
Abstract
Objective:
Identify risk factors and perioperative morbidity for pediatric patients undergoing septoplasty.
Methods:
The American College of Surgeons National Surgical Quality Improvement Program Pediatric (NSQIP-P) database was retrospectively queried to identify patients who underwent septoplasty (CPT 30520) for a diagnosis of deviated nasal septum (ICD J34.2) from 2018 to 2019. Outcomes analyzed include patient demographics, medical comorbidities, surgical setting, operative characteristics, length of stay, and postoperative outcomes.
Results:
A total of 729 children were identified. Median age at time of surgery was 15.8 years, with most patients (82.8%) >12 years of age; no significant association was identified between age at time of surgery and adverse surgical outcomes. Overall, postoperative complications were uncommon (0.6%), including readmission (0.4%), septic shock (0.1%), and surgical site infection (0.1%). A history of asthma was found to be a significant risk factor for postoperative complications (P = .035) as well as BMI (P = .028).
Conclusion:
The 30-day postoperative complications following pediatric septoplasty in children reported in the NSQIP-P database are infrequent. Special considerations regarding young age, complex sinonasal anatomy, and surgical technique remain important features in considering corrective surgery for the pediatric nose and certainly warrant further investigation in subsequent studies.
Introduction
Deviated nasal septum is a common cause for impaired breathing in pediatric patients, and although occasionally asymptomatic, it is present in as many as 30% of children. 1 Septoplasty is a surgical procedure performed to relieve nasal obstruction by correcting this deformity. While this procedure is common in adults, the timing of this surgical intervention in pediatric patients remains controversial. Septal cartilage is known to play a role in midface development; early animal studies cautioned surgeons to avoid corrective nasal surgery in children for perceived risk of stunting nasal and facial development.2 -4 However, recent studies have suggested that a delay in surgical correction may yield further functional, cosmetic, and social impairments including chronic mouth breathing, dental misalignment, rhinosinusitis, and abnormal facial growth.5 -7 Therefore, a balance between functional improvement and craniofacial development must be considered.
Recent literature has supported the safe practice of pediatric septoplasty in children as young as 6 years without developmental sequelae.8 -10 Some studies have also suggested that septal surgery may even be considered in neonates if severe airway obstruction is present as these individuals are obligate nasal breathers.11,12 When appropriately indicated, septoplasty has demonstrated clinical improvement for children across a variety of quality of life measures.13 -16
A recent meta-analysis suggests that there are low complication rates for adult septoplasty. 17 Minor complications including epistaxis, septal hematoma or abscess formation, dental pain, and synechiae are reported at varying rates in the medical literature. While some bleeding in the postoperative period is expected, rates of significant epistaxis following septoplasty are reported at <1%.18,19 Other complications including septal hematoma and infection are reported between 0.5% – 2.5%.18 -22
In the pediatric literature, there is limited data with regards to major postoperative complications following septoplasty, with some small studies commenting on acceptable rates of postoperative pain, epistaxis, and synechiae formation.14,15,23-25 The present study sought to assess 30-day complication rates following pediatric septoplasty. To the best of our knowledge, this is the largest retrospective study exploring these outcomes within a pediatric population.
Methods
A retrospective study was conducted using the American College of Surgeons National Surgical Quality Improvement Program Pediatric (NSQIP-P) database from 2018 to 2019. A total of 1461 pediatric cases of septoplasty were identified using Current Procedural Terminology (CPT) code 30520 (septoplasty or submucous resection, with or without cartilage scoring, contouring or replacement with graft). Patients with a diagnosis of deviated nasal septum were identified for inclusion using the International Statistical Classification of Diseases and Related Health Problems (ICD-10) code J34.2. Patients with other diagnoses, including rhinosinusitis, cleft deformity, or nasal bone fracture were excluded from this analysis. Patients undergoing septoplasty (CPT 30520) plus concurrent inferior turbinate reduction (CPT 30130, 30140, 30801, 30802, 30930), nasal endoscopy (CPT 31231), or adenoidectomy (CPT, 42831, 42835, 42836) were also included in this cohort. Patients undergoing concomitant endoscopic sinus surgery were excluded. A total of 729 patients met inclusion criteria and were therefore included in the final analysis.
Relevant clinical information including patient demographics, medical comorbidities, operative characteristics, and postoperative outcomes was abstracted for subsequent analysis. The primary effect of age was grouped into 4 categories: children (<6 years), pre-pubertal (6-12 years), pubertal (13-15 years), and post-pubertal adolescents (≥16 years). Postoperative complications were classified as total complications, which included infection, dehiscence, pneumonia, reintubation, stroke, seizure, cardiac arrest, bleeding, or shock. Of note, complication categories were not mutually exclusive.
Data analysis was performed using SAS software (version 9.4; SAS Institute, Cary, North Carolina). Demographic and clinical factors were summarized utilizing basic descriptive statistics. Bivariate associations between categorical measures were evaluated using Fisher’s exact test. Significant predictors (defined as P < .05) were considered in multivariable logistic and linear regression models according to distribution, along with the continuous predictor, BMI. A manual backward selection procedure was followed for each model until only factors with P < .05 remained. For the multivariable logistic regression model assessing length of stay (LOS; <1 vs ≥1), location was excluded (inpatient vs outpatient). A P-value < .05 was used to define statistical significance.
Since the NSQIP-P is publicly accessible and does not include patient- or site-specific identifiers, this study was deemed exempt from review by the Penn State Milton S. Hershey Medical Center Institutional Review Board. American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Results
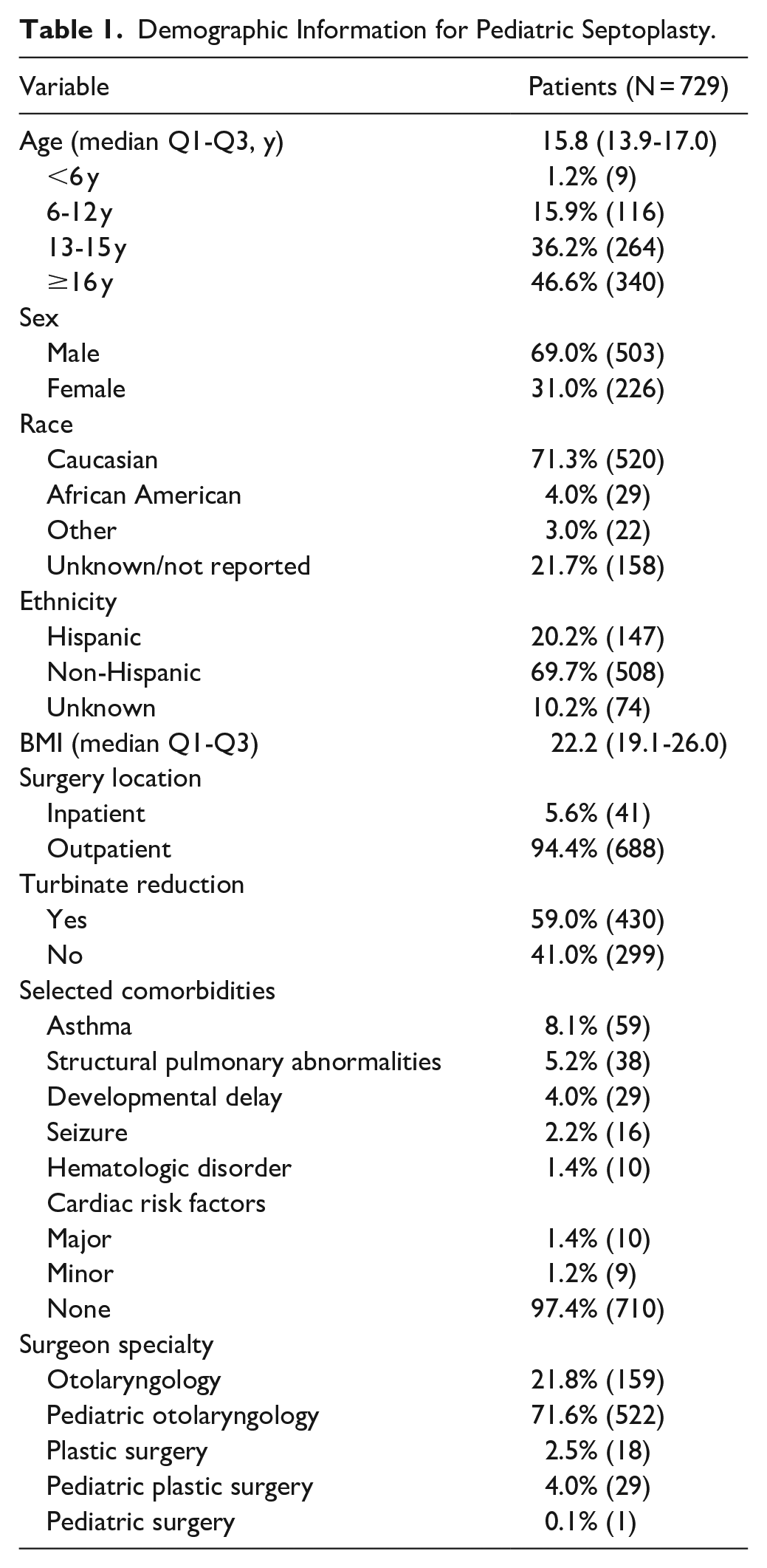
Among the 729 pediatric patients, the median age was 15.8 years, with 36.2% 13 to 15 years old and 46.6 % ≥16 years old. The majority of patients were Caucasian (71.3%) and male (69%) and most cases were performed in an outpatient setting (94.4%). Around 59% of patients had concurrent inferior turbinate reduction (n = 430), 8% had adenoidectomy (n = 55), and 3% had nasal endoscopy (n = 21). Preoperative comorbidities in the population included asthma (8.1%), structural pulmonary or other airway abnormality (5.2%), and developmental delay (4.0%). Most procedures were performed by a pediatric otolaryngologist (71.6%). Table 1 further illustrates the study population’s demographics.
Demographic Information for Pediatric Septoplasty.
The median operative time was 64.0 minutes (Table 2). Caucasian patients had the shortest mean operative time (mean (minutes) [95% CI], 105.3 [86.3-124.2]) while other ethnicities had longer operative times on average (124.9 [99.2-150.5], P < .001). Males also had a significantly longer average operative time compared to females (118.5 [98.7-138.4] vs 110.5 [90.6-130.4], P = .016). Patients who remained inpatient similarly had significantly prolonged operative times compared to those who were outpatient (125.2 [102.9-147.5] vs 103.9 [84.9-122.8], respectively, P = .002). Comorbid structural pulmonary or other airway abnormalities were also significantly associated with longer operative time (122.9 [100.3-145.6] vs 106.1 [87.4-124.8], respectively, P = .015). Otolaryngologists had the shortest operative time (87.3 [75.7-98.8]), followed by pediatric otolaryngologists (95.2 [84.7-105.6]) and pediatric plastic surgeons (98.2 [80.6-115.9]), whereas pediatric surgeons had the longest operative time (177.3 [95.8-258.9], P = .010).
Operative Characteristics and Postoperative Complications for Pediatric Septoplasty.
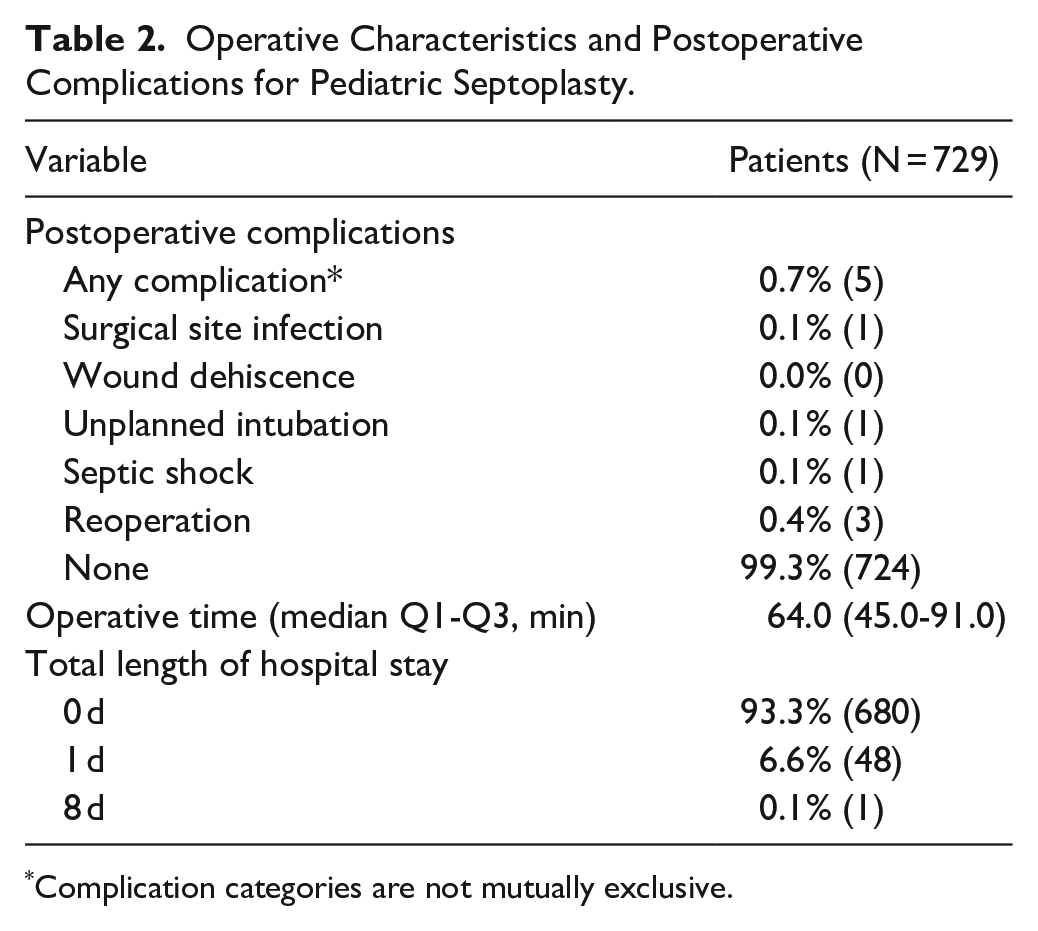
Complication categories are not mutually exclusive.
Most children spent <1 day in the hospital following septoplasty (Table 2). Concomitant inferior turbinate reduction did not have a significant association with LOS (P = .135). Several comorbidities were bivariately associated with increased LOS (≥1 day), including ethnicity (P = .001), asthma (P = .050), developmental delay (P = .010), hematologic disorder (P < .001), and structural pulmonary or other airway abnormality (P = .002). Children with LOS ≥ 1 day also had higher BMI than those with LOS < 1 day (mean BMI [SD], 22.3 [7.18] vs 25.6 [9.60], P = .022). Table 3 demonstrates key findings related to medical comorbidities.
Bivariate Associations Between Patient Demographics and Length of Stay (LOS) for Pediatric Septoplasty.
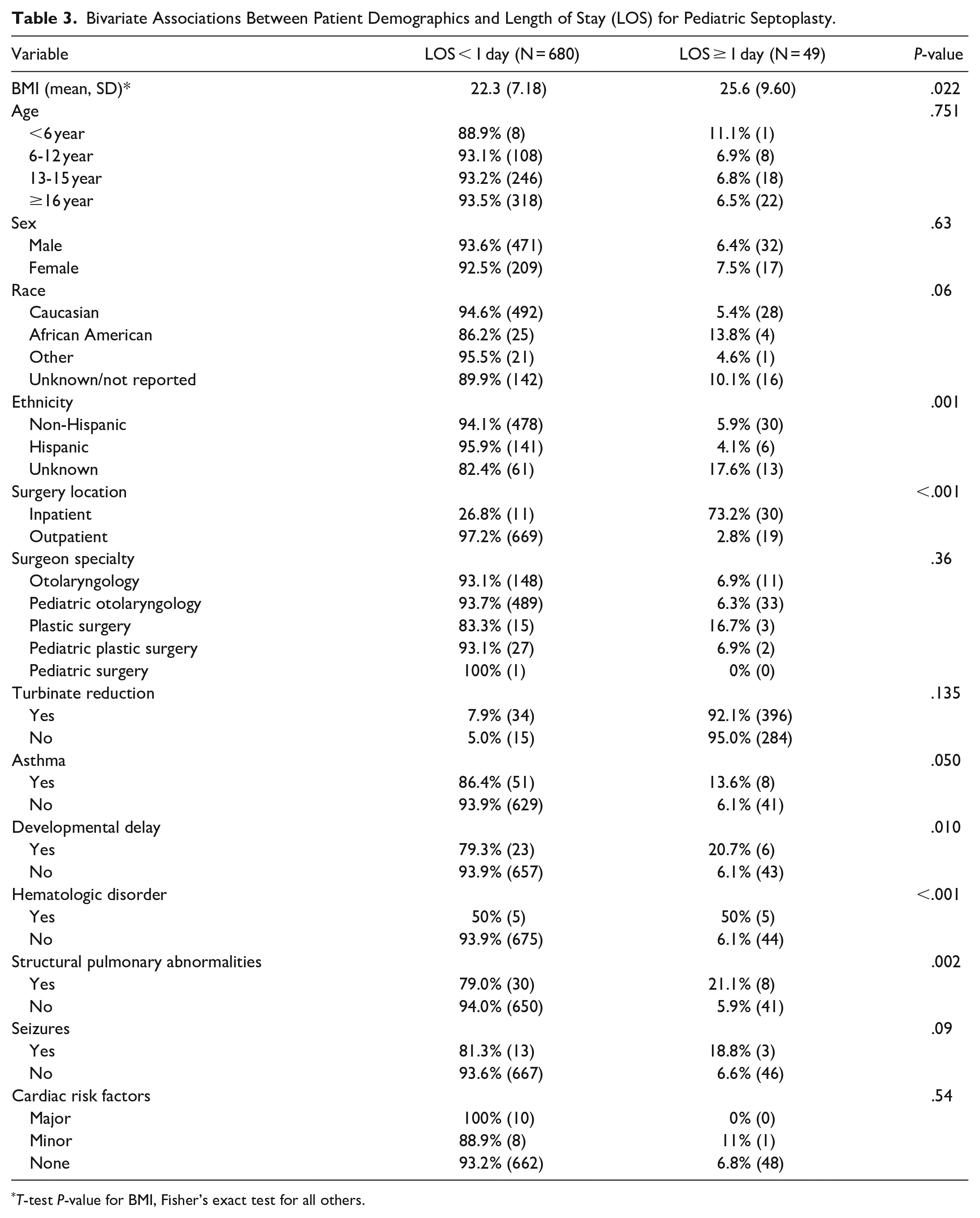
T-test P-value for BMI, Fisher’s exact test for all others.
The overall complication rate was low (0.7%; n = 5), with reoperation serving as the most common postoperative complication (0.4%). Reintubation was necessary for 1 patient and 1 patient had both unplanned intubation and septic shock (Table 2). As demonstrated in Table 4, children with postoperative complications had higher BMI than those without complications (mean [SD], 30.6 [4.94] vs 22.5 [7.40], P = .028). Additionally, a history of asthma was found to be significantly related to postoperative complications bivariately (P = .035), where asthmatics had a complication rate of 3.4%. Children with a history of asthma were 11.7 times more likely to develop a postoperative complication (95% CI [1.62-84.75]). Of note, inferior turbinate reduction did not have a significant association with 30-day complications (P = .654).
Bivariate Associations Between Patient Demographics and Postoperative Complication for Pediatric Septoplasty.
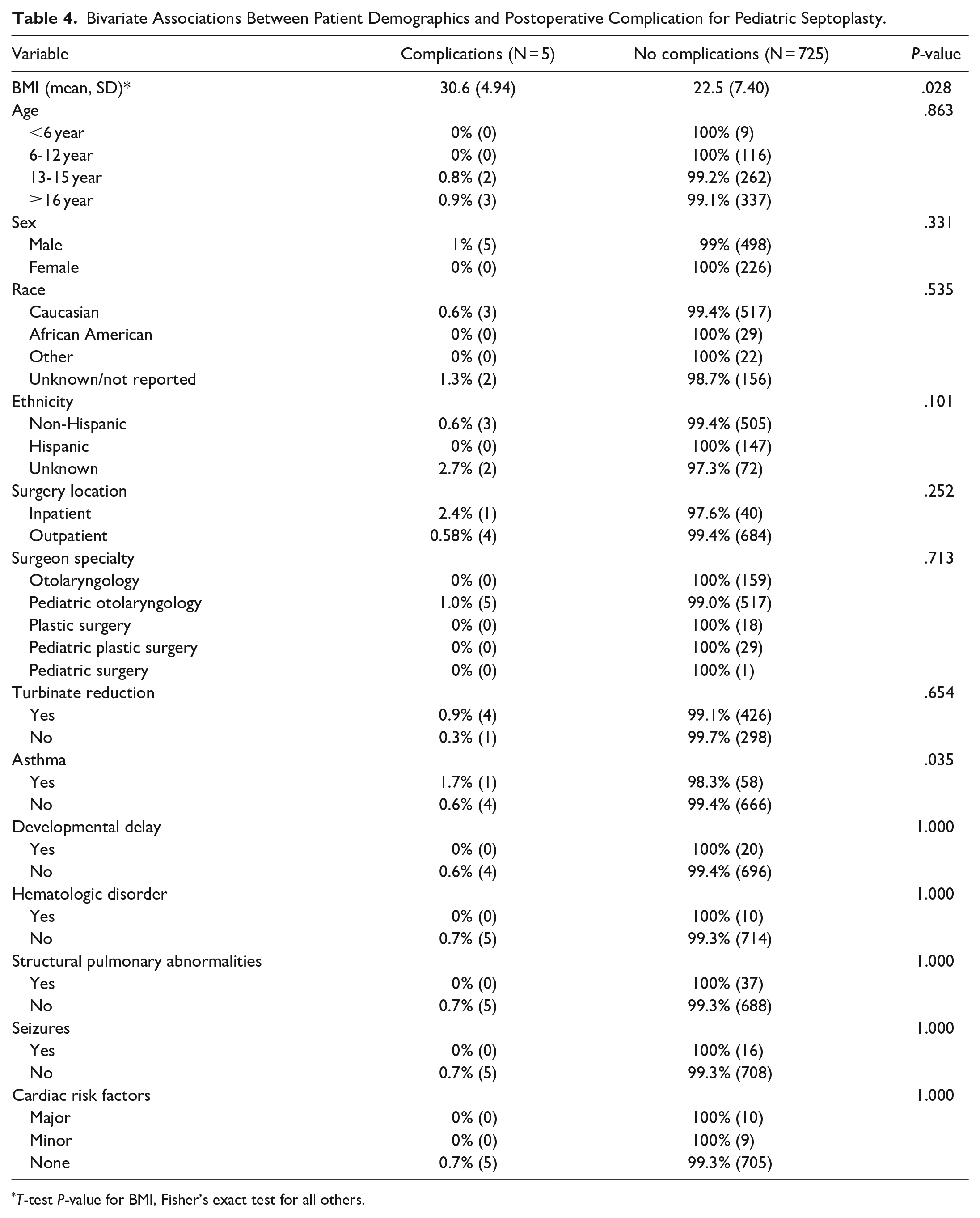
T-test P-value for BMI, Fisher’s exact test for all others.
Discussion
The present study utilizing the NSQIP-P database to assess 30-day postoperative outcomes in pediatric septoplasty is unique in its large size and assessment of age groups and other clinical variables. Most pediatric patients undergoing septoplasty were ≥13 years of age, with just 15.9% and 1.2% ages 6 to 12 and <6 years, respectively. A systematic review of nasal growth and maturation in adolescents reported that maximum nasal growth velocity occurs between ages 8 and 12 in females and at approximately age 13 in males. 26 Evidence also suggests that the completion of nasal growth occurs anywhere from age 14 to 16 in females and 16 to 18 in males.26 -28 Therefore, increased prevalence of septoplasty after age 13 may reflect provider preferences to wait until the pubertal or post-pubertal period when nasal structures have surpassed their peak growth. 29
Notably, most patients were male (69%), which is similar to rates of pediatric male patients undergoing septoplasty reported in the literature (67%-68%).13,30 Additionally, comprehensive otolaryngologists and pediatric otolaryngologists performed the majority of septoplasty. Certainly, fellowship-trained pediatric otolaryngologists may be more likely to see children or adolescents requiring septoplasty as part of their practice as compared to general otolaryngologists. Nonetheless, complication rates did not vary by surgeon subspecialty.
The significant differences in operative time by specialty may reflect surgeon comfort with various surgical techniques for septoplasty as well the degree of complexity associated with performing pediatric septoplasty in young children with complex sinonasal anatomy. While the NSQIP-P database does not contain data on specific operative techniques employed in our study population, endoscopic septoplasty has been associated with significantly shorter operative time as compared to open approaches. 17 Surgical technique may vary by provider specialty as well as on a case by case basis and may contribute to the observed variations in operative time in the present study.
Overall, the 30-day complications following pediatric septoplasty reported in NSQIP-P were rare, demonstrating that severe, life-threatening complications are highly unlikely in pediatric patients. However, data regarding complications specific to septoplasty were unavailable in the NSQIP-P database. Nonetheless, complications commonly reported in septoplasty include persistent nasal obstruction, septal perforation, and external deformity.18-21,31 Additional postoperative complications include epistaxis, septal hematoma or abscess, and synechiae formation,18,20 -22 and major complications such as cerebrospinal fluid leak and blindness are exceedingly rare. 31 A previous retrospective study of outcomes among 194 pediatric septoplasty patients found no difference in perforation, epistaxis, and septal hematoma rates between age groups. 30 The percentage of patients requiring revision septoplasty was significantly higher in patients <14 years of age than patients >14 years. Persistent airway obstruction was the primary indication for revision in both the younger and older cohorts (86% and 50%, respectively). Provider concerns for persistent obstruction or external deformity caused by interruption of nasal growth centers in septoplasty surgery may explain the age trend toward older adolescence among patients in the present study. Nevertheless, the medical literature suggests technical considerations in pediatric septoplasty to reduce interference with normal nasal growth processes.9,32,33
This is the first study to identify asthma as a risk for 30-day complications in pediatric septoplasty, with asthmatics 11.7 times more likely to develop complications than those without. Comorbid asthma also contributed to LOS greater than 24 hours. These associations are likely 2-fold: risks of general anesthesia, such as bronchospasm from intubation, 34 and limited nasal function following septoplasty. In general, asthmatics face higher risks of pulmonary complications during the perioperative period as well as increased risks of various complications following surgery, including pneumonia, septicemia, and urinary tract infections.35 -37 The second concept is related to the unified airway model. This framework states that the respiratory tract is considered an integrated system, behaving as an organized, functional unit. Exacerbation of disease across 1 component of the airway is likely to encourage transient worsening of airway disease diffusely. 38 For example, the medical literature demonstrates associations between nasal allergen provocation and generalized airway inflammation.39,40 Therefore, upper airway manipulation during intubation and the septoplasty surgery itself may contribute toward lower respiratory dysfunction in asthmatics. Routinely querying about a history of asthma exacerbation and medication compliance should be performed by otolaryngology as well as anesthesia in the perioperative period to ensure appropriate counseling is provided to optimize outcomes following pediatric septoplasty. 36 Our findings may allow providers to better inform asthmatic patients of their risk of complications following septoplasty and foster shared decision-making with this subset of the population.
A total of 6.7% of patients required LOS greater than 24 hours, which was found to be significantly driven by African American race. Previous studies have also reported prolonged LOS among African American versus Caucasian patients, 41 even in the setting of uncomplicated surgery and in-hospital recovery, which may be attributed to variation in access to resources such as transportation, socioeconomic status, and distance from the hospital. 42 Additionally, children with developmental delay were more likely to have prolonged LOS. The literature demonstrates significant associations between increased LOS and worse cognitive outcomes in the pediatric population, and children hospitalized for extended periods are disproportionately developmentally delayed or disabled.43,44 Nevertheless, these trends could reflect data not captured by the NSQIP-P database including patient-, provider-, and health care system-level factors that may contribute to these inequities, thus warranting further exploration.
This analysis is the first to demonstrate that overweight patients were more likely to have prolonged LOS following pediatric septoplasty. The medical literature reports a high incidence of postoperative adverse respiratory events in obese children compared to their normal-weight counterparts for all surgical indications. 45 In adenotonsillectomy, poorer surgical outcomes, increased perioperative complications, and longer mean hospital LOS have been observed in obese children.46 -48 Fung et al 46 revealed a biphasic trend in postoperative respiratory complications in obese children after adenotonsillectomy, with the incidence of adverse events in the immediate recovery period seeming predictive of first-night problems; therefore, recommending overnight hospitalization for children with BMI ≥ 90th percentile for age and gender regardless of whether they experience complications after surgery. 46 Additionally, hospital systems may have guidelines in place requiring high-BMI children to be operated upon at the main hospital as opposed to an outpatient surgery center, which may contribute to increased LOS. Furthermore, overnight monitoring among children with high BMI specifically in the setting of septoplasty may be warranted, but certainly requires further exploration.
As expected, inpatient surgical procedures were related to increased LOS. Hematologic disorders also contributed to LOS greater than 24 hours. This may reflect a longer period of observation for bleeding complications such as postoperative hemorrhage and septal hematoma formation among these patients.49,50 Additionally, patients with comorbid pulmonary abnormalities were more likely to have prolonged LOS. The anatomy of a child’s airway can influence the risk of perioperative respiratory complications. 51 As pediatric septoplasty patients often require nasal splints and/or packing, they may become reliant on mouth breathing during the recovery process. Therefore, extending monitoring of breathing and pulmonary functional status may have been necessary in this particular subset of the study population.
Limitations
There are several limitations to consider in this analysis. Databases such as NSQIP-P may have misclassified data elements and not all patients with our inclusion criteria are prospectively enrolled, which introduces informational and selection bias, respectively. Uncontrolled confounders may exist that were not captured by NSQIP-P, which may unknowingly contribute to some of our study findings. NSQIP-P does not have availability of certain variables that may be relevant to our assessment of pediatric septoplasty. For example, we could not compare postoperative pain between age groups, which may be associated with intolerance of nasal splints in younger patients, and a consideration for delaying surgery until the child is more mature. Additionally, we could not assess longer-term complications and the impact of surgical technique, as this may contribute to complication rates beyond 30 days.
Conclusions
Severe postoperative complications in the pediatric population after septoplasty are uncommon, and LOS was less than 24 hours for most patients in this study. Asthma was significantly associated with postoperative complications, highlighting the importance of perioperative assessment of asthma exacerbation history and medication compliance. Interestingly, age did not significantly influence the 30-day complications assessed within NSQIP-P. Several factors may influence operative time and LOS in pediatric septoplasty, including race, gender, BMI, and history of asthma, developmental delay, hematologic disorder, or structural pulmonary abnormality, for which further investigation may be warranted.
Footnotes
Author Contributions
Sarah Benyo: Analysis and interpretation of data, drafting, and critical revisions of the final manuscript. Annie E. Moroco: Concept design, analysis and interpretation of data, drafting, and critical revisions of the final manuscript. Robert A. Saadi: Concept design, drafting and critical revisions of the final manuscript. Vijay A. Patel: Concept design, critical revisions of the final manuscript. Tonya S. King: Analysis and interpretation of the data, final approval of the manuscript. Meghan N. Wilson: Concept design, final approval of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.