
Abstract
Objective:
To describe rates of short-term morbidity following transcervical surgical treatment of hypopharyngeal diverticulum (HD) and analyze predictors of adverse events.
Methods:
The 2005 to 2017 National Surgical Quality Improvement Program database was queried to identify patients diagnosed with HD undergoing open transcervical diverticulectomy.
Results:
A total of 597 patients with a mean age of 71.4 ± 12.3 years were included. Thirty-day adverse events were experienced by 63 (10.6%) subjects, including 6.5% unplanned reoperations, 4.2% surgical complications, 4.4% medical complications, 2.7% readmissions, and 0.7% deaths. Medical complications notably included pneumonia (2.0%), reintubation (1.2%), sepsis (1.2%), intubation >48 hours (0.5%), urinary tract infection (0.5%), or deep vein thrombosis (0.5%), while surgical complications included organ/space infection (2.0%) and superficial (1.3%) or deep (1.0%) surgical site infection. Gender, race, functional status, diabetes, dyspnea, hypertension, steroid use, and recent weight loss were not associated with adverse events. Length of operation and hospitalization were both higher among those with adverse events (127.4 ± 107.9 vs 95.7 ± 59.8 minutes, P = 0.027, and 7.4 ± 7.4 vs 2.8 ± 3.6 days, P < 0.001). On multivariable logistic regression, high American Society of Anesthesiologists (ASA) class (OR = 2.02, P = 0.017), smoking (OR = 2.10, P = 0.044), and operation time (OR = 1.01; P = 0.005) were independent predictors of adverse events. Obesity was not associated with length of stay, readmission/reoperation, or complications. However, increased age was associated with shorter operations (P = 0.020), higher length of hospitalization (P < 0.001), and higher mortality (P = 0.027) and readmission rates (P = 0.023).
Conclusion:
Understanding clinical factors associated with complications following open surgery for HD such as ASA score, smoking status, length of operation, and age can help optimize surgical outcomes for at-risk patients.
Keywords
Introduction
Hypopharyngeal diverticulum (HD), first described by Ludlow and later by Zenker and von Ziemssen, is a posterior outpouching of mucosa and submucosa through a weakened Killian triangle with an estimated incidence of 2 per 100 000.1-3 HD occurs predominately among men and during the seventh and eighth decade of life.4,5 The most common presenting symptoms include dysphagia, regurgitation, aspiration, halitosis, malnutrition, weight loss, cough, and hoarseness. 6 Surgery is the mainstay of treatment, which can be performed via open transcervical or endoscopic transoral approaches. Even with the emergence of endoscopic surgery in the past four decades, open surgery has remained relevant for treating HD with reported success rates upwards of 80%.6,7 A recent meta-analysis of 865 HD patients comparing transcervical and endoscopic diverticulectomies demonstrated that both approaches succeeded in improving symptoms of dysphagia and regurgitation without significant differences between the corresponding outcomes. 8
In a comprehensive analysis by Leibowitz and colleagues, the authors concluded that there is no single “best” surgery for treating HD and both techniques can be similar in effectiveness and outcomes. 9 Regardless, multiple studies have reported a possibly higher rate of morbidity with longer operation time and hospital stay in transcervical open surgery.10-12 These adverse events most commonly consist of leak or perforation, nerve injury, infection, and hematoma. 13 Although there is a trending increase for endoscopic approach, transcervical open surgery is still largely prevalent, warranting continuous examination of its complication profile. Additionally, valuable insights can be elucidated from analyzing the association between various clinical/demographic factors and complications.14-16 As such, this study utilized a large national database to evaluate short-term complications as well as readmission and reoperation rates following transcervical diverticulectomies of HD, and to evaluate the demographic or clinical variables that may predict these outcomes.
Methods
This study was exempted from the institutional review board because of the database’s lack of identifying patient information. Subjects were extracted from the 2005 to 2017 National Surgical Quality Improvement Program (NSQIP) database, which is sponsored by American College of Surgeons and reports risk-adjusted 30-day morbidity and mortality of various surgical operations from more than 600 nationwide hospitals. 17 Subjects were identified using International classification of disease (ICD) codes 530.6 (ICD-9) and K22.5 (ICD-10) for a diagnosis of HD, and current procedural terminology (CPT) code 43130 to select patients who underwent cervical approached diverticulectomies, with or without myotomies. These ICD codes are most commonly used for Zenker’s diverticulum (ZD), but since they could also theoretically include Killian-Jamieson, traction, or iatrogenic diverticulum, this manuscript refers to these subjects as HD. Patient demographics, preoperative and perioperative clinical metrics, and post-surgical outcomes were extracted.
American Society of Anesthesiologists (ASA) classification, which is a metric designed to predict operative risk, 18 was binarized as low (ASA 1-2) or high (ASA 3-4) for analyses. Discharge to facility was defined as discharge to non-home care facilities including hospice, rehabilitation facilities, skilled nursing homes, or transitional care units. Surgical complication was defined to include superficial surgical site infection (SSI), deep SSI, organ/space SSI, wound disruption, and blood transfusion within 72 hours post-operation. Medical complication was defined to include pneumonia, unplanned reintubation, urinary tract infection, deep vein thrombosis, renal insufficiency, pulmonary embolism, intubated for >48 hours, acute renal failure, cerebrovascular accident with neurological deficit, cardiac arrest requiring cardiopulmonary resuscitation, myocardial infarction, sepsis, or septic shock. Readmission and reoperation were recorded if they occurred within 30 days of the primary operation. Adverse event was defined to include any surgical or medical complication, readmission, reoperation, or mortality. Readmission data was not reported for every patient (variable was introduced in 2008) thus their respective percentages are based on the available number of data instead of the entire cohort. Patients were categorized into obese and non-obese groups according to a body mass index (BMI) threshold of 30. For age, patients were divided into tertiles according to 50th and 75th percentile age values.
Statistical analysis was performed with PASW Statistics 18.0 software (SPSS Inc., Chicago, IL) with a P < 0.05 threshold for significance. Continuous and categorical variables were analyzed via two-tailed unpaired t-test and chi-squared or Analysis of Variance, respectively. Bivariate logistical regression was performed on preoperative and intra-operative variables that were individually significant on univariate analysis, for which odds ratio (OR) and 95% confidence interval (CI) were calculated and reported.
Results
A total of 597 patients with a mean age of 71.4 ± 12.3 years (median = 71.0 years), and consisting of 247 (41.4%) females, were included. A total of 63 (10.6%) subjects experienced at least one adverse event within 30 days of operation, including 39 (6.5%) unplanned reoperations, 25 (4.2%) surgical complications, 26 (4.4%) medical complications, and 4 (0.7%) deaths. Also, non-surgical hospital readmission, which was available for 370 patients, was observed in 10 (2.7%) subjects. Medical complications included pneumonia (n = 12, 2.0%), reintubation (n = 7, 1.2%), sepsis (n = 7, 1.2%), intubation >48 hours (n = 3, 0.5%), urinary tract infection (n = 3, 0.5%), deep vein thrombosis (n = 3, 0.5%), pulmonary embolism (n = 2, 0.3%), and septic shock (n = 1, 0.2%). Surgical complications included organ or space infection (n = 12, 2.0%), superficial SSI (n = 8, 1.3%), deep SSI (n = 6, 1.0%), and wound dehiscence (n = 1, 0.2%). Demographic and clinical variables were compared between patients who experienced an adverse event versus those who did not, and the results are demonstrated in Table 1. Of note, active smoking (P = 0.008), high ASA class (P = 0.010), and increased operation time (P = 0.027) were associated with 30-day adverse events. Moreover, discharge to facility (P < 0.001) and length of stay (LOS) (P < 0.001) were postoperative features that positively associated with 30-day adverse events.
Association of Demographic/Clinical Covariates with 30-Day Adverse Events.
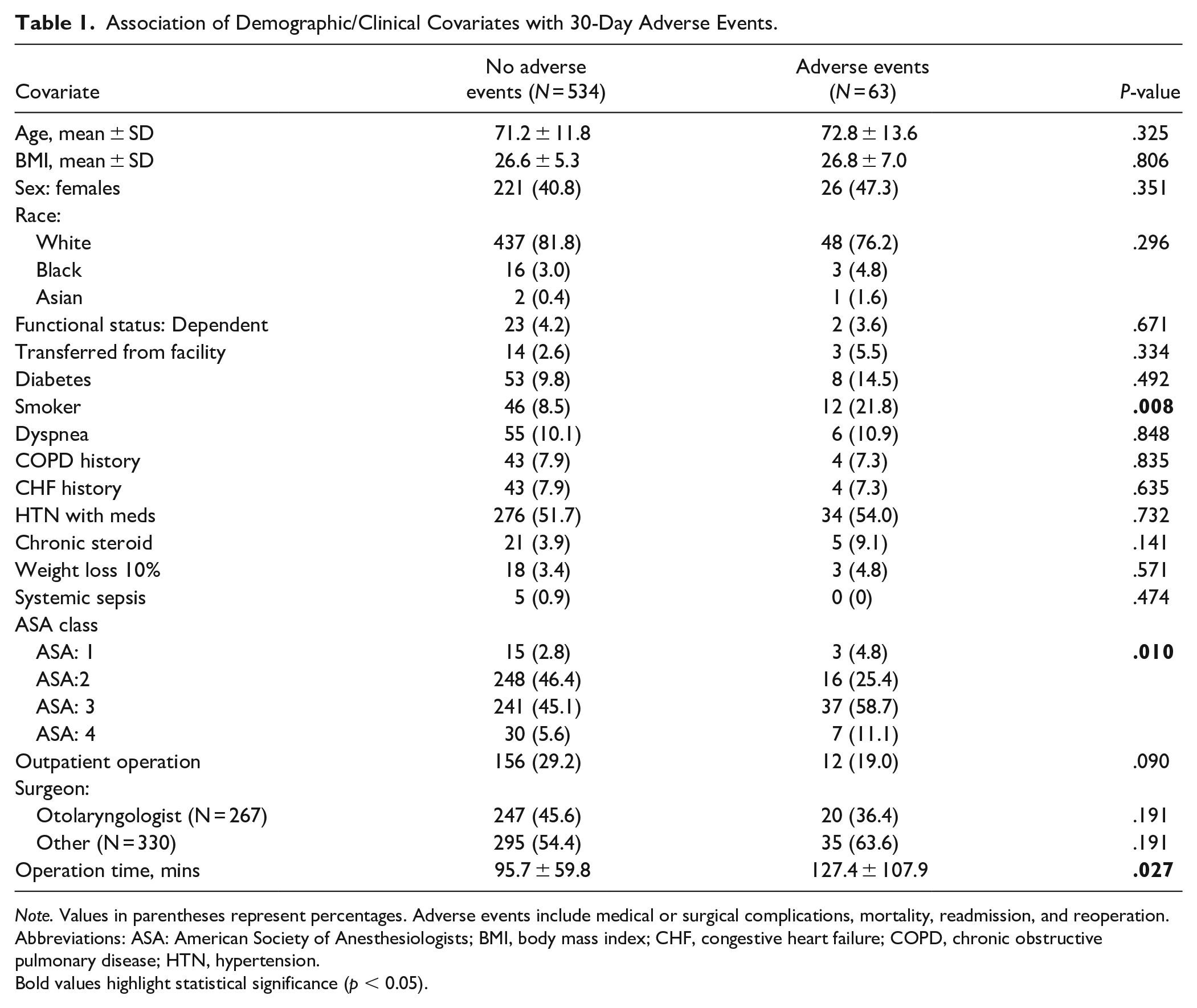
Note. Values in parentheses represent percentages. Adverse events include medical or surgical complications, mortality, readmission, and reoperation.
Abbreviations: ASA: American Society of Anesthesiologists; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HTN, hypertension.
Bold values highlight statistical significance (p < 0.05).
Univariate logistic regression analysis of pre- and perioperative factors in association with adverse events are demonstrated in Table 2, where variables significant on univariate analysis were carried forward for a combined multivariate logistical regression. This demonstrated that patients with high ASA score were 2.0 times (OR = 2.018; 95% CI: 1.136-3.585, P = 0.017) and active smokers were 2.1 times (OR = 2.098; 95% CI: 1.019-4.320, P = 0.044) more likely to have 30-day adverse events. Moreover, higher operation time (OR = 1.005; 95% CI: 1.001-1.008, P = 0.005) was also independently associated with adverse events. Surgical outcomes were further compared according to BMI and age. Table 3 demonstrates that surgical outcomes and adverse events were similar between obese and non-obese patients. However, categorizing patients according to 50th and 75th percentile values into age ≤72, 73-81, and ≥82 demonstrated significant differences in time of surgery (106.5 ± 63.6 vs 93.3 ± 71.7 vs 89.1 ± 67.0 minutes; P = 0.020), LOS (2.6 ± 2.8 vs 3.0 ± 4.3 vs 5.2 ± 6.6 days, P < 0.001), readmission (1.0% vs 3.1% vs 7.1%; P = 0.023), and mortality (0% vs 0.6% vs 2.3%; P = 0.027) rates (Table 4).
Univariate and Multivariate Logistic Regression Analysis of Clinically Relevant Covariates, demonstrating the independent predictors of 30-Day Adverse Event.
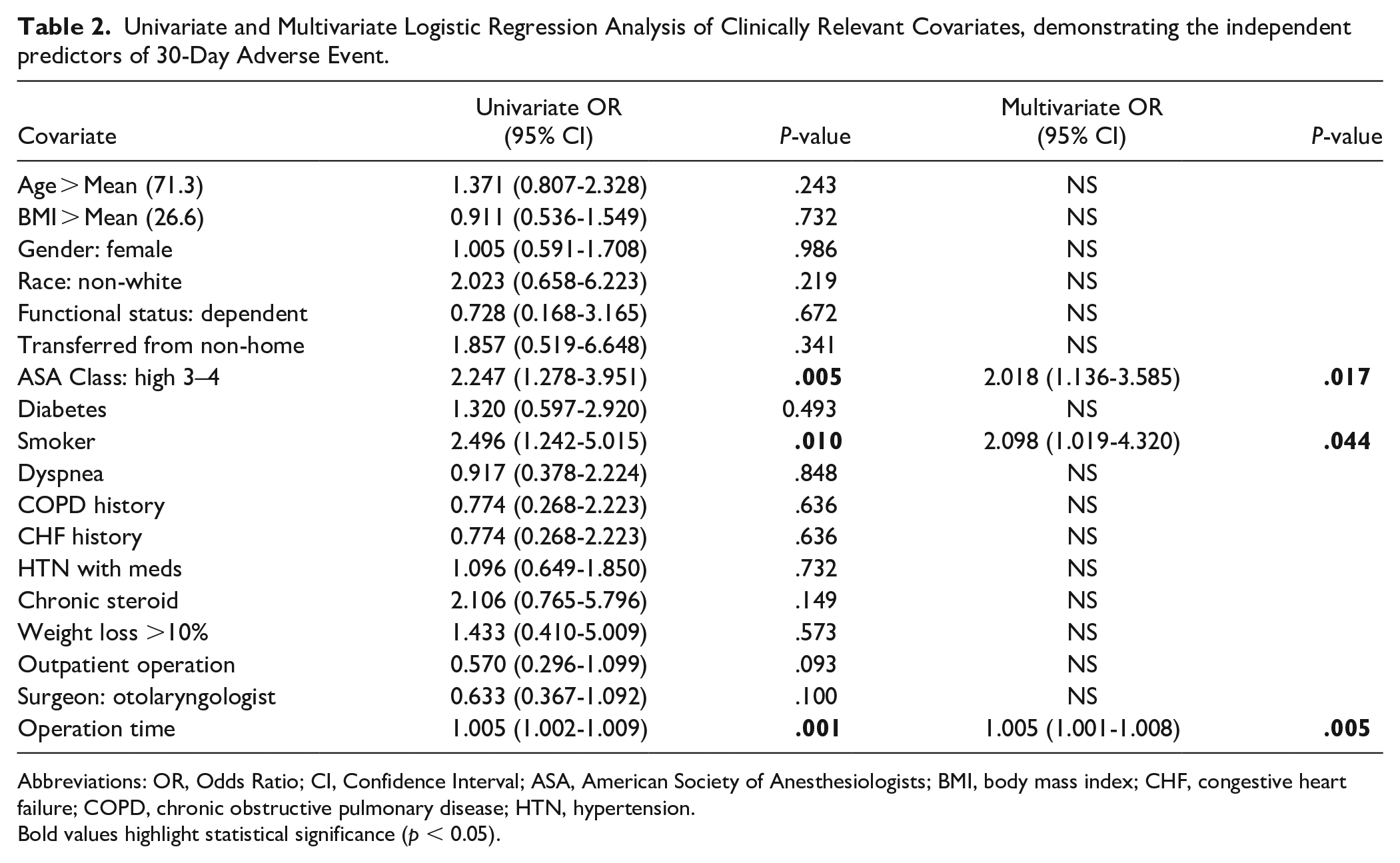
Abbreviations: OR, Odds Ratio; CI, Confidence Interval; ASA, American Society of Anesthesiologists; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HTN, hypertension.
Bold values highlight statistical significance (p < 0.05).
Surgical Outcomes and Complications Following HD Transcervical Surgery in Obese and Non-Obese Patients. All Values in Parenthesis are Percentages.
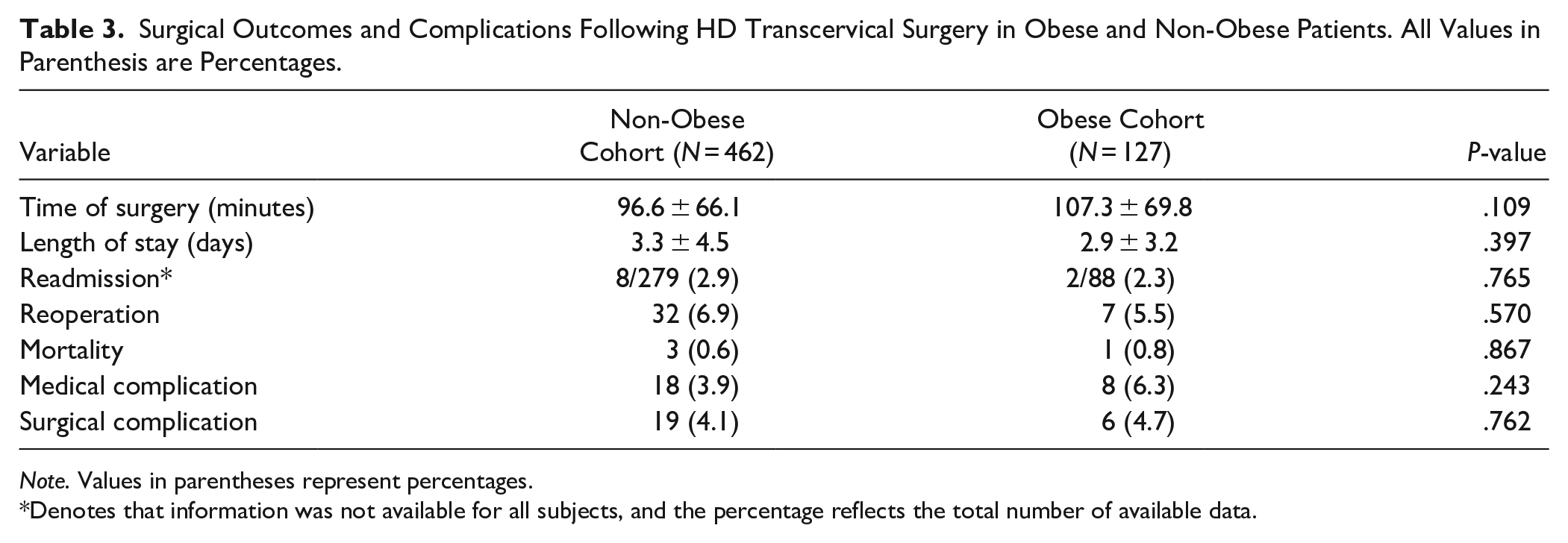
Note. Values in parentheses represent percentages.
Denotes that information was not available for all subjects, and the percentage reflects the total number of available data.
Surgical Outcomes and Complications Following HD Transcervical Surgery According to Patients’ age. All Values in Parenthesis are Percentages.
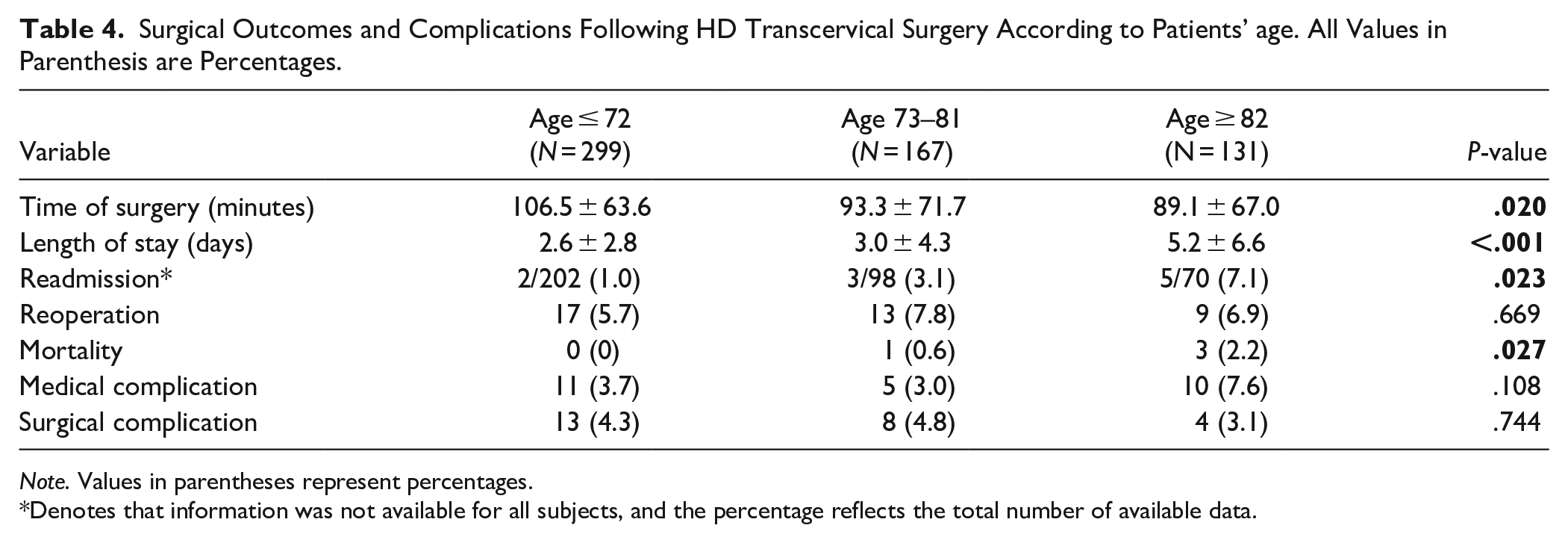
Note. Values in parentheses represent percentages.
Denotes that information was not available for all subjects, and the percentage reflects the total number of available data.
Discussion
In this manuscript, the NSQIP database was examined to assess 30-day adverse events following open transcervical surgical treatment for HD, along with demographic and clinical factors that may predict these morbidities. The presented results included a large cohort of 597 patients and demonstrated an overall 10.6% adverse event rate, most commonly consisting of reoperation, organ or SSI, and readmission. Independent predictors of adverse events included smoking, high ASA class, and longer operations. Lastly, although obesity did not influence operative outcomes, increased age was associated with shorter operation, longer LOS, and higher mortality and readmission rates.
With the significant evolvement of HD surgery over years, both open and endoscopic approaches remain viable options depending on the pouch size, patient’s symptoms and baseline characteristics, surgeon’s preference, and facility resources. 13 Though not compared in this study due to limitations of the database, endoscopic surgery can be associated with less morbidities, shorter operation times, and lower LOS and hospital costs.12,13,19-21 On the other hand, some authors have argued that open transcervical surgery can attain higher resolution of preoperative symptoms 22 and have lower rates of recurrence. 12 Furthermore, open surgery which allows for complete cricopharyngeal myotomy and direct access to the HD can associate with intra- and postoperative complications such as recurrent laryngeal nerve injury, leakage or perforation, cervical infection, hematoma, respiratory infection, stenosis, and mediastinitis. 13 A comprehensive review of 93 studies and 6915 HD patients reported morbidity and mortality rates of 10.5% and 0.6%, 13 which are closely resembled by our values of 10.6% and 0.7%. These percentages further approximate complication rates according to retrospective studies by Leibowitz et al 9 (n = 27) and Nitschke et al 12 (n = 41) and a review by Verdonck et al 23 (n = 1990). A meta-analysis by Howell and colleagues reported a 9.4% reoperation rate 8 which was slightly higher than this manuscript’s 6.5%, likely attributed to their long-term follow-ups as opposed to this database’s 30-day data collection.
Previous HD studies have suggested a lack of association between postoperative complication rates and age.9,12 In this manuscript, after categorizing patients according to 50th and 75th age percentiles, advanced age was associated with prolonged LOS as well as higher rates of mortality and readmission, but shorter operation time. Similar positive associations between age and certain surgical outcomes have been reported in the head and neck literature,24-26 while others have observed a lack of influence.27,28 Furthermore, we attribute that the longer operation time may suggest more aggressive surgical approaches in the younger patients. These warrant further investigation of age as a risk factor in HD surgery, and caution when managing the elderly. Interestingly, we observed that longer operation was positively associated with adverse events, but younger patients (which had longer operation times as a cohort) did not have higher 30-day adverse events compared to older patients. This can be due to a marginally significant effect that is lost once age is factored in. Another possibility is that the influence of operation length on short-term morbidity may be more pronounced in certain age populations. Future research to continue evaluating the influence of operation time on short- and long-term outcomes depending on patients’ age group are warranted.
Contrary to some reports within the head and neck literature reporting risk of adverse events with diabetes, hypertension, weight loss, or ventilator dependence,16,25,29,30 these did not influence morbidity in the presented analysis. As expected, we observed that discharge to a care facility and LOS were positively associated with short-term adverse events. BMI did not influence morbidity following transcervical surgery, resembling the findings of Crippen et al 29 and Lipschitz et al 31 in head and neck free flap and vestibular schwannoma surgeries, respectively. Similar to the literature concerning a wide variety of surgical fields,16,25,32,33 this study demonstrated that smoking, with an OR of 2.1 on multivariate analysis, was predictive of short-term adverse events. In other words, patients who were active smokers were two times more likely to experience acute morbidity following transcervical operation. This can be attributed to decrease in tissue blood flow, diminished collagen production, suppressed immune response, and delayed wound healing.34-36
This manuscript is the first to evaluate the influence of ASA score, which measures preoperative general health and risk for comorbidities, on HD surgery. Previously, Hackett et al’s investigation of more than 2 million subjects demonstrated the utility of ASA class as a reliable independent predictor for postoperative medical complications and mortality. 37 We observed that patients with a high ASA score were more likely to experience short-term adverse events, which is consistent with other reports in the head and neck literature concerning anterior skull base surgeries, 38 neck dissection, 39 and microvascular reconstruction. 40 In this HD cohort, patients with a high ASA score were 2.0 times more likely to experience short-term morbidity following transcervical operation. This demonstrates the utility of ASA score as an important clinical variable when planning HD operations. In addition to high ASA score, longer operation time was another independent predictor of short-term morbidity in the analyzed cohort. This was also in agreement with similar findings in the head and neck literature38,41,42 or in other surgical fields such as spine, 43 hernia, 44 and urolithiasis surgery. 45 As such, this large cohort’s averaged operation time for cases with complication (131.5 ± 112.7 minutes) versus no complication (95.8 ± 59.8 minutes) may serve as a valuable reference for clinicians treating HD.
Despite our effort to carefully analyze and interpret data within the NSQIP database, this study contains several limitations. First, some important clinical variables such as HD size and transcervical-specific complications such as recurrent laryngeal nerve damage or esophageal perforation/leak were not available, and thus were not included in the analyses unless they led to infection, readmission, or reoperation. Furthermore, although specific ICD and CPT codes were utilized to collect a homogenous surgical cohort, this falls short compared to definite clinical diagnoses in an institutional setting. For instance, this manuscript did not distinguish between the different types of diverticula which may influence types and rates of complications. Furthermore, the utilized CPT code was intended for transcervical surgery, however, due to a lack of a standardized endoscopic CPT until more recently, some surgeons may have used the transcervical CPT inappropriately for an endoscopic procedure. Also, in such national database studies with a variety of participating hospitals, homogeneity can further diminish due to differences in regional resources, surgical preferences, preoperative protocols, and post-surgical managements. Despite the aforementioned limitations, this study’s findings based on a large cohort of patients can provide valuable insights into various short-term morbidities associated with transcervical surgery of HD, as well as clinical or demographic factors that can associate with adverse events. Knowledge of these findings can help provide better care and surgical planning for patients undergoing transcervical surgery for HD, especially those with the aforementioned risk factors.
Conclusion
A better understanding of clinical factors associated with adverse events following transcervical diverticulectomy of HD can help optimize surgical outcomes for at-risk patients. Independent predictors of 30-day adverse events, which was observed in 10.6% of the subjects, included smoking, high ASA score, and longer operation. Even though BMI did not influence outcomes, age was negatively associated with operation time and positively association with LOS, mortality, and readmission rates. Future studies are warranted to continue investigating these important risk factors, which can potentially result in better surgical planning, decision-making, and outcomes in patients with HD.
Footnotes
Authors’ Note
Portions of this work was presented as an online poster presentation at the virtual 2020 Combined Otolaryngology Spring Meeting (COSM), May 15-June 14, 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.