
Abstract
Objectives:
Obstructive sleep apnea (OSA) is characterized by repeated upper airway collapse while sleeping which leads to intermittent hypoxemia. Upper airway stimulation (UAS) is a commonly practiced modality for treating OSA in patients who cannot tolerate, or do not benefit from, positive airway pressure (PAP). The purpose of this study is to identify the effect of lateral pharyngeal collapse patterns on therapy response in UAS.
Methods:
A retrospective cohort study from a single, tertiary-care academic center was performed. Patients who underwent UAS between October 2016 and July 2019 were identified and analyzed. Drug-induced Sleep Endoscopy (DISE) outcomes between Apnea-Hypopnea Index (AHI) responders and AHI non-responders were compared. Those with complete concentric collapse at the velopharynx were not candidates for UAS.
Results:
About 95 patients that underwent UAS were included in this study. Pre- to Post-UAS demonstrated significant improvements in Epworth Sleepiness Scale (12.0 vs 4.0, P = .001), AHI (29.8 vs 5.4, P < .001) and minimum oxygen saturation (79% vs 83%, P < .001). No DISE findings significantly predicted AHI response after UAS. Specifically, multiple types of lateral pharyngeal collapse patterns did not adversely effect change in AHI or AHI response rate.
Conclusion:
Demonstration of lateral pharyngeal collapse on DISE, in the absence of complete concentric velopharyngeal obstruction, does not appear to adversely affect AHI outcomes in UAS patients.
Level of Evidence
VI
Keywords
Introduction
Obstructive sleep apnea (OSA) is characterized by repeated upper airway collapse while sleeping which leads to intermittent hypoxemia. 1 This disorder has been reported to occur in 10% of the population and if untreated, OSA can lead to long-term side effects including cardiovascular, pulmonary, and neurocognitive impairment. 2 First line treatment for OSA is positive airway pressure (PAP). While PAP decreases the untoward effects of untreated OSA, adherence and tolerance rates among patients are low. 3
Due to frequent PAP intolerance, adjunctive therapies such as oral appliances and sleep surgery have traditionally been utilized as approaches toward lessening OSA disease burden. In 2014, the United States Food and Drug Administration (FDA) approved upper airway stimulation (UAS) as a new intervention for moderate to severe OSA for patients with PAP intolerance. Approval was based on results from the Stimulation Treatment for Apnea Reduction (STAR) Trial which demonstrated improvements in both apnea-hypopnea index (AHI) and quality of life scores. Subsequent analysis and 5-year outcomes from the STAR Trial cohort have demonstrated a sustained AHI-response in 75% of patients treated.4,5
Prior to undergoing UAS, patients must undergo pre-intervention drug induced sleep endoscopy (DISE). Patients with complete concentric collapse at the velopharynx on DISE are not appropriate for UAS, as the device does not adequately address this pattern of anatomical collapse. 6 However, UAS outcomes are less studied in regards to other patterns of anatomical collapse, specifically partial lateral collapse of the velopharynx, oropharynx, and hypopharynx.
As UAS implantation is becoming a more common modality for treatment of OSA, there is value in further understanding how preoperative DISE findings may affect UAS outcomes. The purpose of this study is to identify the effect of lateral pharyngeal collapse patterns on AHI-response in UAS.
Materials and Methods
This study was approved by the University of Kansas Institutional Review Board.
Adult patients who underwent UAS between October 2016 and July 2019 were retrospectively identified using the Healthcare Enterprise Repository for Ontological Narration (HERON) database. The records of these patients were retrospectively analyzed. Demographics, surgical procedure, DISE findings, pre and post Epworth Sleepiness Scale (ESS), and pre- and post-polysomnography data were collected.
Procedure Selection
Procedural intervention was only considered for patients who were PAP intolerant. All surgical candidates underwent preoperative evaluation which included a medical history and physical examination, ESS, polysomnography and DISE. The protocol for performing DISE included a 50mg bolus of propofol followed by a 50 mcg/kg/min drip with slow titration upwards until patient no longer responding, audible snoring present and respirations monitored via end tidal carbon dioxide. Findings on preoperative DISE were organized using the VOTE classification. 7 UAS was offered to patients with moderate to severe OSA, body mass index (BMI) < 35, and without complete concentric collapse of the velopharynx. The Inspire implantable UAS device (Inspire Medical Systems, Minneapolis, Minnesota, USA) was used for all UAS cases. Patients underwent device activation at approximately 1 month postoperatively and postoperative polysomnography was performed at 2 to 3 months after the surgical procedure. Post-intervention polysomnography was completed as a titration study and thus the estimated treatment AHI was utilized.
UAS Outcomes Analysis
Patients were divided into 2 cohorts (AHI responders versus AHI non-responders). AHI responders were based on Sher criteria and defined as those with >50% AHI reduction and post-intervention AHI < 20. 8 Demographic and DISE data were compared between these two cohorts.
Statistical Analysis
Data were analyzed using SPSS Version 25 (IBM Corporation, Armonk, NY). Descriptive statistics were reported as the median and interquartile range. Group comparisons of scale variables were performed using Mann-Whitney U tests. Group comparisons of categorical variables were performed using Chi-squared or Fisher’s Exact tests (cell count < 10). Comparisons of paired samples (pre/post) were done using the Wilcoxon signed-rank test. The 95% confidence intervals (CI) for the median differences were generated with 1000 bootstrap samples using the bias-corrected accelerated method.
Results
Patient Characteristics
About 95 consecutive patients who underwent UAS were included in this study. There was no significant difference in age, BMI, and pre-intervention polysomnography findings between AHI responders and AHI non-responders (Table 1). Surgical success was demonstrated with AHI response in 76/95 (80%) of patients.
Demographics of AHI Response Following UAS.
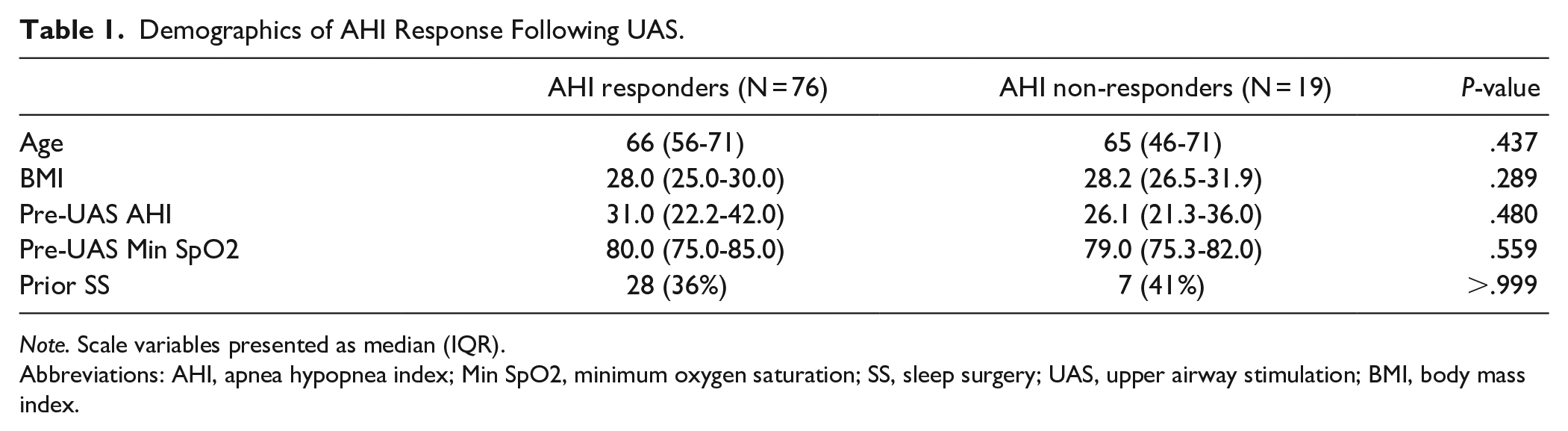
Note. Scale variables presented as median (IQR).
Abbreviations: AHI, apnea hypopnea index; Min SpO2, minimum oxygen saturation; SS, sleep surgery; UAS, upper airway stimulation; BMI, body mass index.
UAS Outcomes
Significant and clinically meaningful improvements from pre- to post-intervention ESS, AHI, and minimum oxygen saturation (min SpO2) were demonstrated (Table 2). A 24.4-point improvement in AHI and a 4.0-point improvement in ESS were noted. Additionally, significant improvement in min SpO2 was achieved (78.9% vs 82.6%, P < .001).
UAS Subjective and Objective Outcomes.
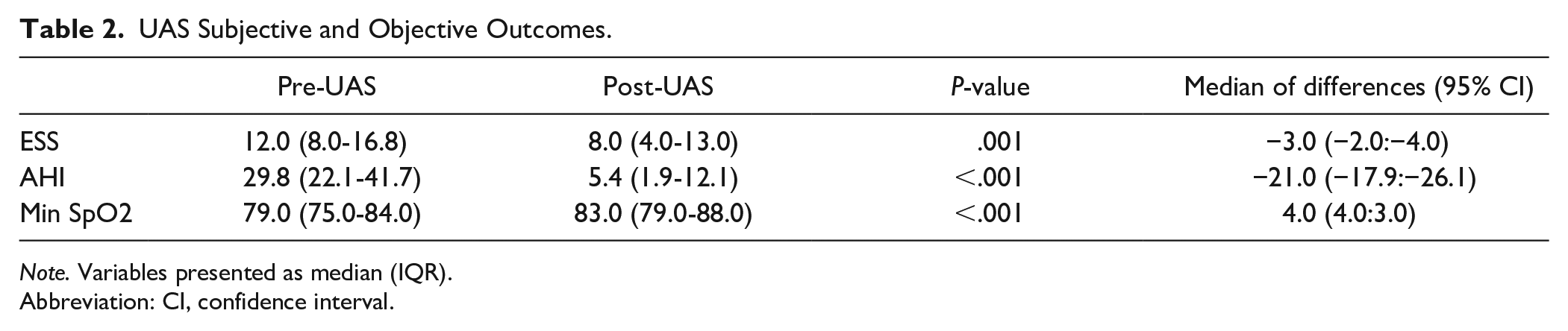
Note. Variables presented as median (IQR).
Abbreviation: CI, confidence interval.
UAS DISE Analysis
Pre-UAS AHI was similar in all types of lateral obstruction cohorts (Table 3), and statistically significant improvement in AHI was noted Post-UAS for all groups except combined velum and oropharynx lateral obstruction. AHI response rate was noted to be similar for all patterns of lateral obstruction (Table 4). In patients with no lateral obstruction (n = 59), AHI response rate was 82.7%. Similarly, in patients with velum lateral obstruction (n = 14), AHI response rate was 78.5%. For patients with combined velum and oropharynx lateral obstruction (n = 5), AHI response rate was 80%.
Effects of Lateral Pharyngeal Collapse on UAS Outcomes.
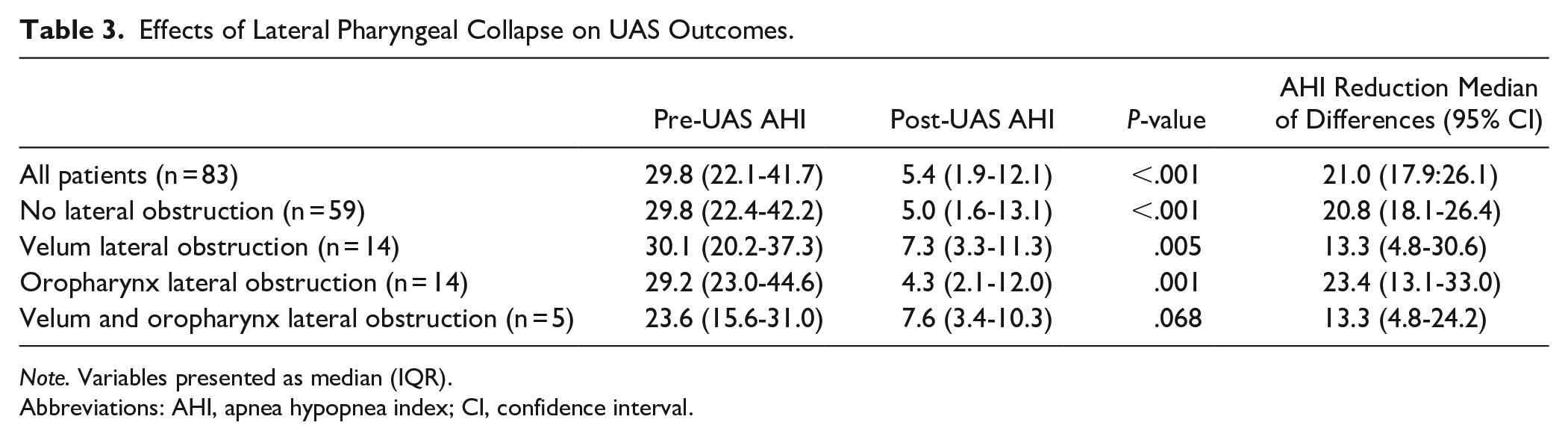
Note. Variables presented as median (IQR).
Abbreviations: AHI, apnea hypopnea index; CI, confidence interval.
Effects of Lateral Collapse on AHI Response Rate.
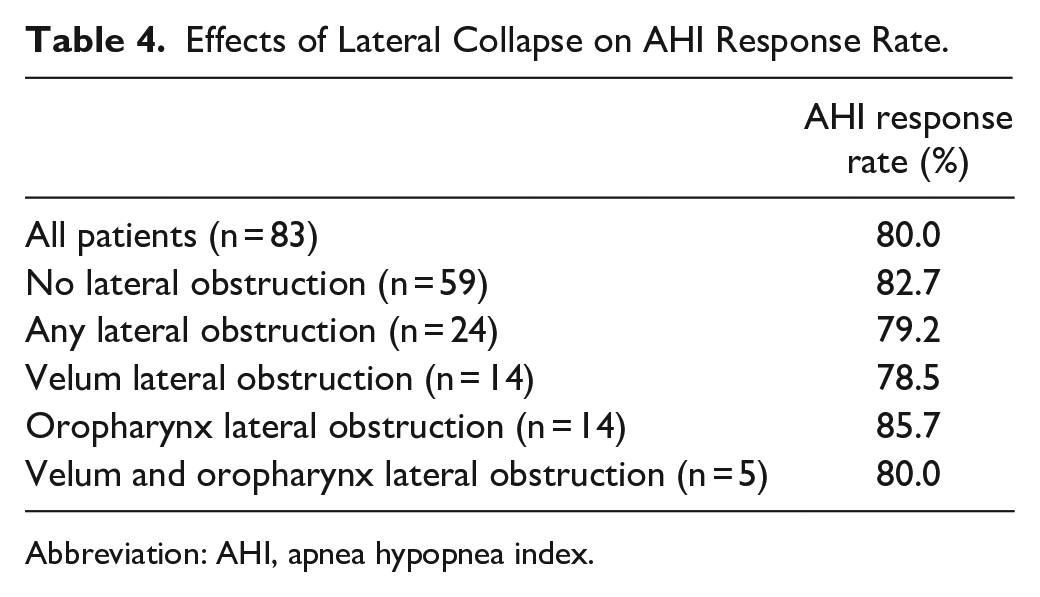
Abbreviation: AHI, apnea hypopnea index.
Discussion
As UAS becomes widely practiced as an adjunctive procedure for patients who suffer from OSA and PAP intolerance, there is benefit in understanding how preoperative DISE findings correlate to AHI outcomes. In this study, 95 patients underwent UAS. Improvement in ESS, AHI, and min SpO2 were demonstrated throughout this cohort. AHI response was noted in 80% of patients. No standalone DISE findings significantly effected AHI response after UAS.
The pivotal data obtained from the STAR clinical trial provided the FDA approval for UAS. Subsequent analysis of the STAR cohort has demonstrated sustained AHI outcomes and safety at 24, 36, 48, and 60 months.4,5,7,9-11 This data has been shown to be reproducible at multiple institutions with improvement in both polysomnographic and quality of life measures. 12 Our experience with UAS adds to this growing body of knowledge as it represents a large patient cohort from a single institution.
Our UAS surgery results appear congruent with those documented in the literature. The STAR trial and a recent systematic review demonstrated a mean reduction in AHI and ESS of 23.9 events/hour and 4.0 points, respectively.3,4 By comparison, our study found a reduction of both AHI and ESS of 24.4 events/hour and 4.0 points.
The prognostic ability of DISE has been extensively studied in sleep surgery procedures, but its prognostic ability in UAS is less studied.13-17 Since complete concentric collapse of the velopharynx was implicated in affecting UAS success, there have been few studies which further examine the prognostic ability of DISE findings.6,18 When stimulating anterior branches of the hypoglossal nerve, a predominantly anterior-posterior dynamic opening of the oropharyngeal airway would be expected. Based on this assumption, and the knowledge that patients with complete concentric collapse at the velopharynx leads to poor UAS outcomes, this study hypothesized that the presence of partial lateral collapse patterns, especially at the velopharynx, would predict worse outcomes following UAS.
However, several studies have demonstrated that stimulation of the hypoglossal nerve does impact airway dimensions at the level velopharynx.19-21 Using fluoroscopy, Goding et al found that opening of the velopharynx occurred in 65% of subjects during upper airway stimulation. 19 Similarly, Safiruddin et al performed awake endoscopy and DISE on a subset of patients after UAS implantation to determine effect of stimulation on both retropalatal and retrolingual collapse. They found that stimulation resulted in significant increase in the cross-sectional area of the airway at both the retropalatal and retrolingual levels. Palatal enlargement occurred in only the anterior-posterior dimension, whereas both anterior-posterior and latero-lateral enlargement were seen at the retrolingual region. 20 Mahmoud et al examined the effect of isolated retropalatal collapse on preoperative DISE and found this pattern to be equivocal to other patterns in regards to UAS success. 21 Our data shows that lateral pharyngeal collapse along the velopharynx and/or oropharynx demonstrated similar results in regards to AHI response rate (Table 4).
In our study, multilevel lateral pharyngeal collapse also demonstrated similar AHI response rates. Although a statistically significant improvement from pre-to-post UAS AHI was not identified (Table 3), an AHI improvement of 13.3 was identified by the median of differences. We suspect that this improvement in AHI is clinically meaningful and significant. There are several reasons this may have not met statistical significance. Firstly, we have a small cohort of patients in this category (n = 5). Secondly, the Pre-UAS AHI tended to be slightly less than the other groups, which makes detection of a meaningful difference more difficult. Thirdly, the Post-UAS AHI tended to be slightly higher (7.6 vs 5.4), which may represent true limitation of UAS in patients with multilevel lateral collapse. Despite this, our study is not adequately powered in order to further elucidate the reason for these findings.
Limitations of this study include its retrospective nature as this limits the ability to fully understand the clinical decision making for each patient. All procedures were performed at a single institution, and therefore, this study is representative of treatment patterns characteristic to the institution. As prior studies have noted, DISE classification using the VOTE system has varying inter-rater consistency. 22 It is not anticipated that this confounding factor altered our results, as DISE classification was performed by only 2 surgeons (CGL and DR). Post-intervention polysomnography data for UAS patients was obtained via titration studies; therefore, the AHI is variable during the encounter. The estimated treatment AHI was utilized to control for this variability.
Conclusion
UAS is successful in treating OSA and lateral pharyngeal collapse patterns did not adversely effect change in AHI or AHI response rate. No standalone DISE findings significantly predicted poorer AHI response after UAS.
Footnotes
Acknowledgements
Mark R. Villwock, MS for statistical support with this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board
The University of Kansas Institutional Review Board reviewed this project and granted approval.
Meeting Information
Data from this manuscript was presented at the AAO-HNSF Annual Meeting September 15 to 18th 2019 in New Orleans, Louisiana.