
Abstract
Objectives:
Appropriate management of chronic rhinosinusitis (CRS) among patients with cystic fibrosis (CF) is important in improving quality of life. Otolaryngologists play a critical role in reducing CRS symptom burden. This study seeks to evaluate the role of patient-reported quality-of-life measures in guiding interventions for CF-related sinus disease.
Methods:
We performed a prospective, cross-sectional study of 105 patients presenting to a CF-accredited clinic between July and September 2018. Demographic data and sinus surgery history were collected, in addition to Sino-Nasal Outcome Test (SNOT-22) and Questionnaire of Olfactory Disorders (QOD-NS) scores. Statistical analysis was conducted using correlation and non-parametric Mann-Whitney U tests.
Results:
Baseline well-care visits accounted for 71.4% of all clinical evaluations. Prior otolaryngology intervention was noted in 69 (66%) patients, where the majority of these patients (63/69; 91%) underwent endoscopic sinus surgery (ESS). Patients with a history of otolaryngology intervention had an average SNOT-22 score of 33.2 (SD = 20.6) compared to 24.9 (SD = 18.5) for patients without prior intervention (P = .048). The average QOD-NS score was 5.5 (SD = 6.4) among patients referred to otolaryngologists and 3.1 (SD = 5.7) for non-referred patients (P = .012). SNOT-22 and QOD-NS scores were modestly correlated (R of .43).
Conclusion:
CF patients with symptoms resulting in worse quality-of-life assessments were more likely to have established coordinated care with an otolaryngologist. Further validation of the utility of SNOT-22 and QOD-NS questionnaires as care coordination metrics is necessary in the CF population.
Keywords
Introduction
Cystic fibrosis (CF) is a genetic disorder characterized by dysfunction of the cystic fibrosis transmembrane conductance regulator (CFTR) gene, leading to inspissated mucus and sinopulmonary disease. 1 As sinus inflammation and bacterial colonization progress, CF patients develop chronic rhinosinusitis (CRS) with an inevitable decrease in sinonasal quality-of-life (QoL).2-4 Patient-reported outcome measures such as the Cystic Fibrosis Questionnaire (CFQR-14) 5 and the Sino-Nasal Outcome Test (SNOT-22)6,7 have proven useful in quantifying QoL decline and guiding future management, especially given the lack of standard treatment algorithms for CF-related CRS. 2 The Questionnaire of Olfactory Disorders (QOD-NS) is another instrument that has not been broadly utilized within the CF population, but captures a clinically significant cardinal symptom of CRS, olfactory decline. 8 Importantly, QoL measures can indicate when referral to a specialist is beneficial,9,10 where combining instruments may improve predictive capacity.
Studies have shown that a multidisciplinary approach significantly improves clinical management decisions and patient satisfaction in CF.2,11 Otolaryngologists, in particular, are crucial in both the medical and surgical management of CF patients, with diverse roles ranging from guiding antibiotic selection to performing endoscopic sinus surgery (ESS). 2 In fact, ESS has become a mainstay of treatment for CF patients, and a number of studies have demonstrated significant overall symptom improvement in CF patients after ESS.12,13
Although beneficial, multidisciplinary care may impart challenges for patients, particularly through the burden of added clinical visits. Thus, identifying value-added multidisciplinary collaborations is of particular importance. Here, we evaluate sinonasal quality-of-life measures among patients who underwent otolaryngology consultation to assess the contribution of otolaryngologists in assisting with symptom control. Specifically, we utilize the SNOT-22 and QOD-NS to correlate sinonasal QoL with past otolaryngology evaluation and ESS. We also use these QoL measures to generate receiver-operating characteristic (ROC) curves as a means of predicting relevance of past otolaryngologic intervention.
Patients and Methods
We performed a prospective cross-sectional study of 105 consecutive patients presenting to a CF-accredited clinic between July and September 2018. Inclusion criteria for patients were age >18 years and genetic diagnosis of CF; the exclusion criterion was history of lung transplantation. Visits consisted of regularly scheduled baseline encounters, during which patients had no acute symptomatology, and exacerbations, characterized by an increase in respiratory symptoms (ie, dyspnea, wheezing, cough, hemoptysis) or decline in lung function necessitating increased mucolytic or antibiotic therapy. Approval for the study was obtained from the institutional review board of Columbia University Irving Medical Center (CUIMC). Demographic data, including age, gender, body mass index (BMI), and genotype, were collected, as well as SNOT-22 scores, QOD-NS scores, and self-reported history of care provided by an otolaryngologist. Additionally, data on pulmonary function, current maintenance therapy, and current colonized organisms were recorded. SNOT-22 and QOD-NS scores were hand-calculated; the SNOT-22 consists of 22 items summed for an overall score out of 110, with 110 indicating the worst symptomatology; the QOD-NS consists of 17 distinct items graded on a 3-point Likert scale, with the highest overall score of 51 indicating the lowest QoL.
A retrospective review of the CUIMC electronic medical record (EMR) was completed for all 105 patients to identify a history of otolaryngologic evaluation and endoscopic sinus surgery and collated with patient-reported historical care outside of CUIMC records. At CUIMC, CF patients are referred to otolaryngology by their pulmonologist if they present with persistent or recurrent sinonasal symptoms or sinus infections; patients with a history of sinus surgery may also be referred if follow-up is deemed necessary. Notes from visits and procedures completed at CUIMC were reviewed and date of first otolaryngology visit was obtained for patients with on-site otolaryngologic care. Dates of all previous primary and revision endoscopic sinus surgeries were also obtained, including procedures completed at CUIMC and other institutions. Patients with otolaryngologic evaluation for non-rhinologic issues (eg, hearing loss, vocal hoarseness) were excluded from analysis. Although escalating levels of intervention are offered when a patient is evaluated by an otolaryngologist, any involvement of a sinonasal expert on the care team allows for tailoring of treatment to patients’ specific needs, typically with improved sinonasal outcomes. 2 For this study, all patients with a history of endoscopic sinus surgery or otolaryngologic evaluation contributing to patient care are considered to have “otolaryngologic intervention” appropriate for their clinical need.
Analysis was conducted in R (R Core Team, Vienna, Austria). Data was non-normally distributed; therefore non-parametric Mann-Whitney U tests were used to assess differences in scores between different levels of otolaryngologic interventions, with P < .05 used as the significance threshold. Correlation coefficients were calculated between the 2 scoring methods and various pulmonary function tests (FEV1, FVC, FEV1/FVC) and results were plotted. Univariable ROC curves were generated to determine the discriminatory power of SNOT-22 and QOD-NS for predicting past otolaryngology intervention among patients. The Youden method was utilized to determine the cutoff point on the ROC curve closest to (0, 1) (the point with perfect sensitivity and specificity).
Results
We collected data for 105 consecutive patients who presented to an accredited cystic fibrosis specialty clinic. Demographic and visit characteristics for each patient are captured in Table 1. The average age of included patients was 32 (range: 20-69), and most patients were female (56.2%). Most patients (91.4%) identified as White/Caucasian (N = 96). Most visits in this cohort were classified as baseline well-care visits (N = 75, 71.4%), while the remaining visits (28.6%) were for an acute exacerbation of symptoms. Of all patients, 65.7% (N = 69) had been previously referred for otolaryngologic management; 23 of these patients (33.3%) were initially seen by a CUIMC-associated otolaryngologist, while 46 (66.6%) were previously seen by otolaryngology providers at a referring practice. Most referred patients (N = 63/69, 91.0%) had a history of undergoing ESS. Of these patients, 41 had a history of revision surgery, of whom 20 had a history of multiple revisions.
Patient Demographics, Visit Type, and History of Otolaryngologic Interventions.
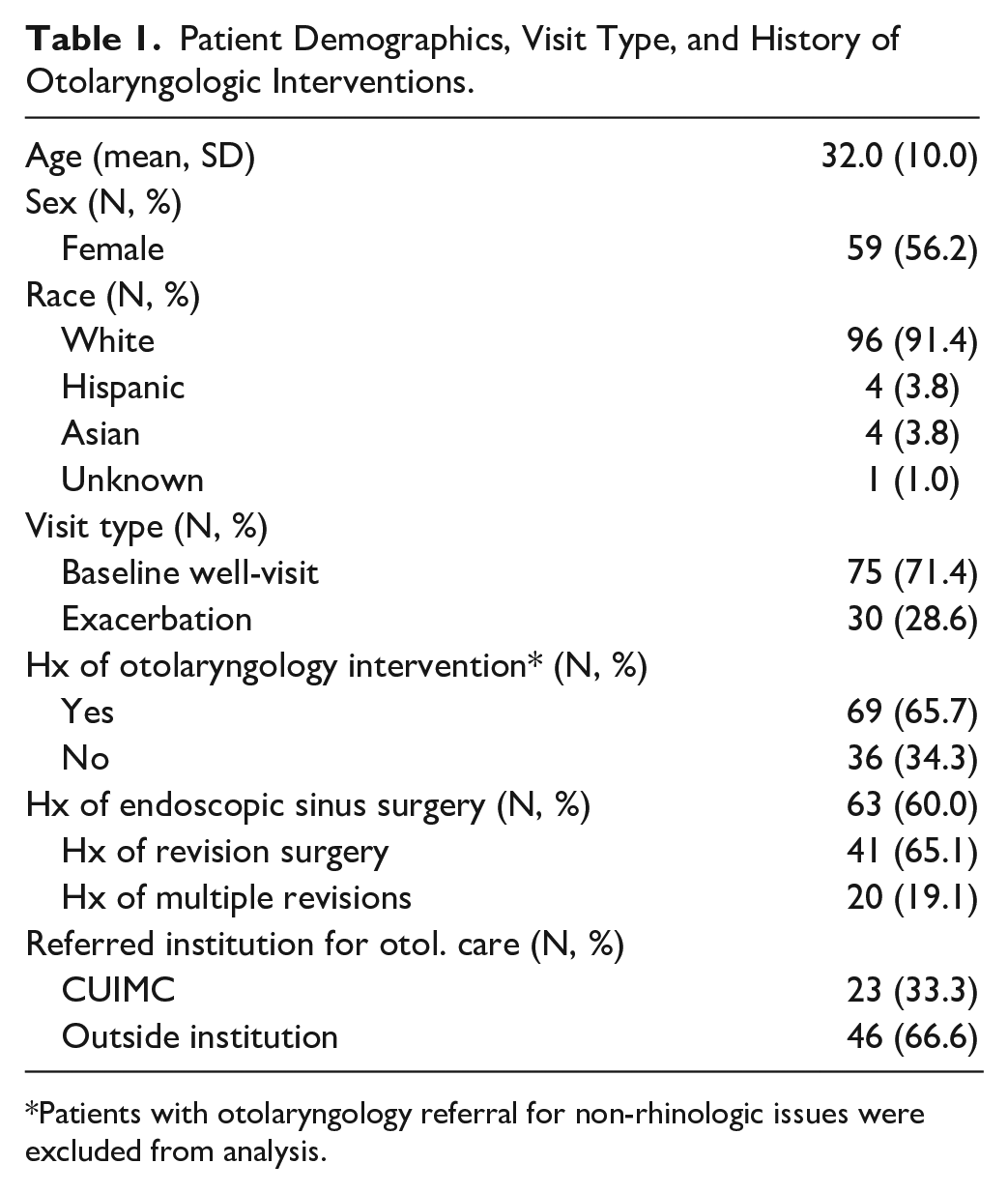
Patients with otolaryngology referral for non-rhinologic issues were excluded from analysis.
Average SNOT-22 and QOD-NS scores were stratified by staged intervention with ESS (Table 2). Within our consecutive patient cohort of 105 CF patients, the average SNOT-22 score was 30.4 (SD = 20.2). The average current SNOT-22 score for those who reported symptoms requiring otolaryngologic care was 33.2 (SD = 20.6) versus 24.9 (SD = 18.5) for those who did not (P = .048). Patients who reported prior ESS had an average SNOT-22 score of 32.7 (SD = 20.6) versus 27.0 (SD = 19.3) for those without surgical intervention (P = .17). Among those patients with a history of ESS, those requiring a single surgical intervention had an average SNOT-22 of 30.1 (SD = 18.3) versus 34.0 (SD = 21.9) for those who underwent revision surgery (single or multiple revision) (P = .67).
SNOT-22 Scores and QOD-NS Scores Stratified by Staged Otolaryngologic Intervention.
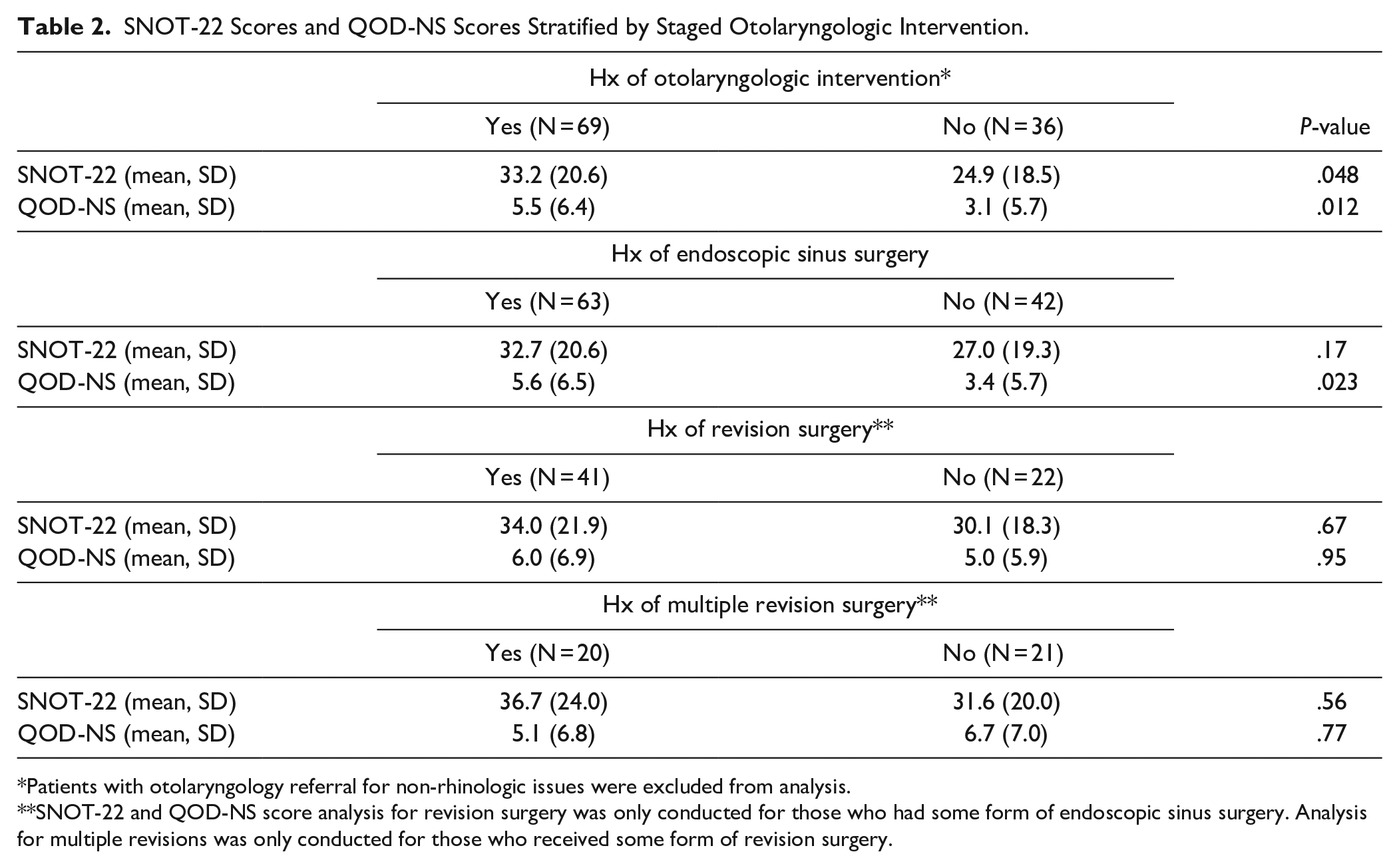
Patients with otolaryngology referral for non-rhinologic issues were excluded from analysis.
SNOT-22 and QOD-NS score analysis for revision surgery was only conducted for those who had some form of endoscopic sinus surgery. Analysis for multiple revisions was only conducted for those who received some form of revision surgery.
The average QOD-NS score for all patients was 4.7 (SD = 6.3). The average QOD-NS score among patients having otolaryngology intervention was 5.5 (SD = 6.4) versus 3.1 (SD = 5.7) for those without prior otolaryngologic issues (P = .012). Patients with a history of ESS had an average QOD-NS of 5.6 (SD = 6.5) versus 3.4 (SD = 5.7) for those without prior surgical intervention (P = .023). Among patients who underwent ESS, those requiring revision surgery had an average QOD-NS of 6.0 (SD = 6.9) versus 5.0 (SD = 5.9) for those avoiding revision surgery (P = .95).
The relationship between SNOT-22 scores and QOD-NS scores for CF patients was plotted, and scores were significantly correlated (P < .001); the R for the relationship was 0.43, indicating a modest correlation (Figure 1). ROC curves were generated using SNOT-22 (Figure 2) and QOD-NS (Figure 3) scores as a means of predicting past otolaryngology intervention. The area under the curve (AUC) for SNOT-22 was 0.62 (95% CI, 0.50-0.73) and the optimal cut-off was 18.5 (sensitivity = 0.71, specificity = 0.50). The AUC for QOD-NS was 0.65 (95% CI, 0.54-0.76), and the optimal cutoff was 3.5 (sensitivity = 0.46, specificity = 0.82).
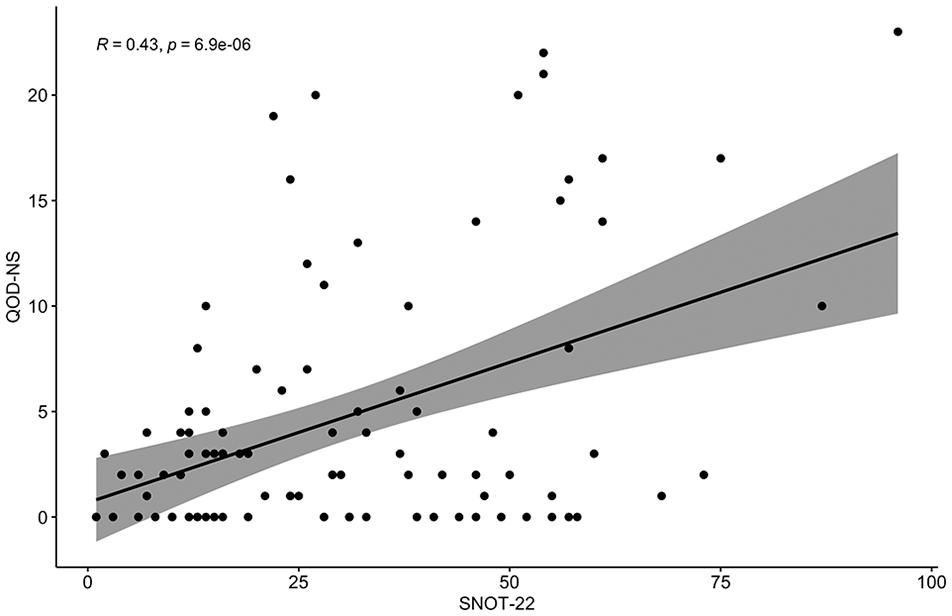
Correlation between QOD-NS and SNOT-22 scores for 105 patients.
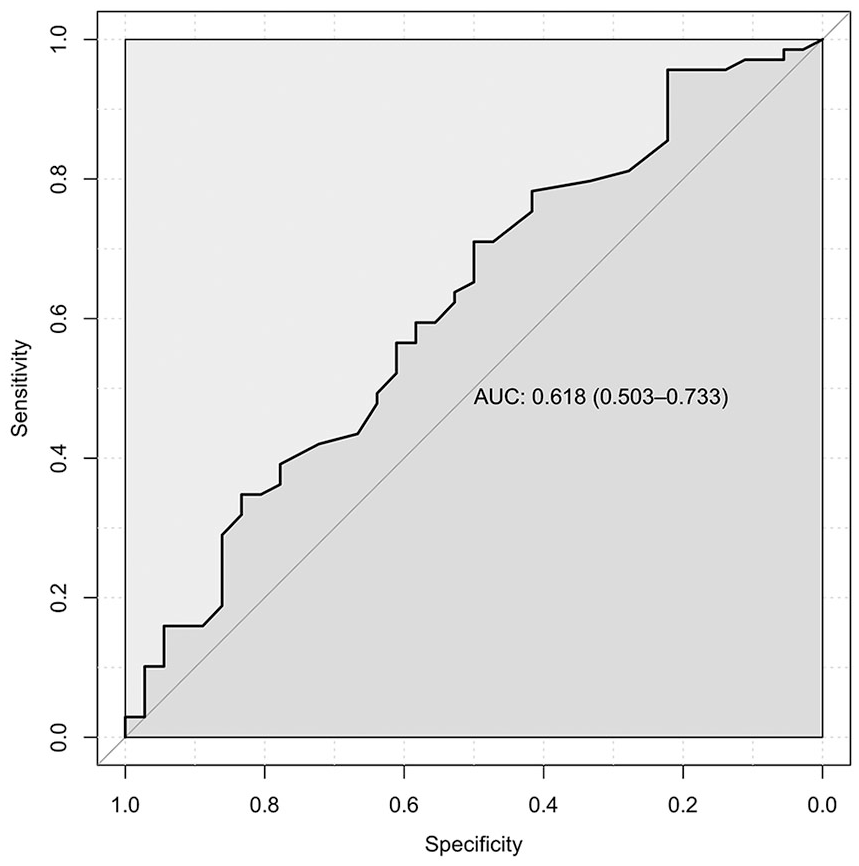
Receiver-operator curve for SNOT-22 values predicting otolaryngology referral.
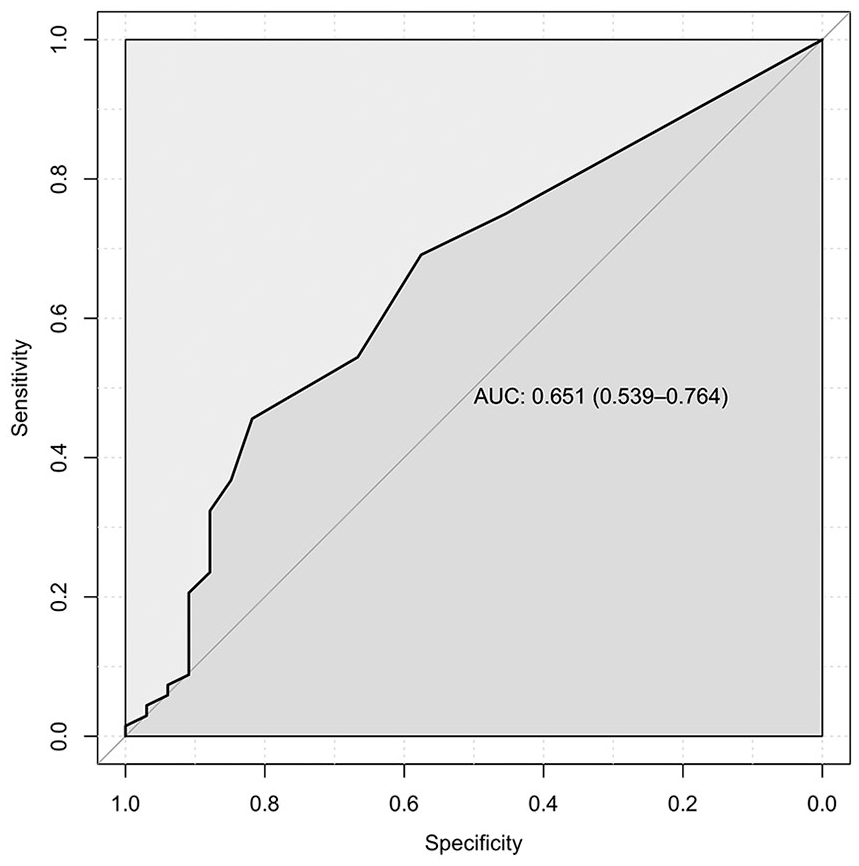
Receiver-operator curve for QOD-NS values predicting otolaryngology referral.
SNOT-22 and QOD-NS scores were also stratified by baseline versus exacerbation visit in addition to staged otolaryngologic intervention (Table 3). A previous study using the same patient population found that SNOT-22 scores were significantly elevated for exacerbation versus baseline visits. 3 In this study, for the baseline groups only, QOD-NS scores were significantly different for patients who had otolaryngologic intervention (5.3, SD 6.4) versus no intervention (3.1, SD 5.8) (P = .0082), as well as ESS (5.8, SD 6.7) versus no surgery (2.8, SD 5.3) (P = .012). Stratification by baseline versus exacerbation did not produce significantly different values for any other groups.
SNOT-22 scores and QOD-NS scores stratified by baseline versus exacerbation visit and staged intervention.
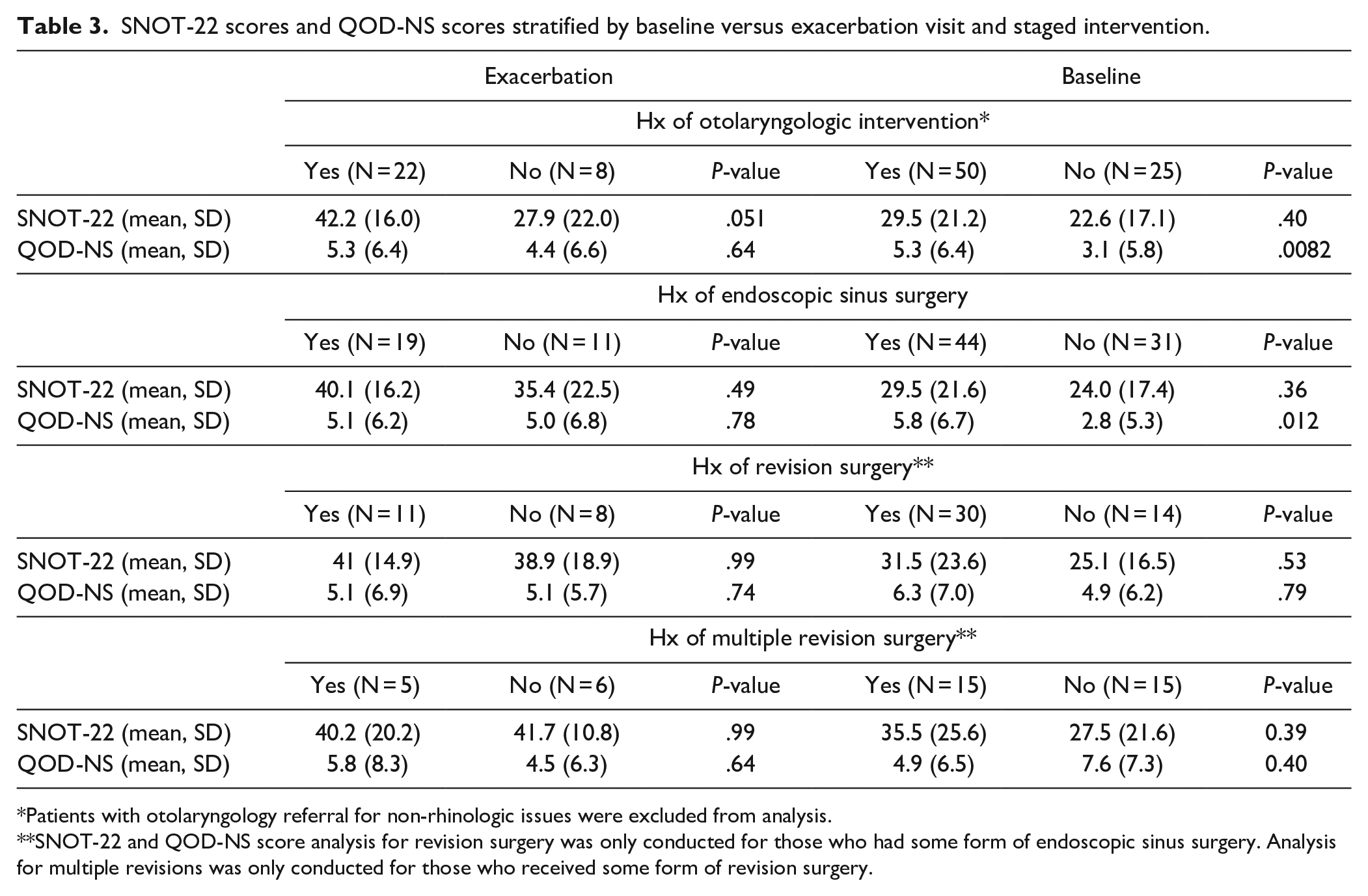
Patients with otolaryngology referral for non-rhinologic issues were excluded from analysis.
SNOT-22 and QOD-NS score analysis for revision surgery was only conducted for those who had some form of endoscopic sinus surgery. Analysis for multiple revisions was only conducted for those who received some form of revision surgery.
To evaluate the relationship between sinonasal quality-of-life and pulmonary function, we plotted QoL scores against 1-minute forced expiratory volume (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio (Supplemental Figure 1). FEV1/FVC ratio, the most frequently used indicator of pulmonary function, was not significantly correlated with SNOT-22 scores (R = −.12, P = .24) (Supplemental Figure 1(c)). FVC, an indicator of total lung capacity, was significantly correlated with SNOT-22 scores (R = −.20, P = .046) (Supplemental Figure 1(b)). FEV1 was not significantly correlated with SNOT-22 scores (R = −.18, P = .061) (Supplemental Figure 1(a)). We did not find an association between QOD-NS scores and any of the above PFTs (Supplemental Figure 2(a)–(c)). Additionally, SNOT-22 and QOD-NS scores were not significantly different for patients taking CFTR modulator therapy versus no modulator (P = .75 and P = .33, respectively) (Supplemental Table 1).
Discussion
Sinonasal quality-of-life is an increasingly important part of CF management, especially with improved life expectancy and greater focus on patient comfort. 14 There is broad awareness that sinonasal health is intrinsically linked to pulmonary health, and appropriate management of sinonasal symptoms may be crucial for optimization of pulmonary function in CF patients.15,16 Notably, we found that elevated SNOT-22 scores were significantly correlated with diminished FVC, although the correlation between SNOT-22 and FEV1/FVC ratio was not statistically significant. The correlation of SNOT-22 and FVC may suggest a relationship between chronic rhinosinusitis and restrictive lung disease, which are both associated with chronic inflammation in the airway mucosa. In fact, previous studies have demonstrated that inflammation in the upper airway leads to propagation of inflammation in the lower airway, predominantly through the transmission of inflammatory cytokines and IgE-mediated hypersensitivity via post-nasal drip mucus.17-20 Although obstructive lung disease with an elevation in FEV1 is classically seen in CF, a restrictive pattern may manifest in patients with a more chronic course of airway insult.
Otolaryngologists are uniquely equipped to improve sinonasal health in CF patients; thus, timely referral is warranted in most, if not all, cases. We demonstrate that patients with higher current SNOT-22 and QOD-NS scores were more likely to have been seen by an otolaryngologist in the past. We specifically show that a SNOT-22 score above 18.5 and a QOD-NS score above 3.5 had discriminatory power to predict past otolaryngology involvement. Additionally, the difference in SNOT-22 scores between patients with a history of multidisciplinary otolaryngologic care and those without care was 8.3, approaching the previously established MCID of 8.9 for this instrument. 21 The MCID for the QOD-NS is not as well established and ranges between 2.6 and 8.6 8 ; in our study, the difference in QOD-NS scores between patients with and without otolaryngologic care was 2.4.
The elevation in current QoL scores among referred patients may indicate prior appropriate triage for CF patients who could most benefit from multi-disciplinary care; alternatively, these elevated scores may suggest a need for additional otolaryngologic intervention. The former notion suggests that QoL scores remain unchanged or inevitably worsen regardless of past otolaryngologic intervention, which in turn implies that all patients with previous intervention should have elevated QoL scores. A study evaluating the longitudinal changes in QoL scores following intervention would help substantiate this claim. The latter possibility suggests that past otolaryngologic intervention was either unsuccessful or inadequate and additional management is required. Importantly, the predictive power of the SNOT-22 and QOD-NS must be relatively robust if these QoL measures are to be used to guide additional management.
To evaluate the predictive utility of QoL outcome measures, we performed an ROC curve analysis using past otolaryngologic intervention. Overall, the SNOT-22 was a moderately sensitive but not highly specific predictor for otolaryngologic intervention (sensitivity = 0.71, specificity = 0.50). In contrast, the QOD-NS had a higher specificity, but worse sensitivity (sensitivity =0.46, specificity = 0.82). These results indicate that the SNOT-22 and QOD-NS alone have limited predictive power for past intervention; however, they may have greater utility when used in combination. Notably, in our non-stratified analysis, the QOD-NS, but not the SNOT-22, was significantly elevated for patients who had received ESS, and when stratifying for baseline versus exacerbation visit, QOD-NS scores were significantly elevated for baseline patients who had received otolaryngologic care or ESS. This result suggests that the QOD-NS may have greater utility than the SNOT-22 in particular patient populations, and may help fill in gaps where the SNOT-22 may be lacking. Further analysis with various combinations of patient-reported outcome measures is required to determine which instruments may help streamline referral and is grounds for future studies.
Currently, there are no definitive diagnostic criteria or treatment algorithms for CF-related CRS.2,10 Though interventions like ESS and nasal irrigation have proven effective, timing of these procedures remains unspecified, especially since CRS is often underdiagnosed in CF patients until symptoms become severe. 10 In fact, timing of intervention, both medical and surgical, is critically important in determining outcomes, as earlier intervention appears to improve outcomes for patients with non-CF related CRS. 22 Though the SNOT-22 and QOD-NS alone have limited predictive power, the fact that patients with past otolaryngologic intervention had persistently elevated QoL scores likely means that past referral for multidisciplinary care was appropriate. Regular integration of sinus-specific patient-reported outcome measures in the management of CF may thus be useful in informing expedited collaboration. By ensuring that patients are screened early for sinonasal dysfunction, care teams will be able to direct subspecialty referral appropriately and ultimately prevent declines in QoL. Additional studies are necessary to determine if QoL instruments have greater predictive value when administered early in disease progression, once sinonasal symptoms appear, at baseline visits, or during exacerbations.
A limitation in this study is the cross-sectional design. Questionnaires were administered at 1 time point for all patients, regardless of symptomatology or disease progression. Longitudinal follow-up with patients at both baseline and exacerbation visits would have provided more information on score fluctuation over time; patients with more or less fluctuant scores may have had differing otolaryngologic needs. An additional limitation is the retrospective chart review used to obtain information on past ESS and otolaryngology evaluation. Though otolaryngology intervention was used as an outcome in our analysis, we were not able to ascertain whether the patient benefitted from these visits. Furthermore, because the electronic medical record (EMR) was limited to visits and procedures completed at CUIMC, all data from outside institutions relied on accurate patient reporting, as this data was obtained from routine history taking during office visits.
Conclusion
Here, we report QoL metrics among CF patients that demonstrate variations based on previous integration of otolaryngology within the ranks of the care team. Patients with higher current SNOT-22 and QOD-NS scores were more likely to have had otolaryngologic intervention in the past, indicating an additional need for otolaryngologic consultation for patients with low sinonasal QoL. In total, ROC analysis revealed marginal predictive value for the SNOT-22 and QOD-NS, with the SNOT-22 having higher sensitivity and the QOD-NS having higher specificity. Previous studies have demonstrated the utility of QoL instruments in diagnosing CRS. Our study further supports the utility of such instruments in directing the involvement of otolaryngologists in the management of CF-related CRS. Future studies will clarify which QoL instruments or combination thereof are optimal in predicting otolaryngologic care, and determine the timing of survey administration with regards to disease progression.
Supplemental Material
sj-docx-1-aor-10.1177_00034894211045636 – Supplemental material for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients
Supplemental material, sj-docx-1-aor-10.1177_00034894211045636 for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients by Stephen Leong, Rahul K. Sharma, Chetan Safi, Emily DiMango, Claire Keating, David A. Gudis and Jonathan B. Overdevest in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-tiff-1-aor-10.1177_00034894211045636 – Supplemental material for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients
Supplemental material, sj-tiff-1-aor-10.1177_00034894211045636 for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients by Stephen Leong, Rahul K. Sharma, Chetan Safi, Emily DiMango, Claire Keating, David A. Gudis and Jonathan B. Overdevest in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-tiff-2-aor-10.1177_00034894211045636 – Supplemental material for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients
Supplemental material, sj-tiff-2-aor-10.1177_00034894211045636 for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients by Stephen Leong, Rahul K. Sharma, Chetan Safi, Emily DiMango, Claire Keating, David A. Gudis and Jonathan B. Overdevest in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-tiff-3-aor-10.1177_00034894211045636 – Supplemental material for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients
Supplemental material, sj-tiff-3-aor-10.1177_00034894211045636 for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients by Stephen Leong, Rahul K. Sharma, Chetan Safi, Emily DiMango, Claire Keating, David A. Gudis and Jonathan B. Overdevest in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-tiff-4-aor-10.1177_00034894211045636 – Supplemental material for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients
Supplemental material, sj-tiff-4-aor-10.1177_00034894211045636 for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients by Stephen Leong, Rahul K. Sharma, Chetan Safi, Emily DiMango, Claire Keating, David A. Gudis and Jonathan B. Overdevest in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-tiff-5-aor-10.1177_00034894211045636 – Supplemental material for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients
Supplemental material, sj-tiff-5-aor-10.1177_00034894211045636 for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients by Stephen Leong, Rahul K. Sharma, Chetan Safi, Emily DiMango, Claire Keating, David A. Gudis and Jonathan B. Overdevest in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-tiff-6-aor-10.1177_00034894211045636 – Supplemental material for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients
Supplemental material, sj-tiff-6-aor-10.1177_00034894211045636 for Association of Quality of Life Measures and Otolaryngologic Care in Cystic Fibrosis Patients by Stephen Leong, Rahul K. Sharma, Chetan Safi, Emily DiMango, Claire Keating, David A. Gudis and Jonathan B. Overdevest in Annals of Otology, Rhinology & Laryngology
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.