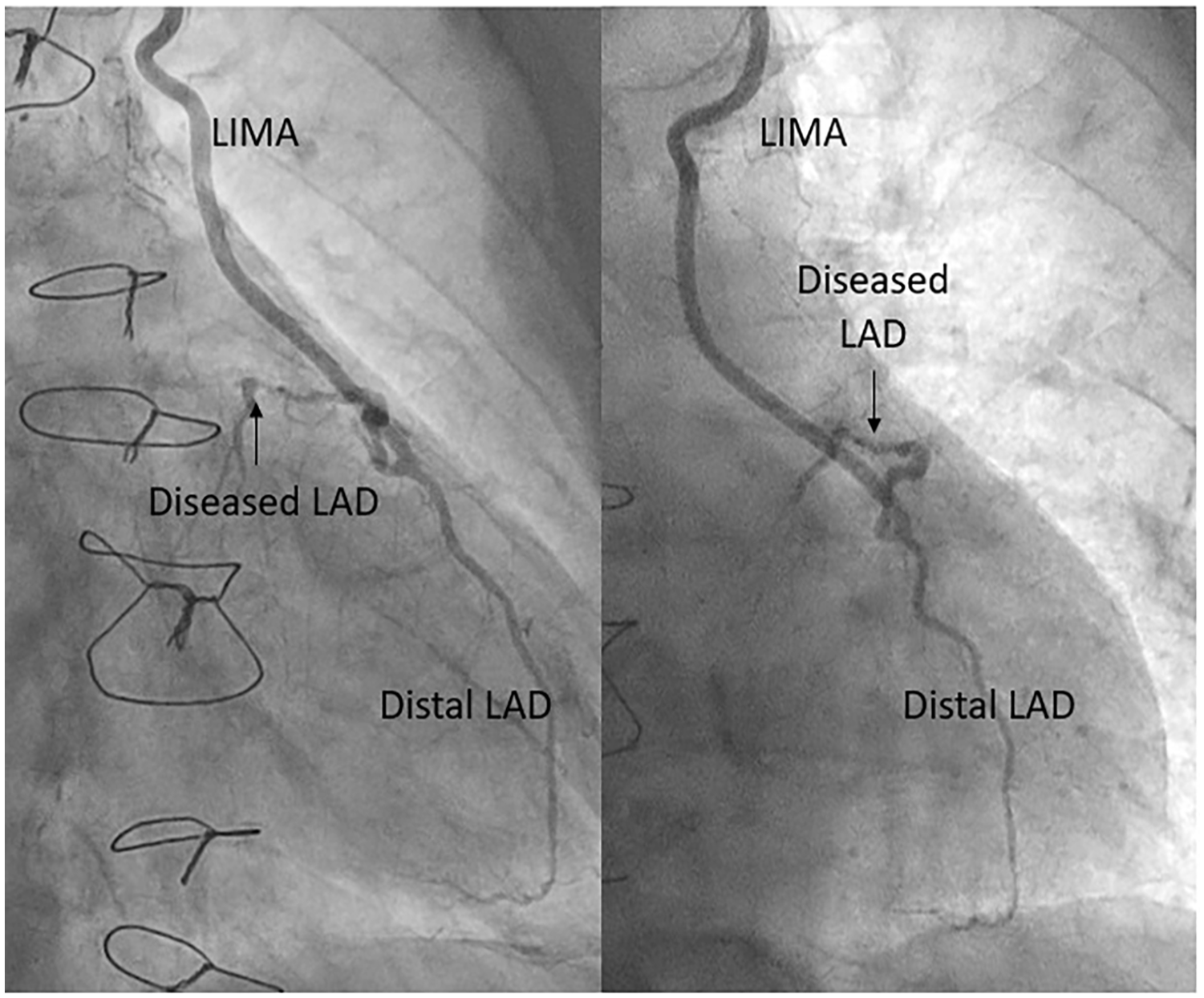
Example of an excellent LIMA graft with good distal LAD run-off.
There are, however, disadvantages of this graft. First, as with any surgical approach, is its invasive nature, which poses challenges for operating on patients with frailty and co-morbidity, stimulating efforts to perform “off pump” and minimal access surgery. Second, is the need to combine it with less durable vein grafts in multi-vessel disease. Third, is the potential for chest wall ischemia and wound dehiscence, especially when both mammary arteries are used. Fourth, is its proximity to the anterior chest wall, making it vulnerable to damage at the time of dissection and mobilization, which is particularly important at re-sternotomy. 22 Fifth, is its small but important failure rate, which is the subject of this paper. One documented cause of graft failure is competitive flow from native coronary arteries. When applied to vessels with a (CT-assessed) stenosis <70%, long-term LIMA patency was found to be 83%, compared with those applied to vessels stenosed >70%, in which patency was 100%. 23 Other causes are less well documented.
The aim of this paper was to explore the modes and frequency of sub-optimal LIMA grafts, as revealed by clinically driven graft angiography, in a “real world” clinical population, in modern clinical practice.
Methods
This was a retrospective cohort study of all patients who underwent graft angiography between 2016 and 2020 at Sheffield Teaching Hospitals, which is a large tertiary cardiothoracic center serving five general hospitals and a population of 1.8 million people in the North of England. For those who had received a LIMA graft to the LAD, the graft angiograms and operation notes were reviewed. Graft angiograms were organized and performed according to the standard practice of the patients’ cardiologists and based upon individual clinical need. A successful LIMA was defined as having a thrombolysis in myocardial infarction (TIMI) flow grade of 3 to the LAD with <50% stenosis throughout. The remaining cases were categorized as being sub-optimal; comprising those which were totally occluded, exhibiting the “string sign” (atretic or cord-like), focally stenosed, or patent but placed on a diseased target vessel. The probable cause of graft failure was categorized as a poor quality or diseased LAD target, a non-flow-limiting proximal lesion, anastomosis-related, insertion at a lesion, an acute thrombotic occlusion, and other causes. The quality of the LIMA and LAD was taken from the operation notes where these were available. The rate of LIMA failure was estimated by determining the total number of isolated CABG operations performed in the period spanning the dates of the operations of the patients undergoing graft angiograms, allowing for deaths in the group (which were assumed not to be related to LIMA failure).24 –26 Only isolated CABG operations which included a LIMA graft were selected for analysis to reduce risk of confounding from physiological factors associated with co-existing cardiac conditions such as valvular disease or atrial fibrillation (AF). All patients had standard sternotomy and no minimally invasive procedures were performed. The majority of cases were performed on-pump and no patients had hybrid revascularization at their index surgery. Characteristics of the patients with patent vs suboptimal LIMA grafts were compared. Survival was determined from the UK Office of National Statistics.
Statistics
Simple descriptive statistics were used, with means and standard deviations, or medians and interquartile ranges, as appropriate. When comparing groups (patent vs suboptimal LIMA), continuous variables were compared using the Mann-Whitney U test and categorical variables were presented as total numbers (proportions) and compared using the Chi-squared test or Fisher’s exact test, as appropriate.
Ethical Statement
This was a retrospective study of anonymized data so no specific ethical permission was required by the NHS Health Research Authority and Medical Research Council.
Results
In the period 2016–2020, 620 graft angiograms were performed at Sheffield Teaching Hospitals. Of these, 551 were identified after duplicates and cases with incomplete data were removed, including those whose operation had occurred prior to 2001. Of the remaining 385 patients, we excluded 38 patients who had their CABG with another procedure, such as AF ablation or valve surgery, and 24 who did not have a LIMA graft. None of these patients had had a re-do operation. Three hundred and twenty-three patients remained who had undergone an isolated CABG with a LIMA graft after 2001 (Figure 2). The time interval between operation and graft angiograms was median 9 (IQR 3–13) years. In the period 2001–2021, 10,766 CABG operations were performed at Sheffield, of which 9450 (90%) included a LIMA graft. Of these patients, 80% were male. Reasons for not achieving a 100% LIMA grafting rate include emergency operations, unsuitable LIMA quality and patients who did not require LAD grafting. From 2001, the all-cause mortality rate was 12% at 5 years (9135 operations), 25% at 10 years (7502 operations), and 39% at 15 years (4647 operations).
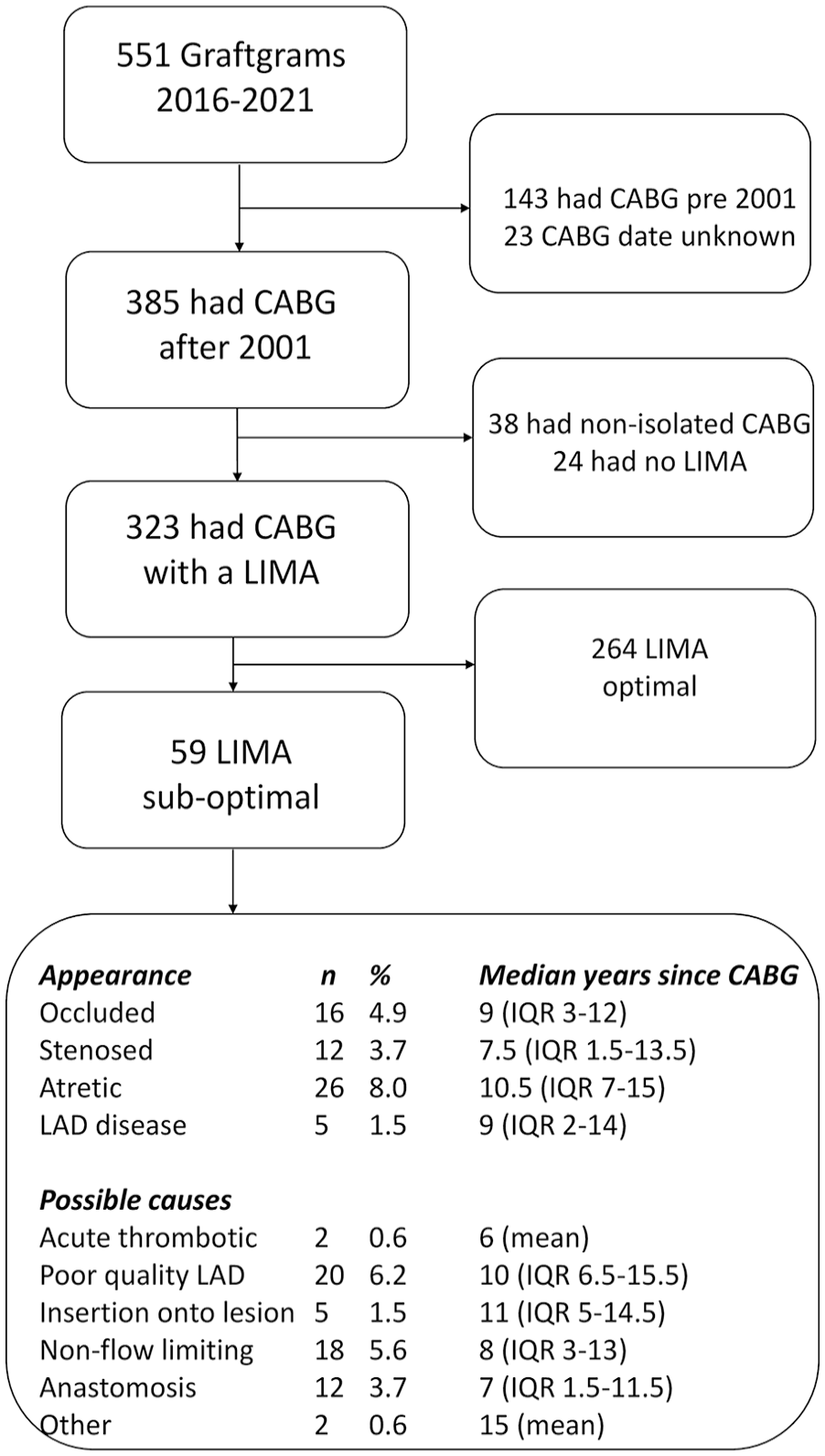
Consort diagram with exclusions and main findings.
Of the 323 graft angiograms of patients who originally had an isolated CABG operation including a LIMA, 84% were male and the median age was 71 (IQR 63–77); 59 (18%) LIMA grafts were found to be sub-optimal. Of the 279 patients for whom full clinical details were available, 25% were diabetic, 62% hypertensive, 9% peripherally arteriopathic, 10% had chronic obstructive pulmonary disease (COPD), 67% had a smoking history, none had renal failure requiring dialysis, and 28% were in-patients (emergency or acute). The breakdown of co-morbidities for patients with good vs sub-optimal LIMA with operation notes is shown in Table 1. Females made up 16% of the total cohort, and accounted for 29% of sub-optimal LIMA cases (P = .003).
Characteristics of Patient Cohort.
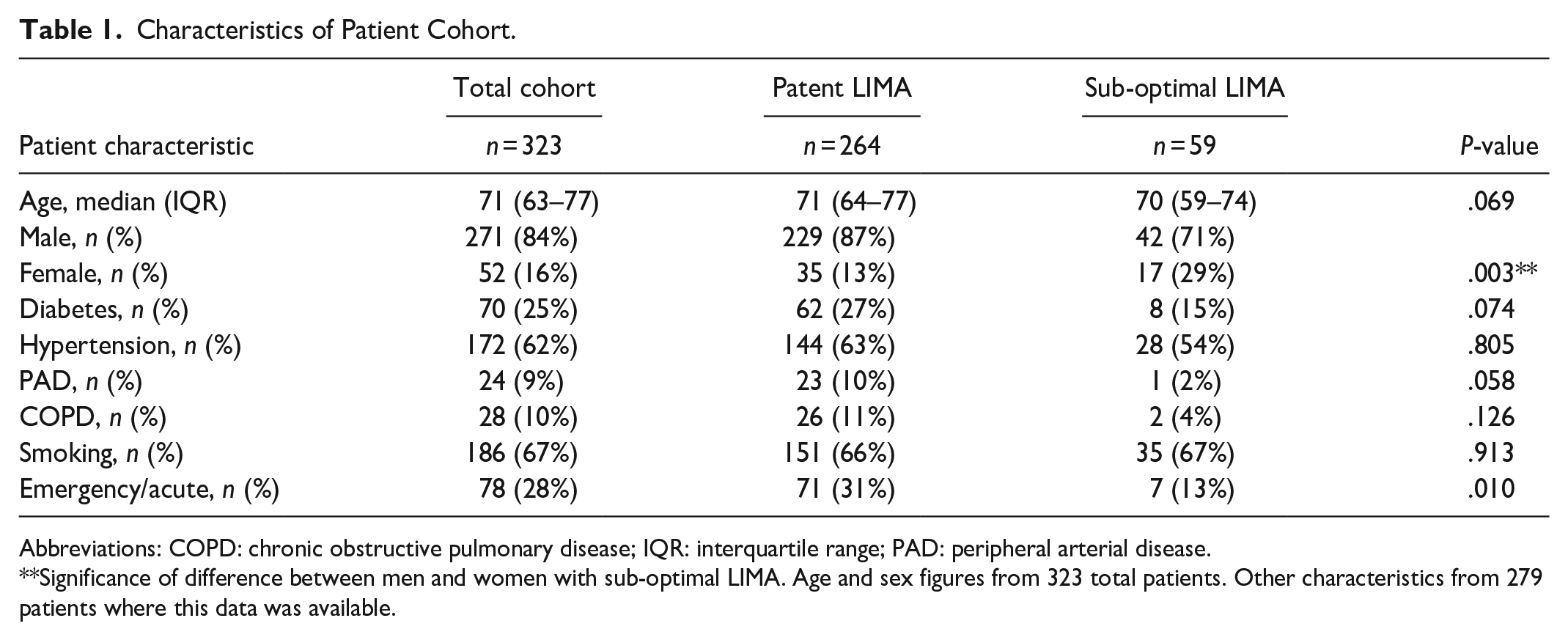
Abbreviations: COPD: chronic obstructive pulmonary disease; IQR: interquartile range; PAD: peripheral arterial disease.
Significance of difference between men and women with sub-optimal LIMA. Age and sex figures from 323 total patients. Other characteristics from 279 patients where this data was available.
Of the 59 sub-optimal LIMA grafts, 16 (5%) were totally occluded, 26 (8%) exhibited the “string sign,” 12 (4%) were focally stenosed, and 5 (1.5%) were patent but placed on a diffusely diseased LAD or vessel other than the LAD. The cause of graft failure was poor-quality LAD target in 20 (6%), non-flow-limiting lesion (resulting in competitive flow) in 18 (5.5%), anastomosis-related in 12 (4%), insertion near or at a lesion in 5 (1.5%), acute thrombotic occlusion in 2 (<1%), and other causes in 2 (<1%). Both cases of thrombotic occlusion presented as acute myocardial infarction. See Figures 3 and 4. The overall sub-optimal LIMA rate, observed as a proportion of all operations performed (n = 9450) was estimated at 0.6%, although this figure is an underestimate owing to the selection bias of the patients included in this study.
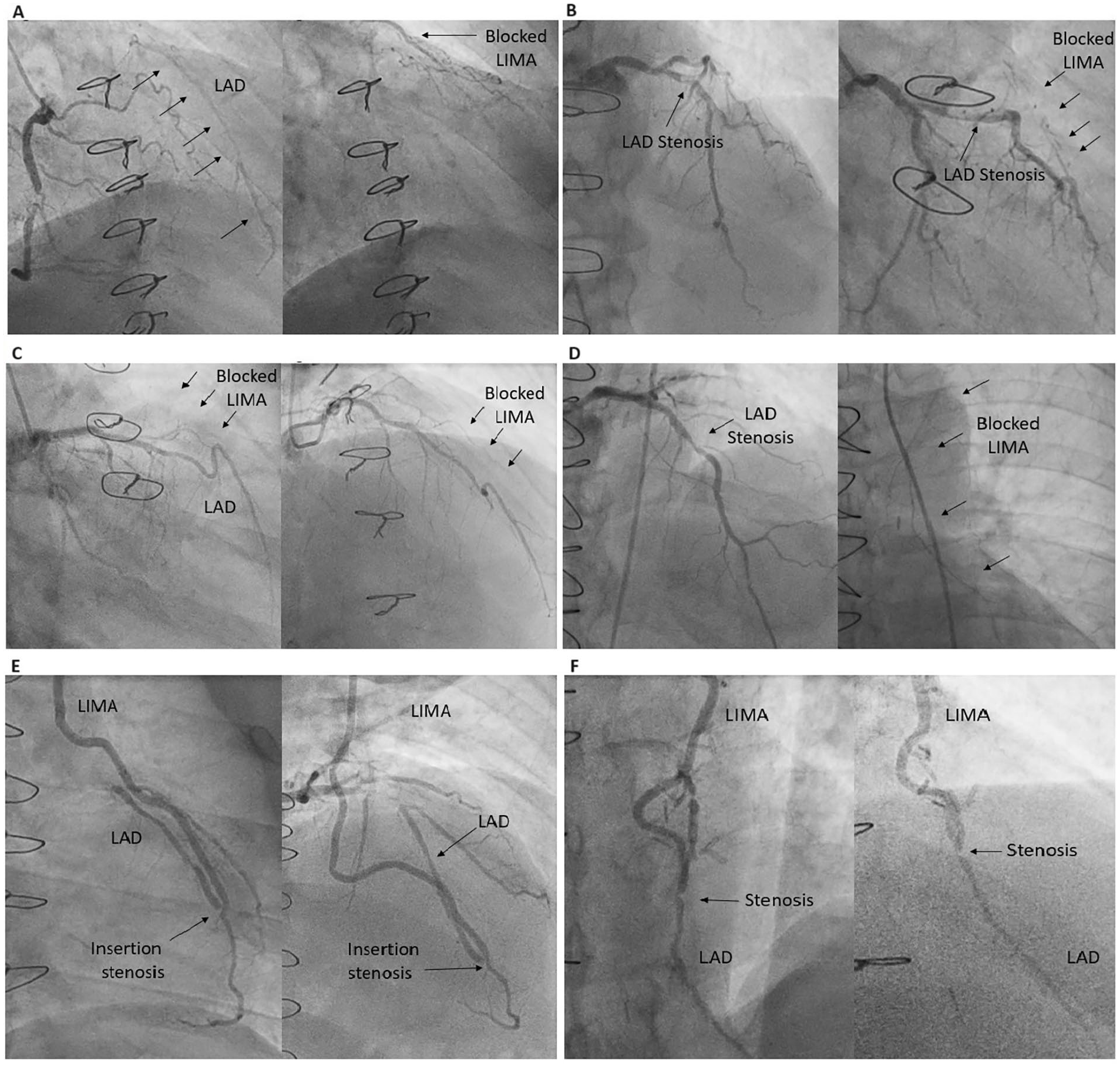
Examples of sub-optimal LIMA grafts at the time of graft angiography. (A) The LAD is heavily diseased throughout its length which probably explains the occluded LIMA. (B) The LIMA is distally applied to the LAD, where run-off is limited. (C) There is no lesion visible in the left main or LAD, so competitive flow probably explains the occluded LIMA. (D) There is brisk flow through the stenosis in the LAD, so competitive flow probably explains the occluded LIMA. (E) There is a tight stenosis in the LAD just proximal to the anastomosis. (F) There is a stenosis in the LAD just distal to the anastomosis.
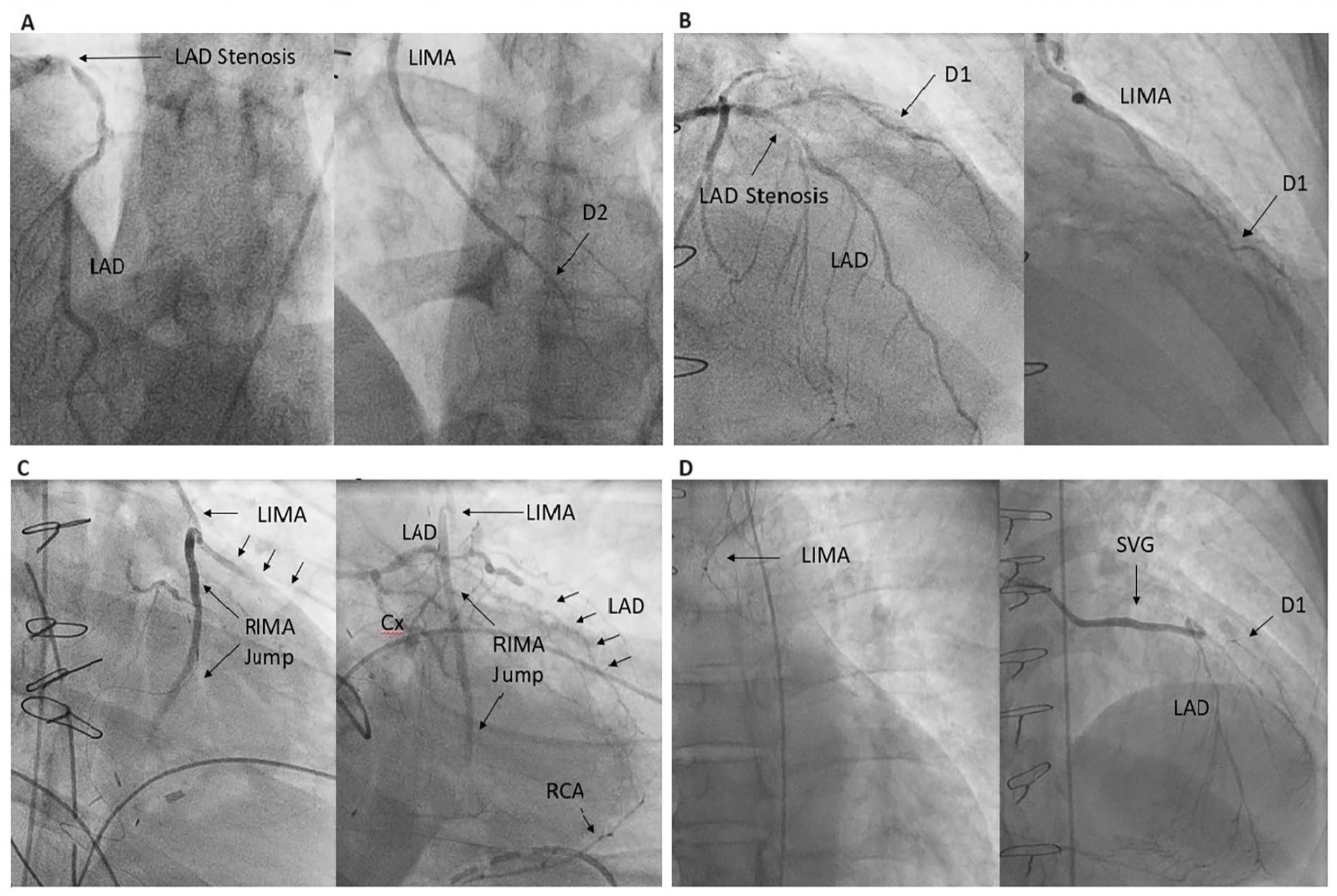
Further examples of sub-optimal LIMA grafts at the time of graft angiography. (A) The LIMA is grafted onto a small second diagonal branch. (B) The LIMA is grafted onto a first diagonal branch, which arises proximal to the LAD stenosis. (C) The LIMA is anastomosed to the LAD, and a free RIMA fashioned as a T-graft from LIMA to the first obtuse marginal and then to the second obtuse marginal artery. Combined failure of run-off led to myocardial infarction. (D) There is an SVG on a diagonal artery which is backfilling the LAD, leading to competitive flow from the SVG which, combined with poor run-off in the diseased LAD, led to occlusion of the LIMA.
Discussion
In this “real world” and single center retrospective study, we estimated the rate of sub-optimal LIMA graft in patients attending for coronary and graft angiography at median 9 (IQR 3–13) years to be 18% of all graftgrams, and approximately 0.6% of all operations, allowing for all-cause mortality, which cannot be assumed to be unrelated LIMA failure. This figure is therefore likely to be grossly under-estimated due to asymptomatic LIMA graft failure, out of hospital cardiac death or graft angiography performed at a different center. It is also important to note that only patients who attended for invasive angiography are included in this analysis and did not routinely perform CT angiography for graft patients during the period spanned by this study. CT coronary angiography has good diagnostic accuracy for graft disease and patients are often referred for non-invasive imaging to avoid the risks of invasive angiography and technically challenging graft angiography. 27 As such, the non-inclusion of such patients may add to the underestimation of total graft failure. There is seemingly a preponderance for women in the sub-optimal LIMA group, however this is likely to be inaccurate due to the low numbers studied. The commonest causes of a sub-optimal LIMA were non-flow-limiting lesion in 5.5%, poor-quality LAD in 6%, anastomosis-related in 4%, and insertion onto a vessel other than the LAD in 1.5%. The five- and ten-year all-cause mortality rate following CABG was 12% and 25%, respectively. There are lessons for cardiologists and surgeons involved in the care of patients being considered for CABG with a LIMA graft.
First, the failure rate of the LIMA was confirmed, in accordance with extensive clinical experience and literature, to be extremely low, so it is advantageous to use the LIMA, if possible, as the graft to the LAD.
Second, although it is clearly impossible to know the rate of sub-optimal LIMA in all patients without flow-limiting LAD disease, due to the low overall re-presentation and graftgram rate, we have shown that non-flow limiting disease in the LAD is commonly associated with a sub-optimal LIMA at follow-up angiography. Grafting such a vessel should be avoided. Pressure wire-based indices of ischemia in the appropriate territory may assist decision-making, and are currently under-used at the time of diagnostic angiography. Many referrals for CABG are made by non-interventional cardiologists, or those based at centers without the capacity to perform invasive physiological coronary assessment, which may contribute. In those circumstances, computed tomography (CT) derived fractional flow reserve (FFR) or angiography-derived (virtual) FFR 28 may be useful. The use of a “pull-back” during FFR measurement can provide data on the tightest point of the LAD lesion and help to guide placement of the LIMA on the correct location of the LAD. Computed FFR, based upon angiographic or CT images, can offer the same advantage. However, even a borderline FFR-positive lesion may allow sufficient competitive flow at rest to provoke graft failure, although a large caliber, slow-flow, vein graft is more vulnerable than a LIMA.
Third, we have shown that diffuse disease of the LAD is also associated with a sub-optimal LIMA. Whilst extremely badly diseased LAD vessels are clearly unsuitable for grafting, moderately diseased vessels merit careful scrutiny to avoid fashioning an anastomosis in a segment of significant stenosis or a long lesion. If there is doubt about the adequacy of graft performance in such a case, intra-operative graft Doppler flow measurements may be considered. 29 None of the cases performed at our center had intra-operative endarterectomy, angiography or Doppler flow measurements.
Fourth, in a few cases, the LIMA was found to be anastomosed to an anterior wall vessel other than the LAD. This may be a deliberate decision at the time of surgery, if the LAD is found to be smaller than the diagonal branch, badly diseased, intra-myocardial or not found at all. Very occasionally, a diagonal may be mistaken for the LAD.
Finally, care must be taken to minimize damage to the LIMA intra-operatively and the use of the “no touch” technique may be employed. This is achieved by never handling the LIMA directly during harvest; instead using surrounding tissues of fat and muscle. Low power diathermy may be utilized to coagulate and cut pedicle tissues, avoiding direct contact with the artery. Meticulous anastomotic technique is important to avoid creating an iatrogenic stenosis.
There are several limitations of this study. First, it was retrospective, involving an era in which clinical records were recorded on several different media, and the quality of available information was variable. We therefore focused on procedures from 2001 onwards. Despite these precautions, it is possible that the rates of failure quoted, particularly of LIMA failure as a proportion of all operations performed, are inaccurate. Second, the state of the LIMA and the anastomosis at the time of graft angiography may not have reflected its original state at the time of operation, for which surgical notes may have been incomplete, or for which the pre-operative angiogram was not available. Third, graft angiograms were only performed on patients presenting with significant symptoms, and we had to assume that patients not undergoing graft angiography had a long-term successful LIMA graft. We also made the assumption that the LIMA was patent in individuals who had died since their operation, which is over-optimistic. Fourth, some graft angiograms were indistinct; and, in cases in which the LIMA was blocked, it was sometimes not possible to be sure of the cause of failure.
Conclusions
The LIMA graft is an effective and durable treatment for patients with a diseased LAD. Failure is rare. Our estimate is that, at a median 9 years, a sub-optimal LIMA is found in about 18% of patients attending for graft angiography. The common causes appear to be a poor-quality LAD, a non-flow-limiting lesion causing competitive flow, and technical problems with the anastomosis. These findings may be useful in assessing patients’ suitability for CABG incorporating a LIMA graft to the LAD.
Footnotes
Abbreviations
AF Atrial Fibrillation
CABG Coronary artery bypass graft
CHD Coronary heart disease
COPD Chronic obstructive pulmonary disease
EACTS European Association of Cardiothoracic Surgeons
ESC European Society of Cardiology
FFR Fractional flow reserve
LIMA Left internal mammary (thoracic) artery
LAD Left anterior descending (coronary artery)
RCA Right coronary artery
STH Sheffield Teaching Hospitals
SVG Saphenous vein graft
TIMI Thrombolysis in Myocardial Infarction
Author Contributions
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Data Availability Statement
The data for this study are stored on the Sheffield Teaching Hospitals secure network. It may be made available in anonymized format upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PDM was funded by the Wellcome Trust [214567/Z/18/Z]. For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission.
This study/research is partly funded by the National Institute for Health and Care Research (NIHR) Sheffield Biomedical Research Centre (NIHR203321*). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.