
Abstract
Objective:
Review a single institution’s vestibular schwannoma (VS) microsurgery experience to determine (1) correlations between demographics, comorbidities, and/or surgical approach on hospital length of stay (LOS) and discharge disposition and (2) trends in surgical approach over time.
Methods:
Retrospective case series from a multidisciplinary skull base program at a tertiary care, academic hospital. All adult (>18 years) patients undergoing primary microsurgery for VS between 2008 and 2018 were included.
Results:
A total of 147 subjects were identified. Surgical approach was split between middle fossa (MF) (16%), retrosigmoid (RS) (35%), and translabyrinthine (TL) (49%) craniotomies. For the 8% of patients had other than routine (OTR) discharge. Mean LOS was significantly longer for patients undergoing RS than either MF or TL. Brainstem compression by the tumor was associated with longer LOS as were diagnoses of chronic obstructive pulmonary disease (COPD) and peripheral vascular disease (PVD). For all discharges, the 40 to 50- and 50 to 60-year-old subgroups had significantly shorter LOS than the 70-years-and-older patients. For the 92% of patients routinely discharged, there was a significantly shorter LOS in the 40 to 50-year-olds compared to the 70-years-and-older patients. There was a significant shift in surgical approach from RS to TL over the study period.
Conclusion:
Over 90% of VS microsurgery patients were routinely discharged with a median hospital LOS of 3.2 days, both of which are consistent with published data. There is an inverse relationship between age and LOS with patients older than 70 years having significantly longer LOS. Brainstem compression, COPD, PVD, and the RS approach negatively affect LOS.
Level of Evidence
4
Introduction
Vestibular schwannoma (VS) is a benign tumor of the nerve sheath of the vestibular branch of the eighth cranial nerve. VS is the most common neoplasm of the cerebellopontine angle (CPA) and internal auditory canal (IAC), representing 90% of all CPA neoplasms. 1 Various population-based registries have estimated the incidence of VS in the United States to be approximately 1 per 100 000 person-years,2,3 but the true incidence based on radiographic and post-mortem studies suggests the incidence may be higher (0.02%-0.9%).4,5
Mean age at the time of VS diagnosis has increased over the past several decades, and tumors are being diagnosed at smaller sizes than in the past.3,6 Studies on the natural history of VS have consistently shown many of these tumors demonstrate slow growth or no growth over time.7-9 Thus, current data supports an initial approach of active surveillance with interval radiographic imaging. 10 However, between 39% and 59% of patients will ultimately require microsurgical excision.3,11-14
Due to the popularization of stereotactic radiation and increasing rates of radiographic surveillance, both of which minimize the potential for adverse outcomes, neurosurgeons and neurotologists are increasingly pressured to provide surgical care that reduces the risk of facial nerve injury and minimizes complications.3,11,12,15 In addition to surgical outcomes, the recent emphasis on healthcare economics can influence the treatment of VS. Specifically, metrics such as hospital length of stay (LOS) contribute to and can be used as proxies for overall treatment cost. This may impact the choice of surgical approach as it affects total hospital adjusted cost. 16 These conclusions are typically generated from large national tumor registry databases, state-wide consortiums, and other collective data repositories rather than within a single institution. The primary objective of the current study is to describe tumor-specific and patient-specific factors that positively or negatively affect hospital LOS following VS microsurgery in a single, tertiary care institution. We also evaluated the effect of surgical approach and patient age on hospital LOS and discharge disposition.
Materials and Methods
Following institutional review board approval, all patients 18-years and older with a diagnosis of VS based on the International Classifications of Disease 9 and 10 (ICD-9 and -10) treated at a single, tertiary care skull base center between 2008 and 2018 were identified. A trained medical abstractor confirmed each diagnosis. Patients with Neurofibromatosis (NF) Type 1 or 2 were excluded. Patients with a prior history of microsurgery and those undergoing salvage microsurgery following radiation therapy were also excluded.
The decision regarding the choice of microsurgical approach (translabyrinthine, TL; retrosigmoid, RS; middle fossa, MF) was made by a multidisciplinary team. Factors including tumor size and location, presenting symptoms, radiographic features, patient age, general health status, and hearing status were taken into consideration.
Data including demographics, medical comorbidities (Diabetes Mellitus, DM; peripheral vascular disease, PVD; chronic obstructive pulmonary disease, COPD; history of cerebrovascular accident, CVA), symptoms, tumor characteristics, audiometric data, and imaging details were collected from the electronic medical record. Pure tone average (PTA) in the tumor ear was calculated using 4 frequency PTA (0.5, 1, 2, and 4 kHz). Tumor volume calculations were performed with commercially available MR segmentation software using semi-automated 3-D conformal volumetric analysis (Philips IntelliSpace Portal Version 9.0, Philips Healthcare, Best, The Netherlands) described previously by the senior author. 17 Brainstem compression by the tumor was determined based on the interpretation of the attending neuroradiologist using the most recent MRI preceding surgical intervention.
Specifics regarding treatment modality were collected, in addition to surgical approach and operative details. Details regarding the postoperative hospital course, including complications, LOS, and discharge disposition were also collected. These data were entered into a Research Electronic Data Capture (REDCap) database, and a retrospective review of the database was performed.
Statistical Analysis
Descriptive statistics were used to summarize the characteristics of the study sample. Several analyzes were performed. Hospital LOS was compared by age group ordinally divided by decade. Tumor size, pre-operative PTA and word recognition score (WRS), LOS, and other than routine (OTR) discharge (OTR discharge includes any disposition other than home including inpatient rehabilitation, skilled nursing facility, discharge to home with live-in nursing care among others, etc.) were compared between the 3 surgical approaches (RS, TL, MF). The comparisons between the surgical groups were performed with both parametric and nonparametric methods depending on the distribution of the data. Comparisons between 2 categorical variables were performed with the chi-squared test or Fisher’s exact test. Nonparametric continuous data were compared using inferential statistics including Kruskal-Wallis rank sum test, eta squared based on the H-statistic, and Cramer’s V. Multivariate analyzes were performed with Poisson regression modeling. RStudio (RStudio, Inc., Version 1.2.5033) and JMP Statistical Discovery Software (Version 16.0.0) were used for statistical analyzes. The criterion for statistical significance was set at P ≤ .05 and effect size was calculated with Hedge’s g due to the different sample sizes between groups. A Hedges’ g value of 0.2 to 0.5 represents a small effect, 0.5 to 0.8 a medium effect, and >0.8 a large effect.
Results
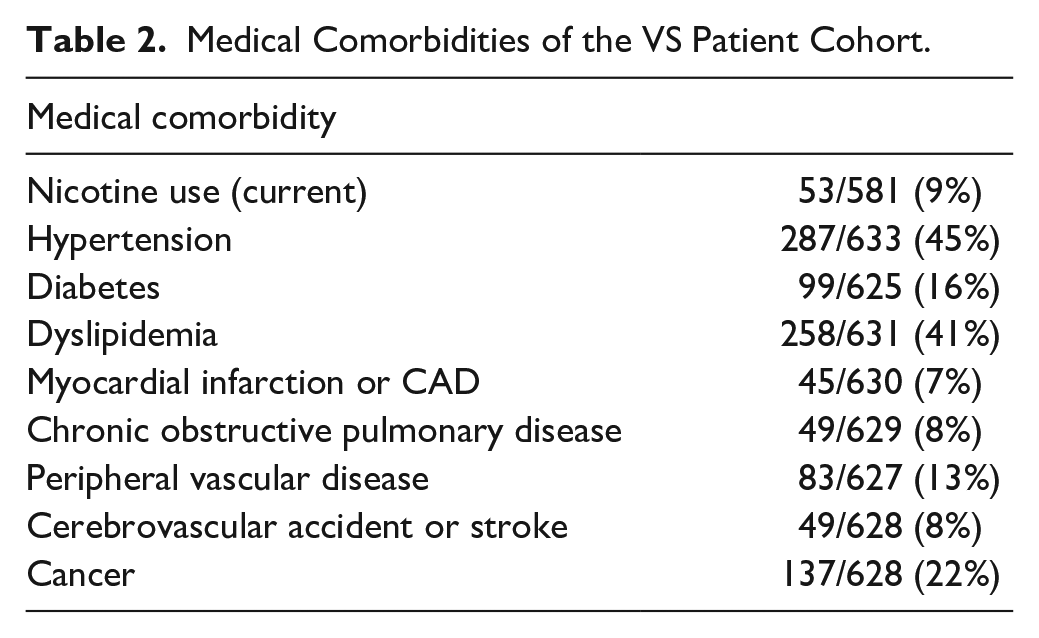
Nine hundred seventy-three patients were identified. Patients with NF/NF-2 (70), history of radiation (11), and patients with a history of prior treatment (270) were excluded. Six hundred twenty-two patients were included (438 observation, 147 microsurgery, and 37 radiotherapy). The inclusion/exclusion flow chart is summarized in Figure 1. Demographic data for the group is shown in Table 1 and a summary of medical comorbidities is summarized in Table 2. Mean pre-operative PTA and WRS for the microsurgery group were 55 dB and 61%, respectively. PTA and WRS in the affected ear did not differ significantly between the observation group and the surgical group. In the surgical group, brainstem compression was seen in 23% of patients and median tumor volume was 840 mm3 (range, 216-8316 mm3). For the entire cohort, brainstem compression was seen in 18% and median tumor volume was 630 mm3. Median tumor volume was significantly larger in the surgical group than the observation group (840 mm3 vs 390 mm3, P = .01).
Baseline Patient Demographics.
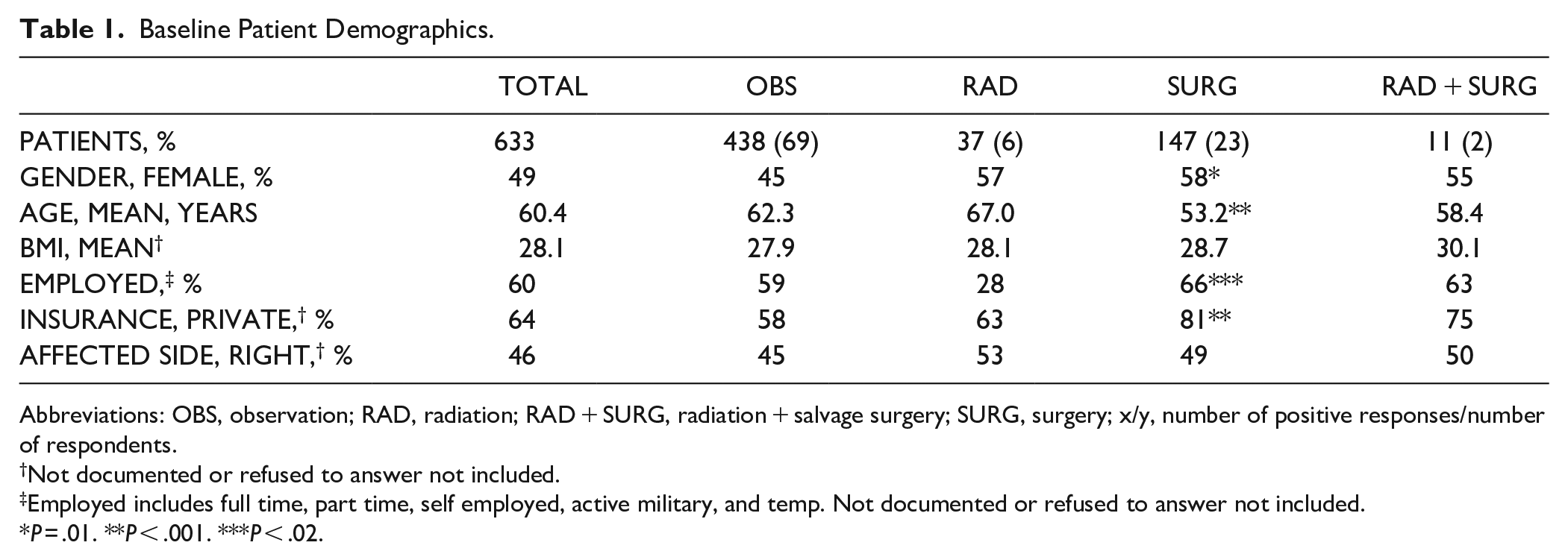
Abbreviations: OBS, observation; RAD, radiation; RAD + SURG, radiation + salvage surgery; SURG, surgery; x/y, number of positive responses/number of respondents.
Not documented or refused to answer not included.
Employed includes full time, part time, self employed, active military, and temp. Not documented or refused to answer not included.
P = .01. **P < .001. ***P < .02.
Medical Comorbidities of the VS Patient Cohort.
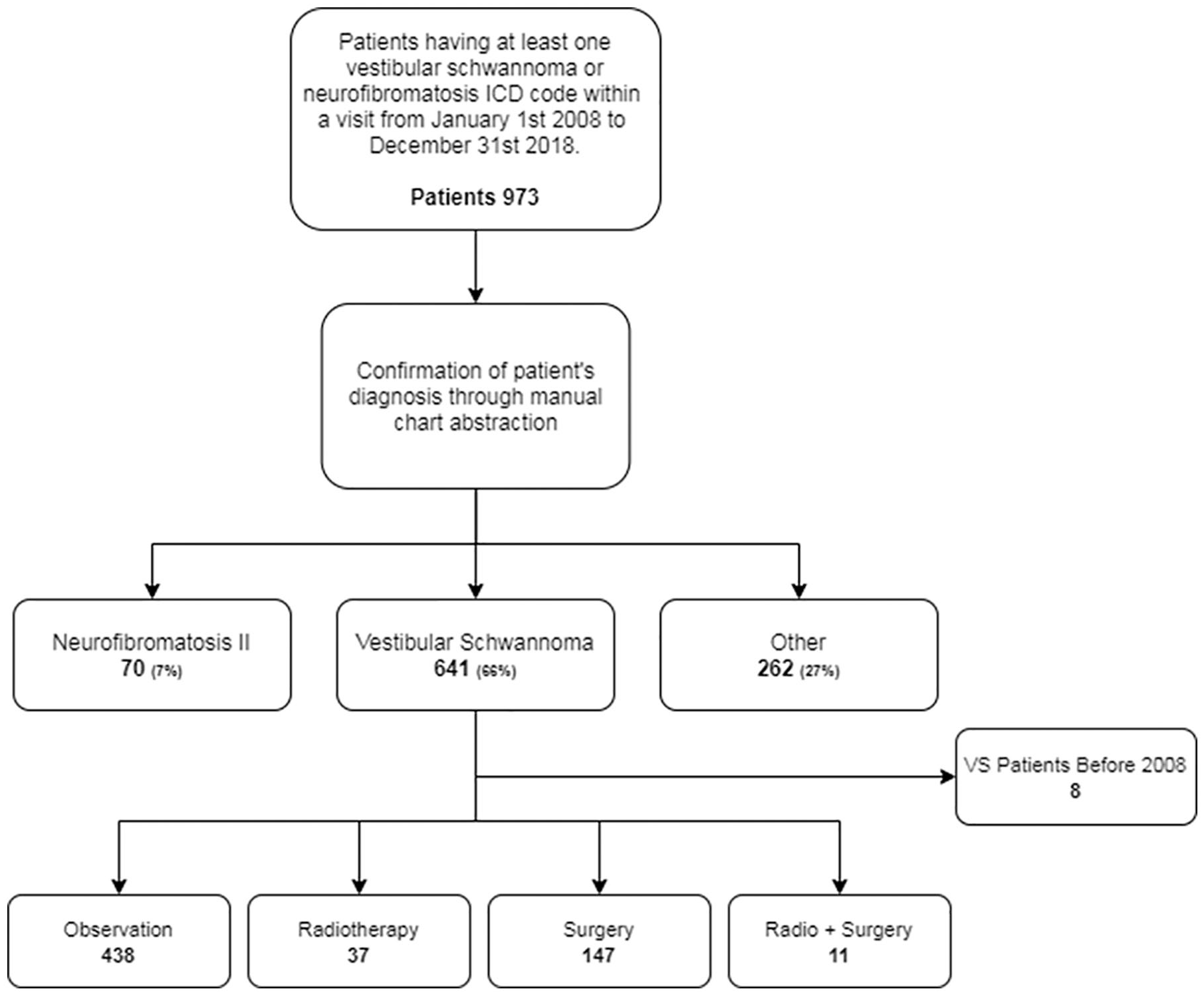
Inclusion/exlusion criteria flow diagram.
Patient age
For all 622 patients, mean age was 60.4 years (SD, 13.4). One hundred forty-seven patients (23%) underwent primary microsurgery. Despite equal distribution of men and women in the surgical cohort (51% vs 49%), women were significantly more likely to undergo microsurgery than men (58% women; 85 women vs 62 men; MF = 11, RS = 30, TL = 44) (P = .01) and patients undergoing microsurgery were significantly younger than patients maintained in radiographic surveillance (53.2 years vs 62.3 years, P < .001). Patients with private insurance were significantly more likely to have microsurgery than radiographic surveillance (81% vs 58%, P < .001).
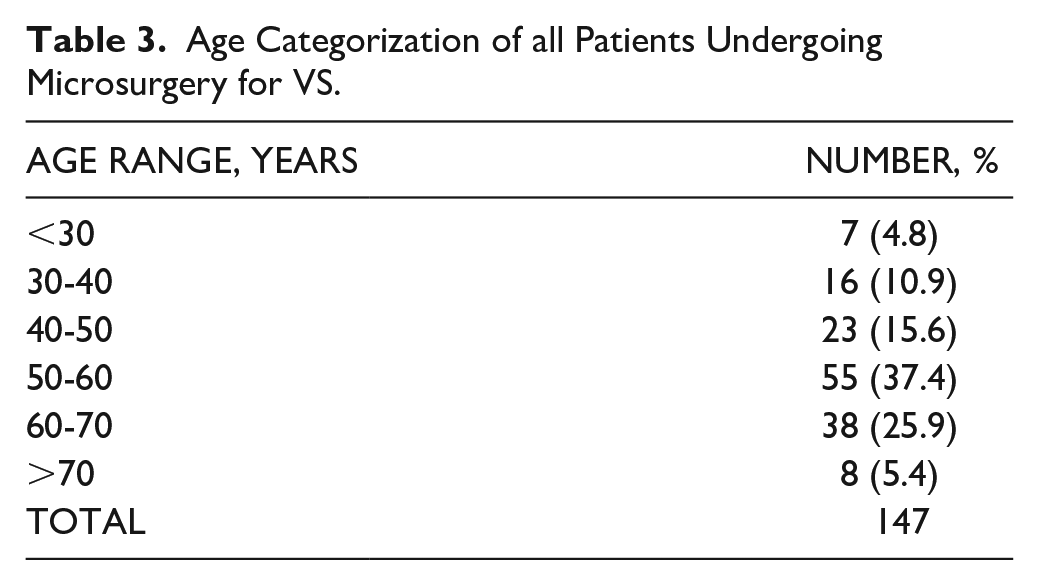
Within our primary microsurgery cohort, mean age was 53.2 years (range, 23.8-74.6). Mean age year-over-year was not statistically different across the study period and ranged from 48 years in 2016 to 59 years in 2012. Approximately 30% of patients were over 60 years old at the time of surgery, and 5.4% over the age of 70 (Table 3). There were never more than 2 patients older than 70 years that underwent surgery in any given year, and in 6/11 study years there was not a single patient over 70 years that underwent microsurgery.
Age Categorization of all Patients Undergoing Microsurgery for VS.
Hospital LOS
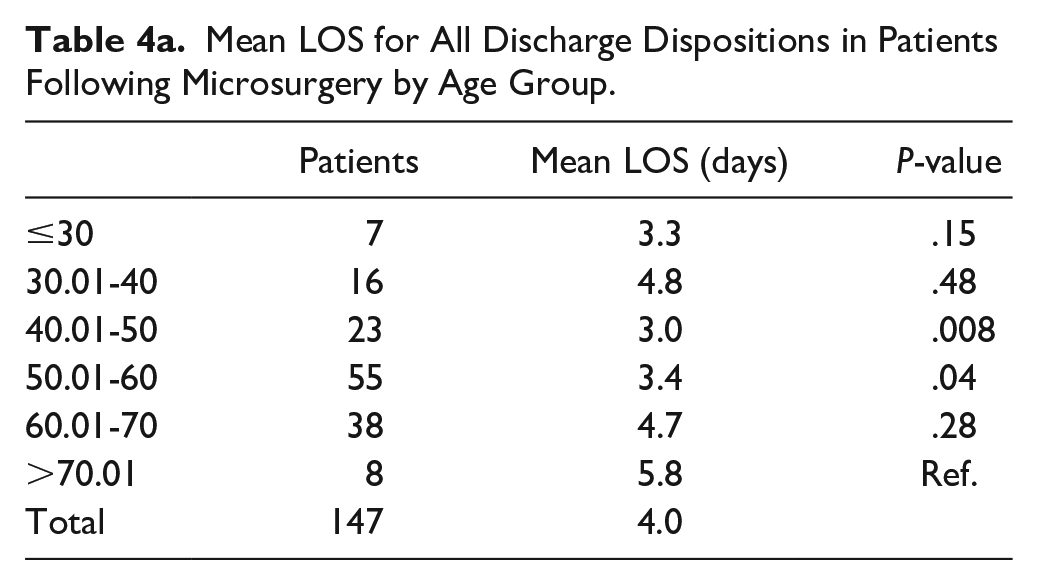
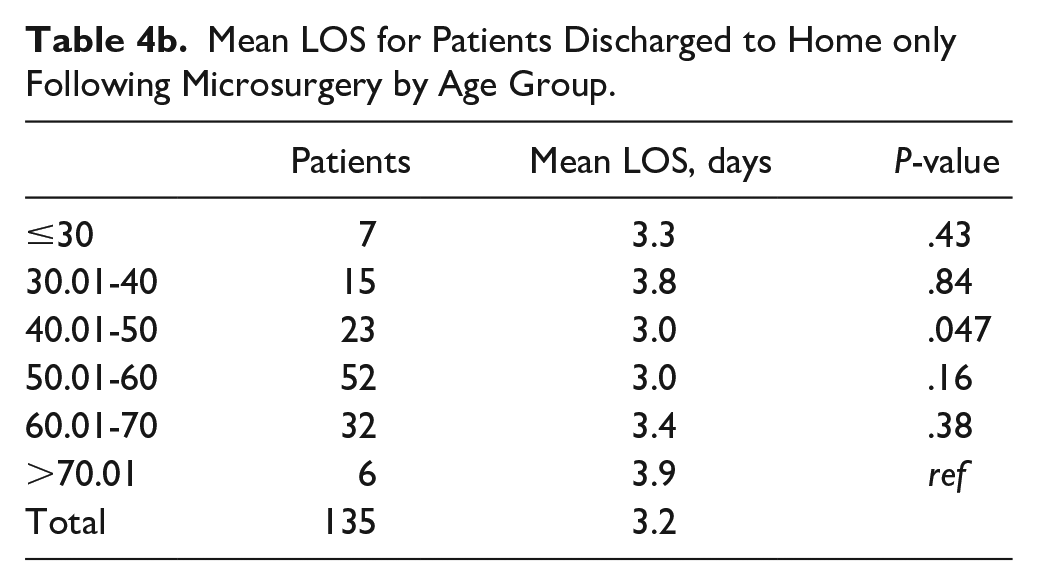
For the 147 microsurgery patients, mean LOS was 4.0 days (median, 3.2 days). Mean LOS in the >70-year-old group was 5.8 days with no other age group having a mean LOS over 5 days. Using the >70-year-old group as reference, there was a significantly shorter LOS in the 40 to 50-year-old and 50 to 60-year-old groups when all discharges were considered (Table 4a). Only 8% of all microsurgery patients had OTR discharge. Considering only the 135 patients with routine discharge, mean LOS was 3.2 days (median, 3.1; range, 1.3-11.2). Mean LOS in the >70-year-old group was 3.9 days, and using the >70-year-old group as reference, there was a significantly shorter LOS in the 40 to 50-year-old group (Table 4b). Although mean LOS decreased between the first half of the study (4.2 days, 2008-2013) and the second half of the study (3.6 days, 2013-2018), this difference was not statistically significant.
Mean LOS for All Discharge Dispositions in Patients Following Microsurgery by Age Group.
Mean LOS for Patients Discharged to Home only Following Microsurgery by Age Group.
Although excluded from analysis, 11 patients with a history of radiation underwent salvage microsurgery. While surgical approach was divided between craniotomy type (MF 18%, RS 27%, TL 55%), median LOS was 4.1 days and 27% (3/11) had OTR discharge. Due to the small number of patients, statistical analysis was not performed.
Differences by Surgical Approach
Table 5 summarizes the data for the 3 microsurgical approaches. The majority of patients underwent RS or TL craniotomy (84%). Mean hospital LOS was significantly longer for patients undergoing RS (2.48 days) than TL (2.09 days, P < .0001) and MF (2.17 days, P = .03) (Figure 2), but surgical approach did not affect routine discharge to home. Brainstem compression was significantly more common in the TL group (22/147; 15%) compared to the MF group (0/147; 0%) (P = .02), but there was no significant difference between the RS (11/147; 7%) and TL groups. Mean tumor volume was significantly larger in both the RS (7291 mm3) (P < .001; Hedges’ g = 0.87) and TL (8780 mm3) groups (P < .001; Hedges’ g = 0.66) compared to the MF (187.2 mm3) group. Mean pre-operative PTA and WRS did not differ between the RS and TL groups, but mean PTA was significantly worse in the TL group (59.4 dB) compared to the MF group (41.7 dB) (P < .1; Hedges’ g = 0.61). Mean WRS was significantly better in the MF group (83.3%) compared to both the RS (64.6%) (P = .02; Hedges’ g = 0.81) and TL (51.5%) (P = .02; Hedges’ g = 0.91) groups. When comparing the first half of the study period to the second half, there was a significant shift from RS to TL procedures (P < .001).
Pre- and Post-Operative Data Broken Down by Microsurgical Approach.
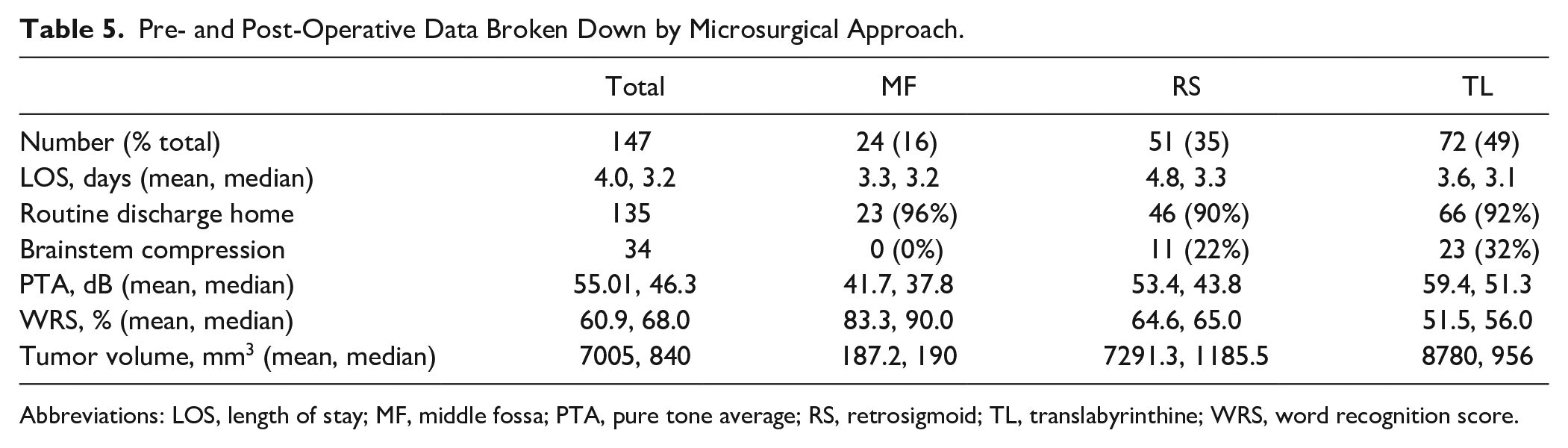
Abbreviations: LOS, length of stay; MF, middle fossa; PTA, pure tone average; RS, retrosigmoid; TL, translabyrinthine; WRS, word recognition score.
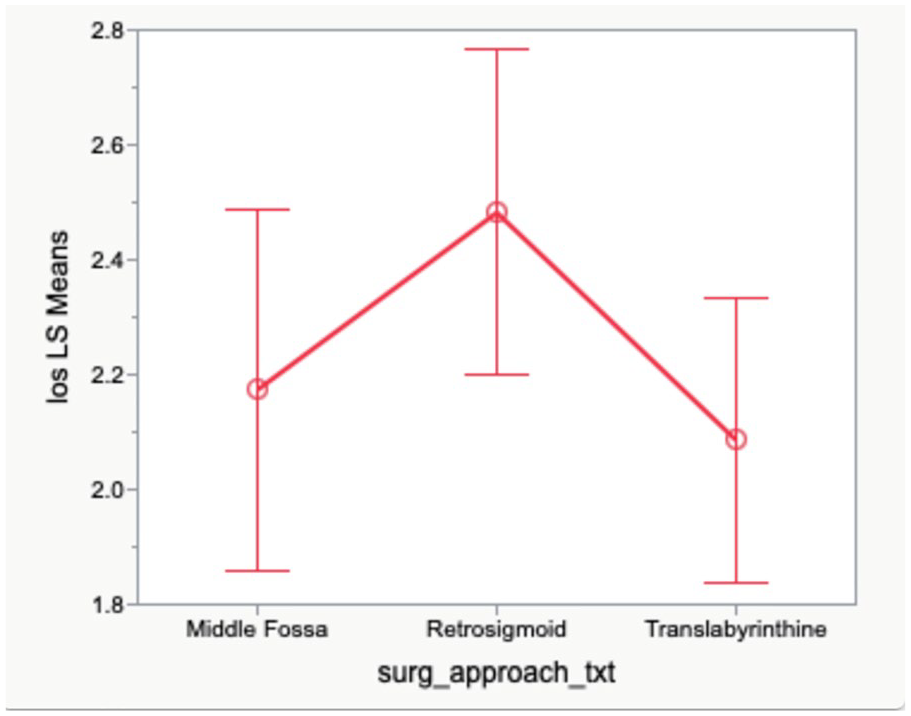
Effect of surgical approach on mean hospital length of stay following VS microsurgery.
Comorbidities and LOS
Patients with brainstem compression had significantly longer mean LOS than patients without (1.96 vs 2.53 days, P < .0001). Patients with a diagnosis of COPD had significantly longer mean LOS than patients without (1.84 days vs 2.66 days, P < .0001). Patients with PVD had significantly longer mean LOS than patients without (1.5 days vs 3.0 days, P < .0001). Interestingly, patients with a diagnosis of DM had a significantly shorter mean LOS than those without (2.13 days vs 2.37 days, P < .05) and patients with a history of CVA had a significantly shorter mean LOS than those without (2.02 days vs 2.48 days, P = .01).
Discussion
Due to the expanding knowledge of the cellular biology and natural history of VS tumors, there has been a gradual shift in the management of these tumors with increasing numbers of patients initially placed into a “wait-and-scan” approach rather than primary microsurgery.13,14,18,19 The majority of the studies comparing treatment modalities use large national tumor registries, state-wide consortiums, and other collective data repositories. These large, pooled data sets likely eliminate institutional and regional biases making the results generalizable, but conversely require assimilation of thousands of data points. Furthermore, many of the large studies rely on survey data which are inherently biased.18-20
There is a relative paucity of literature looking at a large cohort of VS patients treated at a single institution. Single institution data are particularly important given the increasing importance of quality assurance and the economic implications of VS surgery. The present study aims to describe both the tumor-specific and patient-specific factors that affect hospital LOS following VS surgery as well as the trends and practice patterns in a cohort of 147 patients who underwent microsurgical management of VS between 2008 and 2018 at a single, tertiary referral high volume center (HVC) (definition of high volume as >100 cases per Ahmed 2014). 21
The mean patient age for the surgery cohort in the current study is similar to previously published results. Babu et al 12 reported a mean age of 49.8 years in patients undergoing surgery for VS with 23% of all patients ≥65 years old. Multiple studies have similarly demonstrated older patients are less likely to undergo surgical resection of VS, as well as declining rates of VS surgery in patients 65 years and older over the last 2 decades.13,21,22 Torres-Maldonado showed that patients <54 years old were more likely to have surgery than patients 54 to 64 years old (OR, 0.56) and were significantly less likely to undergo surgery as a single treatment modality as they aged. 14
Other studies have shown that patients >65 years old with VS are up to 2.5 times more likely to be managed with observation than definitive treatment, with elderly patients undergoing surgery only in cases of brainstem mass effect.12,13,22,23 One explanation for this tendency towards conservative management in the elderly are the higher complication and mortality rates after VS surgery.24,25 Our study demonstrated that patients undergoing surgery were more likely to have brainstem compression and had significantly larger tumor volumes than the observation group. Unfortunately, these effects were not broken down by patient age. While we did not look specifically at complication rates as a function of patient age, there was only one surgery-related fatality in our cohort, a 69-year-old patient who had a cerebral hemorrhage on post-operative day 2 following TL VS resection.
The patients in our study had a mean hospital LOS of 4.0 days, and when all discharges were considered, the 70-year-old and older group had significantly longer LOS than the 40 to 50- and 50 to 60-year-old groups. While statistical analysis was not performed, persistent headache and ataxia/imbalance were common reasons for prolonged LOS. Hospital LOS is one useful metric when evaluating the health economics of a given intervention, and when accurately predicted can increase the overall efficiency of hospital bed occupancy with resultant financial incentives. 26 Beyond the economic implications of LOS, prolonged hospital stay may place an otherwise healthy patient at risk of nosocomial infections. 27 Previous reports in the general surgery literature demonstrate advanced age impacts postoperative LOS.28,29 Additionally, previous data has shown advanced age significantly impacts intensive care LOS following VS surgery, 25 and advanced age (>65 years) prolongs hospital LOS following VS surgery. 30 Our data are consistent with other large studies showing similar LOS and routine discharge to home rates. 21 Additionally, our result showing older age as a risk factor for prolong LOS is consistent with the literature.
When looking specifically at OTR discharge, 8% of all patients required placement into a skilled nursing facility or inpatient rehabilitation center. The difference in LOS for patients with routine discharge was significantly shorter only for the 40 to 50-year-old group when compared to the >70-year-olds. Some authors have shown higher rates of OTR discharge in patients undergoing RS microsurgery compared to TL.16,31 Our data did not show any significant difference in OTR discharge based on approach. The rate of routine discharge in the current study (92%) is also consistent with other studies showing rates of routine discharge at HVCs between 94% and 96%.21,31
The current study looked at the differences in LOS between the different VS microsurgical approaches and showed patients undergoing RS craniotomy had significantly longer LOS than those undergoing either TL or MF. However, it is important to note, we did not stratify LOS by tumor size. Visagan et al 27 showed that for large tumors (31-40 mm), patients undergoing TL approach had a significantly shorter LOS than patients undergoing RS approach (7 vs 11 days) as well as a significantly shorter intensive care stay. These differences were not significant for smaller tumors. Semaan et al 16 demonstrated LOS and intensive care LOS were significantly longer in the RS group than the TL group, and remained significant for hospital LOS when tumors were stratified by size (≥20 mm). These differences equated to adjusted total hospital cost increases of nearly $10,000. Obaid and colleagues showed a significant difference in LOS between TL and RS (7.5 vs 16 days). The authors attributed this difference to the higher incidence of postoperative ataxia in the RS group due to cerebellar retraction.32,33 Other studies have shown no difference in LOS between approaches. 34 Our study did not evaluate the difference in total costs or complication rates between the approaches. We plan to address these questions in future studies.
Previous studies have shown that tumor size is correlated with postoperative LOS following VS surgery.27,35 However, to our knowledge this is the first study to specifically look at brainstem compression as an independent predictor of LOS regardless of tumor size. Larger tumors are more often associated with brainstem compression, which can complicate surgery and postoperative care, thereby increasing LOS. However, it is also possible that with brainstem compression comes a higher likelihood for postoperative dizziness and/or headaches which can independently prolong hospital stay. 36 It will be interesting in future studies to more closely examine the factors associated with brainstem compression as they relate to hospital stay.
Like other previous studies, the current study showed that comorbid diagnoses of PVD and COPD were predictive of longer hospital LOS.25,37 Similarly, previous research has shown that DM increases postoperative complication risks in non-cardiac surgery, 38 as well as the risk of readmission, acute myocardial infarction, and pneumonia following VS surgery. 39 Interestingly, the current study showed that patients with a history of DM and CVA had a significantly shorter LOS than those without. Importantly, there were no significant differences in frequency of surgical approach for any of the 4 comorbidities examined (PVD, COPD, DM, CVA). It is possible that patients with DM and/or history of CVA are more thoroughly medically optimized prior to surgery thus reducing their risk of complications and subsequently LOS. It is also possible that patients with a history of CVA are more closely surveilled with imaging by their healthcare team and therefore present with smaller tumors without brainstem compression. We did not perform an analysis of tumor size in patients with DM or history of CVA, and this will be the subject of a future study.
Our study demonstrated a significant shift from RS to TL approach over the study period. While the reason(s) for this shift is (are) not completely understood, there are a few possible explanations. First, our experience demonstrated over time that patients undergoing the RS approach tended to have prolonged/chronic headaches following surgery. In patients with non-serviceable hearing or large tumors we therefore tended towards the TL approach even if the tumor was confined mostly to the CPA. Second, over the study period several new surgeons joined the group in both neurosurgery and neurotology, and perhaps some confounding bias was introduced given their experience and preferences. These data have not been specifically explored to elucidate these differences. Third, in performing internal quality assessment of this cohort over time prior to the development of the database, there was some thought that the TL may offer lower rates of post-operative cerebrospinal fluid leak and facial nerve paresis. This question will be the subject of future publications.
This study has several limitations. The main limitation is the retrospective design. Certain data may not have been available or incorrectly entered into the medical record. Missing data can decrease the power of the analysis and incorrect entries can lead to misclassification errors. Retrospective studies introduce a number of potential biases such as selection bias, confounding bias, and allocation bias. The small number of patients in the MF group limited the statistical analysis between groups. Additionally, while LOS and routine discharge were tracked, this study did not specifically investigate the reasons for prolonged LOS or OTR discharge. While this study does show that tumor size can affect microsurgical approach, this dataset does not specifically characterize tumor location, which can often guide recommendations for microsurgical approach. Despite these limitations, our findings demonstrate a comparison of the outcomes between 3 microsurgical approaches to VS as they relate to LOS and hospital discharge. These data are independent of preoperative decision making and are not intended to modify the surgical selection criteria or to determine the surgical approach for VS excision.
Conclusions
The current study is one of the largest, single-institution cohorts to examine surgical management of VS. Over the 11-year period, greater than 90% of all surgical patients were routinely discharged home, with significantly longer LOS in the 70-years-and-older group compared to the 40 to 50- and 50 to 60-year-old groups. Patients undergoing MF approach had smaller tumors by volume and a significantly lower incidence of brainstem compression, and patients undergoing RS craniotomy had a significantly longer LOS than those undergoing MF and TL. Brainstem compression, history of COPD, and history of PVD were correlated with longer average LOS, while history of DM and CVA were correlated with shorter average LOS. The decision to manage VS patients with either microsurgery or radiographic surveillance, as well the choice of microsurgical approach is complex and dependent on many factors including patient preference, symptoms and comorbidities, tumor size and location, and surgeon bias among others. LOS alone cannot be used as a stand-alone outcome for VS microsurgery, but is a useful measure in the assessment of the economics of a health care intervention and has implications for patient care. We believe that a multidisciplinary team approach to VS is ultimately most important for successful outcomes, and future studies are needed to more specifically compare complication rates, costs, and outcomes between the various microsurgical approaches.
Footnotes
Acknowledgements
The authors would like to thank Anna Wright, PhD for assistance with data assimilation, and Tee Bahnson for assistance with statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.